
Healing Capacity of Bone Surrounding Biofilm-Infected and Non-Infected Gutta-Percha: A Study of Rat Calvaria



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
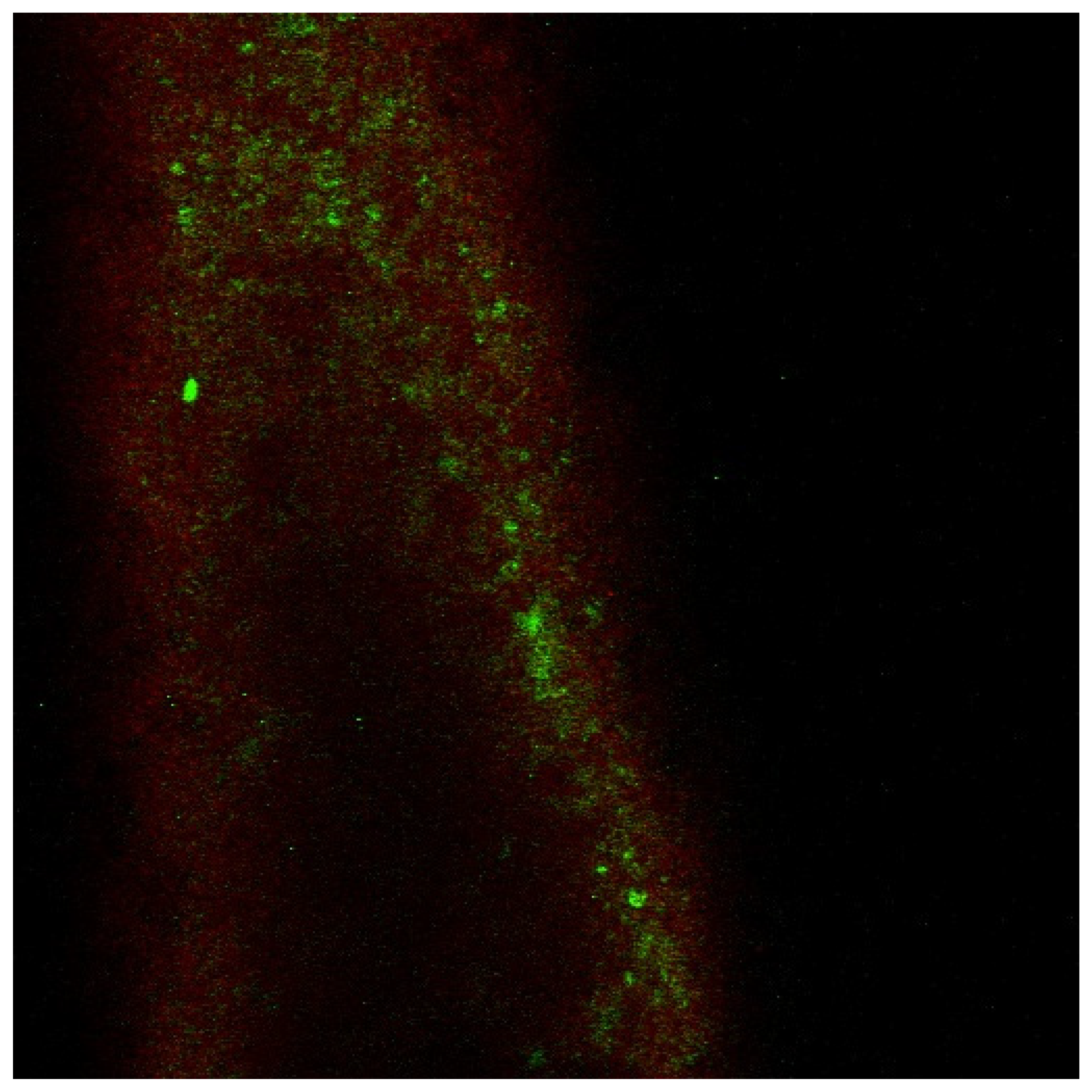
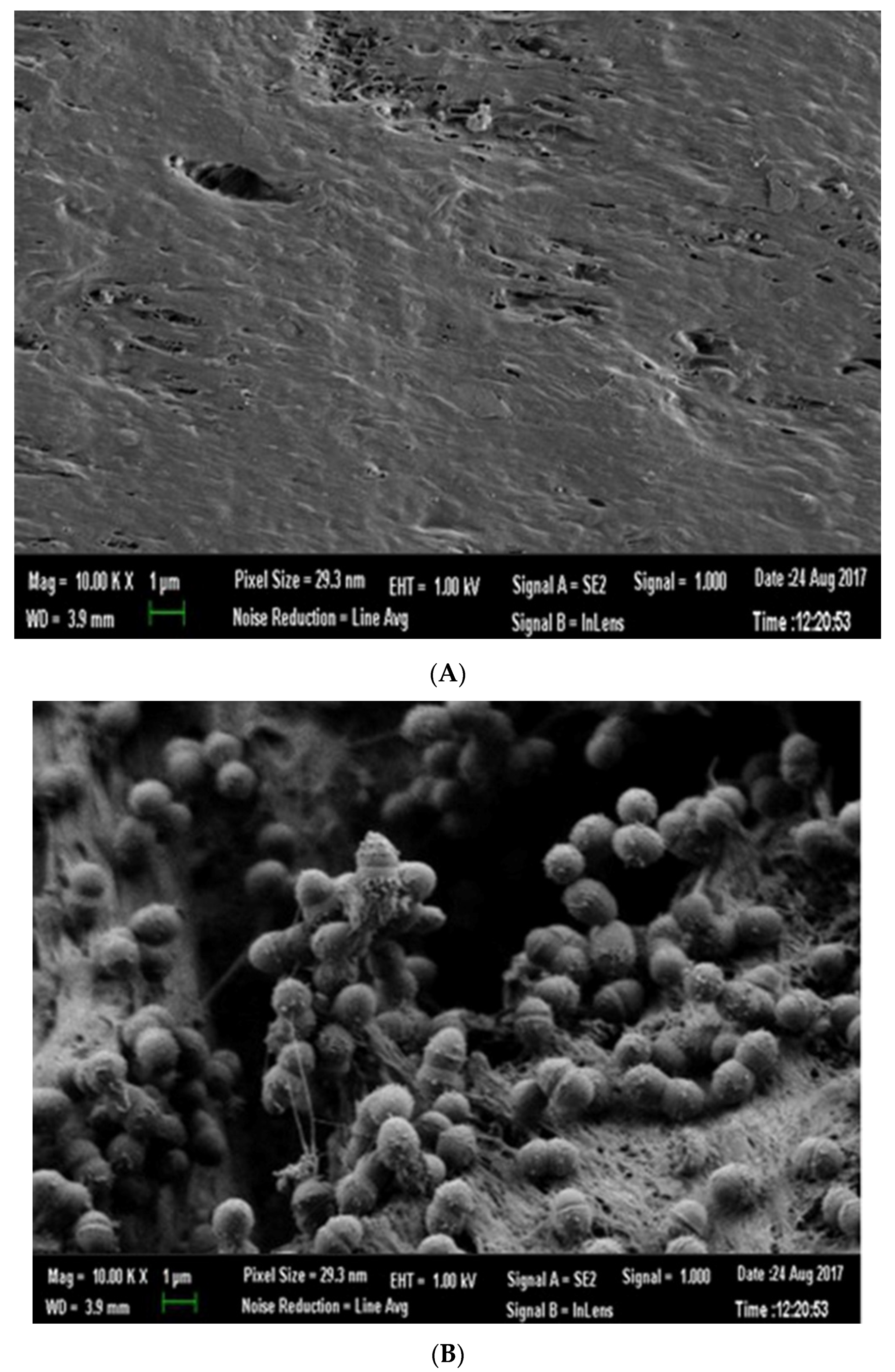
2.1. Biofilm Culture on GP
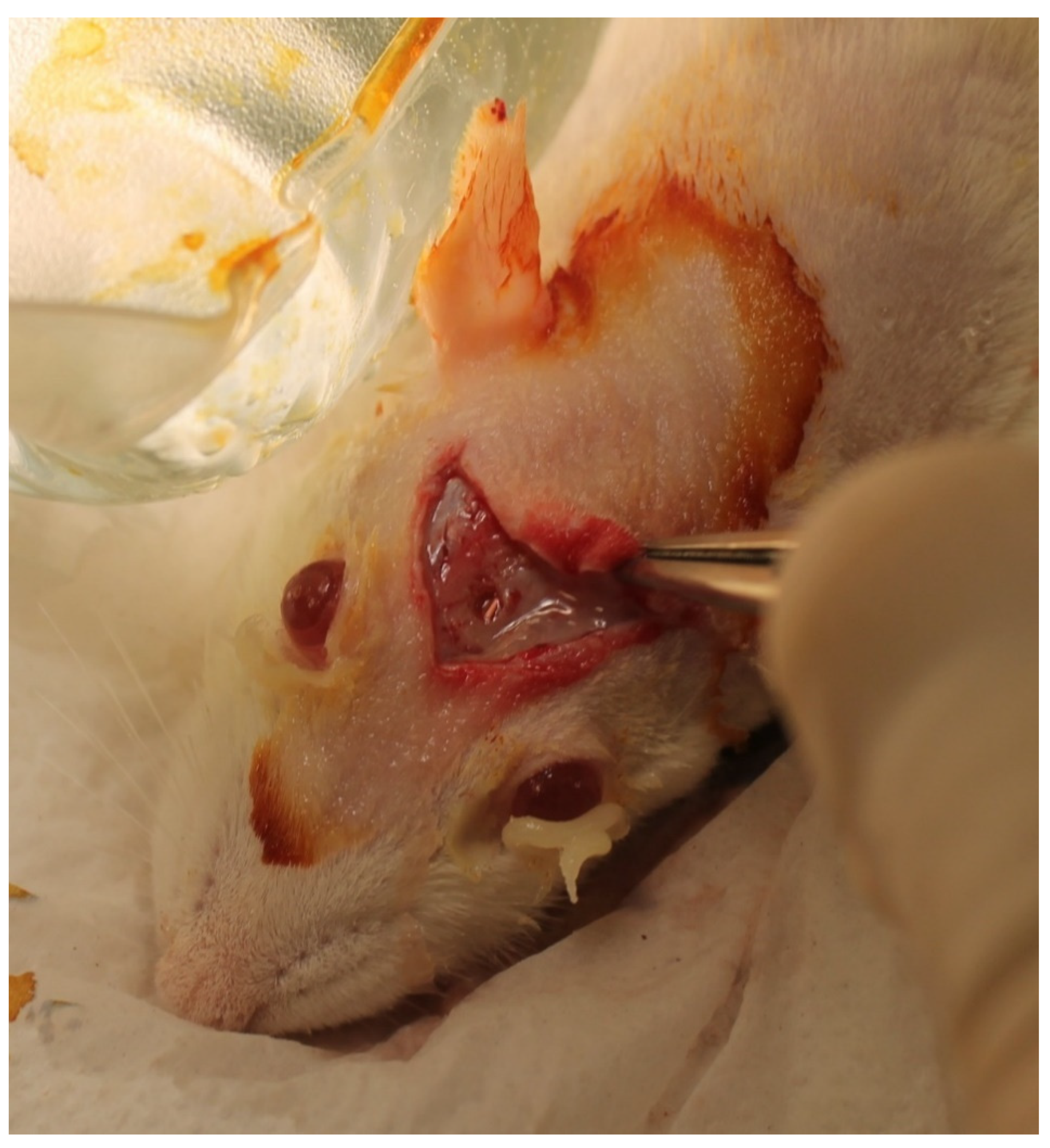
2.2. Animals and Surgery
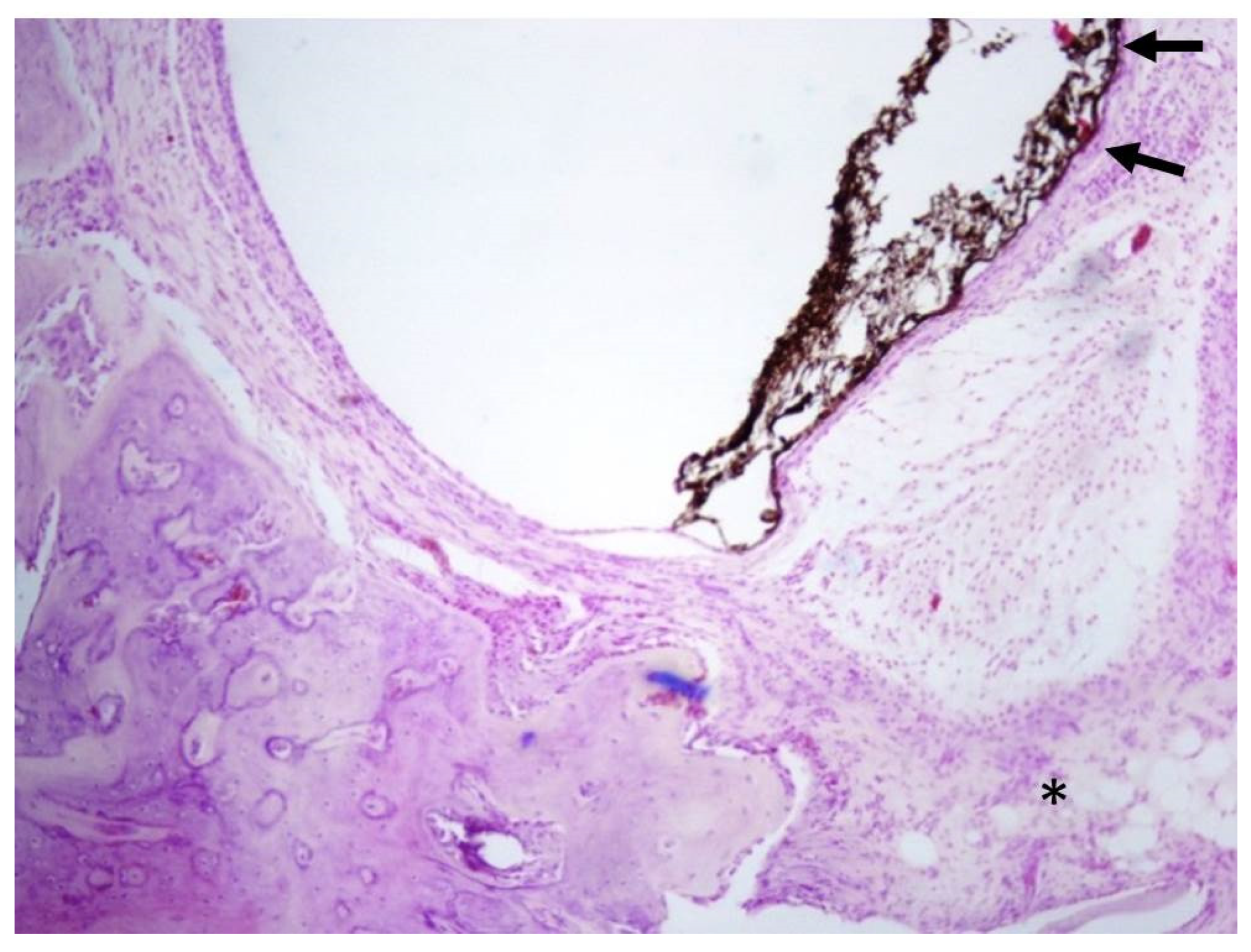
3. Results
3.1. Control (n = 4)
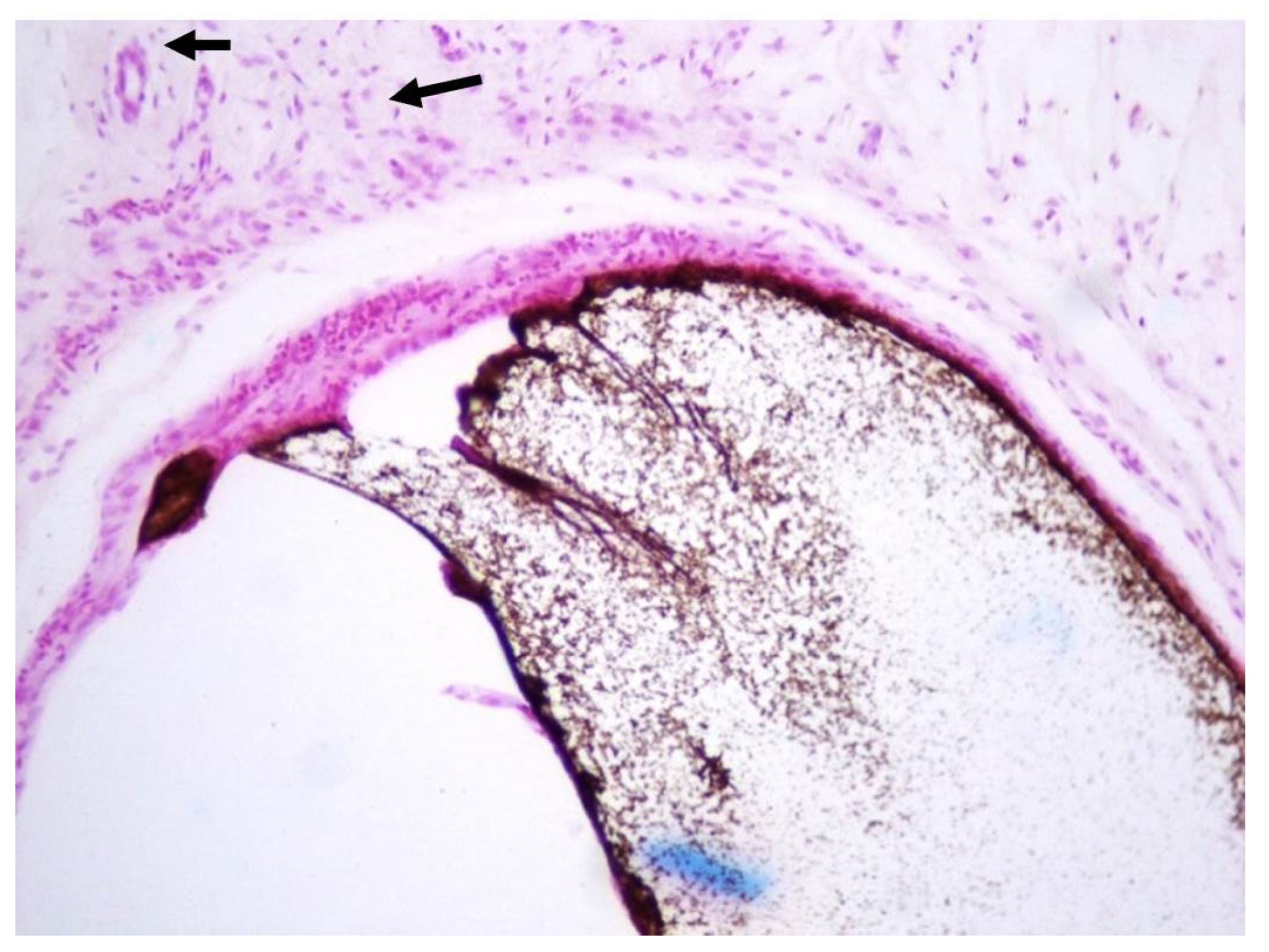
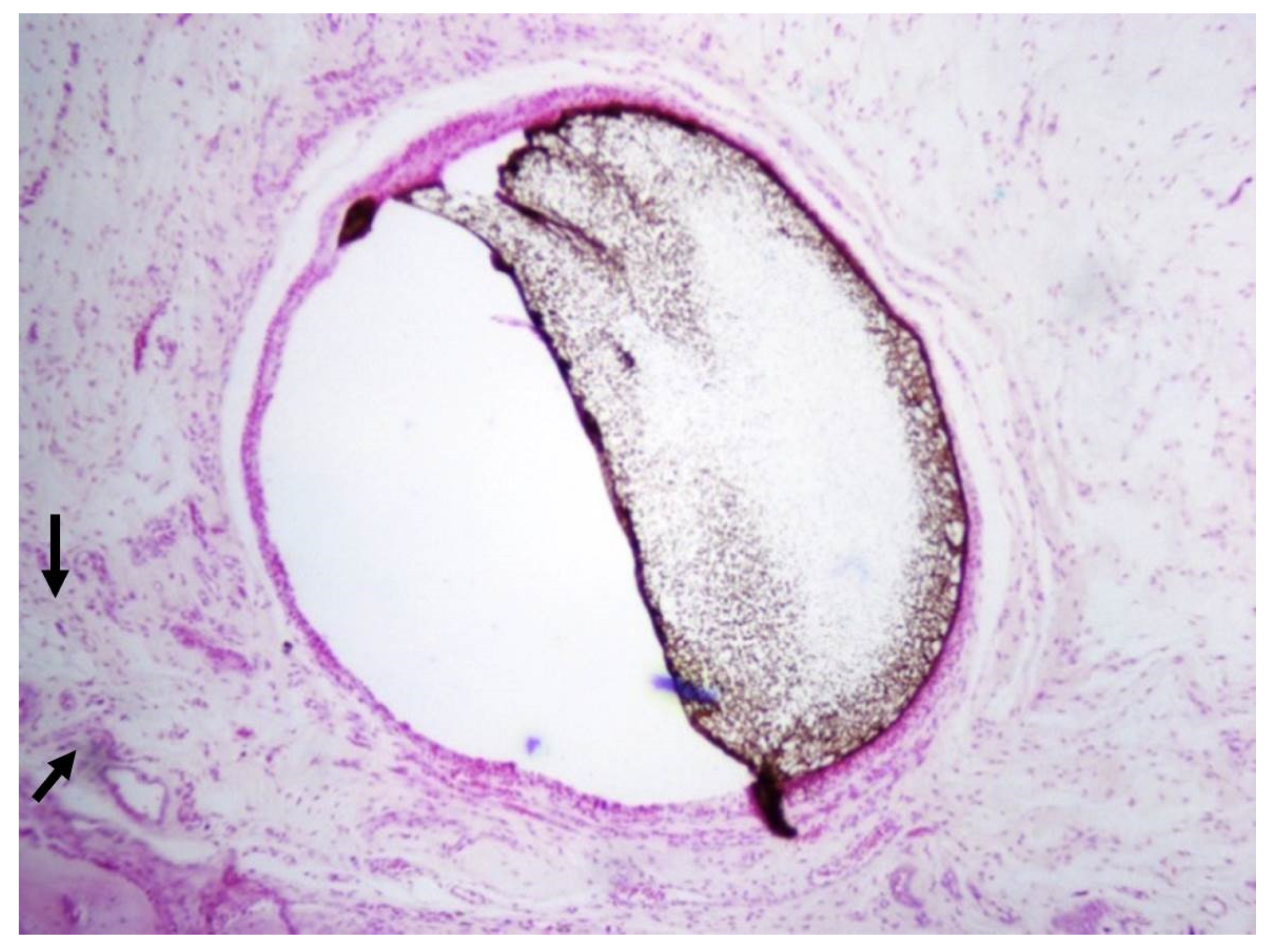
3.2. Non-Infected GP Points (n = 12)
3.3. Infected GP Points (n = 12)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johnson, W.; Kulild, J. Obturation of the Cleaned and Shaped Root Canal System; Elsevier: St. Louis, MO, USA, 2011; pp. 349–388. [Google Scholar]
- Ng, Y.L.; Mann, V.; Gulabivala, K. Outcome of secondary root canal treatment: A systematic review of the literature. Int. Endod. J. 2008, 41, 1026–1046. [Google Scholar] [CrossRef]
- Fristad, I.; Molven, O.; Halse, A. Nonsurgically retreated root filled teeth—Radiographic findings after 20–27 years. Int. Endod. J. 2004, 37, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Bergenholtz, G.; Lekholm, U.; Milthon, R.; Engstrom, B. Influence of apical overinstrumentation and overfilling on re-treated root canals. J. Endod. 1979, 5, 310–314. [Google Scholar] [CrossRef]
- Bergenholtz, G.; Lekholm, U.; Milthon, R.; Heden, G.; Odesjö, B.; Engström, B. Retreatment of endodontic fillings. Scand. J. Dent. Res. 1979, 87, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Van Nieuwenhuysen, J.P.; Aouar, M.; D’Hoore, W. Retreatment or radiographic monitoring in endodontics. Int. Endod. J. 1994, 27, 75–81. [Google Scholar] [CrossRef]
- Nair, P.N. On the causes of persistent apical periodontitis: A review. Int. Endod. J. 2006, 39, 249–281. [Google Scholar] [CrossRef]
- Haapasalo, M.; Shen, Y.A.; Ricucci, D. Reasons for persistent and emerging post-treatment endodontic disease: Reasons for persistent and emerging post-treatment endodontic disease. Endod. Top. 2008, 18, 31–50. [Google Scholar] [CrossRef]
- Ingle, J.I.; Bakland, L.K.; Baumgartner, J.C. Ingle’s Endodontics 6; BC Decker: Raleigh, NC, USA, 2008. [Google Scholar]
- Siqueira, J.F., Jr. Aetiology of root canal treatment failure: Why well-treated teeth can fail. Int. Endod. J. 2001, 34, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Friedman, S. Prognosis of initial endodontic therapy. Endod. Top. 2002, 2, 59–88. [Google Scholar] [CrossRef] [Green Version]
- Farzaneh, M.; Abitbol, S.; Lawrence, H.P.; Friedman, S. Treatment outcome in endodontics-the Toronto Study. Phase II: Initial treatment. J. Endod. 2004, 30, 302–309. [Google Scholar] [CrossRef]
- Yusuf, H. The significance of the presence of foreign material periapically as a cause of failure of root treatment. Oral Surg. Oral Med. Oral Pathol. 1982, 54, 566–574. [Google Scholar] [CrossRef]
- Senia, E.S.; Marraro, R.V.; Mitchell, J.L.; Lewis, A.G.; Thomas, L. Rapid sterilization of gutta-percha cones with 5.25% sodium hypochlorite. J. Endod. 1975, 1, 136–140. [Google Scholar] [CrossRef]
- Takemura, N.; Noiri, Y.; Ehara, A.; Kawahara, T.; Noguchi, N.; Ebisu, S. Single species biofilm-forming ability of root canal isolates on gutta-percha points. Eur. J. Oral Sci. 2004, 112, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Strathmann, M.; Wingender, J.; Flemming, H.C. Application of fluorescently labelled lectins for the visualization and biochemical characterization of polysaccharides in biofilms of Pseudomonas aeruginosa. J. Microbiol. Methods 2002, 50, 237–248. [Google Scholar] [CrossRef]
- George, S.; Basrani, B.; Kishen, A. Possibilities of gutta-percha-centered infection in endodontically treated teeth: An in vitro study. J. Endod. 2010, 36, 1241–1244. [Google Scholar] [CrossRef]
- Turnbull, R.S.; Freeman, E. Use of wounds in the parietal bone of the rat for evaluating bone marrow for grafting into periodontal defects. J. Periodontal. Res. 1974, 9, 39–43. [Google Scholar] [CrossRef]
- Ramachandran Nair, P.N. Light and electron microscopic studies of root canal flora and periapical lesions. J. Endod. 1987, 13, 29–39. [Google Scholar] [CrossRef]
- Moses, O.; Vitrial, D.; Aboodi, G.; Sculean, A.; Tal, H.; Kozlovsky, A.; Artzi, Z.; Weinreb, M.; Nemcovsky, C.E. Biodegradation of three different collagen membranes in the rat calvarium: A comparative study. J. Periodontol. 2008, 79, 905–911. [Google Scholar] [CrossRef]
- Kozlovsky, A.; Aboodi, G.; Moses, O.; Tal, H.; Artzi, Z.; Weinreb, M.; Nemcovsky, C.E. Bio-degradation of a resorbable collagen membrane (Bio-Gide) applied in a double-layer technique in rats. Clin. Oral Implant. Res. 2009, 20, 1116–1123. [Google Scholar] [CrossRef]
- Peters, O.A.; Peters, C.I. Chapter 9—Cleaning and Shaping of the Root Canal System. In Cohen’s Pathways of the Pulp, 10th ed.; Hargreaves, K.M., Cohen, S., Eds.; Mosby: St. Louis, Mo, USA, 2011; pp. 283–348. [Google Scholar]
- Nair, P.N.; Sjögren, U.; Krey, G.; Sundqvist, G. Therapy-resistant foreign body giant cell granuloma at the periapex of a root-filled human tooth. J. Endod. 1990, 16, 589–595. [Google Scholar] [CrossRef]
- Friedman, C.E.; Sandrik, J.L.; Heuer, M.A.; Rapp, G.W. Composition and physical properties of gutta-percha endodontic filling materials. J. Endod. 1977, 3, 304–308. [Google Scholar] [CrossRef]
- Wolfson, E.M.; Seltzer, S. Reaction of rat connective tissue to some gutta-percha formulations. J Endod. 1975, 1, 395–402. [Google Scholar] [CrossRef]
- Sjögren, U.; Sundqvist, G.; Nair, P.N. Tissue reaction to gutta-percha particles of various sizes when implanted subcutaneously in guinea pigs. Eur. J. Oral Sci. 1995, 103, 313–321. [Google Scholar] [CrossRef]
- Lin, L.M.; Huang, G.T.J. Chapter 14—Pathobiology of the Periapex. In Cohen’s Pathways of the Pulp, 10th ed.; Hargreaves, K.M., Cohen, S., Eds.; Mosby: St. Louis, Mo, USA, 2011; pp. 529–558. [Google Scholar]
- Metzger, Z.; Ben-Amar, A. Removal of overextended gutta-percha root canal fillings in endodontic failure cases. J. Endod. 1995, 21, 287–288. [Google Scholar] [CrossRef]
- Molander, A.; Reit, C.; Dahlén, G.; Kvist, T. Microbiological status of root-filled teeth with apical periodontitis. Int. Endod. J. 1998, 31, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Happonen, R.P. Periapical actinomycosis: A follow-up study of 16 surgically treated cases. Endod. Dent. Traumatol. 1986, 2, 205209. [Google Scholar] [CrossRef] [PubMed]
- Siquera, J.F., Jr. Periapical Actinomycosis and infection with Propionibacterium Propionicum. Endod. Top. 2003, 6, 78–95. [Google Scholar] [CrossRef]
- Lin, S.; Sela, G.; Sprecher, H. Periopathogenic bacteria in persistent periapical lesions: An in vivo prospective study. J. Periodontol. 2007, 78, 905–908. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moreinos, D.; Wigler, R.; Geffen, Y.; Akrish, S.; Lin, S. Healing Capacity of Bone Surrounding Biofilm-Infected and Non-Infected Gutta-Percha: A Study of Rat Calvaria. Appl. Sci. 2021, 11, 6710. https://doi.org/10.3390/app11156710
Moreinos D, Wigler R, Geffen Y, Akrish S, Lin S. Healing Capacity of Bone Surrounding Biofilm-Infected and Non-Infected Gutta-Percha: A Study of Rat Calvaria. Applied Sciences. 2021; 11(15):6710. https://doi.org/10.3390/app11156710
Chicago/Turabian StyleMoreinos, Daniel, Ronald Wigler, Yuval Geffen, Sharon Akrish, and Shaul Lin. 2021. "Healing Capacity of Bone Surrounding Biofilm-Infected and Non-Infected Gutta-Percha: A Study of Rat Calvaria" Applied Sciences 11, no. 15: 6710. https://doi.org/10.3390/app11156710
APA StyleMoreinos, D., Wigler, R., Geffen, Y., Akrish, S., & Lin, S. (2021). Healing Capacity of Bone Surrounding Biofilm-Infected and Non-Infected Gutta-Percha: A Study of Rat Calvaria. Applied Sciences, 11(15), 6710. https://doi.org/10.3390/app11156710