Abstract
Conventional methods that have been developed to immobilize the mouth and tongue for radiotherapy (RT) in head and neck cancer (HNC) treatment have been unsatisfactory. We, therefore, developed three-dimensional (3D), customizable, silicone bite blocks and examined their clinical feasibility. For HNC patients, before RT, the 3D printed bite blocks were fabricated based on primary computed tomography (CT) simulation images. The placement of the 3D bite blocks was followed by a secondary CT simulation before RT planning was finalized. Dosimetric parameters and positioning verification achieved with the propose bite blocks were compared with conventional universal oral corks. The 3D printed bite blocks were conformal to the occlusal surface, ensuring immobilization of the tongue without eliciting a gag reflex, and an elastic and firm texture that supports opening of the mouth, with a smooth surface with tolerable intraoral tactility. The dosimetry of patients using the proposed bite blocks showed better coverage of the planning target volume and surface of a tumour bed along with reduction in normal tissue doses. Good concordance of positioning by 3D printed bite blocks during the RT course was verified. The 3D printed bite blocks with silicone might be a customizable, safe, and practical advanced technology in RT for HNC.
1. Introduction
Head and neck cancer (HNC) is one of the most common malignancies worldwide. Approximately 650,000 patients are diagnosed annually with HNC worldwide [1]. Most HNCs arise in the epithelial lining of the oral cavity, oropharynx, larynx, and hypopharynx. They share similar risk factors, including cigarette smoking and alcohol drinking [2].
For patients with HNC, many strategies are utilized, such as surgery, definitive radiotherapy (RT), and chemoradiation (CCRT) [3]. HNC is relatively sensitive to radiation and anti-cancer drugs, such as cisplatin. Therefore, CCRT is increasingly used, not only in definitive settings but also as sequential treatment after induction chemotherapy of hypopharyngeal cancer, especially in locally advanced disease, where organ preservation, and lower rates of complications and mortality compared to surgery, can be achieved [4]. However, treatment-related toxicities, including oral mucositis, dysphagia, xerostomia, and weight loss occur, and may interfere and prolong the RT process with discomfort. Oral fixation has been considered important for RT dose reduction in adjacent normal tissues and toxicity prevention. Multiple conventional universal oral corks are manufactured for the benefit of oral fixation, and widely used in head and neck RT with low cost and easy production. Nowadays, a variety of bite blocks are commercialized, and their usefulness has been well-reported [5]. In external beam RT for cancer of the tongue, floor of the mouth, and lower gingiva, bite blocks can reduce the radiation dose to the upper gingiva or hard palate by supporting opening of the mouth. Bite blocks also immobilize oral tongue, which is important when treating HNC patients. Bite blocks can also reduce the radiation dose to adjacent normal tissue, such as salivary gland and mandible [6,7].
The usefulness of commercialized bite blocks in RT is well known, but studies on customized devices to fix the mouth and tongue are few. There is a growing interest in the application of three-dimensional (3D) printing to the RT process. The majority of studies focus on the creation of boluses [8,9], masks [10,11], and phantoms for quality assurance [12,13]. Their clinical use in HNC RT is still under investigation. We aim to customize the bite blocks by establishing a 3D printing technology and examining its clinical feasibility and practicality.
2. Materials and Methods
2.1. Development of Treatment Process
The RT preparation process for HNC at our institution is shown in Figure 1.
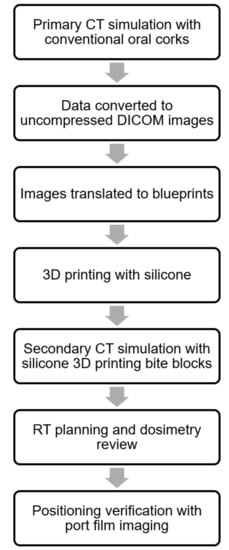
Figure 1.
Clinical flow chart showing the steps in the head and neck RT process with the silicone 3D printed bite blocks. First, a primary CT simulation for the head and neck was performed with conventional oral corks; second, the obtained CT images were converted to uncompressed DICOM images; third, the DICOM images were translated into blueprints with the occlusal surface and tongue contoured, and the blueprints were checked by radiation oncologists; fourth, 3D printing with silicone proceeded according to the blueprints; fifth, secondary CT simulation with silicone 3D printed bite blocks was carried out; sixth, RT planning and dosimetry with silicone 3D printed bite blocks was reviewed before treatment; seventh, the patient positioning verification was checked by port film imaging. RT, radiotherapy; 3D, 3-dimensional; CT, computed tomography; DICOM, Digital Imaging and Communications in Medicine.
2.2. Materials of 3D Printed Bite Blocks
Initially, the 3D printed bite blocks were laid out with MED610, a biocompatible material widely used in medical treatment, surgical guides, orthopaedic procedures, and dental implants. However, patients with HNC often complained of pain and discomfort when 3D printed bite blocks, fabricated from the rigid MED610, were used for oral wounds, mucositis, or xerostomia during RT. Therefore, we fabricated the 3D printed bite blocks with silicone, an elastic but firm, strong, durable, and safe material. These 3D printed bite blocks were manufactured by the silicone 3D printer (S100, San Draw Inc., Taichung, Taiwan), and the material of bite blocks was SIL 28 (San Draw Inc., Taiwan), which was one part of Room Temperature Vulcanization (RTV) silicone specially designed for 3D printing, has passed biocompatibility testing of ISO 10993-5 (Figure 2). The hardness (ASTM D2240) of SIL 28 was 28, Shore A, and the tensile strength was 270psi. The tear strength was 5 kgf/cm, and the elongation was 300%. The silicone bite blocks had superior mechanical and physical properties, such as good elasticity, adequate rigidity, heat and cold resistance, and great biocompatibility. The hardness of the unique silicone 3D printed bite blocks was adjustable by varying their internal structures and silicone components. The silicone bite blocks lost their smell after being left to stand in air. Their dosimetry was examined and showed no interference in RT planning. All patients tolerated the blocks well in intraoral placement.
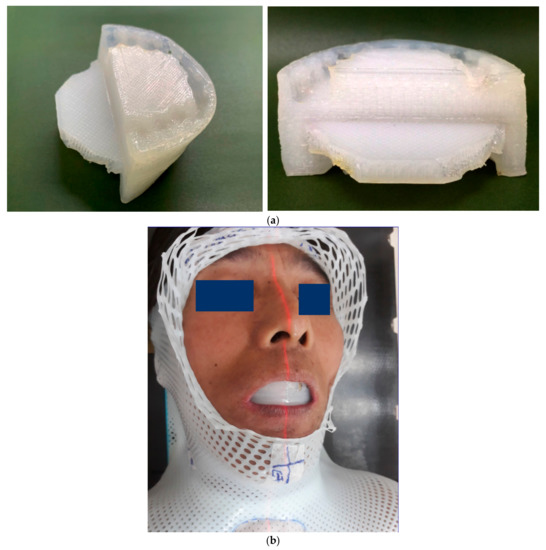
Figure 2.
Shape and clinical use of the silicone 3D-printing bite block. The silicone 3D printing bite block exhibited superior mechanical and physical properties, such as good elasticity, adequate rigidity, heat and cold resistance, and great biocompatibility. (a) The shapes of the occlusal surface and tongue depressor were integrated into one piece. (b) The patient tolerated the silicone 3D printed bite block well in the CT simulation and RT process.
2.3. Patients
All patients had biopsy-proven HNC. Patients with dentures or missing incisors or canines were excluded. All patients with an indication for RT were enrolled.
2.4. Computed Tomography (CT) Simulation
Patients underwent a primary CT simulation in the supine position and were immobilized with thermoplastic masks. Planning CT images with a maximum slice thickness of 3 mm were acquired through the head and neck. Conventional oral corks were inserted into the patients’ mouths to keep them open. Tongue depressors were designed to immobilize the tongue during the CT simulation. A contrast medium was used to increase the contrast of the tumour and involved lymph nodes. The 3D printed bite blocks were prepared using the primary CT simulation images.
2.5. 3D Printing Process
The CT images were converted into uncompressed digital imaging and communications in medicine (DICOM) images, and the occlusal surfaces were contoured. Tongue depressors were also contoured for tongue fixation. All data was saved as standard tessellation language (STL) files and imported into the 3D modeling software (Tinkercad, v. 2017, Autodesk Inc., San Rafael, CA, USA). The 3D printing process was performed after the blueprint was checked by the radiation oncologists. The blueprint was shown in Figure 3. The STL files of the final digitalized 3D printed bite blocks were imported into the silicone 3D printer (S100, San Draw Inc., Taiwan) for 3D printing. A 3D printing system (FAMTM, San Draw Inc., Taiwan) was introduced for the process. FAMTM, which stood for Full-colour, Adjustable hardness, and Multi-material 3D printing, was specially designed to create multi-colour models out of RTV silicone, a flexible and tactile material. The 3D printed bite blocks were created with 3 mm of uniform thickness. The time required for 3D printing was approximate 2 h. After the 3D bite blocks were printed, patients underwent a secondary CT simulation without contrast with the customized oral devices for RT planning.
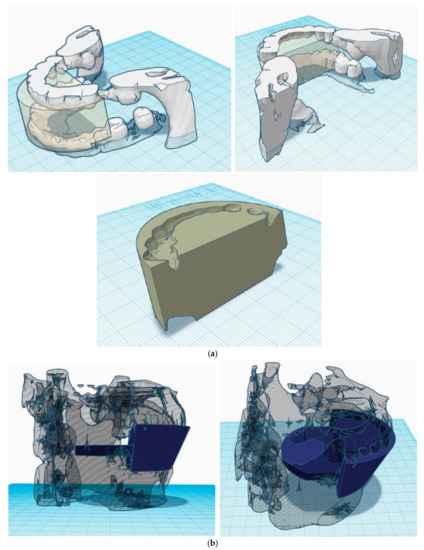
Figure 3.
Blueprint for 3D printing. (a) The occlusal surface was contoured in the blueprint with incisors, canines, and molars well expressed. (b) The tongue depressor was designed to immobilize the tongue, and the length of the tongue depressor was adjusted to prevent occurrence of the gag reflex caused by over-extension of the tongue depressor.
2.6. RT Design
The gross tumour volume (GTV) consisted of the primary tumour and involved lymph nodes. The high risk clinical target volume (CTVH) was defined as the GTV plus margins of at least 5 mm in the definitive settings or the surgical bed with margins in the adjuvant settings. The intermediate risk CTV (CTVM) included the lymph node area of high risk subclinical disease. The bilateral neck, especially the ipsilateral neck, was often categorized as the CTVM, depending on clinical or pathologic stage, primary tumour sites, and the involved lymph nodes. The low risk CTV (CTVL) was defined as the lymph node area of low risk disease. The planning target volume (PTV) was defined as the CTV plus a 0.3 cm margin in all directions for HNC. The radiation dose in the definitive settings was typically 66–70 Gy in the high risk PTV (PTVH) and 54–63 Gy in the low and intermediate risk PTV (PTVL and PTVM, respectively) according to the NCCN guideline. The radiation dose in the adjuvant settings was typically 60–66 Gy in the PTVH and 54–63 Gy in the PTVL and PTVM.
2.7. RT Planning
Intensity modulated radiation therapy (IMRT) with SIB techniques was used for all patients. The treatment plans were generated using 6-MV or 10-MV photons. The patients were all treated with linear accelerators (Eclipse Treatment Planning System; Varian Medical Systems Inc., Palo Alto, CA, USA). The prescribed doses were 70 Gy for the PTVH, 63 Gy for the PTVM, and 56 Gy for the PTVL in the definitive settings, and 60–66 Gy for the PTVH and 54–60 Gy for the PTVM and PTVL in the adjuvant settings. The goals were to deliver the prescribed dose to ≥ 95% of the PTV and deliver 95% of the prescribed dose to ≥ 99% of the PTV. Dose distributions of planning with the silicone 3D printed bite blocks and conventional oral corks were compared by using the isodose lines at 95% of the prescribed dose for the PTVH and dose-volume histogram (DVH).
2.8. Dosimetric Comparison
Dosimetric parameters such as the PTV D100%, maximum dose in the PTV (PTVmax), minimum dose in the PTV (PTVmin), conformity index (CI), and homogeneity index (HI) of the PTV were calculated to analyse the quality of our RT planning. PTV D100% was the volume with minimum dose received by 100% of prescribed dose. PTVmax should not exceed 107% of the dose, and PTVmin should not be smaller than 95% of dose. The CI was defined as the ratio between the volume covered by the reference isodose, which according to the ICRU was 95% isodose and the target volume designated in this study was the PTVH. CI = VRI/TV, where VRI was reference isodose volume, and TV was target volume. The CI equal to 1 corresponded to the ideal dose coverage or high conformity. The CI greater than 1 indicated that irradiated volume exceeded the target volume and covered part of the healthy tissue. The CI less than 1 meant that the target volume was partially radiated. The HI was defined as the ratio of the maximum dose in the target volume to the reference isodose. HI was Imax/RI, where Imax was maximum isodose in the target, and RI was reference isodose. HI was an objective tool to analyze the uniformity of dose distribution in the target volume. The ideal value of HI was 1, and it increased as the plan became less homogeneous. The mean dose of the oral cavity was recorded for constraint concerning mucositis, and the V26 of bilateral parotid glands (the volume of the RT dose to 26 Gy in the parotid glands) was used for xerostomia consideration [14]. All dosimetric parameters were measured in comparison with conventional universal oral corks [15].
2.9. Images Verification
The kilovoltage (kV) X-ray imaging systems provided radiographic modes that were used to verify isocentre and patient positioning. The patient positioning verification was checked by radiation oncologists on the first day of RT and every week if required. The positioning verification was measured and compared with that obtained with conventional universal oral corks.
2.10. Ethical Statement
This study was approved by the Institutional Review Board of our institution (IRB number: 19MMHIS218e).
3. Results
3.1. Special Consideration of the Unique Technology of 3D Printing Bite Blocks
3.1.1. Conformal to Occlusal Surface
The occlusal surfaces of a patient would be influenced by the patient’s teeth and their environment, so patients’ teeth were checked by dentists. Tooth decay and tooth erosion were treated to ensure better 3D printing and RT settings. The shape of the 3D printed bite blocks were fabricated according to the primary CT simulation images with incisors, canines, first, and second molars contoured in the blueprint. Therefore, the 3D printed bite blocks fit the upper and lower dental arches well.
3.1.2. Immobilization of the Tongue without Gag Reflex
Initially, the 3D printed bite blocks were produced by CT images with oral corks only. However, the tongue position was poorly controlled. To solve this problem, the oral devices with tongue depressors were delivered to immobilize the tongue during the CT simulation. Then, the 3D printed bite blocks with tongue depressors were manufactured. Another problem was the discomfort due to the gag reflex if the tongue depressors extended to the posterior tongue. Excessive deformation of the tongue was also observed. Therefore, the 3D printed bite blocks with tongue depressors were mainly designed to fix the position of the anterior tongue.
3.1.3. Elastic and Firm Texture that Supports Opening of the Mouth
The silicone 3D printed bite blocks were selected for their elasticity and because they were firm enough to support an open mouth and to separate the contralateral buccal mucosa from the ipsilateral buccal mucosa. The RT dose that scattered to contralateral healthy organs was then reduced.
3.1.4. Smooth Surface with Tolerable Intraoral Tactility
The 3D printed bite blocks were designed to fit patients’ occlusal surfaces, and many biocompatible materials were tested. The silicone 3D printed bite blocks were selected for their smooth surface and intraoral tactility. Patients tolerated the RT process well.
3.2. Dosimetric Comparison
The dose distribution and dosimetry were reviewed as follows with the PTV D100%, PTVmax, PTVmin, CI, and HI of PTVH. The mean dose of the oral cavity and V26 of the bilateral parotid glands were also evaluated. For Patient 1, who was diagnosed with tongue cancer, cT2N0M0, stage II, he received composite resection for the primary tumour and neck lymph node dissection with pT2N0Mb, stage II. Adjuvant RT was arranged for perineural invasion. The PTVH was the surgical bed of the primary tumour with margins. The dosimetry, when silicone 3D-printed bite blocks were used, showed better coverage of the PTVH and surface of the oral tongue than when conventional universal oral corks were used. The CIs of the PTVH of the plan with 3D printed bite blocks was 0.96, compared to the plan with conventional oral corks, 0.94. The HIs of the PTVH were 1.13 and 1.12. The median dose for the oral cavity was 45.7 Gy and 48.6 Gy (Table 1). The isodose line in 95% of the prescribed dose to the PTVH showed better coverage when silicone 3D printed bite blocks were used than conventional oral corks in the RT process (Figure 4a versus Figure 4b with arrowhead indicated). The dose scattered to the oral cavity was lower when silicone 3D printed bite blocks were used than conventional oral corks. The radiation dose and hot spot of the oral tongue were higher with better constraints of adjacent normal tissues when silicone 3D printed bite blocks functioned as boluses (Figure 4).

Table 1.
Dosimetry of Patient 1.
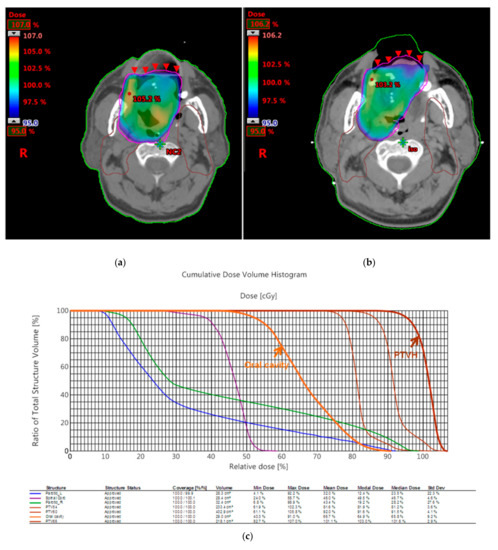
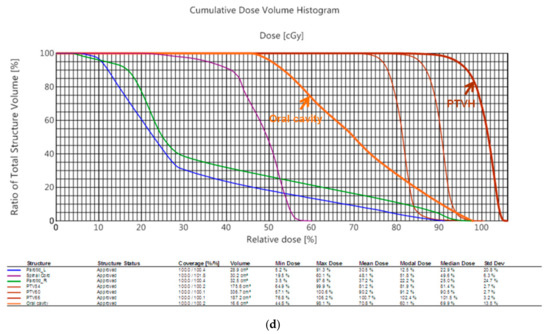
Figure 4.
Dose distributions of Patient 1 with two plans with silicone 3D printed bite blocks or conventional oral corks. (a) Dosimetry with the silicone 3D printing bite block showed better coverage of the PTVH and surface of the residual tongue compared to (b) that with the conventional oral cork. (c) In the DVH analysis, the radiation dose of the PTVH and residual tongue was higher and seemed to indicate that a lower dose had scattered to the oral cavity with the silicone 3D printing bite block than (d) with the conventional oral cork.
Patient 2, who was diagnosed as having left tonsil cancer, received an operation and a positive margin was noted in pathologic review. Adjuvant RT was arranged. The PTVH was the surgical bed of the primary tumour with margins. Dosimetry with the silicone 3D printing bite block showed similar distribution in PTVH to that with the conventional oral cork. In the DVH analysis, the RT dose, which scattered to adjacent normal tissues, such as bilateral parotid glands, was lower using the silicone 3D printing bite block than with conventional oral cork. The CIs of the PTVH of each plan were 0.99 and 1.00, and the HIs of the PTVH were 1.08 and 1.12. The HI was lower with 3D printed bite blocks, indicating a higher homogeneity. The V26 of the right parotid gland was 38% and 70%, and V26 of the left parotid gland was 34% and 68% (Table 2). The radiation dose to the bilateral parotid glands was lower with silicone 3D printing bite blocks (Figure 5).
Table 2.
Dosimetry of Patient 2.
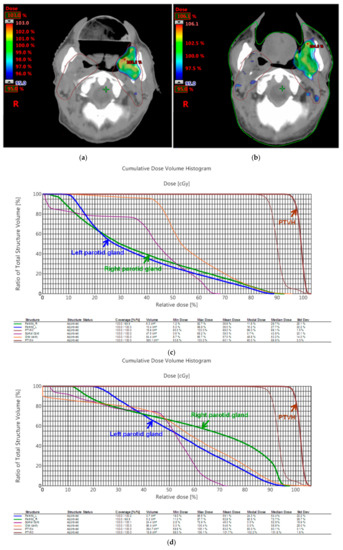
Figure 5.
Dose distributions of Patient 2 with two plans with silicone 3D printed bite blocks or conventional oral corks. (a) Dosimetry with the silicone 3D printing bite block showed similar distribution in PTVH to that (b) containing the conventional oral cork. (c) In the DVH analysis, the RT dose that scattered to adjacent normal tissues such as bilateral parotid glands was lower when using the silicone 3D printing bite block than (d) with conventional oral cork.
3.3. Image Verification
Patient positioning verification was checked by kV imaging, rather than megavoltage (MV) imaging, because it improved soft tissue contrast and ensured a lower radiation dose was needed to generate images and image quality was close to that of simulation images for facilitating comparisons. The port film images, checked by radiation oncologists, showed good alignment in the occlusal surface without displacement during the RT course (Figure 6).
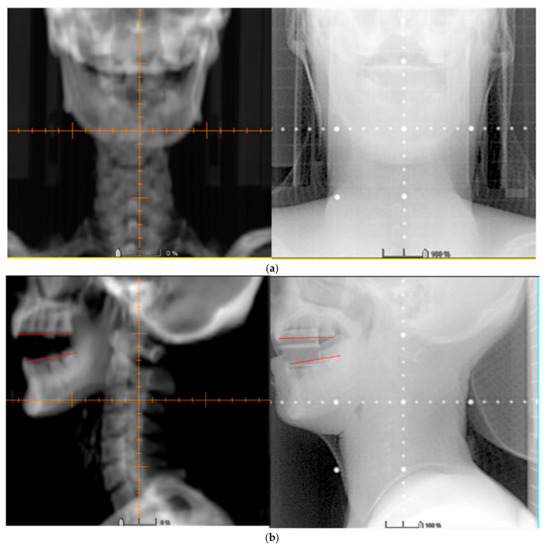
Figure 6.
Imaging verification by port film images. Orthogonal (a) anterior-posterior; and (b) lateral images were obtained to verify isocentre placement for patients receiving head and neck RT. The port film images showed good alignment in the occlusal surface without displacement.
4. Discussion
In this study, we evaluated the usefulness of silicone 3D printed bite blocks as fixation devices for head and neck RT patients. Dosimetry of patients, treated with the silicone 3D printed bite blocks, showed better coverage of the PTVH and surface of the tumour bed, and less scattering of the RT dose to adjacent normal tissues, than conventional universal corks. Good alignment in the occlusal surface was observed by port film imaging verification. Patients felt more comfortable using the silicone 3D printed bite blocks than other rigid materials.
Oral fixation in the RT process has been an important issue for decades, and various oral devices, such as bite blocks have been widely use in clinical treatment. Oita et al. examined the use of bite blocks to reduce setup error and intrafractional movement in the head and neck RT with a real-time tumour tracking RT system [6]. Verrone et al. reported the use of an intraoral stent as a mouth-opening device to reduce the radiation dose to healthy structures, especially bone tissue and salivary glands during RT [16]. For patients with HNC who could not tolerate the intraoral devices, Kil et al. proposed RT methods in which the tongue is stuck out. Decreasing the RT dose was noted, but the reproducibility of such a dose decrease should be a concern [17]. Musha et al. declared decreased radiation-induced mucositis with the use of a customized bite block for carbon-ion RT [18]. Kudoh et al. stated the effectiveness of water-equivalent bite blocks during external beam RT for oral cancer. In-homogeneity correction was achieved by the use of a water-equivalent material [19]. Ikawa et al. recommended the use of custom-made bite blocks incorporating tongue depressors or elevators to reduce radiation-induced mucositis during carbon-ion RT. According to different origins of HNC, depressors or elevators were used to reduce incidental exposure of the tongue and healthy structures during RT [20]. These kinds of 3D printed bite blocks were manufactured recently, and their clinical use is still being investigated and evaluated [21,22,23].
We have designed silicone 3D printed bite blocks to support opening of the mouth and fixation of the upper and lower dental arches, and tongue in CT simulations and RT. For tongue cancer, the tumour bed or surgical bed is presented in the air cavity. The skin-sparing effect of high energy photon beams may reduce the dose on the surface of the tongue. A higher dose was needed to compensate for the skin-sparing effect with unacceptable non-uniformity of the dose within the PTVH, and caused excessive irradiation to sensitive structures, which resulted in severe toxicities. The silicone 3D printed bite blocks with tongue depressors may work as boluses to overcome the skin-sparing effect so that a uniform dose may be obtained. The bolus effect still exists for patients with HNC other than tongue cancer. A homogeneous dose in the PTVH that presented in the air cavity was also observed in the 3D printed bite blocks, and not containing the conventional oral corks.
This is the first publication in which silicone 3D printed bite blocks have been customized in clinical RT treatment. The material and shape of the 3D printed bite blocks can be customized to fit every patient’s oral cavity. The dosimetric parameters, CI and HI, were used to evaluate the RT plans. Patients stated that they felt more comfortable when silicone 3D printed bite blocks were used, and we speculated that this meant greater fixation and better compliance in the RT process, which was confirmed by port film images verification.
In this investigation, we mainly aimed to establish the technique and processing procedures with optimization of intraoral materials for 3D printing. It is our understanding that the preliminary results of clinical test from too few patients are not convincing enough to draw conclusions that 3D printed silicone bite blocks are better than conventional oral corks. However, the preliminary study shows a trend of better PTV coverage, dose homogeneity, and a lower scattered dose to healthy tissue in the two patients. Further investigation is warranted for validation. In summary, the limitation of this study included the following issues. First, the case number included in the study was small. A large prospective study may be needed to reduce the setup errors. Second, patients stated that they did not experience discomfort with the silicone 3D printing bite blocks. The assumption that this implies better fixation should be further examined. Third, standard operating procedures (SOPs) and templates for fixing every mouth in CT simulation should be established. Although, we have produced templates of bite blocks with tongue depressors in the CT simulations, different sizes of templates are needed to fit every mouth in the future.
5. Conclusions
We fabricated silicone 3D printed bite blocks and used them in a clinical RT process. The material and shape of the oral devices were determined after taking into account the comfort of patients and potential setup errors. The tongue depressors helped to improve oral fixation during RT. A homogeneous dose may be obtained in the tumour bed with the 3D printed bite blocks when RT evaluation. The scattered dose to healthy tissue may decrease when uniform dose focused on the tumour bed. The 3D printed bite blocks with silicone might be a customizable, safe, and practical advanced technology for RT of head and neck cancer. However, considering the small case number, a larger prospective study is needed, and SOPs should also be established, for future work. Further clinical investigations for validation are warranted.
Author Contributions
Conceptualization, Y.-M.H. and Y.-J.C.; data curation, Y.-M.H., J.-C.L., and Y.-J.C.; formal analysis, Y.-M.H., C.-M.C. and Y.-J.C.; methodology, Y.-M.H., C.-M.C., H.-C.T., C.-W.C., and Y.-J.C.; supervision, Y.-J.C.; writing—original draft, Y.-M.H.; writing—review and editing, T.-C.H., F.Y.-S.C., and Y.-J.C. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by the MacKay Memorial Hospital [Grant numbers MMH-TW-10601, MMH-E-107-13, MMH-E-108-13].
Acknowledgments
We would like to thank Editage for providing their editing services.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Cohen, N.; Fedewa, S.; Chen, A.Y. Epidemiology and demographics of the head and neck cancer population. Oral Maxillofac. Surg. Clin. N. Am. 2018, 30, 381–395. [Google Scholar] [CrossRef]
- Lee, Y.A.; Li, S.; Chen, Y.; Li, Q.; Chen, C.J.; Hsu, W.L.; Lou, P.J.; Zhu, C.; Pan, J.; Shen, H.; et al. Tobacco smoking, alcohol drinking, betel quid chewing, and the risk of head and neck cancer in an East Asian population. Head Neck 2019, 41, 92–102. [Google Scholar] [CrossRef] [PubMed]
- Pignon, J.P.; le Maitre, A.; Maillard, E.; Bourhis, J. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): An update on 93 randomised trials and 17,346 patients. Radiother. Oncol. 2009, 92, 4–14. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, P.; Bourhis, J.; Lacas, B.; Posner, M.R.; Vermorken, J.B.; Hernandez, J.J.C.; Bourredjem, A.; Calais, G.; Paccagnella, A.; Hitt, R.; et al. Taxane-cisplatin-fluorouracil as induction chemotherapy in locally advanced head and neck cancers: An individual patient data meta-analysis of the meta-analysis of chemotherapy in head and neck cancer group. J. Clin. Oncol. 2013, 31, 2854–2860. [Google Scholar] [CrossRef]
- Hollows, P.; Hayter, J.P.; Vasanthan, S. The Leicester radiotherapy bite block: An aid to head and neck radiotherapy. Br. J. Oral Maxillofac. Surg. 2001, 39, 49–51. [Google Scholar] [CrossRef][Green Version]
- Oita, M.; Ohmori, K.; Obinata, K.; Kinoshita, R.; Onimaru, R.; Tsuchiya, K.; Suzuki, K.; Nishioka, T.; Ohsaka, H.; Fujita, K.; et al. Uncertainty in treatment of head-and-neck tumours by use of intraoral mouthpiece and embedded fiducials. Int. J. Radiat. Oncol. Biol. Phys. 2006, 64, 1581–1588. [Google Scholar] [CrossRef]
- Wagner, D.; Anton, M.; Vorwerk, H. Dose uncertainty in radiotherapy of patients with head and neck cancer measured by in vivo ESR/alanine dosimetry using a mouthpiece. Phys. Med. Biol. 2011, 56, 1373. [Google Scholar] [CrossRef]
- Robar, J.L.; Moran, K.; Allan, J.; Clancey, J.; Joseph, T.; Chytyk-Praznik, K.; MacDonald, R.L.; Lincoln, J.; Sadeghi, P.; Rutledge, R. Intrapatient study comparing 3D printed bolus versus standard vinyl gel sheet bolus for postmastectomy chest wall radiation therapy. Pract. Radiat. Oncol. 2018, 8, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Craft, D.; Balter, P.; Woodward, W.; Kry, S.; Salehpour, M.; Howell, R. Design and feasibility of 3D printed tissue compensators for postmastectomy radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, S184. [Google Scholar] [CrossRef]
- Haefner, M.F.; Giesel, F.L.; Mattke, M.; Rath, D.; Wade, M.; Kuypers, J.; Preuss, A.; Kauczor, H.U.; Schenk, J.P.; Debus, J.; et al. 3D-Printed masks as a new approach for immobilization in radiotherapy–a study of positioning accuracy. Oncotarget 2018, 9, 6490. [Google Scholar] [CrossRef] [PubMed]
- Loja, M.; Craveiro, D.; Vieira, L.; Sousa, E.; Rodrigues, J.; Portal, R. Radiotherapy-customized head immobilization masks: From modeling and analysis to 3D printing. Nucl. Sci. Tech. 2019, 30, 142. [Google Scholar] [CrossRef]
- Tino, R.; Yeo, A.; Leary, M.; Brandt, M.; Kron, T. A systematic review on 3D-printed imaging and dosimetry phantoms in radiation therapy. Technol. Cancer. Res. Treat. 2019, 1, 1–14. [Google Scholar] [CrossRef]
- Grehn, M.; Stille, M.; Ziemann, C.; Cremers, F.; Rades, D.; Buzug, T.M. A new phantom for individual verification of the dose distribution in precision radiotherapy for head-and-neck cancer. Anticancer Res. 2019, 39, 6931–6938. [Google Scholar] [CrossRef]
- Deasy, J.O.; Moiseenko, V.; Marks, L.; Chao, K.C.; Nam, J.; Eisbruch, A. Radiotherapy dose–volume effects on salivary gland function. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, S58–S63. [Google Scholar] [CrossRef] [PubMed]
- Brodin, N.P.; Kabarriti, R.; Garg, M.K.; Guha, C.; Tome, W.A. Systematic review of normal tissue complication models relevant to standard fractionation radiation therapy of the head and neck region published after the QUANTEC reports. Int. J. Radiat. Oncol. Biol. Phys. 2018, 100, 391–407. [Google Scholar] [CrossRef]
- Verrone, J.R.; Alves, F.A.; Prado, J.D.; Boccaletti, K.W.; Sereno, M.P.; Silva, M.L.; Jaguar, G.C. Impact of intraoral stent on the side effects of radiotherapy for oral cancer. Head Neck 2013, 35, E213–E217. [Google Scholar] [CrossRef]
- Kil, W.J.; Kulasekere, C.; Derrwaldt, R.; Bugno, J.; Hatch, C. Decreased radiation doses to tongue with “stick-out” tongue position over neutral tongue position in head and neck cancer patients who refused or could not tolerate an intraoral device (bite-block, tongue blade, or mouthpiece) due to trismus, gag reflex, or discomfort during intensity-modulated radiation therapy. Oncotarget 2016, 7, 53029. [Google Scholar] [PubMed]
- Musha, A.; Saitoh, J.; Shirai, K.; Kubota, Y.; Shimada, H.; Abe, T.; Komatsu, Y.; Komatsu, S.; Ohno, T.; Nakano, T.; et al. Customized mouthpieces designed to reduce tongue mucositis in carbon-ion radiotherapy for tumours of the nasal and paranasal sinuses. Phys. Imaging Radiat. Oncol. 2017, 3, 1–4. [Google Scholar] [CrossRef]
- Kudoh, T.; Ikushima, H.; Kudoh, K.; Furutani, S.; Kawanaka, T.; Kubo, A.; Takamaru, N.; Tamatani, T.; Miyamoto, Y. Effectiveness of newly developed water-equivalent mouthpiece during external beam radiotherapy for oral cancer. Ann. Carcinog. 2017, 2, 1007. [Google Scholar]
- Ikawa, H.; Koto, M.; Ebner, D.K.; Takagi, R.; Hayashi, K.; Tsuji, H.; Kamada, T. A custom-made mouthpiece incorporating tongue depressors and elevators to reduce radiation-induced tongue mucositis during carbon-ion radiation therapy for head and neck cancer. Pract. Radiat. Oncol. 2018, 8, e27–e31. [Google Scholar] [CrossRef]
- Hong, C.S.; Oh, D.; Ju, S.G.; Ahn, Y.C.; Na, C.H.; Kwon, D.Y.; Kim, C.C. Development of a semi-customized tongue displacement device using a 3D printer for head and neck IMRT. Radiat. Oncol. 2019, 14, 79. [Google Scholar] [CrossRef] [PubMed]
- Zaid, M.; Bajaj, N.; Burrows, H.; Mathew, R.; Dai, A.; Wilke, C.T.; Palasi, S.; Hergenrother, R.; Chung, C.; Fuller, C.D.; et al. Creating customized oral stents for head and neck radiotherapy using 3D scanning and printing. Radiat. Oncol. 2019, 14, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kitamori, H.; Sumida, I.; Tsujimoto, T.; Shimamoto, H.; Murakami, S.; Ohki, M. Evaluation of mouthpiece fixation devices for head and neck radiotherapy patients fabricated in PolyJet photopolymer by a 3D printer. Phys. Med. 2019, 58, 90–98. [Google Scholar] [CrossRef] [PubMed]







© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).