Geometrical Calibration of a 2.5D Periapical Radiography System

 ,
,
Abstract
1. Introduction
2. Materials and Methods
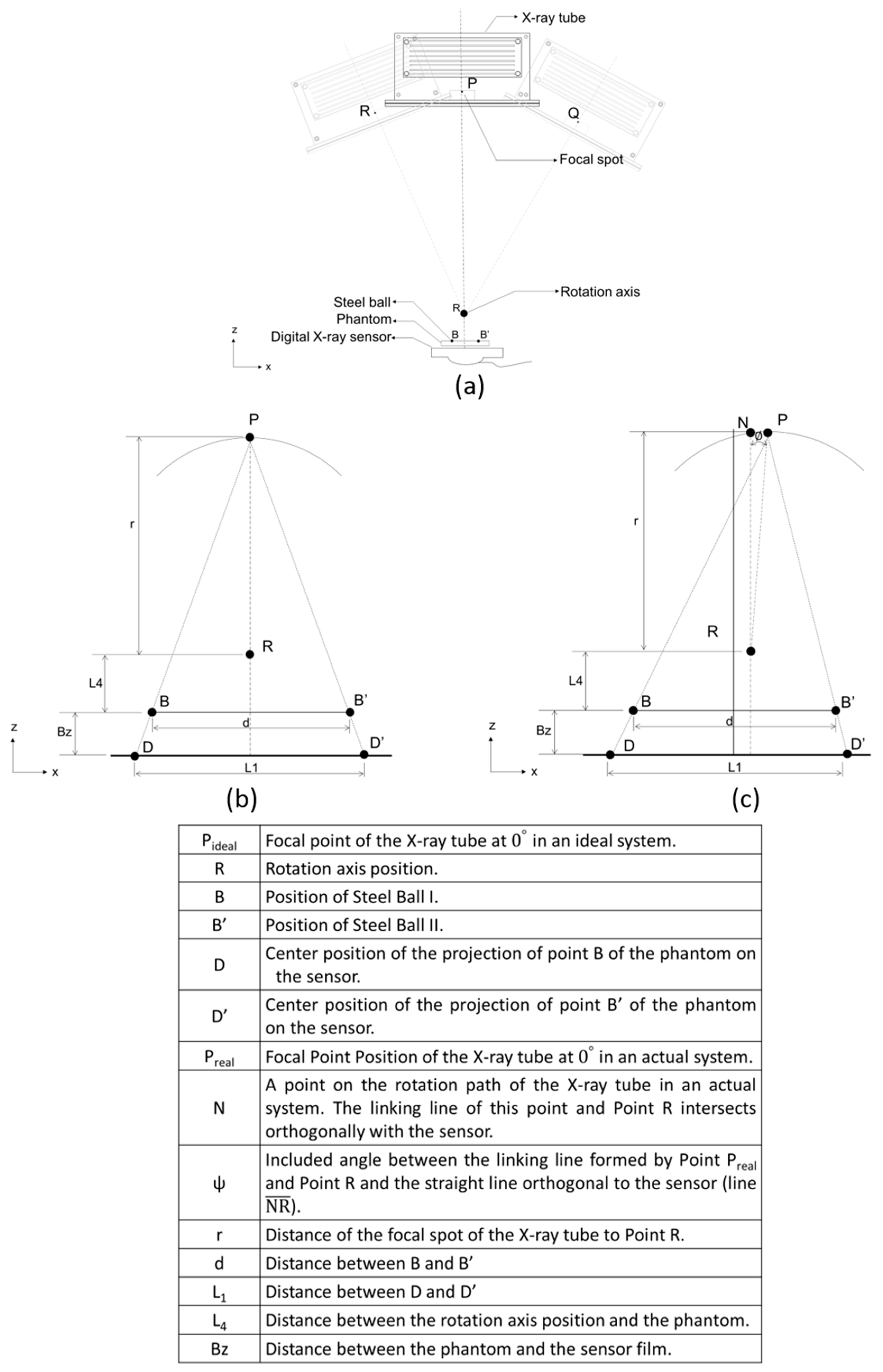
2.1. 2.5D Periapical Radiography System
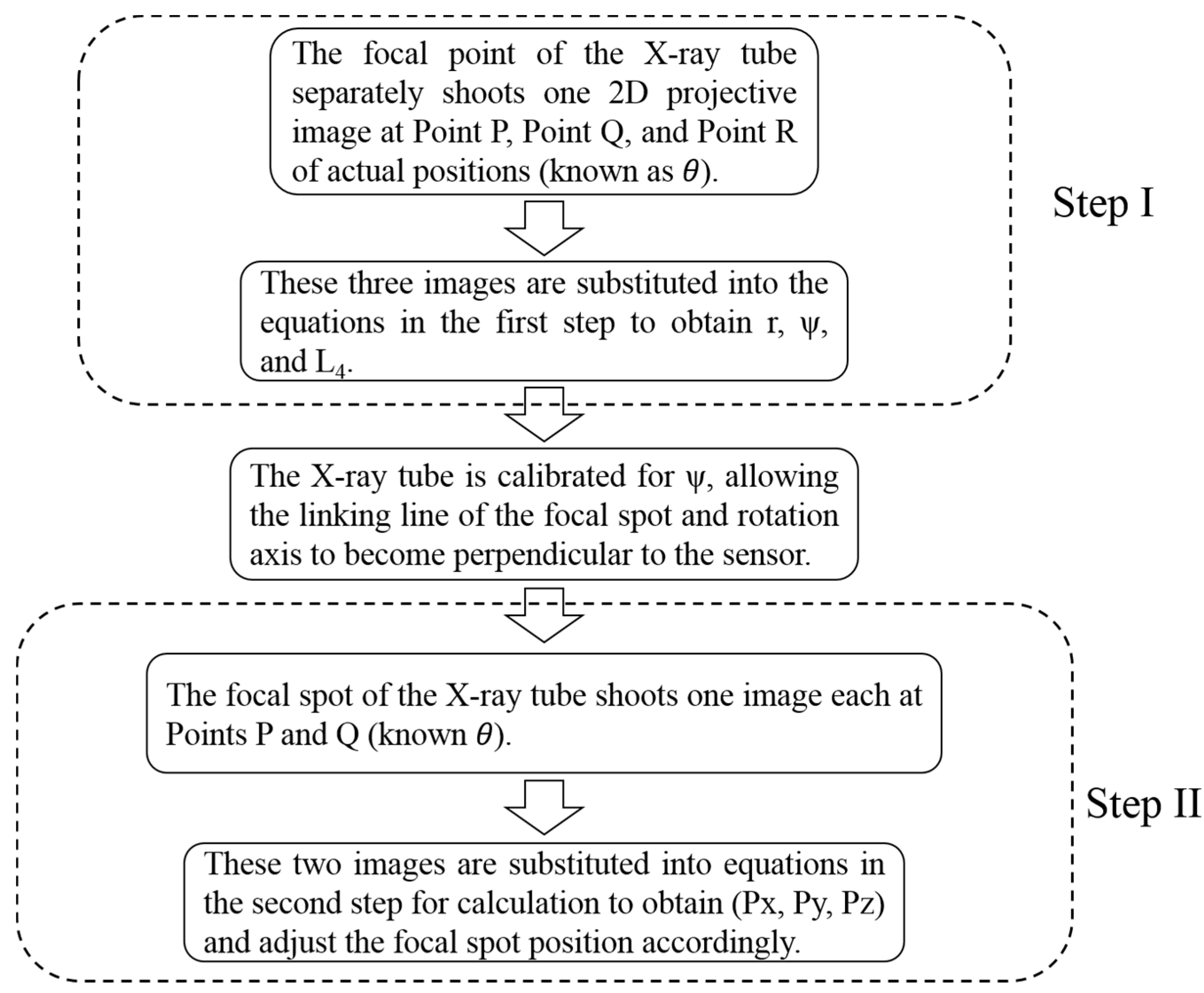
2.2. Geometric Calibration Algorithm
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
Appendix A
References
- Fava, L.; Dummer, P. Periapical radiographic techniques during endodontic diagnosis and treatment. Int. Endod. J. 1997, 30, 250–261. [Google Scholar] [CrossRef]
- Vandenberghe, B.; Jacobs, R.; Bosmans, H. Modern dental imaging: A review of the current technology and clinical applications in dental practice. Eur. Radiol. 2010, 20, 2637–2655. [Google Scholar] [CrossRef] [PubMed]
- Fu, H.-M.; Chueh, H.-S.; Tsai, W.-K.; Chen, J.-C.J.B.E.A. Development and evaluation of reconstruction methods for an in-house designed cone-beam micro-CT imaging system. Biomed. Eng. Appl. Basis Commun. 2006, 18, 270–275. [Google Scholar] [CrossRef]
- Kiljunen, T.; Kaasalainen, T.; Suomalainen, A.; Kortesniemi, M. Dental cone beam CT: A review. Physica Med. 2015, 31, 844–860. [Google Scholar] [CrossRef] [PubMed]
- Pauwels, R.; Araki, K.; Siewerdsen, J.; Thongvigitmanee, S. Technical aspects of dental CBCT: State of the art. Dentomaxillofacial Radiol. 2014, 44, 20140224. [Google Scholar] [CrossRef] [PubMed]
- Metsälä, E.; Henner, A.; Ekholm, M. Quality assurance in digital dental imaging: A systematic review. Acta Odontol. Scand. 2014, 72, 362–371. [Google Scholar] [CrossRef]
- Patel, S.; Dawood, A.; Whaites, E.; Pitt Ford, T. New dimensions in endodontic imaging: Part 1. Conventional and alternative radiographic systems. Int. Endod. J. 2009, 42, 447–462. [Google Scholar] [CrossRef]
- Liao, C.-W.; Hsieh, C.-J.; Huang, H.-L.; Fuh, L.-J.; Kuo, C.-W.; Lin, Y.-b.; Chen, J.-C.; Hsu, J.-T.J.B.E.A. Prototype of a 2.5 D periapical radiography system using an intraoral computed tomosynthesis approach. Biomed. Eng. Appl. Basis Commun. 2018, 30, 1850004. [Google Scholar] [CrossRef]
- Shan, J.; Tucker, A.; Gaalaas, L.; Wu, G.; Platin, E.; Mol, A.; Lu, J.; Zhou, O.J.D.R. Stationary intraoral digital tomosynthesis using a carbon nanotube X-ray source array. Dentomaxillofacial Radiol. 2015, 44, 20150098. [Google Scholar] [CrossRef]
- Inscoe, C.R.; Wu, G.; Soulioti, D.E.; Platin, E.; Mol, A.; Gaalaas, L.R.; Anderson, M.R.; Tucker, A.W.; Boyce, S.; Shan, J. Stationary intraoral tomosynthesis for dental imaging. In Proceedings of the Medical Imaging 2017: Physics of Medical Imaging, Orlando, FL, USA, 13–16 February 2017; p. 1013203. [Google Scholar]
- Inscoe, C.R.; Platin, E.; Mauriello, S.M.; Broome, A.; Mol, A.; Gaalaas, L.R.; Regan Anderson, M.W.; Puett, C.; Lu, J.; Zhou, O.J.M.p. Characterization and preliminary imaging evaluation of a clinical prototype stationary intraoral tomosynthesis system. Med. Phys. 2018, 45, 5172–5185. [Google Scholar] [CrossRef]
- Liao, C.-W.; Huang, K.-J.; Chen, J.-C.; Kuo, C.-W.; Wu, Y.-Y.; Hsu, J.-T. A Prototype Intraoral Periapical Sensor with High Frame Rates for a 2.5 D Periapical Radiography System. Appl. Bionics Biomech. 2019, 2019. [Google Scholar] [CrossRef] [PubMed]
- Xiang, Q.; Wang, J.; Cai, Y. A geometric calibration method for cone beam CT system. In Proceedings of the Eighth International Conference on Digital Image Processing (ICDIP 2016), Chengu, China, 20–22 May 2016; p. 100333G. [Google Scholar]
- Zhao, J.; Hu, X.; Zou, J.; Hu, X.J.S. Geometric parameters estimation and calibration in cone-beam micro-CT. Sensor 2015, 15, 22811–22825. [Google Scholar] [CrossRef] [PubMed]
- Johnston, S.M.; Johnson, G.A.; Badea, C.T.J.M.p. Geometric calibration for a dual tube/detector micro-CT system. Med. Phys. 2008, 35, 1820–1829. [Google Scholar] [CrossRef]
- Von Smekal, L.; Kachelrieß, M.; Stepina, E.; Kalender, W.A.J.M.p. Geometric misalignment and calibration in cone-beam tomography: Geometric misalignment and calibration in cone-beam tomography. Med. Phys. 2004, 31, 3242–3266. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Yang, Y.; Chen, Z.J.O.E. Geometric estimation method for x-ray digital intraoral tomosynthesis. Opt. Eng. 2016, 55, 063105. [Google Scholar] [CrossRef]
- Richard, L.; Webber, W.-S. Self-calibrated tomosynthetic, radiographic-imaging system, method, and device. U.S. Patent No 5,359,637, 25 October 1994. [Google Scholar]
- Yang, Y.; Li, L.; Chen, Z.; Chang, M. Geometrical calibration method for x-ray intra-oral digital tomosynthesis. In Proceedings of the 2014 IEEE Nuclear Science Symposium and Medical Imaging Conference (NSS/MIC), Seattle, WA, USA, 8–15 November 2014; pp. 1–4. [Google Scholar]
- Li, L.; Chen, Z.; Zhao, Z.; Wu, D. X-ray digital intra-oral tomosynthesis for quasi-three-dimensional imaging: System, reconstruction algorithm, and experiments. Opt. Eng. 2013, 52, 013201. [Google Scholar] [CrossRef]
- Sato, K.; Ohnishi, T.; Sekine, M.; Haneishi, H. Geometry calibration between X-ray source and detector for tomosynthesis with a portable X-ray system. Int. J. Comput. Assisted Radiol. Surg. 2017, 12, 707–717. [Google Scholar] [CrossRef][Green Version]
- Miao, H.; Wu, X.; Zhao, H.; Liu, H. A phantom-based calibration method for digital x-ray tomosynthesis. J. X-Ray Sci. Technol. 2012, 20, 17–29. [Google Scholar] [CrossRef]
- Chtcheprov, P.; Hartman, A.; Shan, J.; Lee, Y.Z.; Zhou, O.; Lu, J. Optical geometry calibration method for free-form digital tomosynthesis. In Proceedings of the Medical Imaging 2016: Physics of Medical Imaging, San Diego, CA, USA, 27 February–3 March 2016; p. 978365. [Google Scholar]
- Fayad, M.I.; Nair, M.; Levin, M.D.; Benavides, E.; Rubinstein, R.A.; Barghan, S.; Hirschberg, C.S.; Ruprecht, A. AAE and AAOMR joint position statement: Use of cone beam computed tomography in endodontics 2015 update. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 120, 508–512. [Google Scholar] [CrossRef]
- Hayakawa, Y.; Yamamoto, K.; Kousuge, Y.; Kobayashi, N.; Wakoh, M.; Sekiguchi, H.; Yakushiji, M.; Farman, A. Clinical validity of the interactive and low-dose three-dimensional dento-alveolar imaging system, Tuned-Aperture Computed Tomography. Bull. Tokyo Dent. Coll. 2003, 44, 159–167. [Google Scholar] [CrossRef]
- Groenhuis, R.A.; Webber, R.L.; Ruttimann, U.E.J.O.S. Computerized tomosynthesis of dental tissues. Oral Med. Oral Pathol. 1983, 56, 206–214. [Google Scholar] [CrossRef]
- Grant, D.G. Tomosynthesis: A three-dimensional radiographic imaging technique. IEEE Trans. Biomed. Eng. 1972, 1, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, C.M.; Franetzki, M.; Denig, T.; Muhling, J.; Hassfeld, S. Digital tomosynthesis-experiences with a new imaging device for the dental field. Clin. Oral Investig. 2003, 7, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Rashedi, B.; Tyndall, D.A.; Ludlow, J.B.; Chaffee, N.R.; Guckes, A. Tuned aperture computed tomography (TACT®) for cross-sectional implant site assessment in the posterior mandible. J. Prosthodontics 2003, 12, 176–186. [Google Scholar] [CrossRef]
- Harase, Y.; Araki, K.; Okano, T. Diagnostic ability of extraoral tuned aperture computed tomography (TACT) for impacted third molars. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2005, 100, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Limrachtamorn, S.; Edge, M.; Gettleman, L.; Scheetz, J.; Farman, A. Array geometry for assessment of mandibular implant position using tuned aperture computed tomography (TACT™). Dentomaxillofacial Radiol. 2004, 33, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Harase, Y.; Araki, K.; Okano, T. Accuracy of extraoral tuned aperture computed tomography (TACT) for proximal caries detection. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2006, 101, 791–796. [Google Scholar] [CrossRef]
- Yang, K.; Kwan, A.L.; Miller, D.F.; Boone, J. A geometric calibration method for cone beam CT systems. Med. Phys. 2006, 33, 1695–1706. [Google Scholar] [CrossRef]
- Sun, Y.; Hou, Y.; Zhao, F.; Hu, J. A calibration method for misaligned scanner geometry in cone-beam computed tomography. NDT E Int. 2006, 39, 499–513. [Google Scholar] [CrossRef]
- Wang, X.; Mainprize, J.G.; Kempston, M.P.; Mawdsley, G.E.; Yaffe, M.J. Digital breast tomosynthesis geometry calibration. In Proceedings of the Medical Imaging 2007: Physics of Medical Imaging, San Diego, CA, USA, 18–22 February 2007; p. 65103B. [Google Scholar]
- Claus, B.E.H.; Opsahl-Ong, B.; Yavuz, M. Method, apparatus, and medium for calibration of tomosynthesis system geometry using fiducial markers with non-determined position. U.S. Patent No. 6,888,924, 3 May 2005. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Test Number | L4 (mm) | ψ (°) | r (mm) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Ideal | Estimate | Error (%) | Ideal | Estimate | Error (%) | Ideal | Estimate | Error (%) | |
| 1 | 5.0 | 5.00004399 | 0.00088 | 3.0 | 3.00034641 | 0.01155 | 335 | 335.000001 | 0.00000 |
| 2 | 6.5 | 6.499985761 | −0.00022 | 2.8 | 2.79995015 | −0.00178 | 332 | 331.5000007 | 0.00000 |
| 3 | 4.1 | 4.100159545 | 0.00389 | 3.7 | 3.70041803 | 0.01130 | 337 | 337.2999967 | 0.00000 |
| 4 | 5.3 | 5.300042976 | 0.00081 | 1.3 | 1.300326732 | 0.02513 | 334 | 333.8000022 | 0.00000 |
| 5 | 4.2 | 4.199978173 | −0.00052 | 5.9 | 5.899961593 | −0.00065 | 333 | 332.6999966 | 0.00000 |
| Group 1 | |||
| Parameter | Ideal | Estimate | Error (%) |
| Pz | 350 | 350.000001 | 0.00000 |
| B’x | −12.1756613 | −12.1756622 | 0.00001 |
| B’y | 1.6572935 | 1.6572934 | −0.00001 |
| Bx | 7.8076613 | 7.8076605 | −0.00001 |
| By | 0.8407065 | 0.8407063 | −0.00002 |
| Px | −2.438 | −2.4380285 | 0.00117 |
| Py | 6.892 | 6.8919944 | −0.00008 |
| Group 2 | |||
| Parameter | Ideal | Estimate | Error (%) |
| Pz | 350 | 349.999999 | 0.00000 |
| B’x | 9.25091935 | 9.25091994 | 0.00001 |
| B’y | −0.13745354 | −0.1374539 | 0.00026 |
| Bx | −10.7109194 | −10.7109188 | −0.00001 |
| By | 1.09745354 | 1.09745319 | −0.00003 |
| Px | −0.54 | −0.5399793 | −0.00383 |
| Py | 0.19 | 0.1899876 | −0.00653 |
| Group 3 | |||
| Parameter | Ideal | Estimate | Error (%) |
| Pz | 350 | 350.000001 | 0.00000 |
| B’x | −12.1756613 | −12.1756622 | 0.00001 |
| B’y | 1.65729352 | 1.65729336 | −0.00001 |
| Bx | 7.80766134 | 7.80766052 | −0.00001 |
| By | 0.84070648 | 0.84070632 | −0.00002 |
| Px | −2.438 | −2.43802854 | 0.00117 |
| Py | 6.892 | 6.8919944 | −0.00008 |
| Group 4 | |||
| Parameter | Ideal | Estimate | Error (%) |
| Pz | 370.83 | 370.829997 | 0.00000 |
| B’x | 9.25091935 | 9.25092049 | 0.00001 |
| B’y | −0.13745354 | −0.13745374 | 0.00015 |
| Bx | −10.7109194 | −10.7109182 | −0.00001 |
| By | 1.09745354 | 1.09745334 | −0.00002 |
| Px | −0.54 | −0.53995807 | −0.00776 |
| Py | 0.19 | 0.18999275 | −0.00382 |
| Group 5 | |||
| Parameter | Ideal | Estimate | Error (%) |
| Pz | 350 | 349.999997 | 0.00000 |
| B’x | 7.50455987 | 7.50456092 | 0.00001 |
| B’y | 0.81019259 | 0.81019316 | 0.00007 |
| Bx | −12.4845599 | −12.4845588 | −0.00001 |
| By | 1.46980741 | 1.46980797 | 0.00004 |
| Px | −2.92 | −2.91996328 | −0.00126 |
| Py | 1.66 | 1.6600196 | 0.00118 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liao, C.-W.; Tsai, M.-T.; Huang, H.-L.; Fuh, L.-J.; Liu, Y.-L.; Su, Z.-T.; Hsu, J.-T. Geometrical Calibration of a 2.5D Periapical Radiography System. Appl. Sci. 2020, 10, 906. https://doi.org/10.3390/app10030906
Liao C-W, Tsai M-T, Huang H-L, Fuh L-J, Liu Y-L, Su Z-T, Hsu J-T. Geometrical Calibration of a 2.5D Periapical Radiography System. Applied Sciences. 2020; 10(3):906. https://doi.org/10.3390/app10030906
Chicago/Turabian StyleLiao, Che-Wei, Ming-Tzu Tsai, Heng-Li Huang, Lih-Jyh Fuh, Yen-Lin Liu, Zhi-Teng Su, and Jui-Ting Hsu. 2020. "Geometrical Calibration of a 2.5D Periapical Radiography System" Applied Sciences 10, no. 3: 906. https://doi.org/10.3390/app10030906
APA StyleLiao, C.-W., Tsai, M.-T., Huang, H.-L., Fuh, L.-J., Liu, Y.-L., Su, Z.-T., & Hsu, J.-T. (2020). Geometrical Calibration of a 2.5D Periapical Radiography System. Applied Sciences, 10(3), 906. https://doi.org/10.3390/app10030906