A Combination of Biphasic Calcium Phosphate (Maxresorb®) and Hyaluronic Acid Gel (Hyadent®) for Repairing Osseous Defects in a Rat Model

 ,
, 
Abstract
Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Animal Model
2.2. Experimental Groups
- Group I (BCP)
- Bone defects (n = 10 per group per time period) were grafted using 0.5 mL BCP (Maxresorb®, Botiss Biomaterials GmbH, Zossen, Germany) mixed with 1.0 mL sterile saline.
- Group II (BCP + HyA)
- Bone defects (n = 10 per group per time period) were grafted using 0.5 mL BCP (Maxresorb®, Botiss Biomaterials GmbH, Zossen, Germany) mixed with a commercially available hyaluronic acid (HyA) (Hyadent®, BioScience GmbH, Dümmer, Germany). HyA was provided as hydrogel in sterile 1.0 mL syringe. β-TCP granules extemporaneously mixed with HyA. Then, the mixture was immediately pushed into the bony defect with a spatula.
- Group III (HyA)
- Bone defects (n = 10 per group per time period) were filled with 1.0 mL HyA gel (Hyadent®, BioScience GmbH, Dümmer, Germany).
- Group IV (control)
- Bone defects (n = 10 per group per time period) were left empty as a control for natural healing.
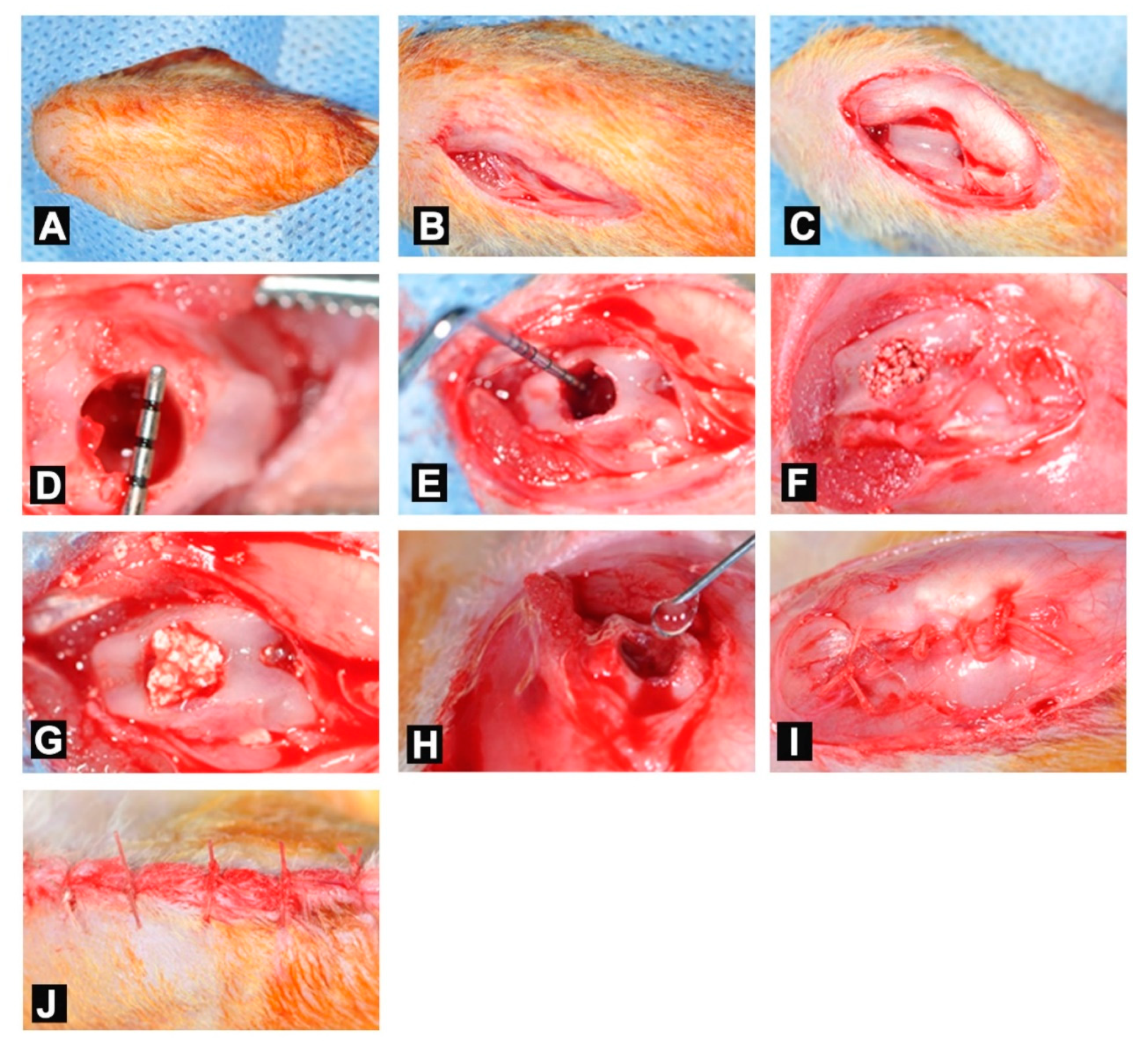
2.3. Surgical Procedure
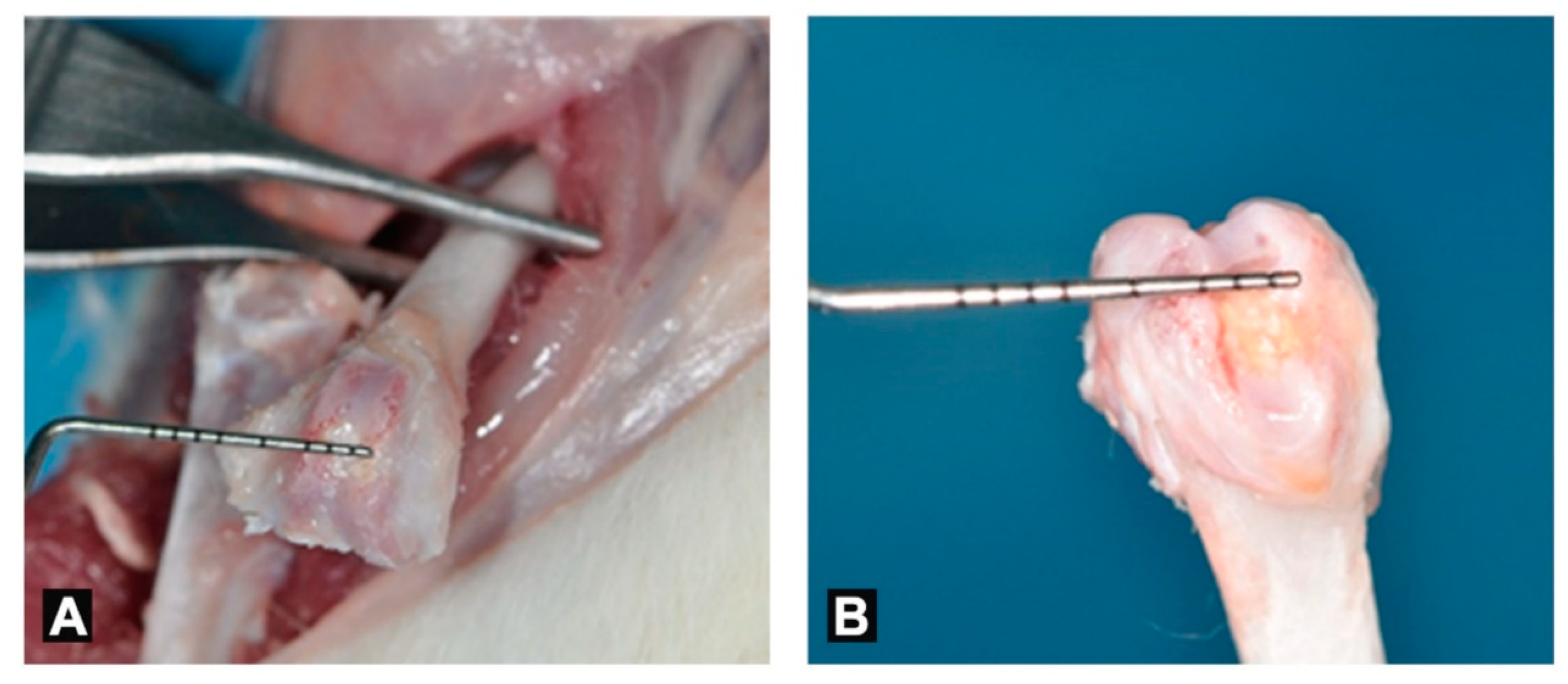
2.4. Retrieval of Samples
2.5. Analyses
2.5.1. Histological Preparations
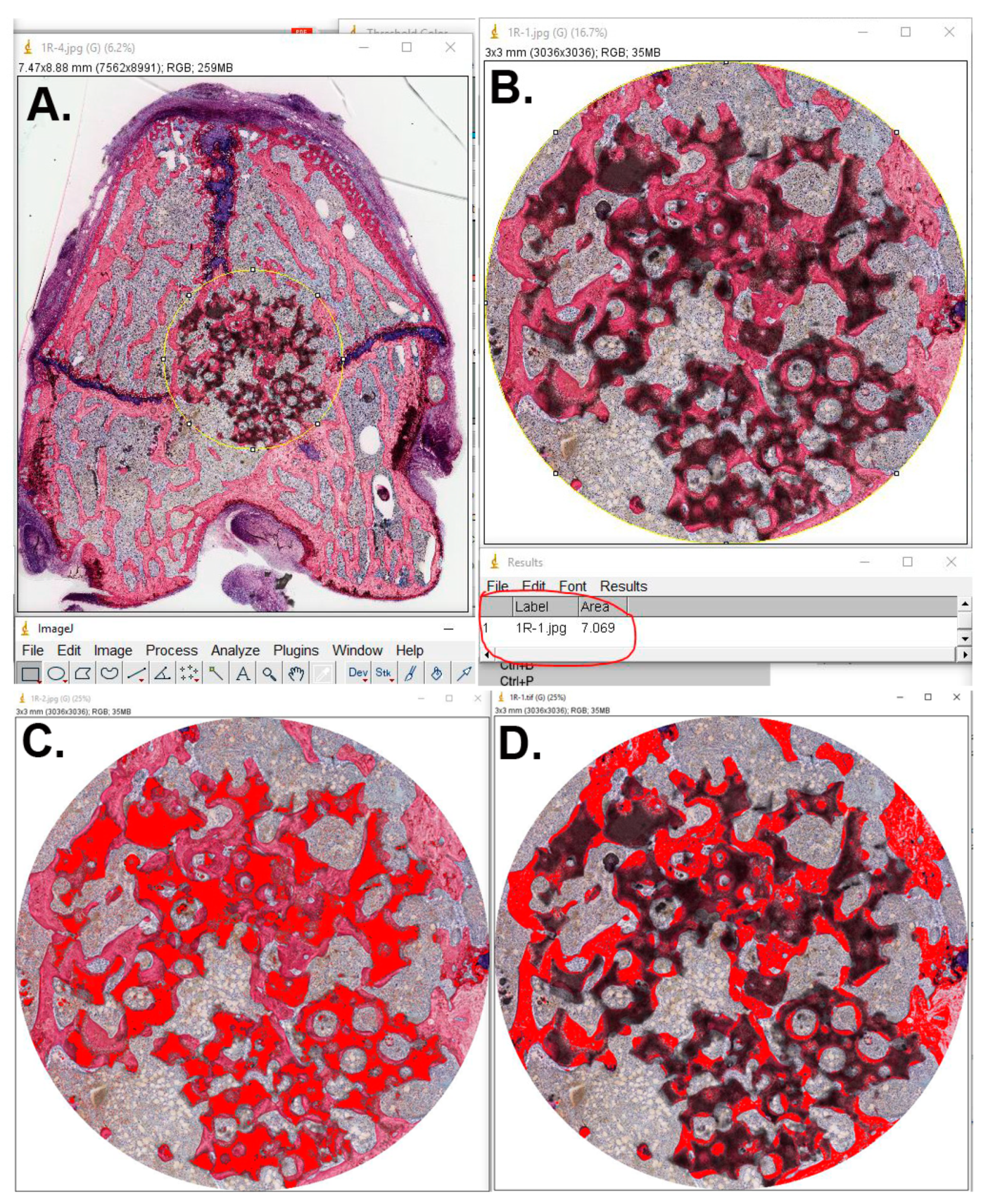
2.5.2. Histological and Histomorphometrical Evaluation
2.6. Statistical Analysis
3. Results
3.1. General Observations and Monitoring of Animals
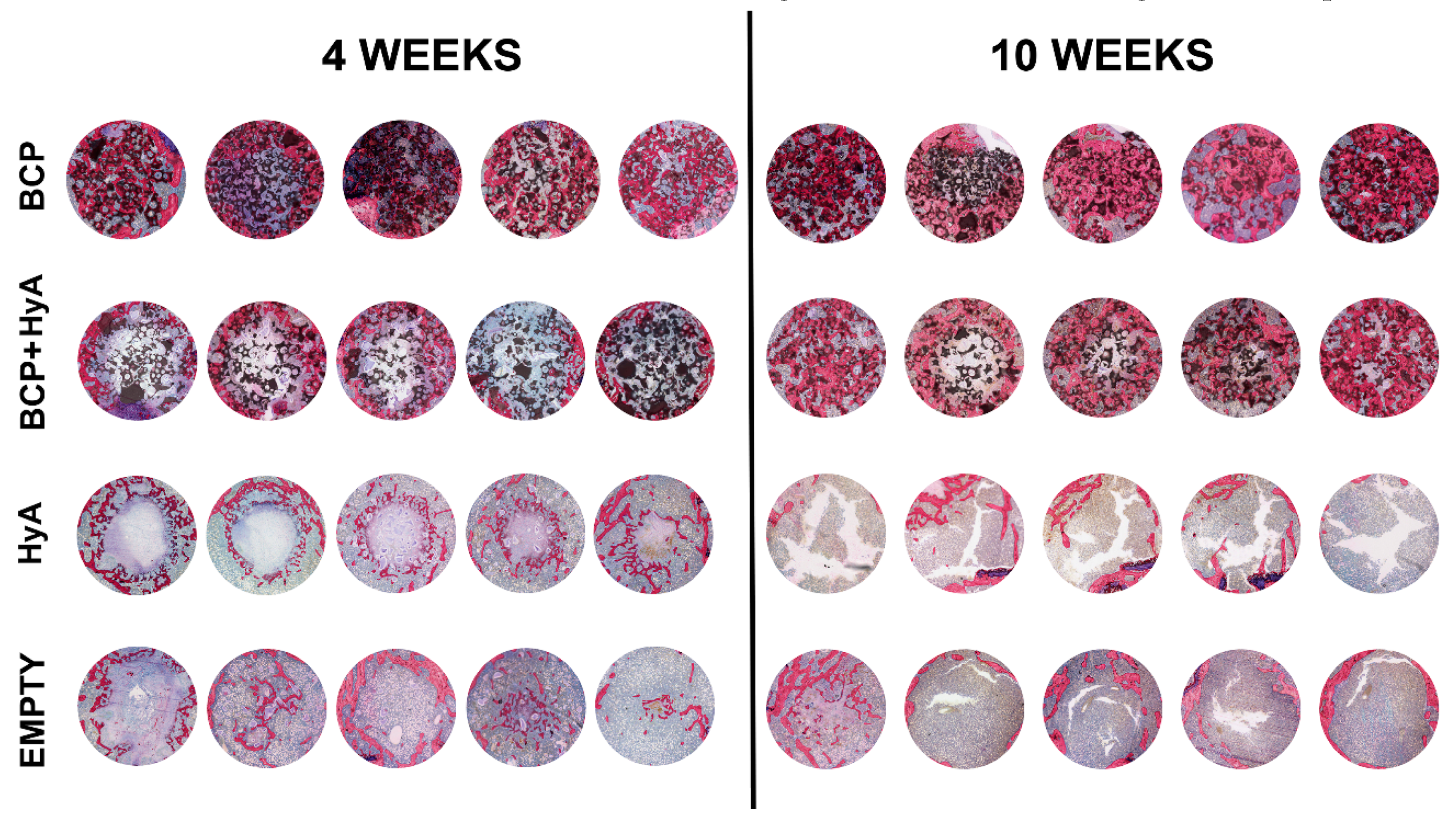
3.2. Qualitative Histological Evaluation
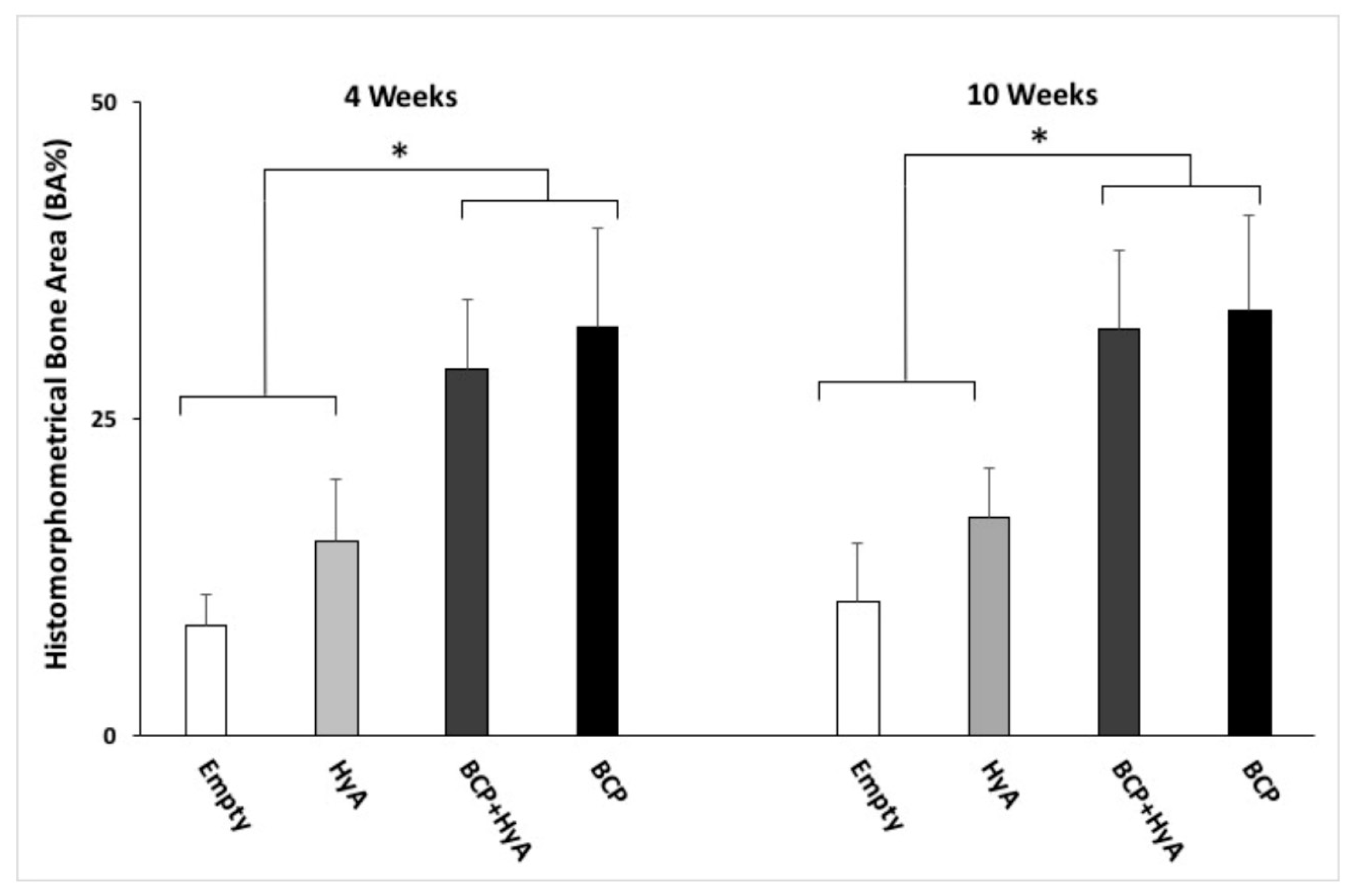
3.3. Quantitative Histomorphometrical Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pihlstrom, B.L.; Michalowicz, B.S.; Johnson, N.W. Periodontal diseases. Lancet 2005, 366, 1809–1820. [Google Scholar] [CrossRef]
- Offenbacher, S. Periodontal diseases: Pathogenesis. Ann. Periodontol. 1996, 1, 821–878. [Google Scholar] [CrossRef] [PubMed]
- Van Dyke, T.; Serhan, C. Resolution of inflammation: A new paradigm for the pathogenesis of periodontal diseases. J. Dent. Res. 2003, 82, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, M.A.; Aichelmann-Reidy, M.E.; Branch-Mays, G.L. Regeneration of periodontal tissue: Bone replacement grafts. Dent. Clin. N. Am. 2010, 54, 55–71. [Google Scholar] [CrossRef]
- Shiau, H.J.; Reynolds, M.A. Sex differences in destructive periodontal disease: Exploring the biologic basis. J. Periodontol. 2010, 81, 1505–1517. [Google Scholar] [CrossRef]
- Kao, R.T.; Nares, S.; Reynolds, M.A. Periodontal regeneration-intrabony defects: A systematic review from the AAP regeneration workshop. J. Periodontol. 2015, 86, S77–S104. [Google Scholar] [CrossRef]
- Rosenberg, E.; Rose, L.F. Biologic and clinical considerations for autografts and allografts in periodontal regeneration therapy. Dent. Clin. N. Am. 1998, 42, 467–490. [Google Scholar]
- Sen, M.K.; Miclau, T. Autologous iliac crest bone graft: Should it still be the gold standard for treating nonunions? Injury 2007, 38, S75–S80. [Google Scholar] [CrossRef]
- Tomford, W.W.; Thongphasuk, J.; Mankin, H.; Ferraro, M. Frozen musculoskeletal allografts. A study of the clinical incidence and causes of infection associated with their use. J. Bone Jt. Surg. Am. 1990, 72, 1137–1143. [Google Scholar] [CrossRef]
- Sutherland, D.; Bostrom, M. Grafts and bone graft substitutes. In Bone Regeneration and Repair; Springer: Berlin/Heidelberg, Germany, 2005; pp. 133–156. [Google Scholar]
- Knaack, D.; Goad, M.; Aiolova, M.; Rey, C.; Tofighi, A.; Chakravarthy, P.; Lee, D.D. Resorbable calcium phosphate bone substitute. J. Biomed. Mater. Res. 1998, 43, 399–409. [Google Scholar] [CrossRef]
- Kolk, A.; Handschel, J.; Drescher, W.; Rothamel, D.; Kloss, F.; Blessmann, M.; Heiland, M.; Wolff, K.D.; Smeets, R. Current trends and future perspectives of bone substitute materials–from space holders to innovative biomaterials. J. Cranio-Maxillofac. Surg. 2012, 40, 706–718. [Google Scholar] [CrossRef] [PubMed]
- Giuliani, A.; Manescu, A.; Mohammadi, S.; Mazzoni, S.; Piattelli, A.; Mangano, F.; Iezzi, G.; Mangano, C. Quantitative Kinetics Evaluation of Blocks Versus Granules of Biphasic Calcium Phosphate Scaffolds (HA/beta-TCP 30/70) by Synchrotron Radiation X-ray Microtomography: A Human Study. Implant Dent. 2016, 25, 6–15. [Google Scholar] [CrossRef] [PubMed]
- Finkemeier, C.G. Bone-grafting and bone-graft substitutes. J Bone Jt. Surg. Am. 2002, 84, 454–464. [Google Scholar] [CrossRef]
- Kim, J.; Kim, I.S.; Cho, T.H.; Lee, K.B.; Hwang, S.J.; Tae, G.; Noh, I.; Lee, S.H.; Park, Y.; Sun, K. Bone regeneration using hyaluronic acid-based hydrogel with bone morphogenic protein-2 and human mesenchymal stem cells. Biomaterials 2007, 28, 1830–1837. [Google Scholar] [CrossRef]
- Diker, N.; Koroglu, T.; Gulsever, S.; Akcay, E.Y.; Oguz, Y. Effects of hyaluronic acid and alloplastic bone graft combination on bone regeneration. Int. J. Oral Maxillofac. Surg. 2015, 44, e55. [Google Scholar] [CrossRef]
- Prestwich, G.D. Hyaluronic acid-based clinical biomaterials derived for cell and molecule delivery in regenerative medicine. J. Control. Release 2011, 155, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Patterson, J.; Siew, R.; Herring, S.W.; Lin, A.S.; Guldberg, R.; Stayton, P.S. Hyaluronic acid hydrogels with controlled degradation properties for oriented bone regeneration. Biomaterials 2010, 31, 6772–6781. [Google Scholar] [CrossRef]
- Aslan, M.; Şimşek, G.; Dayi, E. The effect of hyaluronic acid-supplemented bone graft in bone healing: Experimental study in rabbits. J. Biomater. Appl. 2006, 20, 209–220. [Google Scholar] [CrossRef]
- Hahn, S.K.; Jelacic, S.; Maier, R.V.; Stayton, P.S.; Hoffman, A.S. Anti-inflammatory drug delivery from hyaluronic acid hydrogels. J. Biomater. Sci. Polym. Ed. 2004, 15, 1111–1119. [Google Scholar] [CrossRef]
- Awartani, F.A.; Tatakis, D.N. Interdental papilla loss: Treatment by hyaluronic acid gel injection: A case series. Clin. Oral Investig. 2016, 20, 1775–1780. [Google Scholar] [CrossRef]
- Van der Lubbe, H.; Klein, C.; De Groot, K. A simple method for preparing thin (10 μm) histological sections of undecalcified plastic embedded bone with implants. Stain Technol. 1988, 63, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Contar, C.M.; Sarot, J.R.; Bordini, J., Jr.; Galvao, G.H.; Nicolau, G.V.; Machado, M.A. Maxillary ridge augmentation with fresh-frozen bone allografts. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 2009, 67, 1280–1285. [Google Scholar] [CrossRef] [PubMed]
- Lobo, S.E.; Livingston Arinzeh, T. Biphasic calcium phosphate ceramics for bone regeneration and tissue engineering applications. Materials 2010, 3, 815–826. [Google Scholar] [CrossRef]
- Fellah, B.H.; Gauthier, O.; Weiss, P.; Chappard, D.; Layrolle, P. Osteogenicity of biphasic calcium phosphate ceramics and bone autograft in a goat model. Biomaterials 2008, 29, 1177–1188. [Google Scholar] [CrossRef]
- Nery, E.B.; Legeros, R.Z.; Lynch, K.L.; Lee, K. Tissue response to biphasic calcium phosphate ceramic with different ratios of HA/βTCP in periodontal osseous defects. J. Periodontol. 1992, 63, 729–735. [Google Scholar] [CrossRef]
- Jelusic, D.; Zirk, M.L.; Fienitz, T.; Plancak, D.; Puhar, I.; Rothamel, D. Monophasic ß-TCP vs. biphasic HA/ß--TCP in two-stage sinus floor augmentation procedures—A prospective randomized clinical trial. Clin. Oral Implants Res. 2016, 28, e175–e183. [Google Scholar] [CrossRef]
- Huang, L.; Cheng, Y.; Koo, P.; Lee, K.M.; Qin, L.; Cheng, J.C.Y.; Kumta, S.M. The effect of hyaluronan on osteoblast proliferation and differentiation in rat calvarial—Derived cell cultures. J. Biomed. Mater. Res. 2003, 66, 880–884. [Google Scholar] [CrossRef]
- Kuo, J.; Prestwich, G. Hyaluronic acid. In Comprehensive Biomaterials; Elsevier: Amsterdam, The Netherlands, 2011. [Google Scholar]
- ELkarargy, A. Alveolar sockets preservation using hydroxyapatite/beta tricalcium phosphate with hyaluronic acid (histomorphometric study). J. Am. Sci. 2013, 9, 556–563. [Google Scholar]
- Sasaki, T.; Watanabe, C. Stimulation of osteoinduction in bone wound healing by high-molecular hyaluronic acid. Bone 1995, 16, 9–15. [Google Scholar] [CrossRef]
- Stern, M.; Schmidt, B.; Dodson, T.B.; Stern, R.; Kaban, L.B. Fetal cleft lip repair in rabbits: Histology and role of hyaluronic acid. J. Oral Maxillofac. Surg. 1992, 50, 263–268. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Groups (n = 10 Per Group Per Time Period) | Bone Healing Time | |||
|---|---|---|---|---|
| 4 Weeks | 10 Weeks | |||
| Newly Formed Bone Area (%) | Remaining BCP (%) | Newly Formed Bone Area (%) | Remaining BCP (%) | |
| BCP | 32.2 ± 7.7 | 28.7 ± 7.6 | 33.5 ± 7.4 | 23.9 ± 6.3 |
| BCP + HyA | 28.8 ± 5.6 | 22.6 ± 5.1 | 32.0 ± 6.2 | 21.6 ± 3.7 |
| HyA | 15.3 ± 4.9 | - | 17.1 ± 3.9 | - |
| Control | 8.6 ± 2.5 | - | 10.6 ± 4.5 | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmed, A.G.; Awartani, F.A.; Niazy, A.A.; Jansen, J.A.; Alghamdi, H.S. A Combination of Biphasic Calcium Phosphate (Maxresorb®) and Hyaluronic Acid Gel (Hyadent®) for Repairing Osseous Defects in a Rat Model. Appl. Sci. 2020, 10, 1651. https://doi.org/10.3390/app10051651
Ahmed AG, Awartani FA, Niazy AA, Jansen JA, Alghamdi HS. A Combination of Biphasic Calcium Phosphate (Maxresorb®) and Hyaluronic Acid Gel (Hyadent®) for Repairing Osseous Defects in a Rat Model. Applied Sciences. 2020; 10(5):1651. https://doi.org/10.3390/app10051651
Chicago/Turabian StyleAhmed, Abeer G., Fatin A. Awartani, Abdurahman A. Niazy, John A. Jansen, and Hamdan S. Alghamdi. 2020. "A Combination of Biphasic Calcium Phosphate (Maxresorb®) and Hyaluronic Acid Gel (Hyadent®) for Repairing Osseous Defects in a Rat Model" Applied Sciences 10, no. 5: 1651. https://doi.org/10.3390/app10051651
APA StyleAhmed, A. G., Awartani, F. A., Niazy, A. A., Jansen, J. A., & Alghamdi, H. S. (2020). A Combination of Biphasic Calcium Phosphate (Maxresorb®) and Hyaluronic Acid Gel (Hyadent®) for Repairing Osseous Defects in a Rat Model. Applied Sciences, 10(5), 1651. https://doi.org/10.3390/app10051651