
Spontaneous Bone Regeneration after Enucleation of Mandibular Cysts: Retrospective Analysis of the Volumetric Increase with a Full-3D Measurement Protocol


 ,
,  ,
,  ,
, 

Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Manor, E.; Kachko, L.; Puterman, M.B.; Szabo, G.; Bodner, L. Cystic lesions of the jaws—A clinicopathological study of 322 cases and review of the literature. Int. J. Med. Sci. 2012, 9, 20–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peker, E.; Öğütlü, F.; Karaca, İ.R.; Gültekin, E.S.; Çakır, M. A 5 year retrospective study of biopsied jaw lesions with the assessment of concordance between clinical and histopathological diagnoses. J. Oral Maxillofac. Pathol. 2016, 20, 78–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolokythas, A.; Fernandes, R.P.; Pazoki, A.; Ord, R.A. Odontogenic keratocyst: To decompress or not to decompress? A comparative study of decompression and enucleation versus resection/peripheral ostectomy. J. Oral Maxillofac. Surg. 2007, 65, 640–644. [Google Scholar] [CrossRef] [PubMed]
- Nyimi, B.F.; Yifang, Z.; Liu, B. The Changing Landscape in Treatment of Cystic Lesions of the Jaws. J. Int. Soc. Prev. Community Dent. 2019, 9, 328–337. [Google Scholar] [PubMed]
- Asutay, F.; Atalay, Y.; Turamanlar, O.; Horata, E.; Burdurlu, M.Ç. Three-Dimensional Volumetric Assessment of the Effect of Decompression on Large Mandibular Odontogenic Cystic Lesions. J. Oral Maxillofac. Surg. 2016, 74, 1159–1166. [Google Scholar] [CrossRef] [PubMed]
- Marin, S.; Kirnbauer, B.; Rugani, P.; Mellacher, A.; Payer, M.; Jakse, N. The effectiveness of decompression as initial treatment for jaw cysts: A 10-year retrospective study. Med. Oral Patol. Oral Cir. Bucal. 2019, 24, e47–e52. [Google Scholar] [CrossRef] [PubMed]
- Jeong, H.G.; Hwang, J.J.; Lee, S.H.; Nam, W. Effect of decompression for patients with various jaw cysts based on a three-dimensional computed tomography analysis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2017, 123, 445–452. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.K.; Kim, J.W.; Lee, U.L.; Kim, J.W.; Lee, H. Risk Factor Analysis of Graft Failure With Concomitant Cyst Enucleation of the Jaw Bone: A Retrospective Multicenter Study. J. Oral Maxillofac. Surg. 2017, 75, 1668–1678. [Google Scholar] [CrossRef] [PubMed]
- Chacko, R.; Kumar, S.; Paul, A.; Arvind, A. Spontaneous Bone Regeneration after Enucleation of Large Jaw Cysts: A Digital Radiographic Analysis of 44 Consecutive Cases. J. Clin. Diagn. Res. 2015, 9, ZC84. [Google Scholar] [CrossRef] [PubMed]
- Kwon, Y.J.; Ko, K.S.; So, B.K.; Kim, D.H.; Jang, H.S.; Kim, S.H.; Lee, E.S.; Lim, H.K. Effect of Decompression on Jaw Cystic Lesions Based on Three-Dimensional Volumetric Analysis. Medicina (Kaunas). Medicina 2020, 56, 602. [Google Scholar] [CrossRef] [PubMed]
- Kauke, M.; Safi, A.F.; Grandoch, A.; Nickenig, H.J.; Zöller, J.; Kreppel, M. Image segmentation-based volume approximation-volume as a factor in the clinical management of osteolytic jaw lesions. Dentomaxillofac. Radiol. 2019, 48, 20180113. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Site | Patients |
|---|---|
| Ramus | 1 |
| Body | 5 |
| Angle/Ramus | 4 |
| Body/Ramus | 4 |
| Symphysis | 1 |
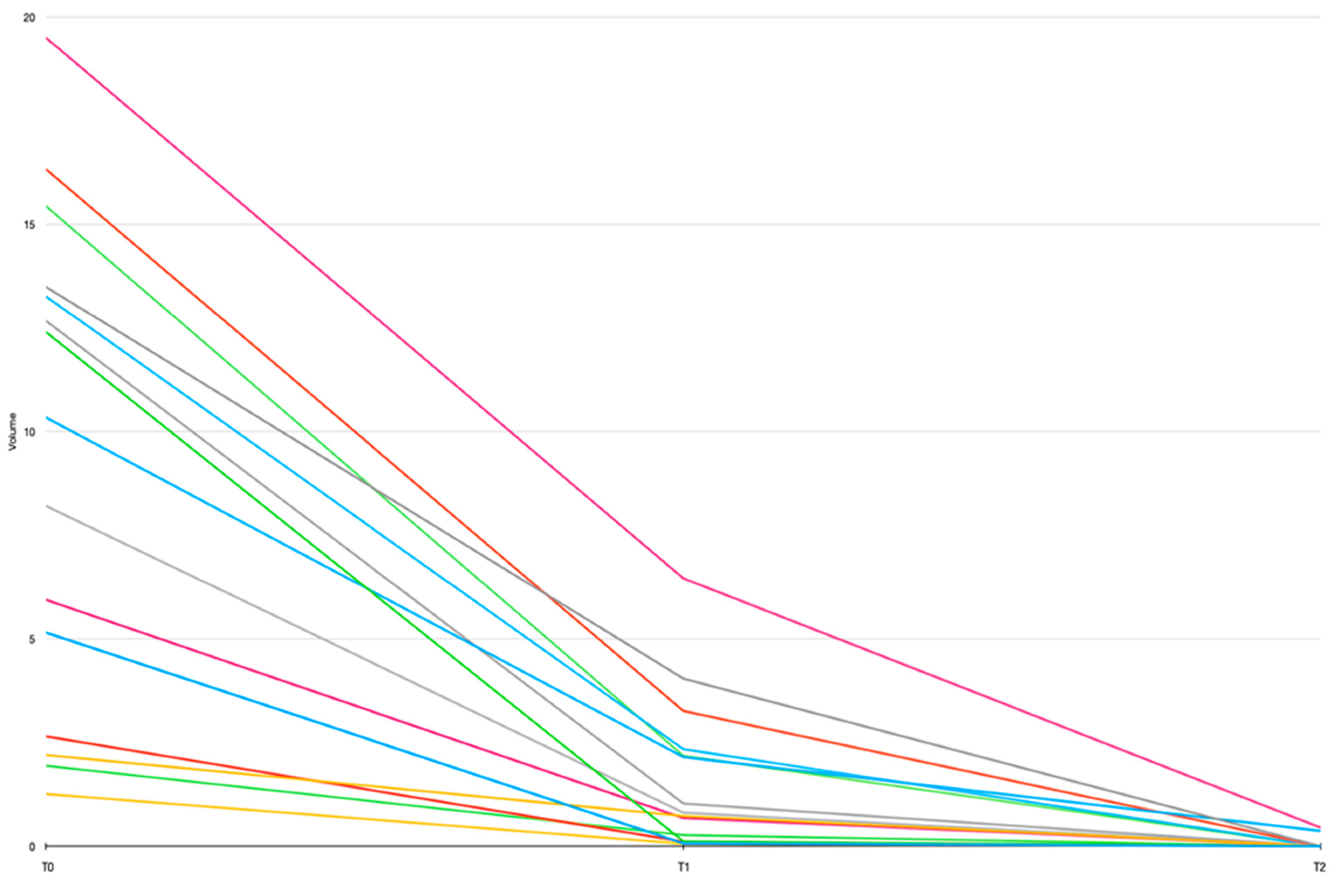
| # | Mandibular Site | T0 Volume (cc) | T1 Volume (cc) | T2 Volume (cc) | 6 Months Residual Volume (%) | 12 Months Residual Volume (%) |
|---|---|---|---|---|---|---|
| 1 | Angle-Ramus dx | 5.15 | 0.07 | 0 | 1.35 | 0 |
| 2 | Angle-Ramus sn | 12.4 | 0.12 | 0 | 0.97 | 0 |
| 3 | Angle-Ramus dx | 13.49 | 4.04 | 0 | 29.95 | 0 |
| 4 | Body sn | 2.20 | 0.73 | 0 | 33.18 | 0 |
| 5 | Body dx | 2.65 | 0.11 | 0 | 4.11 | 0 |
| 6 | Body dx | 5.94 | 0.68 | 0 | 11.45 | 0 |
| 7 | Symphysis | 10.34 | 2.15 | 0.37 | 20.7 | 3.57 |
| 8 | Body sn | 1.94 | 0.27 | 0 | 13.92 | 0 |
| 9 | Ramus sn | 12.67 | 1.03 | 0 | 8.13 | 0 |
| 10 | Body sn | 1.26 | 0.06 | 0 | 4.76 | 0 |
| 11 | Body-Ramus dx | 16.33 | 3.26 | 0 | 19.96 | 0 |
| 12 | Body-Ramus sn | 19.50 | 6.46 | 0.45 | 33.13 | 2.31 |
| 13 | Body-Ramus sx | 13.26 | 2.34 | 0 | 17.6 | 0 |
| 14 | Angle-Ramus dx | 15.44 | 2.18 | 0 | 14.1 | 0 |
| 15 | Body-Ramus sn | 8.21 | 0.81 | 0 | 9.87 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vitale, A.; Battaglia, S.; Crimi, S.; Ricceri, C.; Cervino, G.; Cicciù, M.; De Ponte, F.S.; Leonardi, R.M.; Bianchi, A. Spontaneous Bone Regeneration after Enucleation of Mandibular Cysts: Retrospective Analysis of the Volumetric Increase with a Full-3D Measurement Protocol. Appl. Sci. 2021, 11, 4731. https://doi.org/10.3390/app11114731
Vitale A, Battaglia S, Crimi S, Ricceri C, Cervino G, Cicciù M, De Ponte FS, Leonardi RM, Bianchi A. Spontaneous Bone Regeneration after Enucleation of Mandibular Cysts: Retrospective Analysis of the Volumetric Increase with a Full-3D Measurement Protocol. Applied Sciences. 2021; 11(11):4731. https://doi.org/10.3390/app11114731
Chicago/Turabian StyleVitale, Andrea, Salvatore Battaglia, Salvatore Crimi, Chiara Ricceri, Gabriele Cervino, Marco Cicciù, Francesco Saverio De Ponte, Rosalia Maria Leonardi, and Alberto Bianchi. 2021. "Spontaneous Bone Regeneration after Enucleation of Mandibular Cysts: Retrospective Analysis of the Volumetric Increase with a Full-3D Measurement Protocol" Applied Sciences 11, no. 11: 4731. https://doi.org/10.3390/app11114731
APA StyleVitale, A., Battaglia, S., Crimi, S., Ricceri, C., Cervino, G., Cicciù, M., De Ponte, F. S., Leonardi, R. M., & Bianchi, A. (2021). Spontaneous Bone Regeneration after Enucleation of Mandibular Cysts: Retrospective Analysis of the Volumetric Increase with a Full-3D Measurement Protocol. Applied Sciences, 11(11), 4731. https://doi.org/10.3390/app11114731