Soft Tissue Evaluation of an Immediate Esthetic Zone Single Implant with a Stereolithographic Guide Using 3D Reconstruction and a CAD/CAM Customized Titanium Anatomic Abutment

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Materials
- At least 18 years old
- Both adjacent teeth are intact
- Followed-up for at least 1 year after final restoration
2.2. Exclusion Criteria Were as Listed Below
- Systemic bone disease
- Recent orthodontic treatment
- Presence of an acute infection around the tooth
- Less than one full year of follow-up after definitive restoration
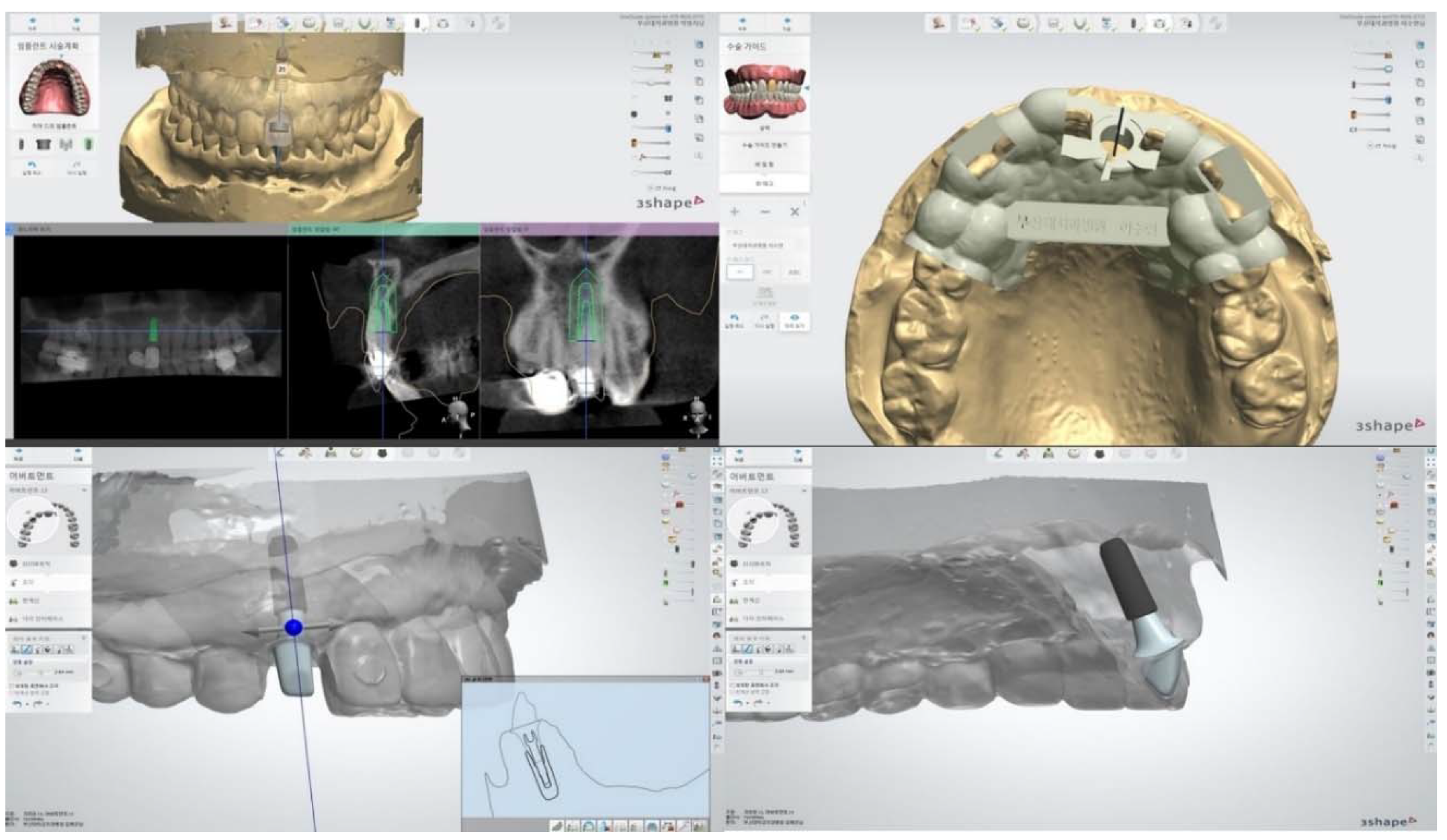
2.3. Preparation for Treatment
2.4. Surgical Procedure
2.5. Restoration Protocol
2.6. Soft Tissue Measurement
2.7. Esthetic Outcome
2.8. Statistical Analysis
3. Results
3.1. Soft Tissue Dimension
3.2. Jemt’s Index
3.3. PES
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Albrektsson, T. A multicenter report on osseo-integrated oral implants. J. Prosthet. Dent. 1988, 60, 75–84. [Google Scholar] [CrossRef]
- Garber, D.A. The esthetic dental implant: Letting restoration be the guide. J. Am. Dent. Assoc. 1995, 12, 319. [Google Scholar] [CrossRef] [PubMed]
- Sclar, A.G. Strategies for management of single-tooth extraction sites in aesthetic implant therapy. J. Oral Maxillofac. Surg. 2004, 62, 90. [Google Scholar] [CrossRef] [PubMed]
- Mohr, A.S. An extreme makeover: Aesthetic demands and patient satisfaction. Dent. Today 2005, 24, 56. [Google Scholar]
- Novaes, A.B.; Suaid, F.; Queiroz, A.C.; Muglia, V.A.; Souza, S.L.; Palioto, D.B.; Taba, M.; Grisi, M.F. Buccal bone plate remodeling after immediate implant placement with and without synthetic bone grafting and flapless surgery: Radiographic study in dogs. J. Oral Implantol. 2012, 38, 687–698. [Google Scholar] [CrossRef]
- Kan, J.Y.; Rungcharassaeng, K.; Lozada, J. Immediate placement and provisionalization of maxillary anterior single implants: 1-year prospective study. Int. J. Oral Maxillofac. Implants 2003, 18, 31–39. [Google Scholar]
- Buser, D.; Martin, W.; Belser, U.C. Optimizing esthetics for implant restorations in the anterior maxilla: Anatomic and surgical considerations. Int. J. Oral Maxillofac. Implants 2004, 19, 43–61. [Google Scholar]
- De Rouck, T.; Collys, K.; Cosyn, J. Immediate single-tooth implants in the anterior maxilla: A 1-year case cohort study on hard and soft tissue response. J. Clin. Periodontol. 2008, 35, 649–657. [Google Scholar] [CrossRef]
- De Rouck, T.; Collys, K.; Wyn, I.; Cosyn, J. Instant provisionalization of immediate single-tooth implants is essential to optimize esthetic treatment outcome. Clin. Oral Implants Res. 2009, 20, 566–570. [Google Scholar] [CrossRef]
- Khzam, N.; Mattheos, N.; Roberts, D.; Bruce, W.L.; Ivanovski, S. Immediate placement and restoration of dental implants in the esthetic region: Clinical case series. J. Esthet. Restor. Dent. 2014, 25, 332–344. [Google Scholar] [CrossRef]
- Tsuda, H.; Rungcharassaeng, K.; Kan, J.Y.; Roe, P.; Lozada, J.L.; Zimmerman, G. Peri-implant tissue response following connective tissue and bone grafting in conjunction with immediate single-tooth replacement in the esthetic zone: A case series. Int. J. Oral Maxillofac. Implants 2011, 26, 427–436. [Google Scholar] [PubMed]
- Brown, S.D.; Payne, A.G. Immediately restored single implants in the aesthetic zone of the maxilla using a novel design: 1-year report. Clin. Oral Implants Res. 2011, 22, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Cosyn, J.; De Bruyn, H.; Cleymaet, R. Soft tissue preservationand pink aesthetics around single immediate implant restorations: A 1-year prospective study. Clin. Implant. Dent. Relat. Res. 2013, 15, 847–857. [Google Scholar] [CrossRef] [PubMed]
- Botticelli, D.; Berglundh, T.; Lindhe, J. Hard-tissue alterations following immediate implant placement in extraction sites. J. Clin. Periodontol. 2004, 31, 820–828. [Google Scholar] [CrossRef]
- Hämmerle, C.H.; Chen, S.T.; Wilson, T.G., Jr. Consensus statements and recommended clinical procedures regarding the placement of implants in extraction sockets. Int. J. Oral Maxillofac. Implant. 2004, 19, 26–28. [Google Scholar]
- Araujo, M.G.; Linder, E.; Lindhe, J. Bio-Oss collagen in the buccal gap at immediate implants: A 6-month study in the dog. Clin. Oral Implants Res. 2011, 22, 1–8. [Google Scholar] [CrossRef]
- Tarnow, D.P.; Chu, S.J.; Salama, M.A.; Stappert, C.F.J.; Salama, H.; Garber, D.A.; Sarnachiaro, G.; Sarnachiaro, E.; Gotta, S.; Saito, H. Flapless post extraction socket implant placement in the esthetic zone: Part 1. The effect of bone grafting and/or provisional restoration on facial-palatal redge dimension change-a retrospective cohort study. Int. J. Periodontics Restor. Dent. 2014, 34, 323–331. [Google Scholar] [CrossRef]
- Tiziano, T.; Tommaso, W.; Fabio, S.; Hom-lay, W.; Giovanni, Z. Implant placement in the esthetic area: Criteria for positioning single and multiple implants. Periodontology 2000 2018, 77, 176–196. [Google Scholar]
- Choi, S.K. Digital technologies for restorative care; Part 1. Decis. Dent. 2018, 4, 33–36. [Google Scholar]
- Hammerle, C.; Stone, P.; Jung, R.E.; Kapos, T.; Brodala, N. Consensus statements and recommended clinical procedures regarding computer-assisted implant dentistry. Int. J. Oral Maxillofac. Implants 2009, 24, 126–131. [Google Scholar]
- Sun, Y.; Lübbers, H.T.; Agbaje, J.O.; Schepers, S.; Politis, C.; Slycke, S.V.; Vrielinck, L. Accuracy of Dental Implant Placement Using CBCT-Derived Mucosa-Supported Stereolithographic Template. Clin. Implant Dent. Relat. Res. 2015, 17, 862–870. [Google Scholar] [CrossRef] [PubMed]
- George, R. Deeb, How Accurate Are Implant Surgical Guides Produced with Desktop Stereolithographic 3-Dimentional Printers? J. Oral Maxillofac. Surg. 2017, 75, e1–e2559. [Google Scholar]
- Mario, B.; Pier, P.P.; Silvia, P.; Sebastian, T.; Mattia, M.; Marco, C.; Carlo, M. Peri-implant soft tissue conditioning by means of customized healing abutment: A randomized controlled clinical trial. Materials 2019, 12, 18. [Google Scholar]
- Kyung, C.O.; Jeongwon, P.; Hee-Hwan, K. Esthetic rehabilitation of maxillary anterior teeth, including an immediate provisionalization with an implant-supported fixed dental prosthesis. J. Clin. Med. 2019, 28, 8. [Google Scholar]
- Dingxiang, Y.; Xin, W.; Su, C. Vertical and horizontal dimensional changes of peri-implant facial bone following immediate placement and provisionalization with customized definite abutment in maxillary anterior single implants. Clin. Oral Implants Res. 2019, 30, 387. [Google Scholar]
- Jemt, T. Regeneration of gingival papillae after single-implant treatment. Int. J. Periodontics Restor. Dent. 1997, 17, 326–333. [Google Scholar]
- Fürhauser, R.; Florescu, D.; Benesch, T.; Haas, R.; Mailath, G.; Watzek, G. Evaluation of soft tissue around single tooth implant crowns: The pink esthetic score. Clin. Oral Implants Res. 2005, 16, 639–644. [Google Scholar] [CrossRef]
- Atieh, M.A.; Payne, A.G.; Duncan, W.J.; Cullinan, M.P. Immediate restoration/loading of immediately placed single implants: Is it an effective bimodal approach? Clin. Oral Implants Res. 2009, 20, 645–659. [Google Scholar] [CrossRef]
- Furze, D.; Byrne, A.; Alam, S.; Wittneben, J.G. Esthetic outcome of implant supported crowns with and without peri-implant conditioning using provisional fixed prosthesis: A randomized controlled clinical trial. Clin. Implant Dent. Relat. Res. 2016, 18, 1153–1162. [Google Scholar] [CrossRef]
- Lewis, S. Anterior single-tooth implant restorations. Int. J. Periodontics Restorative Dent. 1995, 15, 31–41. [Google Scholar]
- Tselios, N.; Parel, S.M.; Jones, J.D. Immediate placement and immediate provisional abutment modeling in anterior single-tooth implant restorations using a CAD/CAM application: A clinical report. J. Prosthet. Dent. 2016, 95, 181–185. [Google Scholar] [CrossRef]
- Bruno, V.; O’Sullivan, D.; Badino, M.; Catapano, S. Preserving soft tissue after placing implants in fresh extraction sockets in the maxillary esthetic zone and a prosthetic template for interim crown fabrication: A prospective study. J. Prosthet. Dent. 2014, 111, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.S.; Harris, B.T.; Morton, D. Use of implant-supported interim restorations to transfer periimplant soft tissue profiles to a milled polyurethane definitive cast. J. Prosthet. Dent. 2013, 109, 333–337. [Google Scholar] [CrossRef]
- Akin, R. A new concept in maintaining the emergence profile in immediate posterior implant placement: The anatomic harmony abutment. J. Oral Maxillofac. Surg. 2016, 74, 2385–2392. [Google Scholar] [CrossRef] [PubMed]
- Fuster-Torres, M.A.; Albalat-Estela, S.; Alcañiz-Raya, M.; Peñarrocha-Diago, M. CAD/CAM dental systems in implant dentistry: Update. Med. Oral Patol. Oral Cir. Bucal. 2009, 14, e141–e145. [Google Scholar]
- Saito, H.; Chu, S.J.; Reynolds, M.A.; Tarnow, D.P. Provisional restorations used in immediate implant placement provide a platform to promote peri-implant soft tissue healing: A pilot study. Int. J. Periodontics Restor. Dent. 2016, 36, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Periklis, P. Immediate provisionalization with a CAD/CAM interim abutment and crown: A guided soft tissue healing technique. J. Prosthet. Dent. 2015, 113, 91–95. [Google Scholar]
- Pesce, P.; Menini, M.; Tommasato, G.; Patini, R.; Canullo, L. Influence of modified titanium abutment surface on peri-implant soft tissue behavior: A systematic review of histological findings. Int. J. Oral Implantol. 2019, 12, 419–429. [Google Scholar]
- Khzam, N.; Arora, H.; Kim, P.; Fisher, A.; Mattheos, N.; Ivanovski, S. Systematic review of soft tissue alterations and esthetic outcomes following immediate implant placement and restoration of single implants in the anterior maxilla. J. Periodontol. 2015, 86, 1321–1330. [Google Scholar] [CrossRef]
- Tian, J.; Wei, D.; Zhao, Y.; Di, P.; Jiang, X.; Lin, Y. Labial soft tissue contour dynamics following immediate implants and immediate provisionalization of single maxillary incisors: A 1-year prospective study. Clin. Implant Dent. Relat. Res. 2019, 21, 492–502. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Amounts of Change | p-Value |
|---|---|---|
| Midfacial mucosa level | 0.27 ± 0.42 | 0.028 |
| Mesial papilla level | 0.32 ± 0.83 | 0.203 |
| Distal papilla level | 0.10 ± 0.06 | 0.594 |
| Horizontal change in the labial soft tissue | 0.32 ± 0.83 | 0.060 |
| Mean ± standard deviation |
| Parameters | Amounts of Change | p-Value |
|---|---|---|
| Mesial papilla | −1.342 * | 0.180 |
| Distal papilla | −1.414 * | 0.157 |
| PES Parameter | Pre-Operative | Follow-Up | p-Value |
|---|---|---|---|
| Mesial papilla | 1.33 ± 0.49 | 1.25 ± 0.45 | 0.586 |
| Distal papilla | 1.42 ± 0.51 | 1.58 ± 0.51 | 0.438 |
| Midfacial mucosa level | 1.67 ± 0.65 | 1.42 ± 0.51 | 0.117 |
| Midfacial contour | 1.58 ± 0.51 | 1.33 ± 0.49 | 0.191 |
| Alveolar process deficiency | 1.33 ± 0.78 | 1.16 ± 0.72 | 0.504 |
| Soft tissue color | 1.58 ± 0.51 | 1.42 ± 0.51 | 0.339 |
| Soft tissue texture | 1.50 ± 0.52 | 1.42 ± 0.51 | 0.586 |
| Total score | 10.58 ± 1.97 | 9.83 ± 1.34 | 0.137 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, T.-H.; Oh, Y.-K.; Jeong, C.-M.; Ko, E.C.; Sándor, G.K.; Kim, Y.-D. Soft Tissue Evaluation of an Immediate Esthetic Zone Single Implant with a Stereolithographic Guide Using 3D Reconstruction and a CAD/CAM Customized Titanium Anatomic Abutment. Appl. Sci. 2020, 10, 1678. https://doi.org/10.3390/app10051678
Kim T-H, Oh Y-K, Jeong C-M, Ko EC, Sándor GK, Kim Y-D. Soft Tissue Evaluation of an Immediate Esthetic Zone Single Implant with a Stereolithographic Guide Using 3D Reconstruction and a CAD/CAM Customized Titanium Anatomic Abutment. Applied Sciences. 2020; 10(5):1678. https://doi.org/10.3390/app10051678
Chicago/Turabian StyleKim, Tae-Heung, You-Kyoung Oh, Chang-Mo Jeong, Edward Chengchuan Ko, George K. Sándor, and Yong-Deok Kim. 2020. "Soft Tissue Evaluation of an Immediate Esthetic Zone Single Implant with a Stereolithographic Guide Using 3D Reconstruction and a CAD/CAM Customized Titanium Anatomic Abutment" Applied Sciences 10, no. 5: 1678. https://doi.org/10.3390/app10051678
APA StyleKim, T.-H., Oh, Y.-K., Jeong, C.-M., Ko, E. C., Sándor, G. K., & Kim, Y.-D. (2020). Soft Tissue Evaluation of an Immediate Esthetic Zone Single Implant with a Stereolithographic Guide Using 3D Reconstruction and a CAD/CAM Customized Titanium Anatomic Abutment. Applied Sciences, 10(5), 1678. https://doi.org/10.3390/app10051678