
Target Maintenance in Gaming via Saliency Augmentation: An Early-Stage Scotoma Simulation Study Using Virtual Reality (VR)


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Set-Up
2.3. Calibration Procedure
2.4. Experimental Procedure
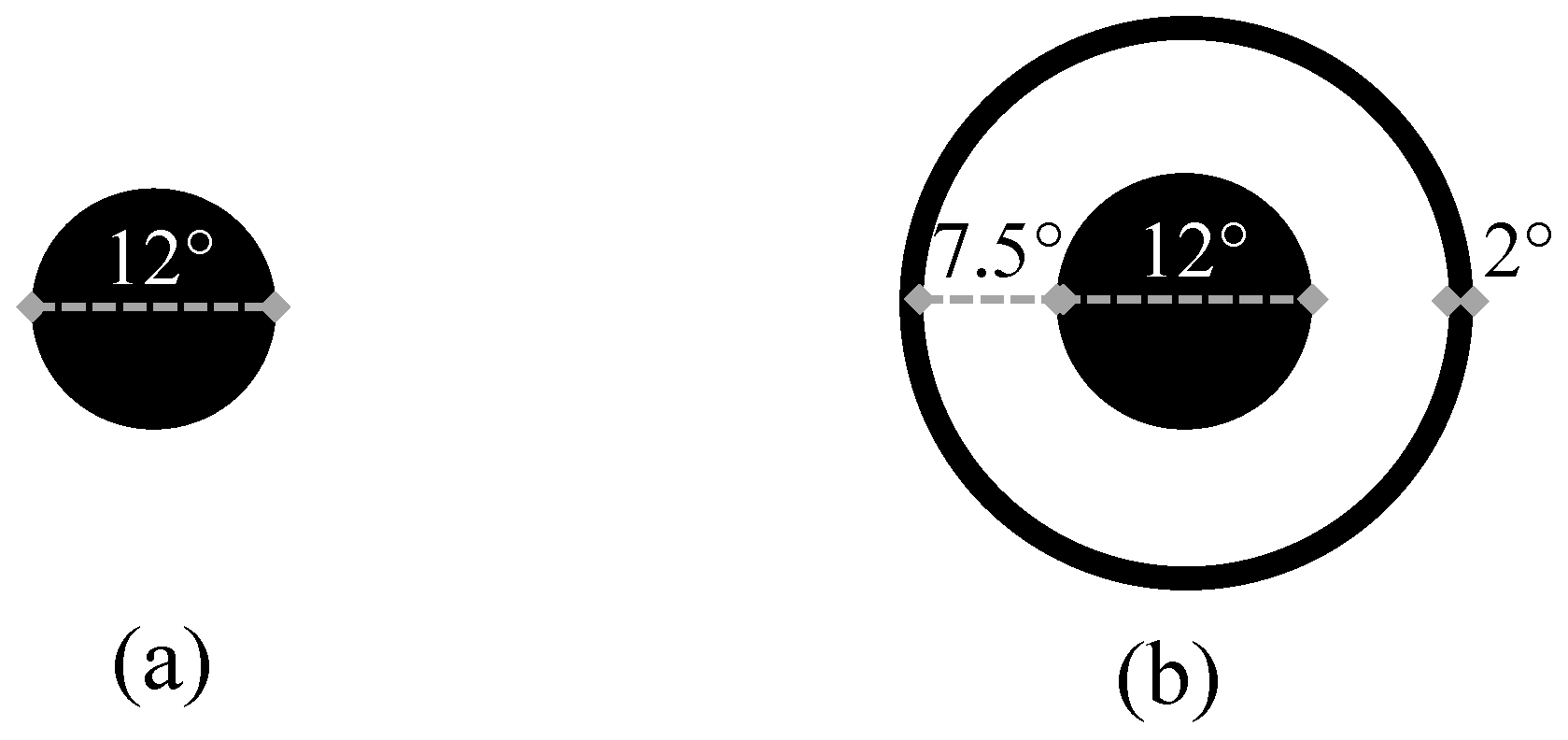
2.4.1. Conditions
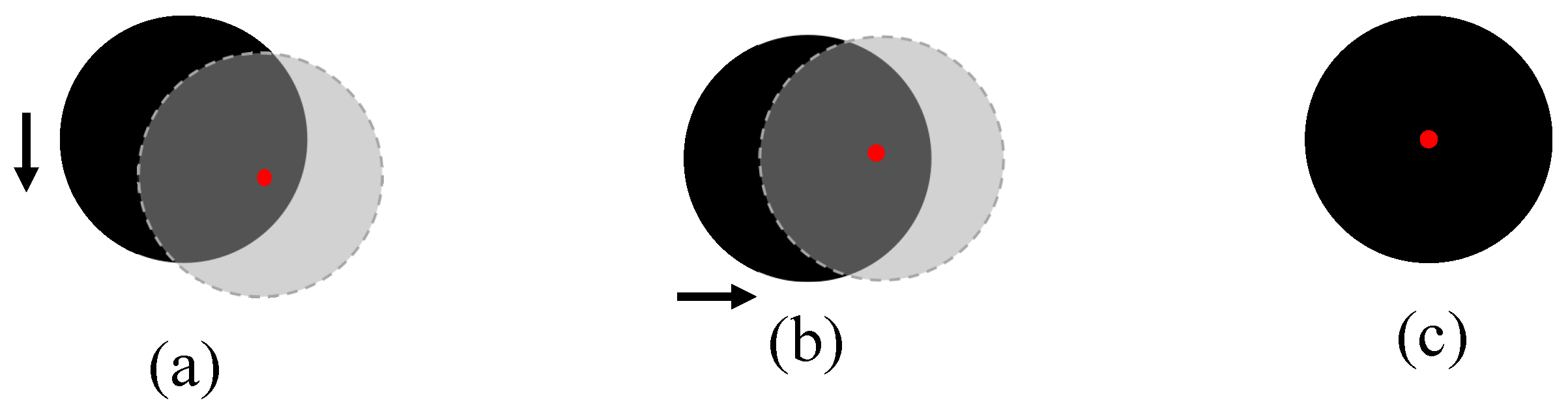
2.4.2. Manual Drift Correction
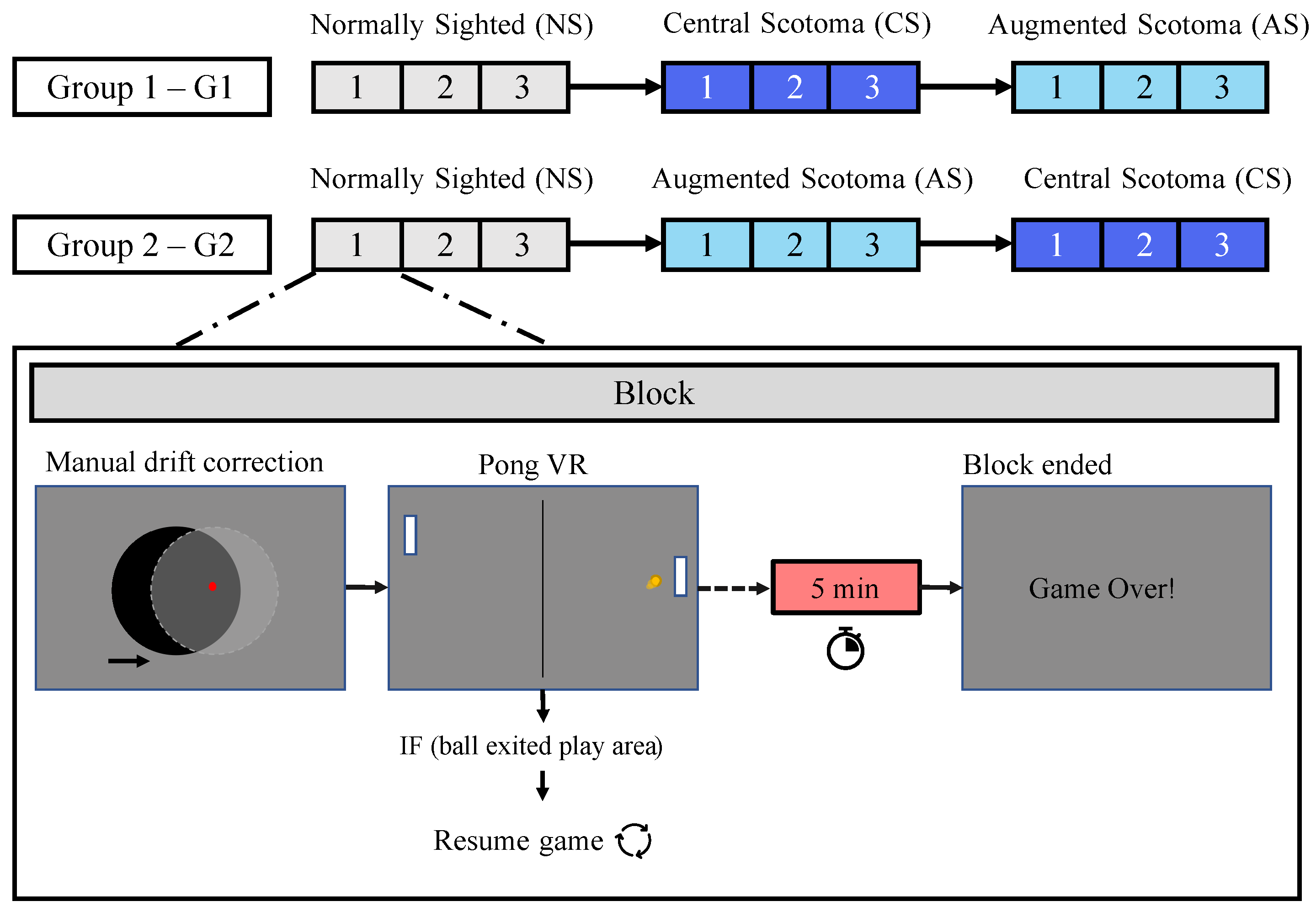
2.5. Groups
3. Data Processing
3.1. Data Pre-Processing
3.1.1. Noise Cancellation: Fluctuation in the Sampling Data
3.1.2. Latency Error Correction
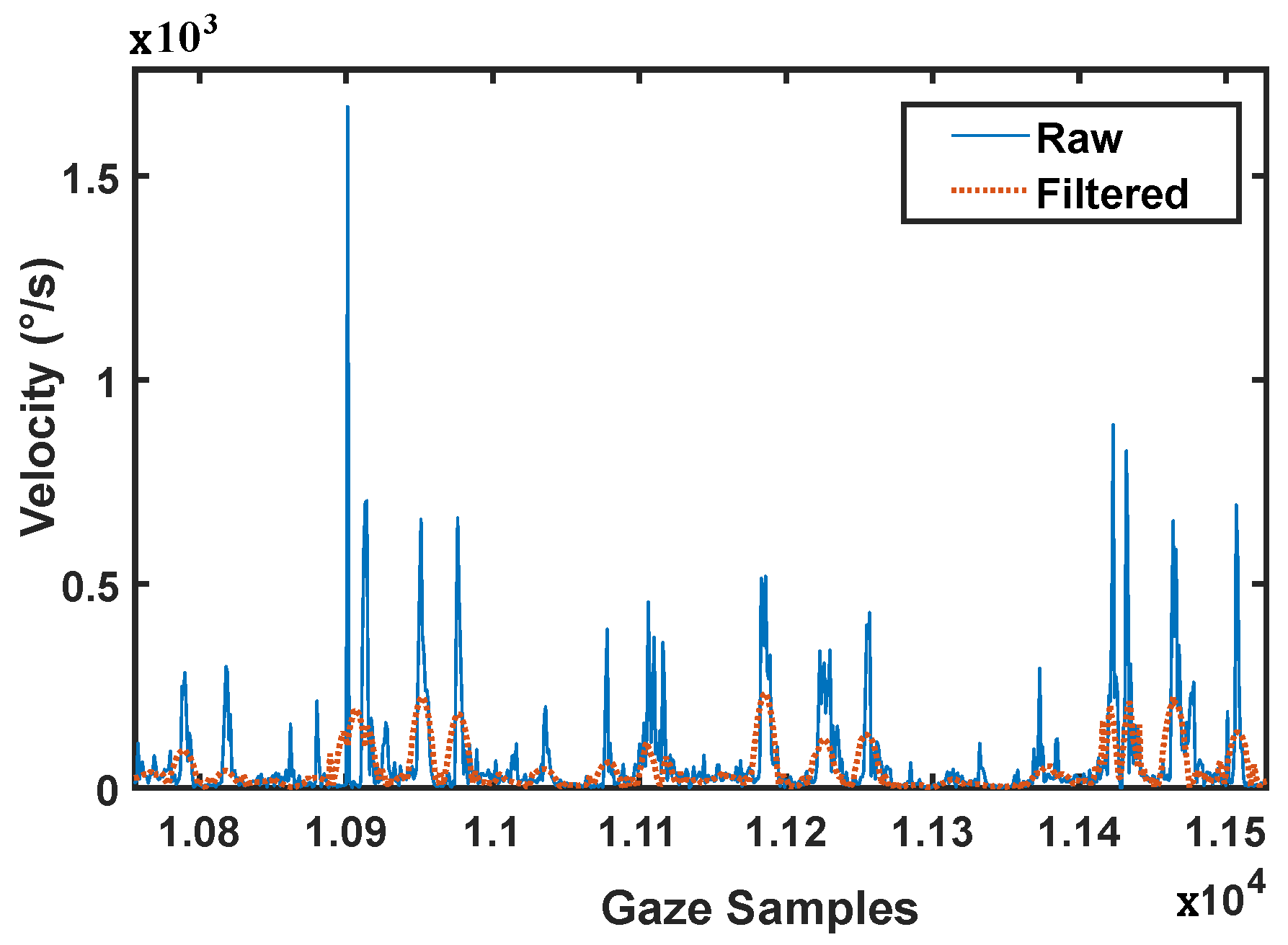
3.1.3. Eye-Tracking Data Filtering
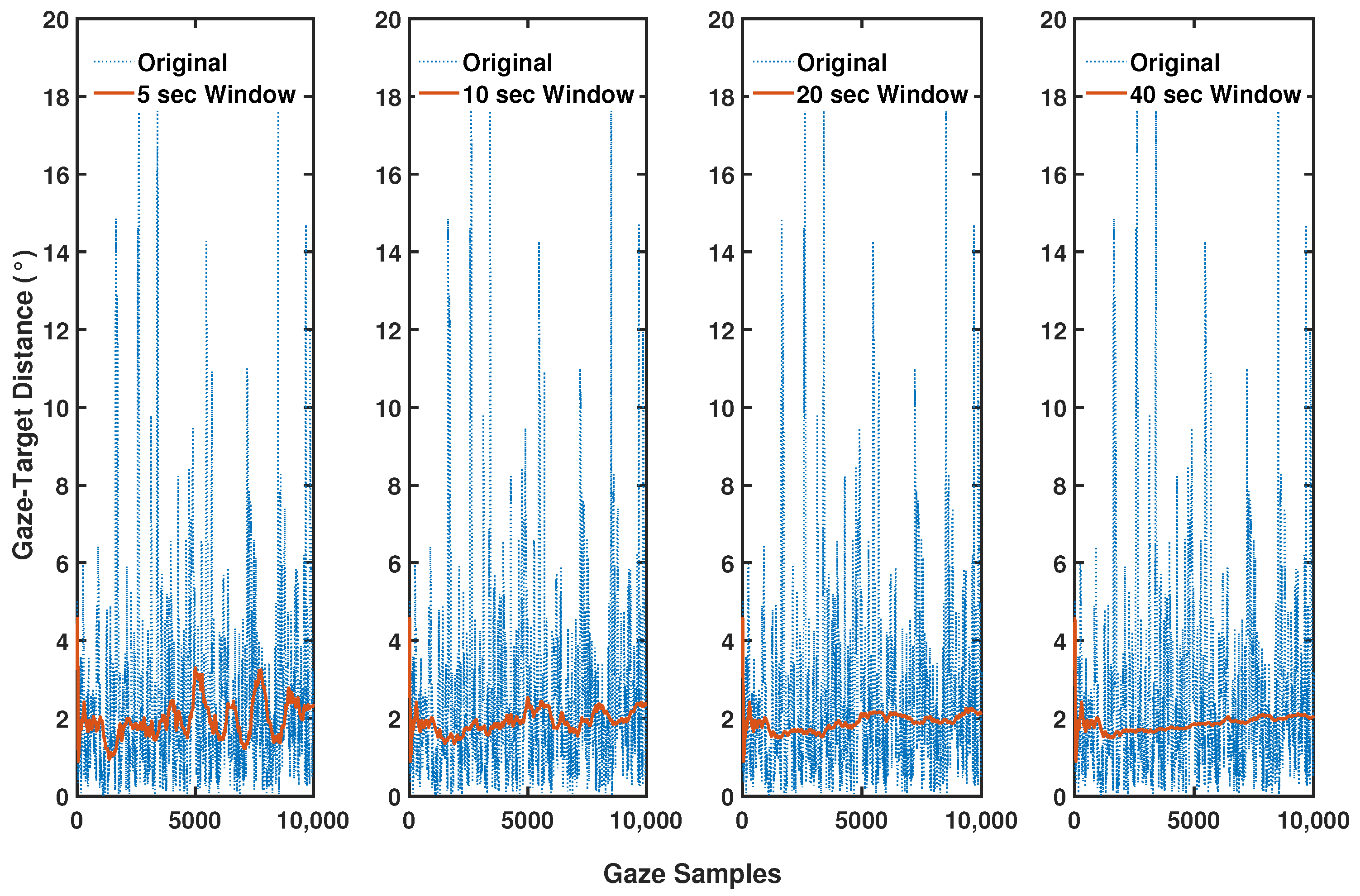
3.1.4. Saccades Smoothing: Moving Median Window
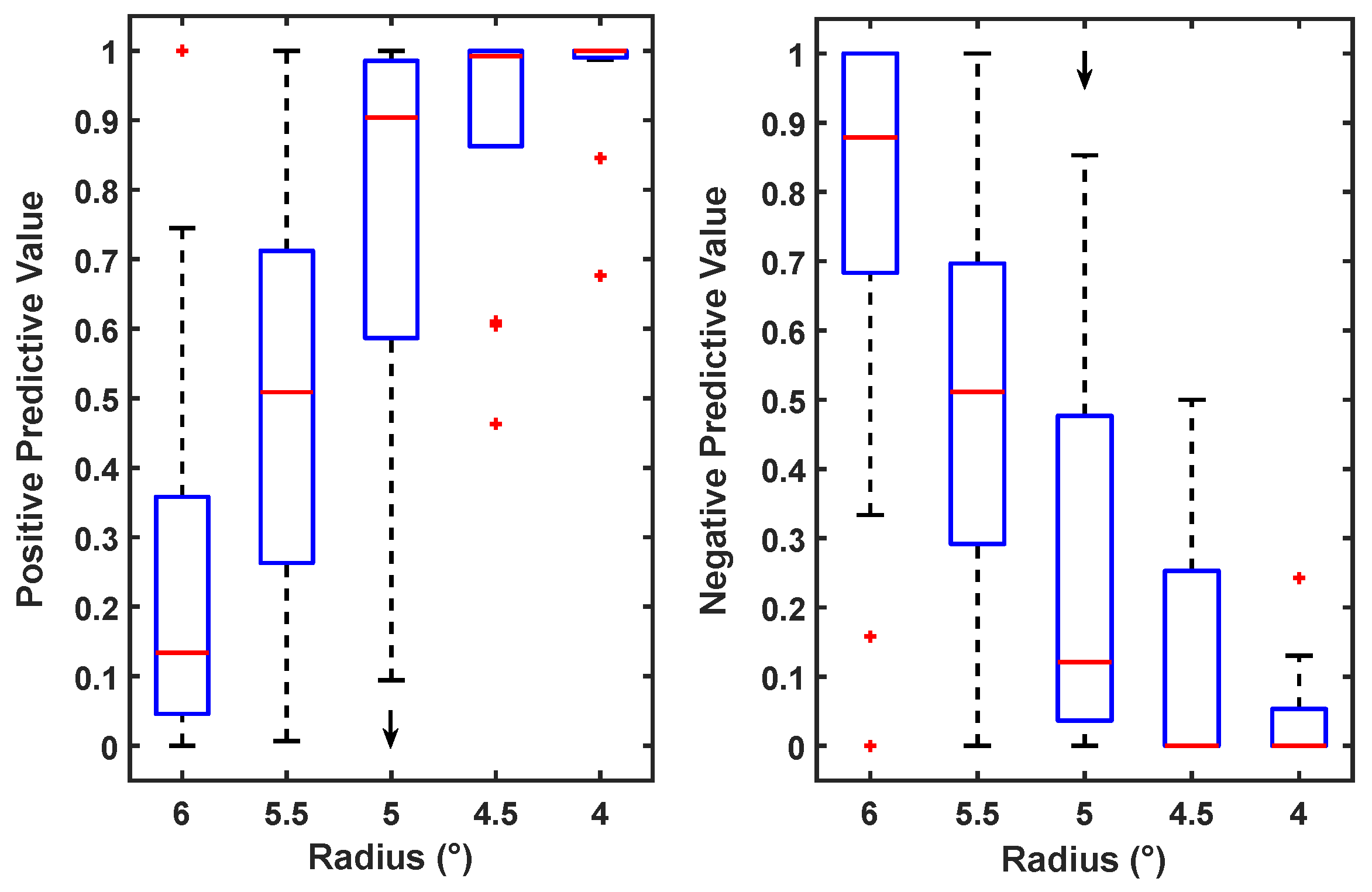
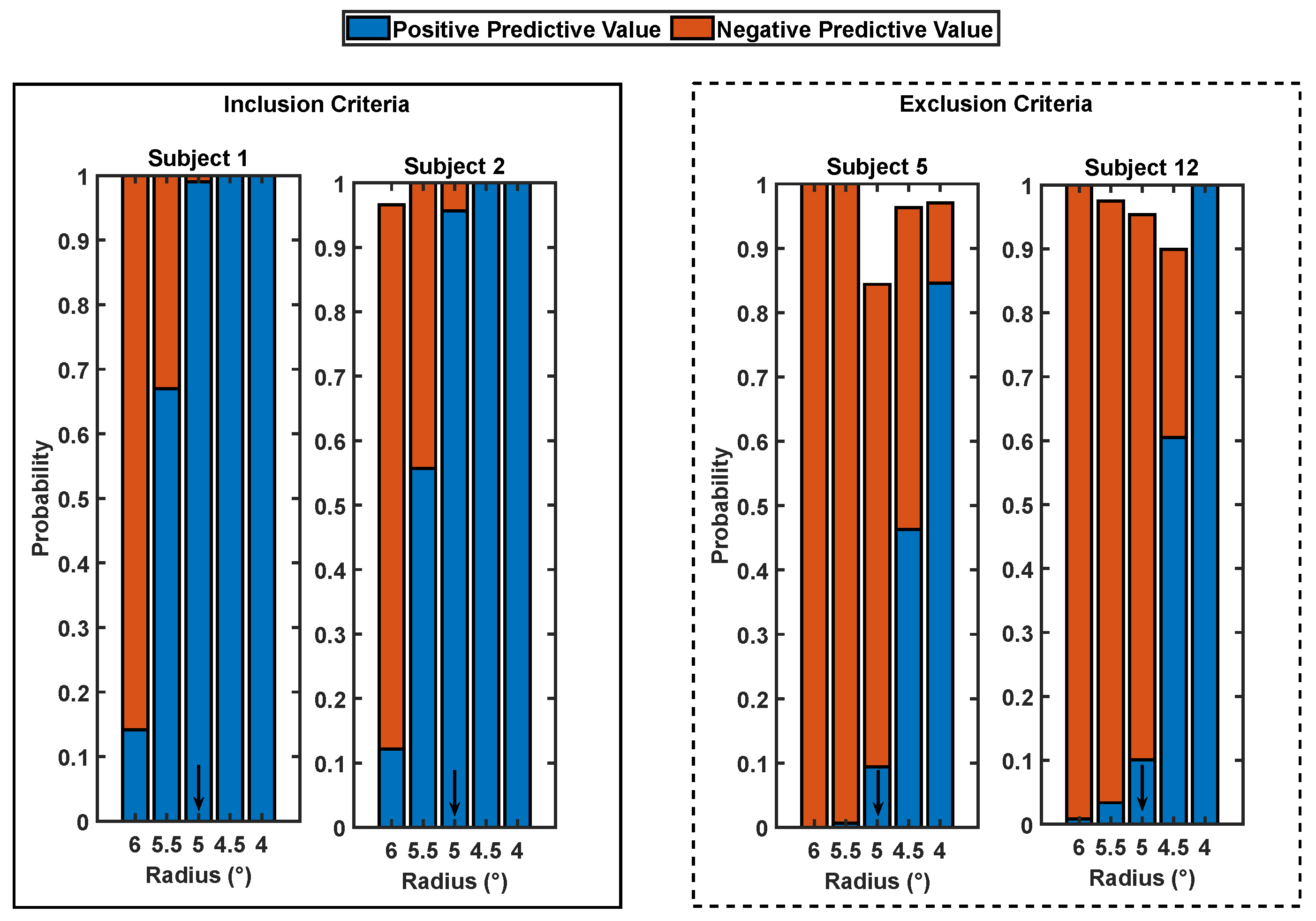
3.1.5. Colour Change Recognition Sub-Task and Scotoma Radius as Cutoff for the Maximum Positive and Negative Predictive Values
3.2. Data Analysis
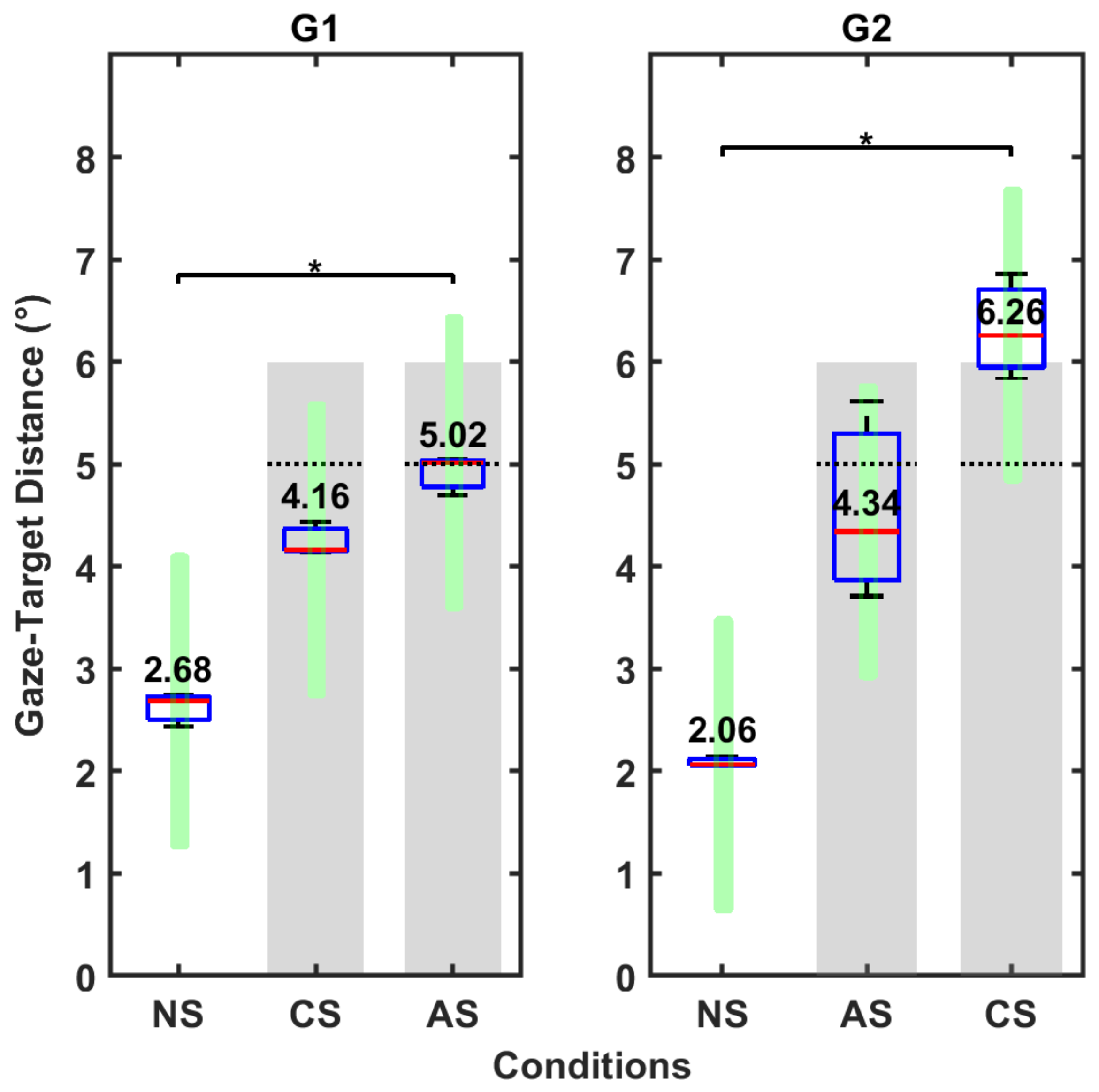
3.2.1. Gaze-Target Distancing: Condition Type Influence over Eye Position
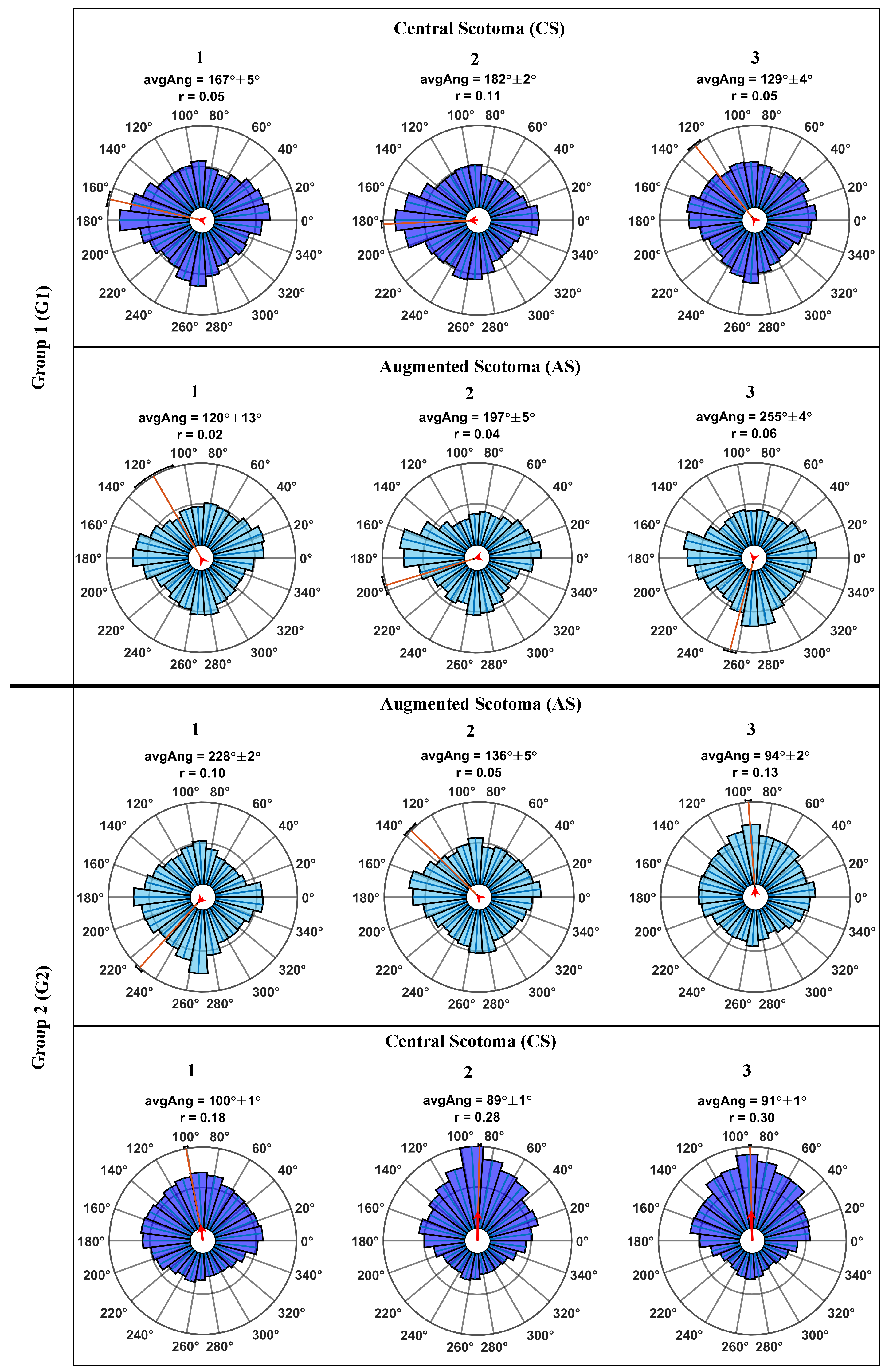
3.2.2. Gaze-Target Direction: Training Effect across Blocks
4. Results
4.1. Data Pre-Processing
4.1.1. Noise Cancellation: Fluctuation in the Sampling Data
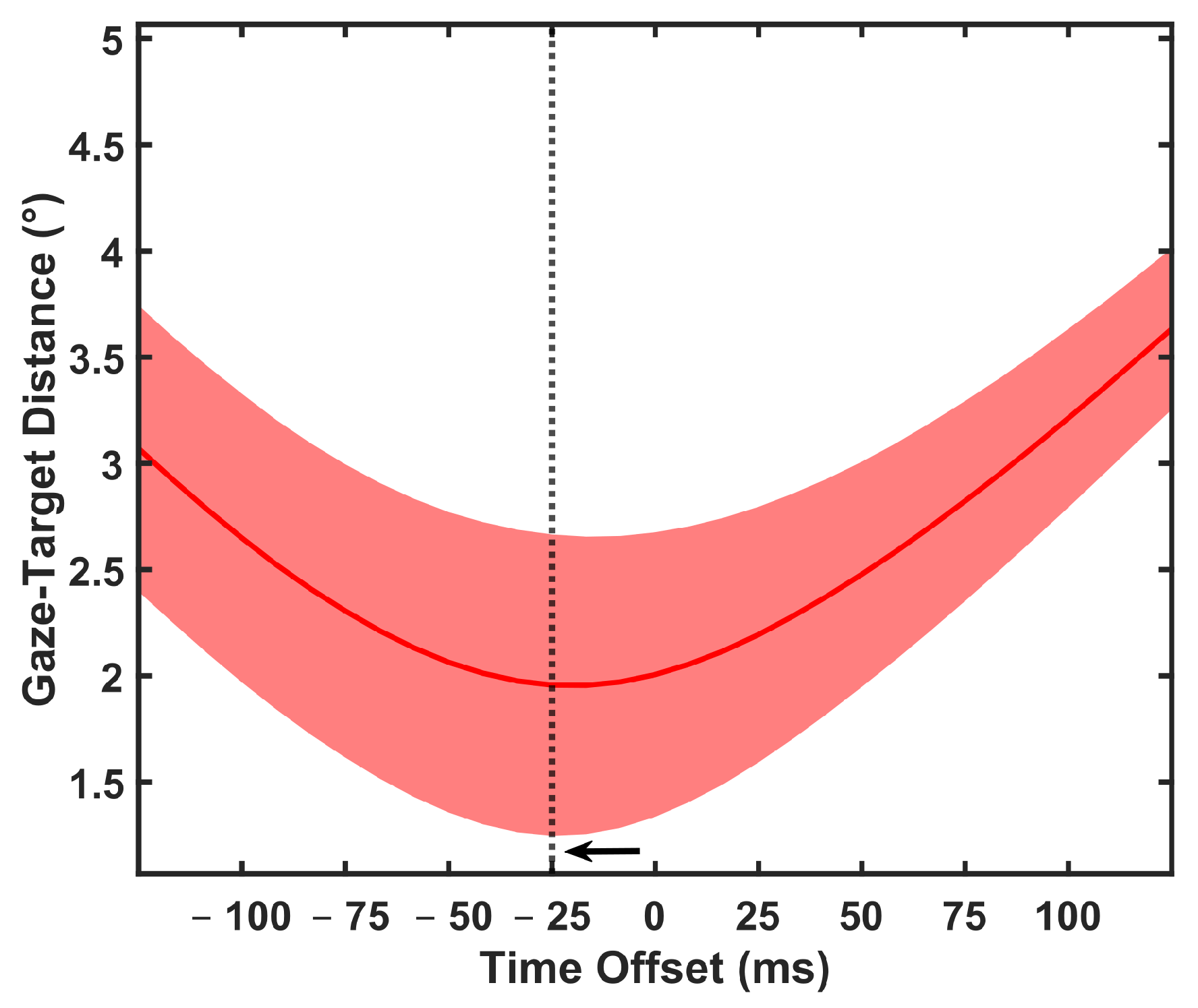
4.1.2. Latency Error Correction
4.1.3. Eye-Tracking Data Filtering
4.1.4. Saccades Smoothing: Moving Median Window
4.1.5. Colour Change Recognition Sub-Task and Scotoma Radius as Cutoff for the Maximum Positive and Negative Predictive Values
4.2. Data Analysis
4.2.1. Gaze-Target Distancing: Condition Type Influence over Eye Position
4.2.2. Gaze-Target Direction: Training Effect across Blocks
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wong, W.L.; Su, X.; Li, X.; Cheung, C.M.G.; Klein, R.; Cheng, C.Y.; Wong, T.Y. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: A systematic review and meta-analysis. Lancet Glob. Health 2014, 2, e106–e116. [Google Scholar] [CrossRef]
- Harvey, P.T. Common Eye Diseases of Elderly People: Identifying and Treating Causes of Vision Loss. Gerontology 2003, 49, 1–11. [Google Scholar] [CrossRef]
- Zou, M.; Wang, S.; Chen, A.; Liu, Z.; Young, C.A.; Zhang, Y.; Jin, G.; Zheng, D. Prevalence of myopic macular degeneration worldwide: A systematic review and meta-analysis. Br. J. Ophthalmol. 2020, 104, 1748–1754. [Google Scholar] [CrossRef] [PubMed]
- Altpeter, E.; Mackeben, M.; Trauzettel-Klosinski, S. The importance of sustained attention for patients with maculopathies. Vis. Res. 2000, 40, 1539–1547. [Google Scholar] [CrossRef]
- Curcio, C.A.; Sloan, K.R.; Kalina, R.E.; Hendrickson, A.E. Human photoreceptor topography. J. Comp. Neurol. 1990, 292, 497–523. [Google Scholar] [CrossRef] [PubMed]
- Cummings, R.W.; Whittaker, S.G.; Watson, G.R.; Budd, J.M. Scanning characters and reading with a central scotoma. Optom. Vis. Sci. 1985, 62, 833–843. [Google Scholar] [CrossRef]
- Timberlake, G.T.; Mainster, M.A.; Peli, E.; Augliere, R.A.; Essock, E.A.; Arend, L.E. Reading with a macular scotoma. I. Retinal location of scotoma and fixation area. Investig. Ophthalmol. Vis. Sci. 1986, 27, 1137–1147. [Google Scholar]
- Timberlake, G.T.; Peli, E.; Essock, E.A.; Augliere, R.A. Reading with a macular scotoma. II. Retinal locus for scanning text. Investig. Ophthalmol. Vis. Sci. 1987, 28, 1268–1274. [Google Scholar]
- White, J.M.; Bedell, H.E. The oculomotor reference in humans with bilateral macular disease. Investig. Ophthalmol. Vis. Sci. 1990, 31, 1149–1161. [Google Scholar]
- Schuchard, R.A. Validity and Interpretation of Amsler Grid Reports. Arch. Ophthalmol. 1993, 111, 776–780. [Google Scholar] [CrossRef]
- Hassan, S.E.; Snyder, B.D. Street-crossing decision-making: A comparison between patients with age-related macular degeneration and normal vision. Investig. Ophthalmol. Vis. Sci. 2012, 53, 6137–6144. [Google Scholar] [CrossRef] [PubMed]
- Almutleb, E.S.; Hassan, S.E. The Effect of Simulated Central Field Loss on Street-crossing Decision-Making in Young Adult Pedestrians. Optom. Vis. Sci. Off. Publ. Am. Acad. Optom. 2020, 97, 229–238. [Google Scholar] [CrossRef]
- Morales, M.U.; Limoli, P.G.; Limoli, C. Augmented reality eyewear for home-based vision training after biofeedback rehabilitation of eccentric fixation. Investig. Ophthalmol. Vis. Sci. 2015, 56, 548. [Google Scholar]
- Pratt, J.D.; Stevenson, S.B.; Bedell, H.E. Scotoma Visibility and Reading Rate with Bilateral Central Scotomas. Optom. Vis. Sci. Off. Publ. Am. Acad. Optom. 2017, 94, 279. [Google Scholar] [CrossRef] [PubMed]
- Deemer, A.D.; Swenor, B.K.; Fujiwara, K.; Deremeik, J.T.; Ross, N.C.; Natale, D.M.; Bradley, C.K.; Werblin, F.S.; Massof, R.W. Preliminary evaluation of two digital image processing strategies for head-mounted magnification for low vision patients. Transl. Vis. Sci. Technol. 2019, 8, 23. [Google Scholar] [CrossRef]
- Bertera, J.H. Oculomotor adaptation with virtual reality scotomas. Simulation 1992, 59, 37–43. [Google Scholar] [CrossRef]
- Bertera, J.H. The Effect of Simulated Scotomas on Visual Search in Normal Subjects. Investig. Ophthalmol. Vis. Sci. 1988, 29, 470–475. [Google Scholar]
- Kwon, M.; Nandy, A.S.; Tjan, B.S. Rapid and persistent adaptability of human oculomotor control in response to simulated central vision loss. Curr. Biol. 2013, 23, 1663–1669. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Ashmead, D.H.; Adams, H.; Bodenheimer, B. Using Virtual Reality to Assess the Street Crossing Behavior of Pedestrians with Simulated Macular Degeneration at a Roundabout. Front. ICT 2018, 5, 27. [Google Scholar] [CrossRef]
- Pidcoe, P.E.; Wetze, P.A. Oculomotor tracking strategy in normal subjects with and without simulated scotoma. Investig. Ophthalmol. Vis. Sci. 2006, 47, 169–178. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Guez, J.E.; Le Gargasson, J.F.; Rigaudiere, F.; O’Regan, J.K. Is there a systematic location for the pseudo-fovea in patients with central scotoma? Vis. Res. 1993, 33, 1271–1279. [Google Scholar] [CrossRef]
- Lewis, J.; Shires, L.; Brown, D.J. Development of a Visual Impairment Simulator Using the Microsoft XNA Framework. In Proceedings of the 9th International Conference on Disability, Virtual Reality and Associated Technologies (ICDVRAT), Laval, France, 10–12 September 2012. [Google Scholar]
- Väyrynen, J.; Colley, A.; Häkkilä, J. Head mounted display design tool for simulating visual disabilities. In Proceedings of the ACM International Conference Proceeding Series, Association for Computing Machinery (MUM 2016), Rovaniemi, Finland, 13–15 December 2016; pp. 69–73. [Google Scholar] [CrossRef]
- Kwon, M.; Ramachandra, C.; Satgunam, P.; Mel, B.W.; Peli, E.; Tjan, B.S. Contour enhancement benefits older adults with simulated central field loss. Optom. Vis. Sci. 2012, 89, 1374–1384. [Google Scholar] [CrossRef] [PubMed]
- Barraza-Bernal, M.J.; Ivanov, I.V.; Nill, S.; Rifai, K.; Trauzettel-Klosinski, S.; Wahl, S. Can positions in the visual field with high attentional capabilities be good candidates for a new preferred retinal locus? Vis. Res. 2017, 140, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Zhaoping, L. Attention capture by eye of origin singletons even without awareness—A hallmark of a bottom-up saliency map in the primary visual cortex. J. Vis. 2008, 8, 1. [Google Scholar] [CrossRef] [PubMed]
- Warner, C.B.; Juola, J.F.; Koshino, H. Voluntary allocation versus automatic capture of visual attention. Percept. Psychophys. 1990, 48, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Parr, T.; Friston, K.J. Attention or Salience? Curr. Opin. Psychol. 2019, 29, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Lumsden, J.; Edwards, E.A.; Lawrence, N.S.; Coyle, D.; Munafò, M.R. Gamification of Cognitive Assessment and Cognitive Training: A Systematic Review of Applications and Efficacy. JMIR Serious Games 2016, 4, e11. [Google Scholar] [CrossRef] [PubMed]
- Vive Pro Eye, VIVE Pro Eye|The Professional-Grade VR Headset. Available online: https://www.vive.com/eu/product/vive-pro-eye/overview/ (accessed on 11 November 2020).
- Sipatchin, A.; Wahl, S.; Rifai, K. Eye-Tracking for Clinical Ophthalmology with Virtual Reality (VR): A Case Study of the HTC Vive Pro Eye’s Usability. Healthcare 2021, 9, 180. [Google Scholar] [CrossRef]
- Stein, N.; Niehorster, D.C.; Watson, T.; Steinicke, F.; Rifai, K.; Wahl, S.; Lappe, M. A Comparison of Eye Tracking Latencies Among Several Commercial Head-Mounted Displays. i-Perception 2021, 12, 1–16. [Google Scholar] [CrossRef]
- Tobii Pro SDK, Tobii Pro SDK v1.7.1.1081. Available online: https://www.tobiipro.com/product-listing/tobii-pro-sdk/ (accessed on 22 June 2020).
- VIVE Eye Tracking SDK (SRanipal), SRanipal SDK v1.0.3.0. Available online: https://developer.vive.com/resources/vive-sense/sdk/vive-eye-tracking-sdk-sranipal/ (accessed on 23 September 2020).
- Clay, V.; König, P.; König, S. Eye tracking in virtual reality. J. Eye Mov. Res. 2019, 12. [Google Scholar] [CrossRef]
- Coey, C.A.; Wallot, S.; Richardson, M.J.; van Orden, G. On the structure of measurement noise in eye-tracking. J. Eye Mov. Res. 2012, 5, 5. [Google Scholar] [CrossRef]
- Liu, B.; Zhao, Q.C.; Ren, Y.Y.; Wang, Q.J.; Zheng, X.L. An elaborate algorithm for automatic processing of eye movement data and identifying fixations in eye-tracking experiments. Adv. Mech. Eng. 2018, 10, 2018. [Google Scholar] [CrossRef]
- Loschky, L.C.; Wolverton, G.S. How late can you update gaze-contingent multiresolutional displays without detection. ACM Trans. Multimed. Comput. Commun. Appl. 2007, 3. [Google Scholar] [CrossRef]
- Musall, S. Stdshade, MATLAB Central File Exchange. Available online: https://www.mathworks.com/matlabcentral/fileexchange/29534-stdshade (accessed on 23 June 2021).
- Nyström, M.; Holmqvist, K. An adaptive algorithm for fixation, saccade, and glissade detection in eyetracking data. Behav. Res. Methods 2010, 42, 188–204. [Google Scholar] [CrossRef]
- Savitzky, A.; Golay, M.J. Smoothing and Differentiation of Data by Simplified Least Squares Procedures. Anal. Chem. 1964, 36, 1627–1639. [Google Scholar] [CrossRef]
- Shanidze, N.; Ghahghaei, S.; Verghese, P. Accuracy of eye position for saccades and smooth pursuit. J. Vis. 2016, 16. [Google Scholar] [CrossRef] [PubMed]
- Whittaker, S.G.; Cummings, R.W.; Swieson, L.R. Saccade control without a fovea. Vis. Res. 1991, 31, 2209–2218. [Google Scholar] [CrossRef]
- Saunders, D.R.; Woods, R.L. Direct measurement of the system latency of gaze-contingent displays. Behav. Res. Methods 2014, 46, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Aguilar, C.; Castet, E. Gaze-contingent simulation of retinopathy: Some potential pitfalls and remedies. Vis. Res. 2011, 51, 997–1012. [Google Scholar] [CrossRef] [PubMed]
- Zittrell, F. CircHist—Circular/Polar/Angle Histogram. Available online: https://de.mathworks.com/matlabcentral/fileexchange/66258-circhist-circular-polar-angle-histogram (accessed on 23 June 2021).
- Berens, P. CircStat: A MATLAB Toolbox for Circular Statistics. J. Stat. Softw. 2009, 31, 1–21. [Google Scholar] [CrossRef]
- Crossland, M.D.; Culham, L.E.; Kabanarou, S.A.; Rubin, G.S. Preferred retinal locus development in patients with macular disease. Ophthalmology 2005, 112, 1579–1585. [Google Scholar] [CrossRef] [PubMed]
- Sunness, J.S.; Applegate, C.A.; Haselwood, D.; Rubin, G.S. Fixation patterns and reading rates in eyes with central scotomas from advanced atrophic age-related macular degeneration and Stargardt disease. Ophthalmology 1996, 103, 1458–1466. [Google Scholar] [CrossRef]
- Trauzettel-Klosinski, S.; Tornow, R.P. Fixation behavior and reading ability in macular scotoma. Assessed by Tuebingen manual perimetry and scanning laser ophthalmoscopy. Neuro Ophthalmol. 1996, 16, 241–253. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, D.C.; Schuchard, R.A. Preferred retinal loci relationship to macular scotomas in a low-vision population. Ophthalmology 1997, 104, 632–638. [Google Scholar] [CrossRef]
- Hibbard, P.B.; van Dam, L.C.; Scarfe, P. The implications of interpupillary distance variability for virtual reality. In Proceedings of the 2020 International Conference on 3D Immersion (IC3D), Brussels, Belgium, 15 December 2020; pp. 1–7. [Google Scholar]










Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sipatchin, A.; García García, M.; Wahl, S. Target Maintenance in Gaming via Saliency Augmentation: An Early-Stage Scotoma Simulation Study Using Virtual Reality (VR). Appl. Sci. 2021, 11, 7164. https://doi.org/10.3390/app11157164
Sipatchin A, García García M, Wahl S. Target Maintenance in Gaming via Saliency Augmentation: An Early-Stage Scotoma Simulation Study Using Virtual Reality (VR). Applied Sciences. 2021; 11(15):7164. https://doi.org/10.3390/app11157164
Chicago/Turabian StyleSipatchin, Alexandra, Miguel García García, and Siegfried Wahl. 2021. "Target Maintenance in Gaming via Saliency Augmentation: An Early-Stage Scotoma Simulation Study Using Virtual Reality (VR)" Applied Sciences 11, no. 15: 7164. https://doi.org/10.3390/app11157164
APA StyleSipatchin, A., García García, M., & Wahl, S. (2021). Target Maintenance in Gaming via Saliency Augmentation: An Early-Stage Scotoma Simulation Study Using Virtual Reality (VR). Applied Sciences, 11(15), 7164. https://doi.org/10.3390/app11157164