1. Introduction
Electrocardiography is the recording of the electrical activity originated by the heart in its duty cycle. The analysis of both rhythm and shape of the characteristic PQRST pattern can reveal altered conditions of the cardiac system. Software-based analysis of the electrocardiogram is a valuable tool, even more so with the increased presence of portable and wearable systems. The first and foremost step of ECG software analysis is heartbeat detection, specifically the ventricular systole which is represented by the combination of the Q, R, and S characteristic waves, the QRS complex. In the ECG analysis pipeline the accuracy of heartbeat detection determines the result quality of the following stages. Thus, this first step should be as accurate as possible. The main limiting factors in QRS detection accuracy are undesired noise, prominent T waves, and abnormal (non-sinus) beats.
Scientific literature on heartbeat detection is rich, and several approaches have been proposed over time. The most notable and referenced is Pan and Tompkins’ algorithm [
1], to which newer approaches are still compared to. Their work is based on differentiation, rectification and integration of the filtered ECG signal and a decision threshold calculated from the estimates of signal and noise levels. Several techniques have been applied to QRS detection [
2], like filter banks, neural networks, wavelets, and other means of signal decomposition. Recently, Phukpattaranont [
3] introduced quadratic filtering to QRS detection that attempts a thorough frequency characterization of the ECG. Wavelet-based processing has been a mainstay of ECG processing and heartbeat detection [
4,
5,
6,
7]. Pal et al. [
8] and Hossain et al. [
9] proposed methods based on empirical mode decomposition while Bashar et al. [
10] proposed an algorithm consisting in a set of rules applied on variable frequency complex demodulation, a time-frequency representation. Another time-frequency representation was applied in QRS detection by Zidelmal et al. [
11], the S-Transform. Manikandan et al. [
12] proposed a QRS peak search logic based on the Hilbert transform applied to the single-step derivative of frequency-filtered ECG. Gutiérrez-Rivas et al. [
13] used a finite state machine as a dynamic threshold for QRS complexes. Data-driven machine learning methods have also been applied in this field, notably convolutional neural networks [
14,
15]. Cai and Hu [
16] reported very high performances on two databases using convolutional neural networks.
Lately, researchers have published several QRS detection algorithms specifically designed for wearable applications [
17,
18,
19] due to the increasing interest towards ambulatory, daily monitoring [
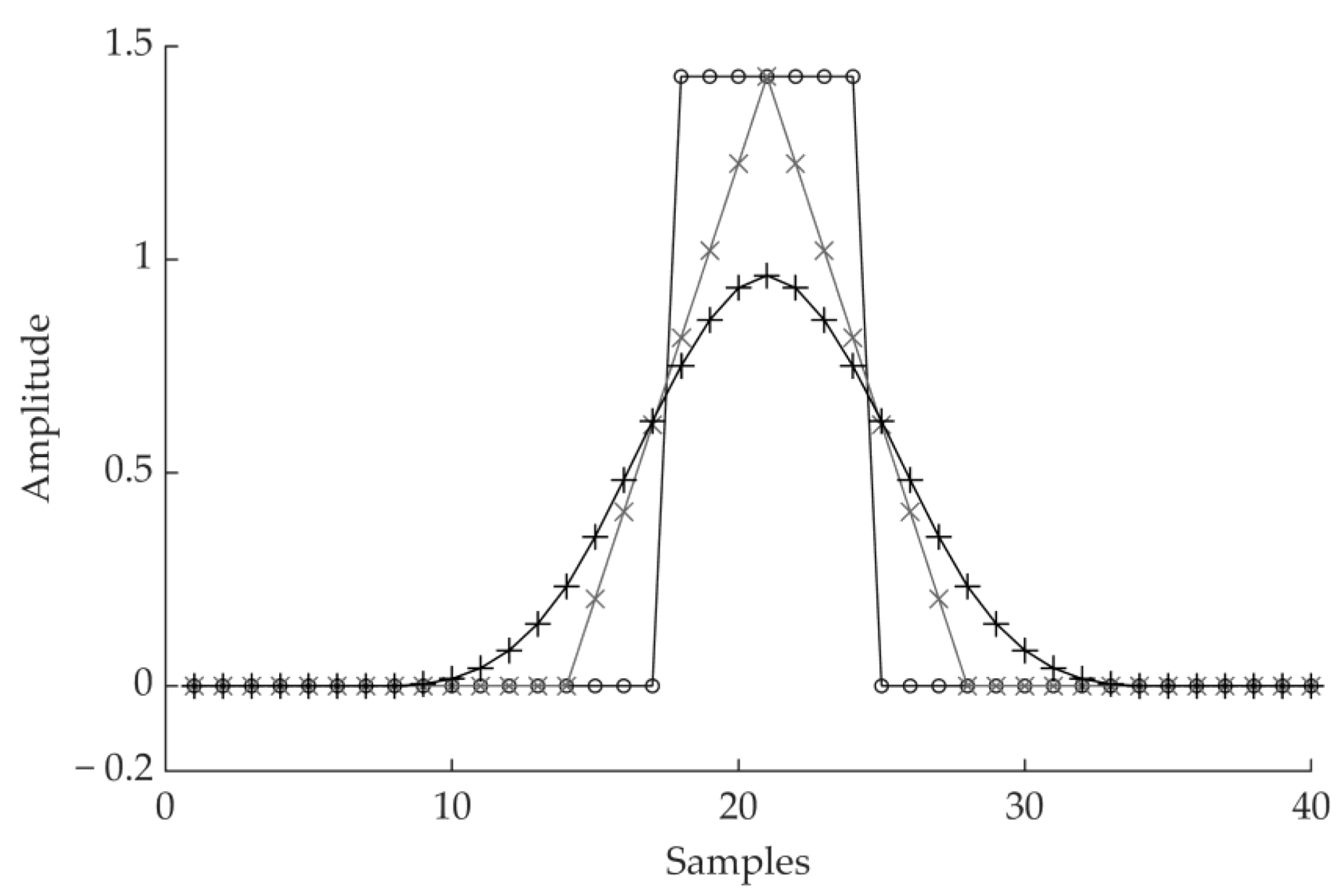
20]. Early detection of cardiac abnormalities may significantly improve the outcome of therapeutic efforts and the general quality of life of the patient. Often, these algorithms designed for wearable applications are based on established, low complexity ECG processing techniques as bandpass filters, single-step derivatives, signal integration, and adaptive amplitude and/or length thresholds. Derivative transforms are often used to enhance the QRS complex [
1,
21,
22], however in the discreet time domain there are several ways to compute the derivative [
2]. Single-step derivative transformations, as in s[n] − s[n − 1], are inherently susceptible to noise. Wider derivative transforms that take in account multiple samples reduce this tendency due to their band-pass behavior.
Complex approaches may afford the highest of performances, at the cost of increased computational load. When heartbeat detection is performed in battery-driven devices, the computational cost of the QRS detection algorithm should also be contained. One of the possible approaches for a lightweight QRS detection is a combination of moving average filters. Moving average filters require few operations and have been shown to be viable in ECG processing. Elgendi [
23] proposed an algorithm where two moving averages were used to determine blocks of interests. Knowledge-based thresholds on the duration of the blocks assessed the presence of the QRS complex. Considering 109,985 beats in the MIT-BIH Arrhythmia database [
24], Elgendi reported an F1 score for his work of 99.82%. Kim et al. [
25] proposed a method based on the energy of the signal and its rate of change. This was done by applying moving average filters to the squared and differentiated ECG filtered signals. QRS complexes were detected though a set of amplitude and duration thresholds in both energy level and energy rate of change. On the MIT-BIH Arrhythmia database the reported F1 score for this method was 99.91%, considering 109,494 beats. Szi-Wen Chen et al. [
4] used the moving average as a high-pass filter, combined it with wavelet denoising and then squared the high-pass filtered signal. QRS complexes were found with an adaptive threshold on the squared signal. This algorithm achieved an F1 score of 99.52% on the MIT-BIH Arrhythmia database, considering 102,654 beats. In Chiarugi et al. [
26], the ECG signal was filtered with a moving average, band-pass filter and then differentiated. A noise index automatically excluded noisy channels which would reduce detection accuracy. This algorithm achieved an F1 score of 99.78% on the MIT-BIH Arrhythmia database, considering 109,494 beats. All the aforementioned methods employ moving average filters in some form.
The performance scores of QRS detectors are customarily computed on standard databases, like the MIT-BIH Arrhythmia database. In theory, such practice should allow a straightforward comparison between different methods. Yet, different authors often adopt different inclusion criteria for the records in the databases. As an example, records 108 and 207 are sometimes excluded from the evaluation of the confusion matrix due to the abnormal shapes taken by the ECG signal [
2]. Moreover, different authors may use different acceptance window values for QRS complex positives. For these reasons, comparing published results could be incorrect, as they may have been calculated on different records and/or with a different acceptance window. On the other hand, some authors compare the algorithm they propose with pertinent literature by rewriting the corresponding routines. However, the description is often not complete enough and the re-written routines do not replicate the published performances. In this paper, we directly compare performances of different QRS detection methods computed using the same rules. To this end we considered the best performing QRS detection softwares we found available to our knowledge. We did not edit the code of the detection routines of other authors in any way.
Authors of QRS detection literature often report performances on a single database. This is the case for many of the works mentioned above. While the printed results may be excellent, the generalizability of the proposed methods to real world data remains indeterminate. For this reason, we included several databases in the evaluation of our work. When optimizing an algorithm on several data sources, overperforming on a single data source may considerably reduce the accuracy achieved on the other databases.
In this paper, we propose a fast, accurate approach to QRS detection based on combining simple unweighted moving averages. In particular, the basic elements of our ECG signal processing are cascades of moving averages (MACs). Our algorithm enhances the QRS complex by selecting a MAC from a pool of wide, derivative MACs that are inherently resistant to noise. We compare the performance of the QRS detector with those of three public algorithms, both in terms of accuracy and execution time, on the same calculator and the same initial conditions. The algorithm we propose aims to be an efficient, accurate, and generalizable method for QRS detection that improves on the concept of derivative transforms.
Our software was developed with MATLAB (The Mathworks Inc., Natick, MA, USA). A preliminary version of this work has been reported in [
27]. The algorithm has since then been further optimized, and one of the algorithms we considered for comparison has been changed to Kim’s detection approach, as it performed better. In this paper, we also elaborate with greater detail on the decision logic. Additionally, we report results on additional databases: the INCART, T Wave Alternans, and MIT-BIH Noise Stress Test databases.
3. Results
The detection performances are reported as F1 scores, which is a global metric of performance. F1 is the harmonic mean of Sensitivity (Se) and Positive Predictive Value (+P)
where TP are the true positives, FP are the false positives and FN are the false negatives of QRS detection.
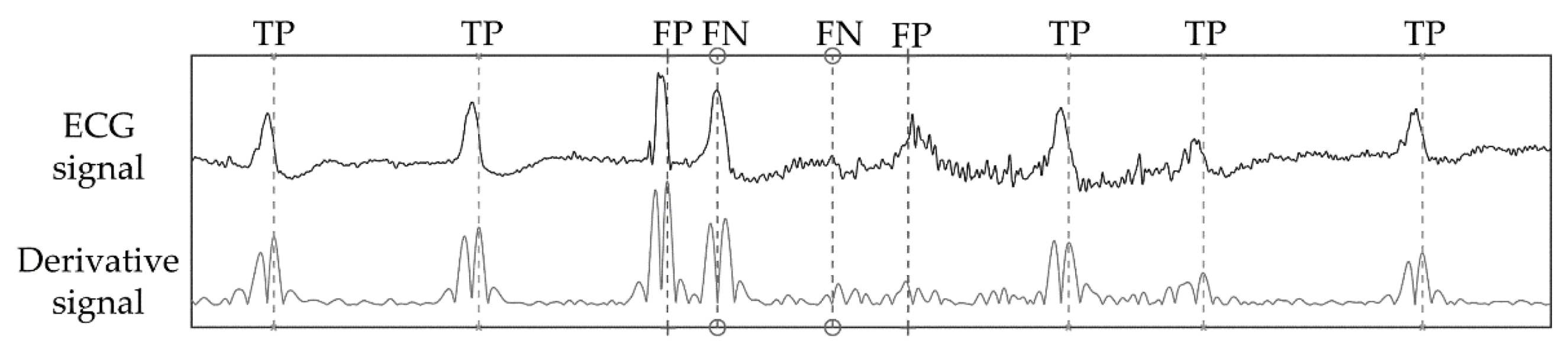
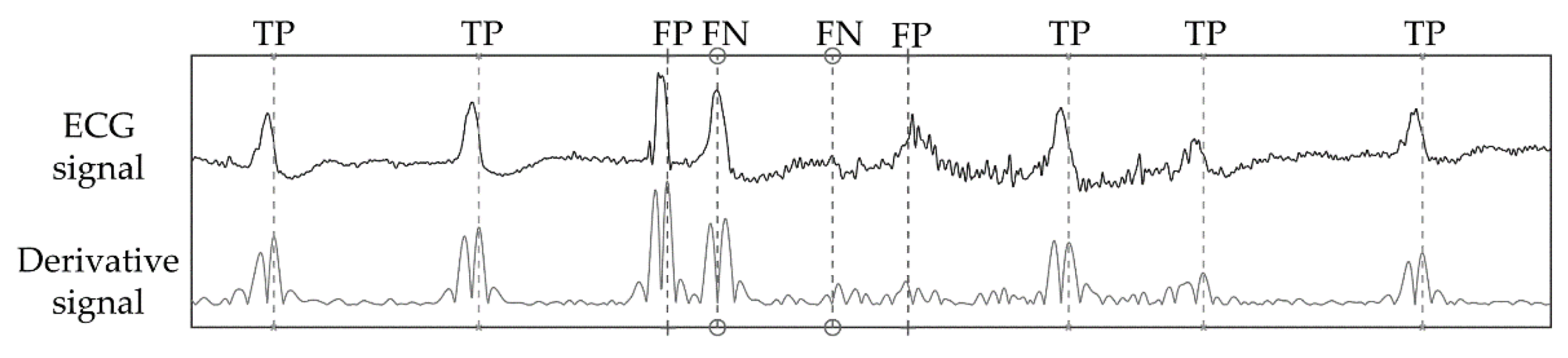
Figure 8 shows a strip of ECG signal, its respective absolute derivative, and detection markers for a strip of signal where true positives, false positives, and false negatives are registered. This is an example of a critical instance of signal. The first false positive of
Figure 8 is caused by an artifact that closely resembles a QRS complex. This misdetection causes the algorithm to enter its refractory period, thus the next true heartbeat is missed resulting in a false negative. The second false negative is a heartbeat with very low amplitude which is challenging to spot even by eye. As this beat is missed, the adaptive threshold decreases until the second false positive is detected, despite its relatively low amplitude. While these instances of error are not common, they represent the challenging aspects of QRS detection.
Heartbeats can be divided in two groups: (1) normal beats, which are originated from the dominant pacemaker, the sinus node and (2) ectopic beats, which are generated by secondary (ectopic) pacemakers. Ectopic beats are often premature and can be atrial, supraventricular or ventricular in origin. Sometimes, sinus beats and ventricular beats collide in a fusion beat. Ectopic beats are expression of cardiac automaticity disorders and can be the hallmark of life-threatening conditions like ventricular tachycardia. The shape of these heartbeats on the ECG can differ substantially from normal beats, and are thus more challenging to detect. This is especially true for beats of ventricular origin. Moreover, conduction disorders like bundle branch blocks can also significantly alter the shape of the normal, healthy ECG pattern. Since bundle branch blocks and ventricular beats are clinically relevant for diagnosis and therapy, we also report sensitivity to these abnormal beats (Se-A)
where
and
are true positive and false negatives of confusion matrix computed only by considering the heartbeats annotated as: bundle branch block, premature ventricular contractions, R-on-T premature ventricular contractions, fusion beats and ventricular escape beats.
Comparing algorithm results to annotations requires the definition of an acceptance window. This is a two-sided interval of appropriate size, centered around annotated beats. When a detected beat falls inside the acceptance window of an annotated beat it is considered a true positive. The following QRS detection results are obtained with a window of 300 ms (+/− 150 ms). This is the same window size used in Physionet’s bxb annotation comparator.
To evaluate the performances of the QRS detector we introduced we implemented and operated three publicly available detectors. They are Behar’s
jqrs [
33], Kim’s [
25] and Sedghamiz’s [
34] detectors. Behar’s QRS detector features a Mexican hat pre-processing filter, maximization of the signal’s energy in local windows, a fixed threshold and a backward search phase for missed heartbeats. In Kim’s approach the QRS detection is performed on the signal’s energy as well, by checking both the quantity and the dynamic of the QRS complex’ energy with adaptive thresholds. A valid heartbeat detection requires both criteria to be satisfied. Sedghamiz’s algorithm is structured on two adaptive thresholds that distinguish between signal and noise peaks, a decision logic that corrects multiple detections due to noise or T waves and a backward search procedure.
These algorithms were made available by their authors. We did not edit their code, but we did optimize their control parameter(s). Usually, each QRS detector is controlled by one or more control parameters that operate on the decision thresholds. The results we report were calculated using the control parameters that yielded the best performances for each algorithm.
Each of these programs was run in MATLAB, on the same calculator (2013 notebook with I7-dual core-cpu@2.00 GHz, 6 Gb RAM), with the same background conditions, at the same time of day, each one in succession.
Table 2 reports the gross and average F1 score achieved by the QRS detectors on all the considered. No record was excluded.
Table 3 shows the gross and average Se-A results. The T Wave Alternans database is not feature in this table, as it lacks annotations for non-sinus beats. The highest F1 and Se-A scores for each channel of each database and for the whole dataset are highlighted in bold.
Regarding the computational cost of the algorithms, in
Table 4 we show that our approach was faster than the other QRS detectors we considered. The comparison was made with the same background conditions. Each detector was run on all the databases we introduced, in succession. We report the average execution time. Our moving average-based approach took on average three times less to process an hour of ECG recording than Sedghamiz’s algorithm: 0.1137 s against 0.3388 s, effectively resulting in a reduction of 0.1137/0.3388 = 33.56% of required CPU time. The processing time of Kim’s algorithm was unexpectedly high.
4. Discussion
In this paper, we presented a QRS complex detection algorithm based on the knowledge of the electrocardiographic phenomena. The algorithm was evaluated on well-known databases and the performances we report are comparable to the best ones published in the literature. We considered several databases, in order to avoid overfitting on a single data source. It should be noted that some published approaches reach higher performances on specific databases, but caution should be exercised in direct comparison between published results. Different papers may adopt different subsets of records from the same databases and different acceptance windows. For this reason, the performances of the algorithm we proposed was compared to three available QRS detectors. As a performance metric, we computed the F1 scores as well as execution speed. We also reported sensitivity on ventricular beats and beats where bundle branch blocks were present, which we defined as Se-A, as they are more challenging to detect. As stated above, we chose to compare available QRS detectors instead of implementing other methods from literature, which was beyond the scope of this work. Additionally, rewriting a method is a developing effort itself. The resulting algorithm is not likely to reach the same accuracy and/or computational efficiency reported by the authors, as algorithms employ a set of specific parameters and rules that the authors have fine-tuned but do not end up in the final paper. We considered available QRS detectors for a direct comparison, so that results are reported for the same set of records, with the same acceptance rule for true positives. We chose the QRS detectors of Behar [
33], Sedghamiz [
34], and Kim [
25] as they were performing best among those we found available to our knowledge.
We evaluated the QRS detection algorithm on the MIT-BIH Arrhythmia, EU ST-T, INCART, MIT-BIH Noise Stress Test, T Wave Alternans, and QT databases. They are popular databases in the topic of automated analysis, and especially for heartbeat detection. Our algorithm outperformed the others, reaching 99.18% gross F1 and 94.81% gross Se-A. Despite this, Kim’s detector obtained a higher F1 score on the first channel of the MIT-BIH database. Detection accuracy for the second leads of the MITH.BIH Arrhythmia, Eu ST-T, and NST databases are lower for each algorithm. This happens as channel 2 is often chosen to highlight specific ECG features, like ST tract elevation, while the QRS complex is prominent in channel 1.
The Se-A score was lower than the overall sensitivity, as anticipated. This is due to the different shape of this subset of beats, as the slopes of the QRS waves are low and so are the corresponding derivatives. For our algorithm the worst-case scenario of Se-V is 86.16%, for the first channel of the INCART database. This particular result is, however, substantially different from the other Se-V scores we report on the other databases (
Table 4), or even the second channel of the same database. This may be caused by the annotation criteria on abnormal beats for channel 1 of the INCART database. For channel 2 of the INCART database and the other databases, sensitivity on abnormal beats lies between 94% and 99%. This means that up to 1 in every 20 abnormal beats is not detected correctly. Future work on this algorithm could address these instances of detection failure. Since identification of abnormal beats is one of the main goals in Holter exams and other lengthier ECG recordings, we feel that sensitivity on abnormal beats is a key characteristic of any QRS detector.
To highlight the light computational cost of the proposed QRS detection algorithm, we measured its execution time. On average, 0.1137 s were required to process an hour of ECG recording on our test machine, which is 33.56% of the time required by the quickest of the other programs. This result confirms the low processing power required by the algorithm we propose. While the detection accuracy of any method remains the fundamental performance metric, low execution time is nonetheless relevant for low-power devices such as wearable and portable devices.
In our algorithm, the derivative filter that maximizes the signal quality index is chosen on a selected 15 s signal interval at the beginning of the record. On longer records, e.g., 24-h-long Holter ECG, the derivative that maximizes the quality index could change throughout the record. Posture changes of the patient can alter the relative position of the heart and the electrodes, thus changing the amplitude and shape of the signal in each lead. To tackle this effect, the derivative filter selection could be repeated at regular intervals. As an alternative, the signal quality index of each derivative filter could be updated iteratively. This would remove the need to maximize the signal quality index multiple times. A derivative filter updating rule is a possible future development of this algorithm.
In the existing literature, the performance reported in some papers achieved higher scores than our algorithm. For example, Cai and Hu [
16] reported higher F1 scores on the first channel of the MIT-BIH Arrhythmia (99.95% vs. 99.84%), the MIT-BIH Noise Stress Test (99.53% vs. 91.71%) and QT (99.98% vs. 99.92%) databases using convolutional neural networks. Machine learning, and specifically deep learning, have been applied with great effect to many biomedical topics, and rightly so. Yet, these approaches come at a cost in both in terms of processing time and memory requirements. Moreover, machine learning algorithms crucially depend on the training data and must satisfy specific regulatory demands to be implemented in commercial devices. The scope of our algorithm is instead to propose an accurate algorithm with an emphasis on execution efficiency and a clear, explainable decision logic.
The literature on QRS detection is rich. Many approaches have been proposed over time, and results are often reported using heterogeneous criteria. Moreover, database annotations are another source of confusion in results comparison, as human observers occasionally disagree on annotation protocols. For this reason, the question of finding the ‘best’ QRS detection approach has no simple, unambiguous answer and comparison of published results may not be equitable.
Elgendi [
8] developed a QRS detection approach that aimed to be efficient and accurate, with moving averages, considering multiple databases, and is thus closer to the scope of our algorithm. Elgendi reported the performances for only the first channel of several databases, including the databases we considered. The comparison with our work is favorable for the MIT-BIH Arrhythmia (99.82% vs. 99.84%) and QT (99.81% vs. 99.92%) databases. Conversely, the performances of the algorithm we propose are lower on the INCART (98.05% vs. 96.51%), MIT-BIT Noise Stress Test (92.75% vs. 91.71%), and T Wave Alternans (99.00% vs. 98.20%) databases. A future comparison of execution time between these two algorithms would be of interest.
Kim [
25] reported performances as high as 99.91% F1 on the MIT-BIH database, which have been confirmed in our implementation of their code (99.88% F1) and are higher than our score (99.84% F1). Despite this, on all the other databases we included their algorithm reached lower performances. This may possibly be an effect of overfitting an algorithm on a small pool of data. For this reason, comparing implemented algorithms on multiple databases can offer greater insight on the characteristics of a QRS detection algorithm. This task, however, is easier when code is shared by its authors. When an algorithm must be re-written from scratch following the pertinent literature, its performances may vary significantly from the published ones.
The algorithm we present inherits the legacy left by the work of Carlo Marchesi and Alessandro Taddei [
35]. At the time, fast QRS detection was a necessity as calculators had limited processing power, which had to be optimized. Today, fast QRS detection remains a relevant topic for all applications involving battery-driven or portable devices.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}