
Effect of Lactobacillus paracasei HII01 Supplementation on Total Cholesterol, and on the Parameters of Lipid and Carbohydrate Metabolism, Oxidative Stress, Inflammation and Digestion in Thai Hypercholesterolemic Subjects

 ,
, 
 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
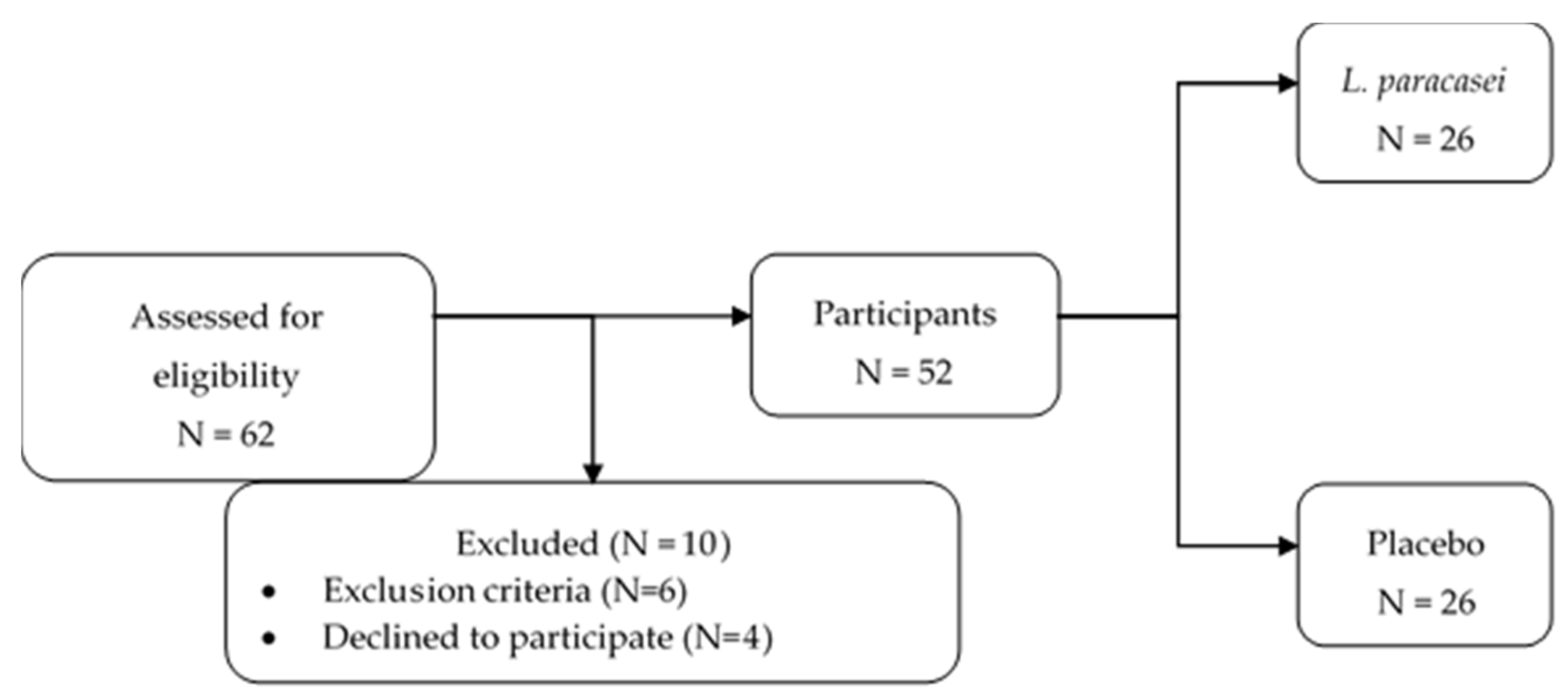
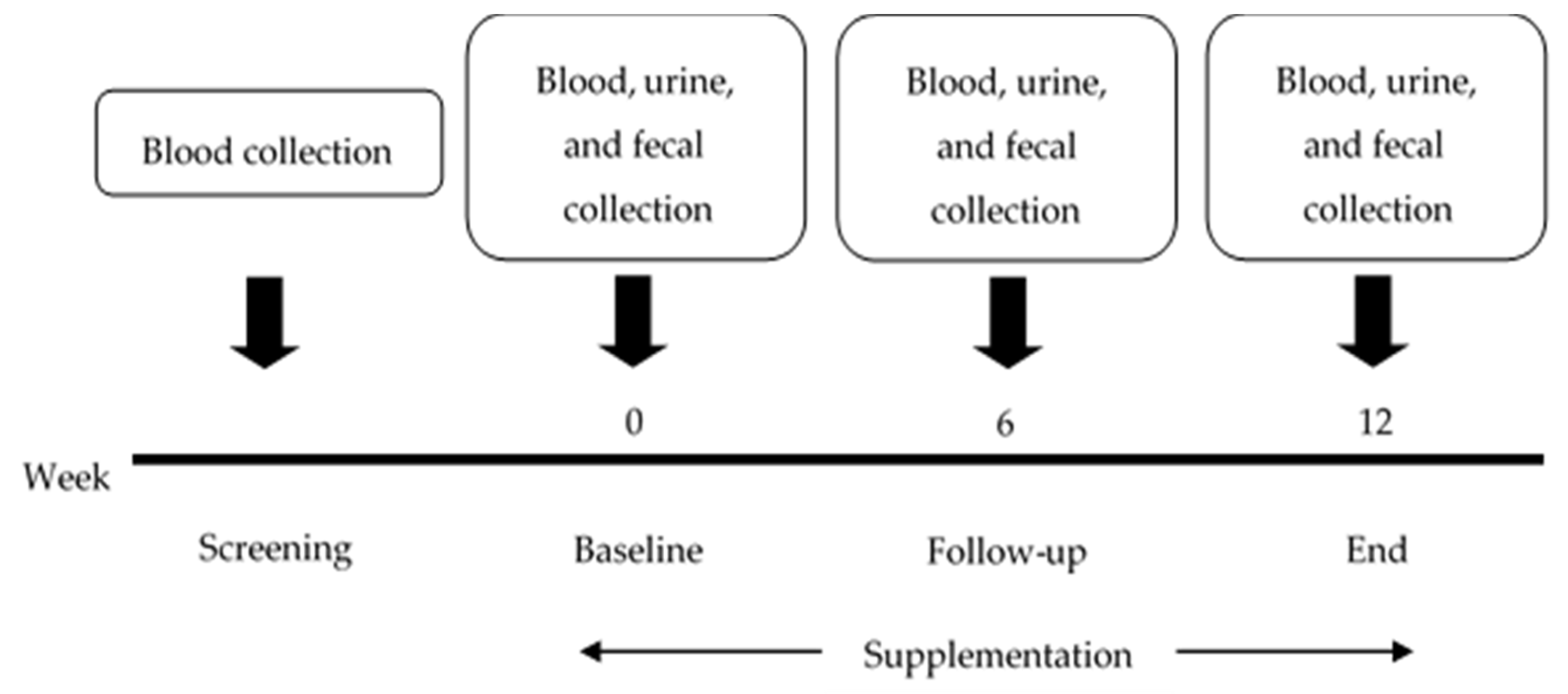
2.1. Study Design and Participants
2.2. Treatment
2.3. Assessments
2.3.1. Clinical Data
2.3.2. Laboratory Data
2.3.3. Statistical Analyses
3. Results
3.1. Participant Characteristics
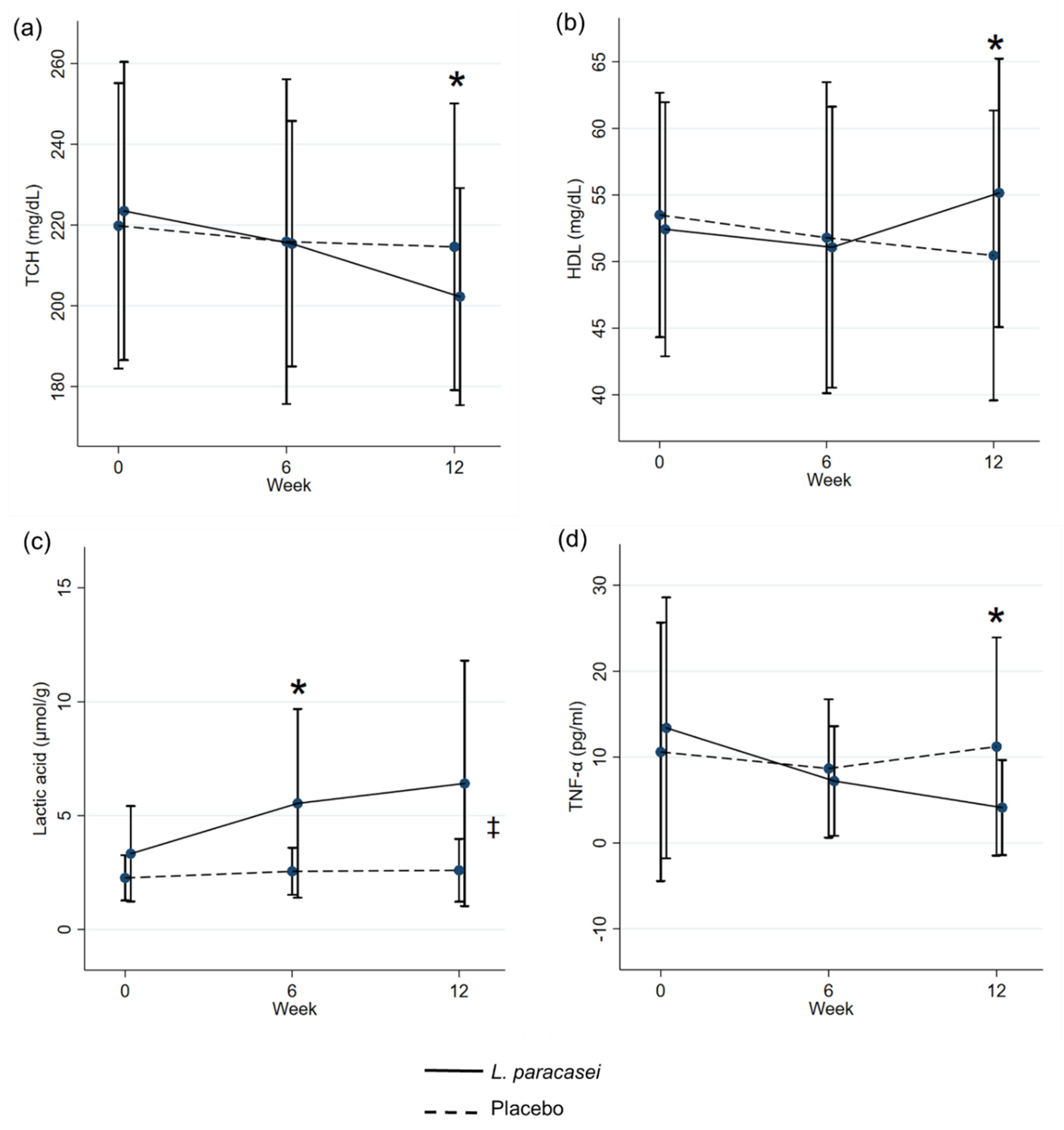
3.2. Effect of L. paracasei Supplementation on Cholesterol, Oxidative Stress, and Biomarkers at Baseline, 6 Weeks, and 12 Weeks
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yu, X.-H.; Zhang, D.-W.; Zheng, X.-L.; Tang, C.-K. Cholesterol transport system: An integrated cholesterol transport model involved in atherosclerosis. Prog. Lipid Res. 2019, 73, 65–91. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.; Nagpal, R.; Kumar, R.; Hemalatha, R.; Verma, V.; Kumar, A.; Yadav, H. Cholesterol-lowering probiotics as potential biotherapeutics for metabolic diseases. Exp. Diabetes Res. 2012, 2012, 902917. [Google Scholar] [CrossRef] [PubMed]
- Houston, M. The role of nutraceutical supplements in the treatment of dyslipidemia. J. Clin. Hypertens. (Greenwich) 2012, 14, 121–132. [Google Scholar] [CrossRef]
- El Mashad, G.M.; ElSayed, H.M.; Nosair, N.A. Effect of vitamin C supplementation on lipid profile, serum uric acid, and ascorbic acid in children on hemodialysis. Saudi J. Kidney Dis. Transplant. 2016, 27, 1148–1154. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Zhang, F.; Han, Y. Effect of probiotics on lipid profiles and blood pressure in patients with type 2 diabetes: A meta-analysis of RCTs. Medicine 2017, 96, e9166. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, T.; Naito, Y. What is oxidative stress? Jpn. Med. Assoc. J. 2002, 45, 271–276. [Google Scholar]
- Balkan, J.; Öztezcan, S.; Küçük, M.; Çevikbaş, U.; Koçak-Toker, N.; Uysal, M. The effect of betaine treatment on triglyceride levels and oxidative stress in the liver of ethanol-treated guinea pigs. Exp. Toxicol. Pathol. 2004, 55, 505–509. [Google Scholar] [CrossRef]
- Pereira DI, A.; Gibson, G.R. Effects of Consumption of Probiotics and Prebiotics on Serum Lipid Levels in Humans. Crit. Rev. Biochem. Mol. Biol. 2002, 37, 259–281. [Google Scholar] [CrossRef]
- Wang, Y.; Wu, Y.; Wang, Y.; Xu, H.; Mei, X.; Yu, D.; Li, W. Antioxidant Properties of Probiotic Bacteria. Nutrients 2017, 9, 521. [Google Scholar] [CrossRef] [PubMed]
- Kechagia, M.; Basoulis, D.; Konstantopoulou, S.; Dimitriadi, D.; Gyftopoulou, K.; Skarmoutsou, N.; Fakiri, E.M. Health benefits of probiotics: A review. ISRN Nutr. 2013, 2013, 481651. [Google Scholar] [CrossRef]
- George Kerry, R.; Patra, J.K.; Gouda, S.; Park, Y.; Shin, H.-S.; Das, G. Benefaction of probiotics for human health: A review. J. Food Drug Anal. 2018, 26, 927–939. [Google Scholar] [CrossRef] [PubMed]
- Lalitsuradej, E.; Sirilun, S.; Chaiyasut, C.; Sittiprapaporn, P. A preliminary study on effect of lactobacillus paracasei hii01 on cortisol in fatigue subjects. In Proceedings of the 16th International Conference on Electrical Engineering/Electronics, Computer, Telecommunications and Information Technology (ECTI-CON 2019), Pattaya, Thailand, 10–13 July 2019. [Google Scholar]
- National Heart, Lung, and Blood Institute (NHLBI). Available online: https://www.nhlbi.nih.gov/files/docs/guidelines/atglance.pdf (accessed on 15 September 2020).
- Sang Gil, L.; Taoran, W.; Terrence, M.V.; Patrice, H.; Dae-Ok, K.; Sung, I.K. Validation of Analytical Methods for Plasma Total Antioxidant Capacity by Comparing with Urinary 8-Isoprostane Level. J. Microbiol. Biotechnol. 2017, 27, 388–394. [Google Scholar] [CrossRef]
- Kambayashi, Y.; Binh, N.T.; WAsakura, H.; Hibino, Y.; Hitomi, Y.; Nakamura, H.; Ogino, K. Efficient assay for total antioxidant capacity in human plasma using a 96-well microplate. J. Clin. Biochem. Nutr. 2009, 44, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Zeb, A.; Ullah, F. A Simple Spectrophotometric Method for the Determination of Thiobarbituric Acid Reactive Substances in Fried Fast Foods. J. Anal. Methods Chem. 2016, 2016, 9412767. [Google Scholar] [CrossRef]
- Atasayar, S.; Orhan, H. Malondialdehyde quantification in blood plasma of tobacco smokers and non-smokers. FABAD J. Pharm. Sci. 2004, 29, 15–19. [Google Scholar]
- Rahman, I.; Kode, A.; Biswas, S.K. Assay for quantitative determination of glutathione and glutathione disulfide levels using enzymatic recycling method. Nat. Protoc. 2006, 1, 3159–3165. [Google Scholar] [CrossRef]
- Sequeira, I.R.; Lentle, R.G.; Kruger, M.C.; Hurst, R.D. Standardising the Lactulose Mannitol Test of Gut Permeability to Minimise Error and Promote Comparability. PLoS ONE 2014, 9, e99256. [Google Scholar] [CrossRef]
- Kotani, A.; Miyaguchi, Y.; Kohama, M.; Ohtsuka, T.; Shiratori, T.; Kusu, F. Determination of Short-chain Fatty Acids in Rat and Human Feces by High-Performance Liquid Chromatography with Electrochemical Detection. Anal. Sci. 2009, 25, 1007–1011. [Google Scholar] [CrossRef]
- Torii, T.; Kanemitsu, K.; Wada, T.; Itoh, S.; Kinugawa, K.; Hagiwara, A. Measurement of short-chain fatty acids in human faeces using high-performance liquid chromatography: Specimen stability. Ann. Clin. Biochem. 2010, 47, 447–452. [Google Scholar] [CrossRef]
- Xiao, J.Z.; Kondo, S.; Takahashi, N.; Miyaji, K.; Oshida, K.; Hiramatsu, A.; Hosono, A. Effects of Milk Products Fermented by Bifidobacterium longum on Blood Lipids in Rats and Healthy Adult Male Volunteers. J. Dairy Sci. 2003, 86, 2452–2461. [Google Scholar] [CrossRef]
- Agerholm-Larsen, L.; Bell, M.L.; Grunwald, G.K.; Astrup, A. The effect of a probiotic milk product on plasma cholesterol: A meta-analysis of short-term intervention studies. Eur. J. Clin. Nutr. 2000, 54, 856–860. [Google Scholar] [CrossRef]
- Rajkumar, H.; Mahmood, N.; Kumar, M.; Varikuti, S.R.; Challa, H.R.; Myakala, S.P. Effect of probiotic (VSL#3) and omega-3 on lipid profile, insulin sensitivity, inflammatory markers, and gut colonization in overweight adults: A randomized, controlled trial. Mediat. Inflamm. 2014, 2014, 348959. [Google Scholar] [CrossRef]
- Homayouni, A.; Payahoo, L.; Azizi, A. Effects of Probiotics on Lipid Profile: A Review. Am. J. Food Technol. 2012, 7, 251–265. [Google Scholar] [CrossRef]
- Ngamchuea, K.; Batchelor-McAuley, C.; Compton, R.G. Rapid Method for the Quantification of Reduced and Oxidized Glutathione in Human Plasma and Saliva. Anal. Chem. 2017, 89, 2901–2908. [Google Scholar] [CrossRef] [PubMed]
- Dayangaç, A.; Erdem, B. The Metabolic Relationships between Probiotics and Fatty Acids. Acta Phys. Pol. A 2017, 132, 816–818. [Google Scholar] [CrossRef]
- LeBlanc, J.G.; Chain, F.; Martín, R.; Bermúdez-Humarán, L.G.; Courau, S.; Langella, P. Beneficial effects on host energy metabolism of short-chain fatty acids and vitamins produced by commensal and probiotic bacteria. Microb. Cell Fact. 2017, 16, 79. [Google Scholar] [CrossRef]
- Granado-Serrano, A.B.; Martín-Garí, M.; Sánchez, V.; Riart Solans, M.; Berdún, R.; Ludwig, I.A.; Serrano, J.C.E. Faecal bacterial and short-chain fatty acids signature in hypercholesterolemia. Sci. Rep. 2019, 9, 1772. [Google Scholar] [CrossRef]
- Underwood, M.A.; Salzman, N.H.; Bennett, S.H.; Barman, M.; Mills, D.A.; Marcobal, A.; Sherman, M.P. A randomized placebo-controlled comparison of 2 prebiotic/probiotic combinations in preterm infants: Impact on weight gain, intestinal microbiota, and fecal short-chain fatty acids. J. Pediatr. Gastroenterol. Nutr. 2009, 48, 216–225. [Google Scholar] [CrossRef] [PubMed]
- Karamese, M.; Aydin, H.; Sengul, E.; Gelen, V.; Sevim, Ç.; Ustek, D.; Karakus, E. The Immunostimulatory Effect of Lactic Acid Bacteria in a Rat Model. Iran. J. Immunol. 2016, 13, 220–228. [Google Scholar]
- Meyer, A.; Elmadfa, I.; Herbacek, I.; Micksche, M. Probiotic, as well as conventional yogurt, can enhance the stimulated production of proinflammatory cytokines. J. Hum. Nutr. Diet. Off. J. Br. Diet. Assoc. 2007, 20, 590–598. [Google Scholar] [CrossRef]
- Rodes, L.; Khan, A.; Paul, A.; Coussa-Charley, M.; Marinescu, D.; Tomaro-Duchesneau, C.; Prakash, S. Effect of Probiotics Lactobacillus and Bifidobacterium on Gut-Derived Lipopolysaccharides and Inflammatory Cytokines: An In Vitro Study Using a Human Colonic Microbiota Model. J. Microbiol. Biotechnol. 2013, 23, 518–526. [Google Scholar] [CrossRef] [PubMed]
- Szulińska, M.; Łoniewski, I.; van Hemert, S.; Sobieska, M.; Bogdański, P. Dose-Dependent Effects of Multispecies Probiotic Supplementation on the Lipopolysaccharide (LPS) Level and Cardiometabolic Profile in Obese Postmenopausal Women: A 12-Week Randomized Clinical Trial. Nutrients 2018, 10, 773. [Google Scholar] [CrossRef] [PubMed]
- do Carmo, M.S.; itapary dos Santos, C.; Araújo, M.C.; Girón, J.A.; Fernandes, E.S.; Monteiro-Neto, V. Probiotics, mechanisms of action, and clinical perspectives for diarrhea management in children. Food Funct. 2018, 9, 5074–5095. [Google Scholar] [CrossRef]
- Hayati, M.; Herman, H.; Rezano, A. The effect of probiotic Lactobacillus casei supplementation on the secretory immunoglobulin A level in the saliva of wistar rats. Bali Med. J. 2018, 7, 727–731. [Google Scholar] [CrossRef]
- Wold, A.E. Immune effects of probiotics. Food Nutr. Res. 2001, 45, 76–85. [Google Scholar] [CrossRef]
- Ulluwishewa, D.; Anderson, R.C.; McNabb, W.C.; Moughan, P.J.; Wells, J.M.; Roy, N.C. Regulation of Tight Junction Permeability by Intestinal Bacteria and Dietary Components. J. Nutr. 2011, 141, 769–776. [Google Scholar] [CrossRef]
- Kelly, J.R.; Kennedy, P.J.; Cryan, J.F.; Dinan, T.G.; Clarke, G.; Hyland, N.P. Breaking down the barriers: The gut microbiome, intestinal permeability and stress-related psychiatric disorders. Front. Cell. Neurosci. 2015, 9, 392. [Google Scholar] [CrossRef]
- Liu, D.; Jiang, X.-Y.; Zhou, L.-S.; Song, J.-H.; Zhang, X. Effects of Probiotics on Intestinal Mucosa Barrier in Patients With Colorectal Cancer after Operation: Meta-Analysis of Randomized Controlled Trials. Medicine 2016, 95, e3342. [Google Scholar] [CrossRef]
- Van Hemert, S.; Verwer, J.; Schuetz, B. Clinical Studies Evaluating Effects of Probiotics on Parameters of Intestinal Barrier Function. Adv. Microbiol. 2013, 3, 212–221. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | L. paracasei Group (N = 26) | Placebo Group (N = 26) | p-Value |
|---|---|---|---|
| Male, n (%) | 9 (34.6) | 8 (30.8) | 1.000 |
| Female, n (%) | 17 (65.4) | 18 (69.2) | |
| Age (years) | 50.81 ± 3.01 | 54.15 ± 2.34 | 0.385 |
| Weight, kg | 68.63 ± 3.25 | 67.32 ± 2.88 | 0.764 |
| Height, cm | 158.54 ± 1.81 | 155.41 ± 1.57 | 0.196 |
| Body mass index, kg/m2 | 27.24 ± 5.76 | 27.43 ± 5.80 | 0.905 |
| Diabetes, n (%) | 2 (8.0) | 6 (23.08) | 0.248 |
| Smoking, n (%) | 1 (3.9) | 2 (7.7) | 1.000 |
| Alcohol drinking, n (%) | 6 (23.1) | 2 (7.7) | 0.248 |
| Parameters | L. paracasei (N = 26) | Placebo (N = 26) | ||||
|---|---|---|---|---|---|---|
| Baseline | 6 Weeks | 12 Weeks | Baseline | 6 Weeks | 12 Weeks | |
| Total cholesterol (mg/dL) | 223.46 ± 7.24 | 215.35 ± 5.97 | 202.23 ± 5.27 | 219.79 ± 7.21 | 215.88 ± 8.21 | 214.58 ± 7.25 |
| Triglycerides (mg/dL) | 143.04 ± 14.73 | 140.92 ± 12.89 | 137.62 ± 11.92 | 140.50 ± 14.05 | 143.54 ± 13.54 | 159.33 ± 14.51 |
| HDL-cholesterol (mg/dL) | 52.42 ± 1.87 | 51.08 ± 2.07 | 55.15 ± 1.98 | 53.50 ± 1.87 | 51.79 ± 2.38 | 50.46 ± 2.22 |
| LDL-cholesterol (mg/dL) | 141.80 ± 6.99 | 140.61 ± 8.34 | 130.69 ± 7.27 | 142.19 ± 7.17 | 136.55 ± 5.81 | 136.71 ± 6.64 |
| FBS (mg/dL) | 99.31 ± 7.50 | 98.46 ± 6.03 | 94.92 ± 5.04 | 95.21 ± 5.24 | 103.79 ± 4.68 | 101.92 ± 5.89 |
| TAC (µmol/mL) | 51.74 ± 5.42 | 56.20 ± 5.57 | 61.50 ± 6.69 | 48.69 ± 3.71 | 50.46 ± 4.44 | 46.92 ± 4.09 |
| MDA (µmol/mL) | 0.54 ± 0.02 a | 0.47 ± 0.02 ab | 0.41 ± 0.02 b | 0.58 ± 0.01 | 0.54 ± 0.02 | 0.51 ± 0.03 |
| GSH (µg/mL) | 125.42 ± 7.38 | 135.67 ± 7.21 | 150.34 ± 10.98 | 131.65 ± 5.51 | 132.18 ± 6.39 | 143.62 ± 8.64 |
| Lactic acid (µmol/g) | 3.33 ± 0.41 a | 5.54 ± 0.81 ab | 6.41 ± 1.06 b | 2.26 ± 0.20 | 2.55 ± 0.21 | 2.60 ± 0.28 |
| Acetic acid (µmol/g) | 3.48 ± 0.32 | 4.50 ± 0.62 | 6.38 ± 1.42 | 3.38 ± 0.21 | 3.61 ± 0.19 | 4.19 ± 0.29 |
| Butyric acid (µmol/g) | 5.21 ± 0.48 | 6.32 ± 0.79 | 7.59 ± 1.44 | 4.61 ± 0.64 | 4.68 ± 0.47 | 4.94 ± 0.66 |
| Propionic acid (µmol/g) | 16.55 ± 1.50 | 17.44 ± 1.22 | 18.22 ± 1.44 | 13.87 ± 1.29 | 12.66 ± 1.01 | 12.78 ± 1.16 |
| IL-10 (pg/mL) | 1.11 ± 0.28 a | 22.48 ± 8.83 ab | 48.40 ± 15.09 b | 3.17 ± 1.12 | 18.41 ± 8.30 | 25.13 ± 11.83 |
| IFN-γ (pg/mL) | 40.52 ± 8.54 a | 63.22 ± 10.90 a | 153.16 ± 29.92 b | 45.77 ± 25.17 | 67.11 ± 16.16 | 99.04 ± 41.95 |
| TNF-α (pg/mL) | 13.40 ± 5.06 | 7.22 ± 2.13 | 4.12 ± 1.84 | 10.60 ± 6.14 | 8.67 ± 3.29 | 11.22 ± 5.18 |
| LPS (pg/mL) | 122.95 ± 17.81 | 94.18 ± 12.36 | 76.86 ± 9.67 | 123.86 ± 17.38 | 108.12 ± 14.31 | 100.76 ± 13.53 |
| IgA (ng/mL) | 403.05 ± 41.52 | 464.24 ± 59.53 | 544.93 ± 80.76 | 406.92 ± 50.67 | 456.74 ± 58.31 | 478.36 ± 61.45 |
| L/M ratio | 0.16 ± 0.03 | 0.12 ± 0.02 | 0.09 ± 0.01 | 0.16 ± 0.02 | 0.13 ± 0.02 | 0.09 ± 0.01 |
| Parameters | Baseline—6 Weeks | p-Value | Baseline—12 Weeks | p-Value | 6 Weeks—12 Weeks | p-Value | |||
|---|---|---|---|---|---|---|---|---|---|
| L. paracasei (N = 26) | Placebo (N = 26) | L. paracasei (N = 26) | Placebo (N = 26) | L. paracasei (N = 26) | Placebo (N = 26) | ||||
| Total cholesterol (mg/dL) | −8.12 | −3.92 | 0.553 | −21.23 | −5.21 | 0.037 * | −13.12 | −1.29 | 0.047 * |
| Triglycerides (mg/dL) | −2.12 | 3.04 | 0.633 | −5.42 | 18.83 | 0.091 | −3.31 | 15.79 | 0.170 |
| HDL-cholesterol (mg/dL) | −1.35 | −1.71 | 0.851 | 2.73 | −3.04 | 0.001 * | 4.08 | −1.33 | 0.003 * |
| LDL-cholesterol (mg/dL) | −1.19 | −5.64 | 0.515 | −11.11 | −5.48 | 0.422 | −9.92 | 0.16 | 0.021 * |
| FBS (mg/dL) | −0.85 | 8.58 | 0.031 * | −4.38 | 6.71 | 0.046 * | −3.54 | −1.88 | 0.611 |
| TAC (µmol/mL) | 4.46 | 1.77 | 0.438 | 9.76 | −1.77 | 0.052 | 5.29 | −3.54 | 0.085 |
| MDA (µmol/mL) | −0.07 | −0.04 | 0.155 | −0.13 | −0.07 | 0.055 | −0.06 | −0.03 | 0.063 |
| GSH (µg/mL) | 10.25 | 0.53 | 0.372 | 24.92 | 11.97 | 0.417 | 14.67 | 11.44 | 0.739 |
| Lactic acid (µmol/g) | 2.21 | 0.29 | 0.009 * | 3.09 | 0.33 | 0.009 * | 0.88 | 0.04 | 0.013 * |
| Acetic acid (µmol/g) | 1.04 | 0.23 | 0.152 | 2.92 | 0.81 | 0.153 | 1.88 | 0.58 | 0.158 |
| Butyric acid (µmol/g) | 1.11 | 0.07 | 0.173 | 2.39 | 0.32 | 0.228 | 1.28 | 0.25 | 0.299 |
| Propionic acid (µmol/g) | 0.89 | −1.21 | 0.202 | 1.67 | −1.09 | 0.244 | 0.77 | 0.12 | 0.399 |
| IL-10 (pg/mL) | 21.37 | 15.24 | 0.630 | 38.04 | 21.96 | 0.434 | 16.67 | 6.72 | 0.232 |
| IFN-γ (pg/mL) | 22.69 | 21.34 | 0.947 | 112.64 | 53.27 | 0.292 | 89.95 | 31.92 | 0.184 |
| TNF-α (pg/mL) | −6.19 | −1.93 | 0.402 | −9.28 | 0.62 | 0.082 | −3.10 | 2.55 | 0.014 * |
| LPS (pg/mL) | −28.77 | −15.74 | 0.169 | −46.09 | −23.10 | 0.126 | −17.32 | −7.36 | 0.092 |
| IgA (ng/mL) | 61.18 | 49.82 | 0.731 | 141.88 | 71.44 | 0.241 | 80.69 | 21.62 | 0.069 |
| L/M ratio | −0.04 | −0.03 | 0.745 | −0.07 | −0.06 | 0.745 | −0.04 | −0.03 | 0.745 |
| Parameter | Coefficient | 95% CI | p-Value |
|---|---|---|---|
| Total cholesterol (mg/dL) | −6.18 | (−21.60 to 9.23) | 0.422 |
| Triglycerides (mg/dL) | −10.02 | (−32.82 to 12.77) | 0.380 |
| HDL-cholesterol (mg/dL) | −0.98 | (−5.39 to 3.42) | 0.655 |
| LDL-cholesterol (mg/dL) | 3.15 | (−11.99 to 18.28) | 0.677 |
| FBS (mg/dL) | −5.78 | (−13.82 to 2.25) | 0.154 |
| TAC (µmol/mL) | 3.77 | (−3.91 to 11.44) | 0.327 |
| MDA (µmol/mL) | −0.03 | (−0.08 to 0.02) | 0.295 |
| GSH (µg/mL) | 8.98 | (−11.18 to 29.13) | 0.373 |
| Lactic acid (µmol/g) | 1.23 | (−0.35 to 2.81) | 0.124 |
| Acetic acid (µmol/g) | 0.28 | (−0.90 to 1.47) | 0.629 |
| Butyric acid (µmol/g) | 0.69 | (−0.89 to 2.27) | 0.384 |
| Propionic acid (µmol/g) | 3.85 | (1.07 to 6.63) | 0.008 * |
| IL-10 (pg/mL) | 30.98 | (−104.94 to 166.89) | 0.212 |
| IFN-γ (pg/mL) | −0.43 | (−43.51 to 42.66) | 0.983 |
| TNF-α (pg/mL) | −2.68 | (−9.44 to 4.08) | 0.380 |
| LPS (pg/mL) | −16.49 | (−29.63 to −3.36) | 0.015 * |
| IgA (ng/mL) | 6.66 | (−59.90 to 73.22) | 0.841 |
| L/M ratio | −0.01 | (−0.02 to 0.01) | 0.519 |
| Parameter | Coefficient | 95% CI | p-Value |
|---|---|---|---|
| Total cholesterol (mg/dL) | −14.41 | (−28.52 to −0.31) | 0.045 * |
| Triglycerides (mg/dL) | −28.19 | (−54.04 to −2.34) | 0.033 * |
| HDL-cholesterol (mg/dL) | 4.45 | (0.86 to 8.05) | 0.016 * |
| LDL-cholesterol (mg/dL) | −7.14 | (−22.44 to 8.17) | 0.352 |
| FBS (mg/dL) | −4.30 | (−13.89 to 5.29) | 0.370 |
| TAC (µmol/mL) | 14.39 | (2.04 to 26.75) | 0.024 * |
| MDA (µmol/mL) | −0.05 | (−0.12 to 0.02) | 0.142 |
| GSH (µg/mL) | 16.27 | (−14.41 to 46.94) | 0.290 |
| Lactic acid (µmol/g) | 1.83 | (−0.44 to 4.09) | 0.111 |
| Acetic acid (µmol/g) | 0.77 | (−2.33 to 3.86) | 0.619 |
| Butyric acid (µmol/g) | 1.53 | (−1.90 to 4.96) | 0.372 |
| Propionic acid (µmol/g) | 5.45 | (1.41 to 9.49) | 0.010 * |
| IL-10 (pg/mL) | 46.09 | (−242.48 to 334.65) | 0.291 |
| IFN-γ (pg/mL) | 33.12 | (−86.70 to 152.94) | 0.565 |
| TNF-α (pg/mL) | −10.94 | (−21.17 to −0.71) | 0.039 * |
| LPS (pg/mL) | −28.32 | (−48.68 to −7.95) | 0.008 * |
| IgA (ng/mL) | 42.31 | (−55.24 to 139.87) | 0.386 |
| L/M ratio | −0.01 | (−0.04 to 0.02) | 0.519 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chaiyasut, C.; Tirawat, Y.; Sivamaruthi, B.S.; Kesika, P.; Thangaleela, S.; Khongtan, S.; Khampithum, N.; Peerajan, S.; Chaiyasut, K.; Sirilun, S.; et al. Effect of Lactobacillus paracasei HII01 Supplementation on Total Cholesterol, and on the Parameters of Lipid and Carbohydrate Metabolism, Oxidative Stress, Inflammation and Digestion in Thai Hypercholesterolemic Subjects. Appl. Sci. 2021, 11, 4333. https://doi.org/10.3390/app11104333
Chaiyasut C, Tirawat Y, Sivamaruthi BS, Kesika P, Thangaleela S, Khongtan S, Khampithum N, Peerajan S, Chaiyasut K, Sirilun S, et al. Effect of Lactobacillus paracasei HII01 Supplementation on Total Cholesterol, and on the Parameters of Lipid and Carbohydrate Metabolism, Oxidative Stress, Inflammation and Digestion in Thai Hypercholesterolemic Subjects. Applied Sciences. 2021; 11(10):4333. https://doi.org/10.3390/app11104333
Chicago/Turabian StyleChaiyasut, Chaiyavat, Yaowalak Tirawat, Bhagavathi Sundaram Sivamaruthi, Periyanaina Kesika, Subramanian Thangaleela, Suchanat Khongtan, Nanticha Khampithum, Sartjin Peerajan, Khontaros Chaiyasut, Sasithorn Sirilun, and et al. 2021. "Effect of Lactobacillus paracasei HII01 Supplementation on Total Cholesterol, and on the Parameters of Lipid and Carbohydrate Metabolism, Oxidative Stress, Inflammation and Digestion in Thai Hypercholesterolemic Subjects" Applied Sciences 11, no. 10: 4333. https://doi.org/10.3390/app11104333
APA StyleChaiyasut, C., Tirawat, Y., Sivamaruthi, B. S., Kesika, P., Thangaleela, S., Khongtan, S., Khampithum, N., Peerajan, S., Chaiyasut, K., Sirilun, S., & Sittiprapaporn, P. (2021). Effect of Lactobacillus paracasei HII01 Supplementation on Total Cholesterol, and on the Parameters of Lipid and Carbohydrate Metabolism, Oxidative Stress, Inflammation and Digestion in Thai Hypercholesterolemic Subjects. Applied Sciences, 11(10), 4333. https://doi.org/10.3390/app11104333