A Methodology of Health Effects Estimation from Air Pollution in Large Asian Cities

Abstract
:1. Research Purpose
2. Relative Risk Model vs. Correlation Model
2.1. Relative Risk Model
- RR: Relative risk
- α: Coefficient of respiratory disease mortality of Osaka, 1974–1988;
- X: Current annual mean of PM2.5 (µg/m3) (converted from PM10);
- X0: Baseline of PM2.5 = 10 (Converted from the PM10 standard);
- M: A change of air quality from the baseline M = X – X0;
- TR: Total respiratory disease mortality numbers in a city (per 1000 population);
- E: Respiratory disease mortality numbers caused by air pollution in a city (per 1000 population);
- AF: Attributable fraction (the ratio of respiratory disease mortality caused by air pollution).
2.2. Correlation Model
- Y: The number of deaths in the compensation system per 1000 population;
- β: The coefficient of respiratory disease mortality.
3. Methodology of Data Verification
3.1. Health Effect Data—TR, E
3.2. Air Pollutant X and X0
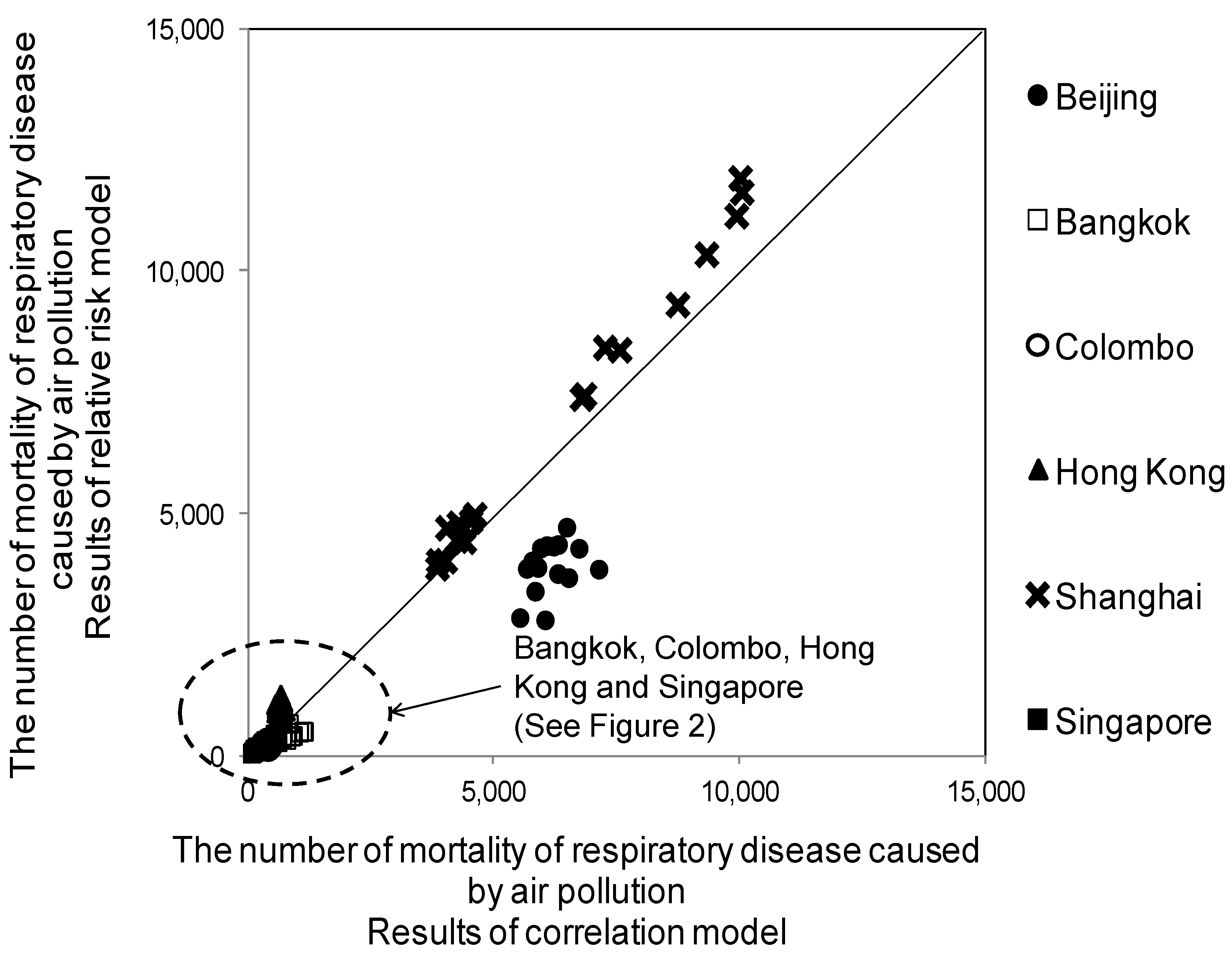
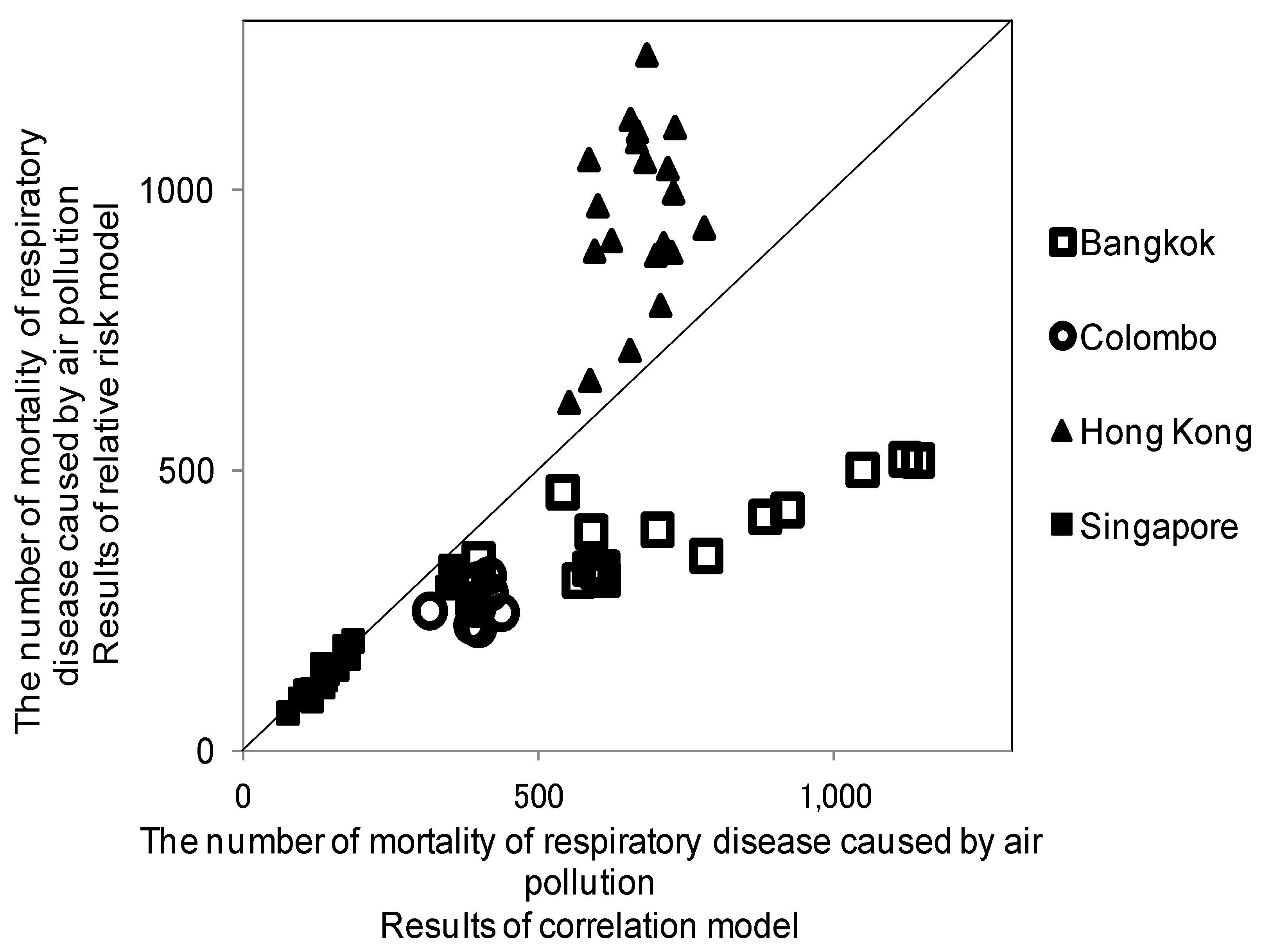
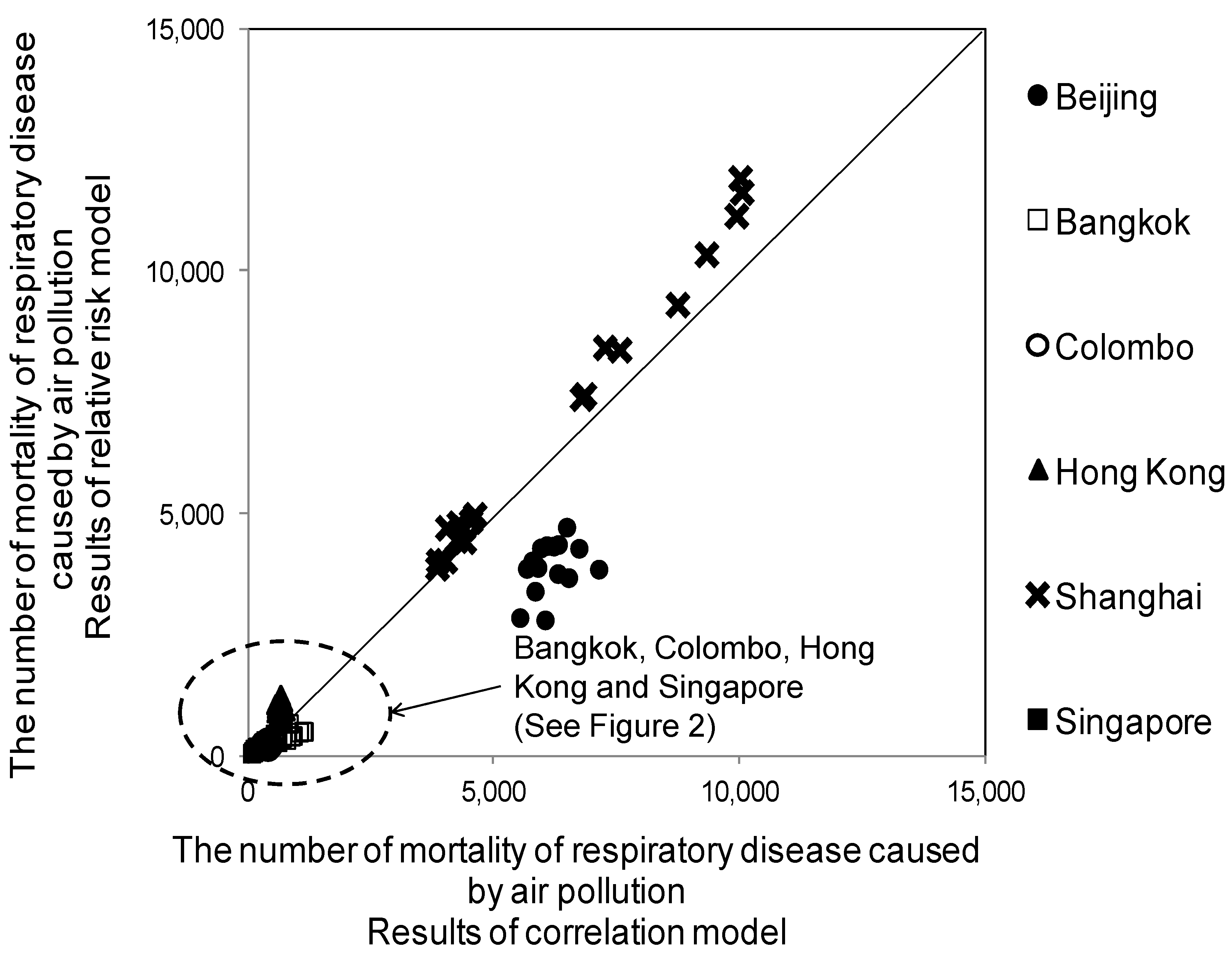
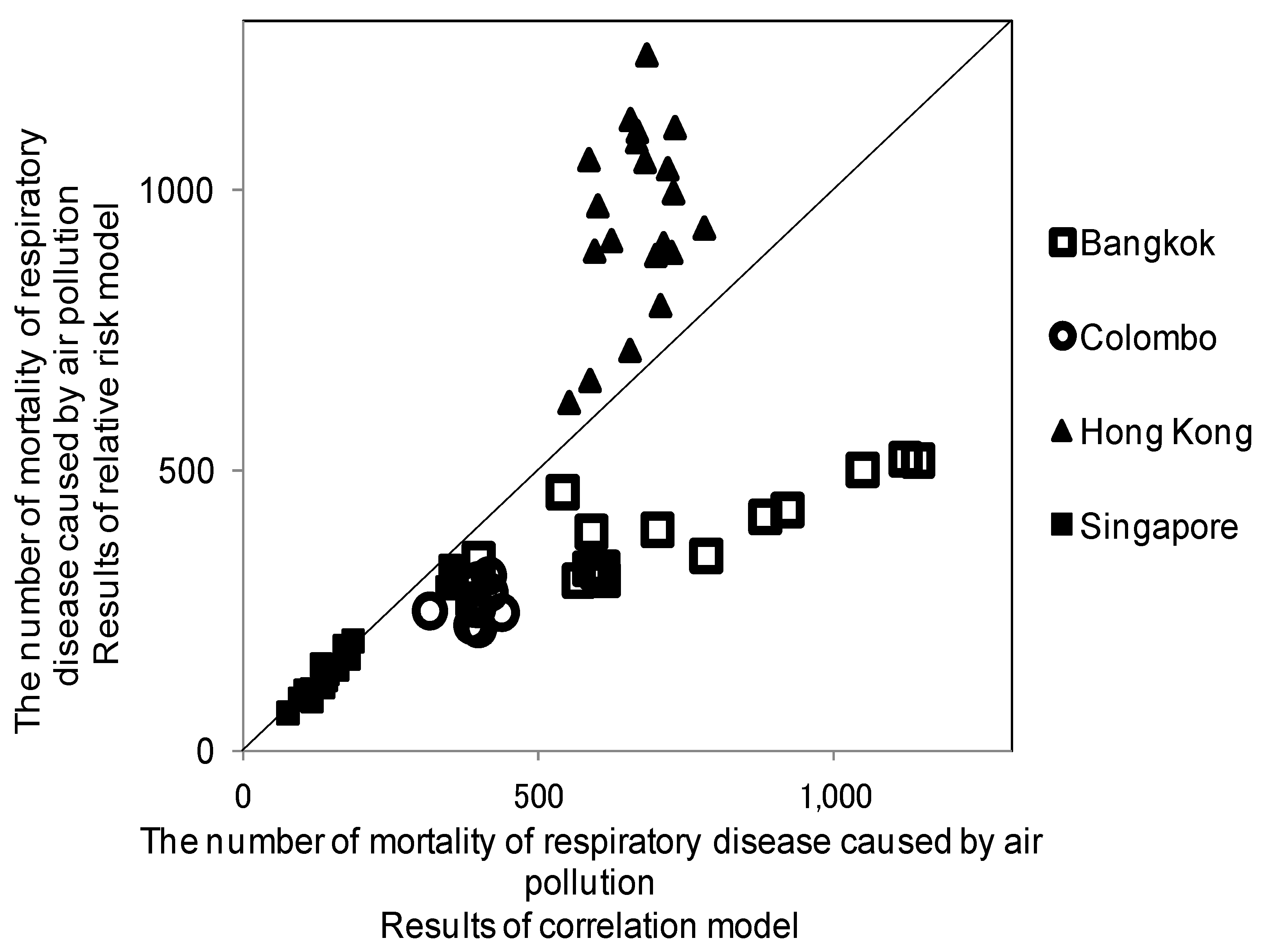
3.3. The Number of Results Expected from the Two Models
4. Results
4.1. Overall Comparison
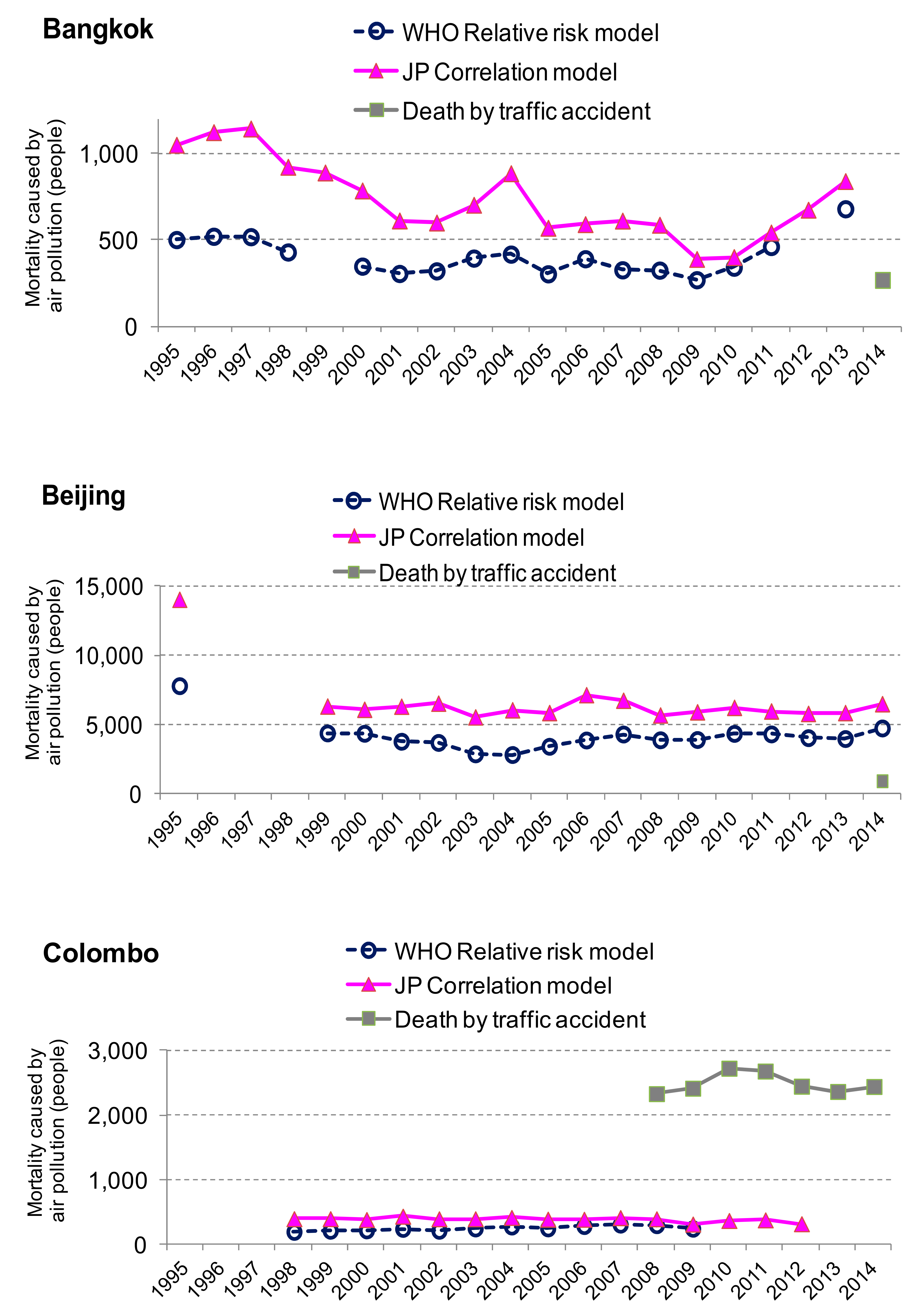
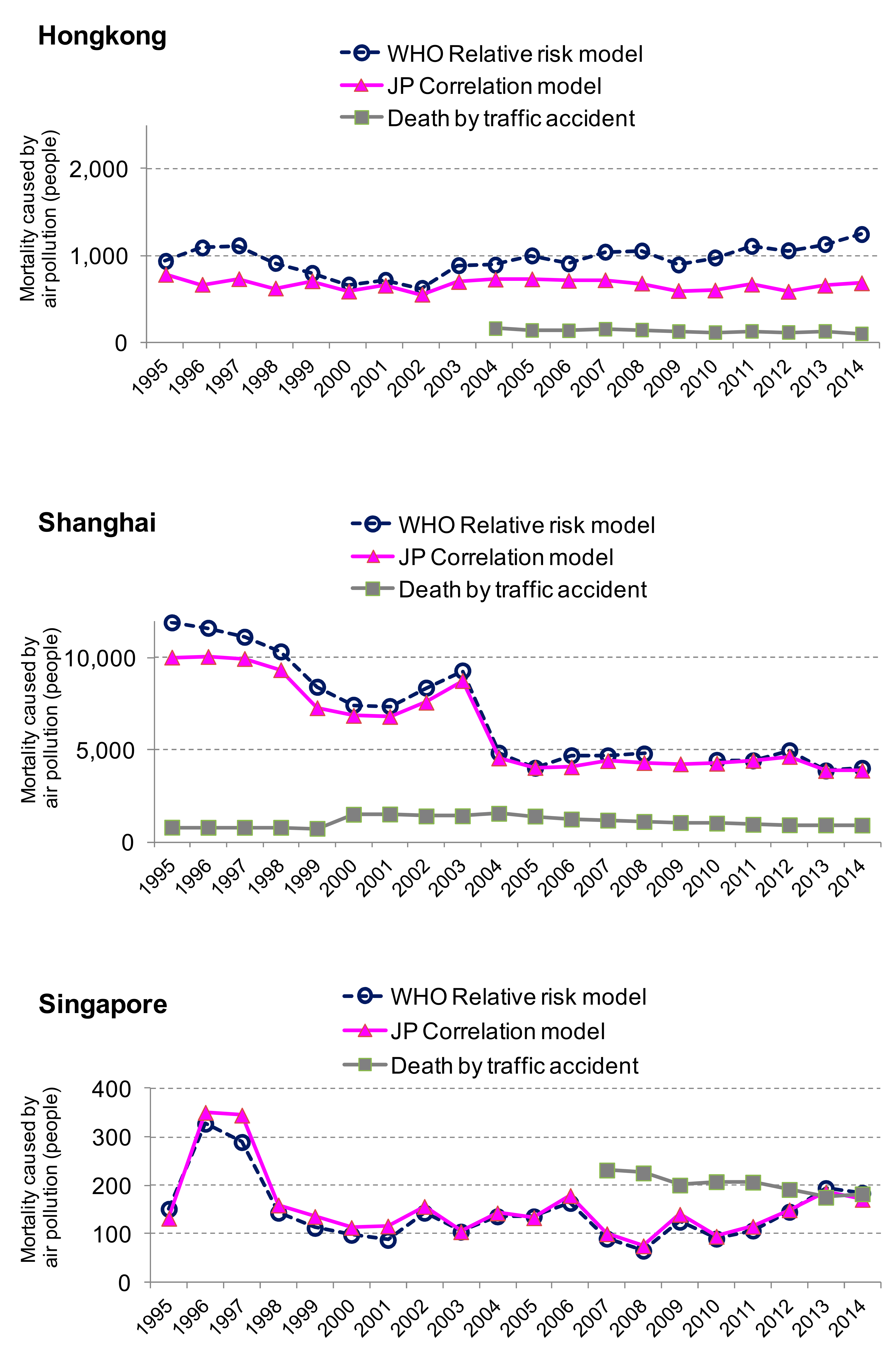
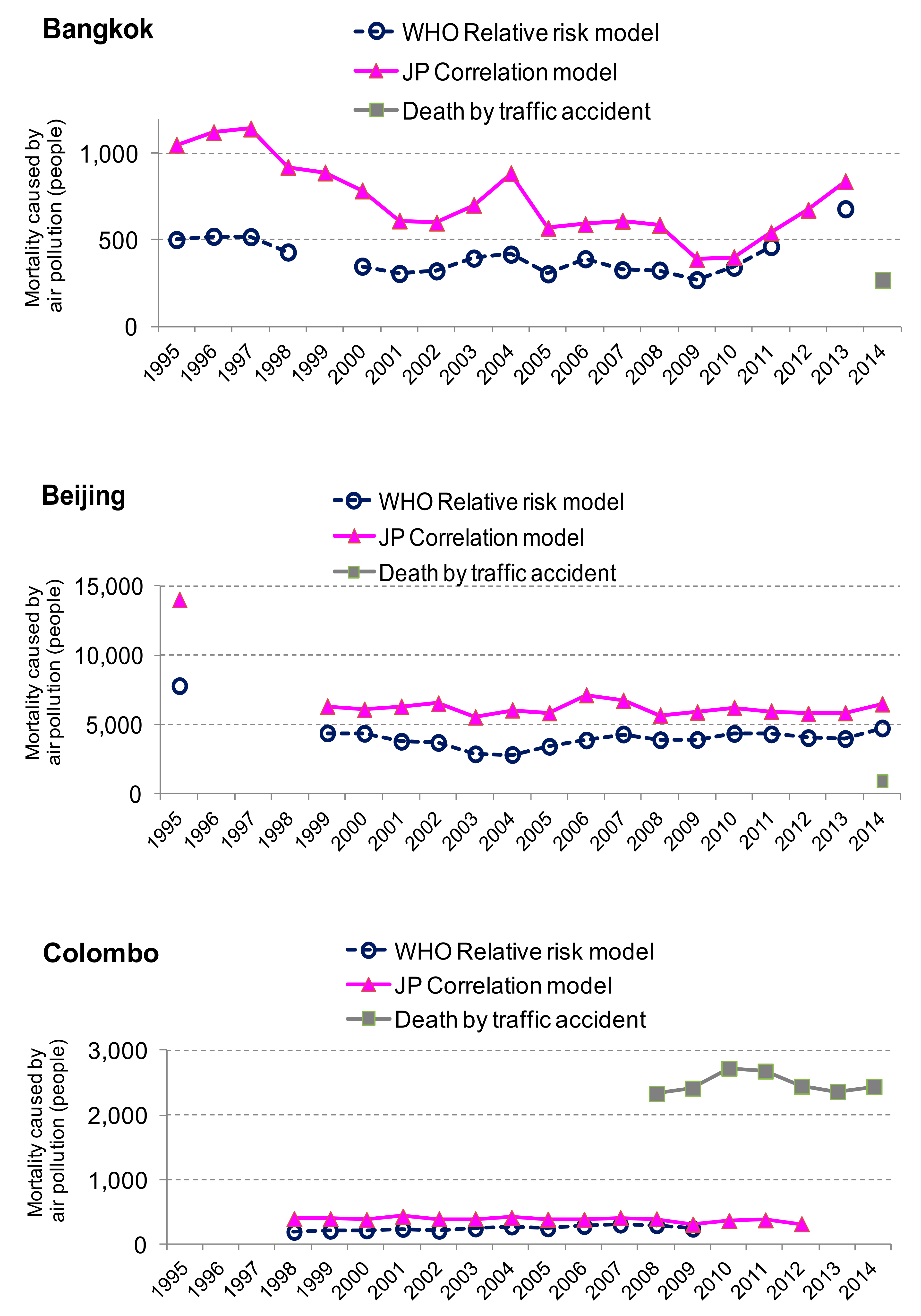
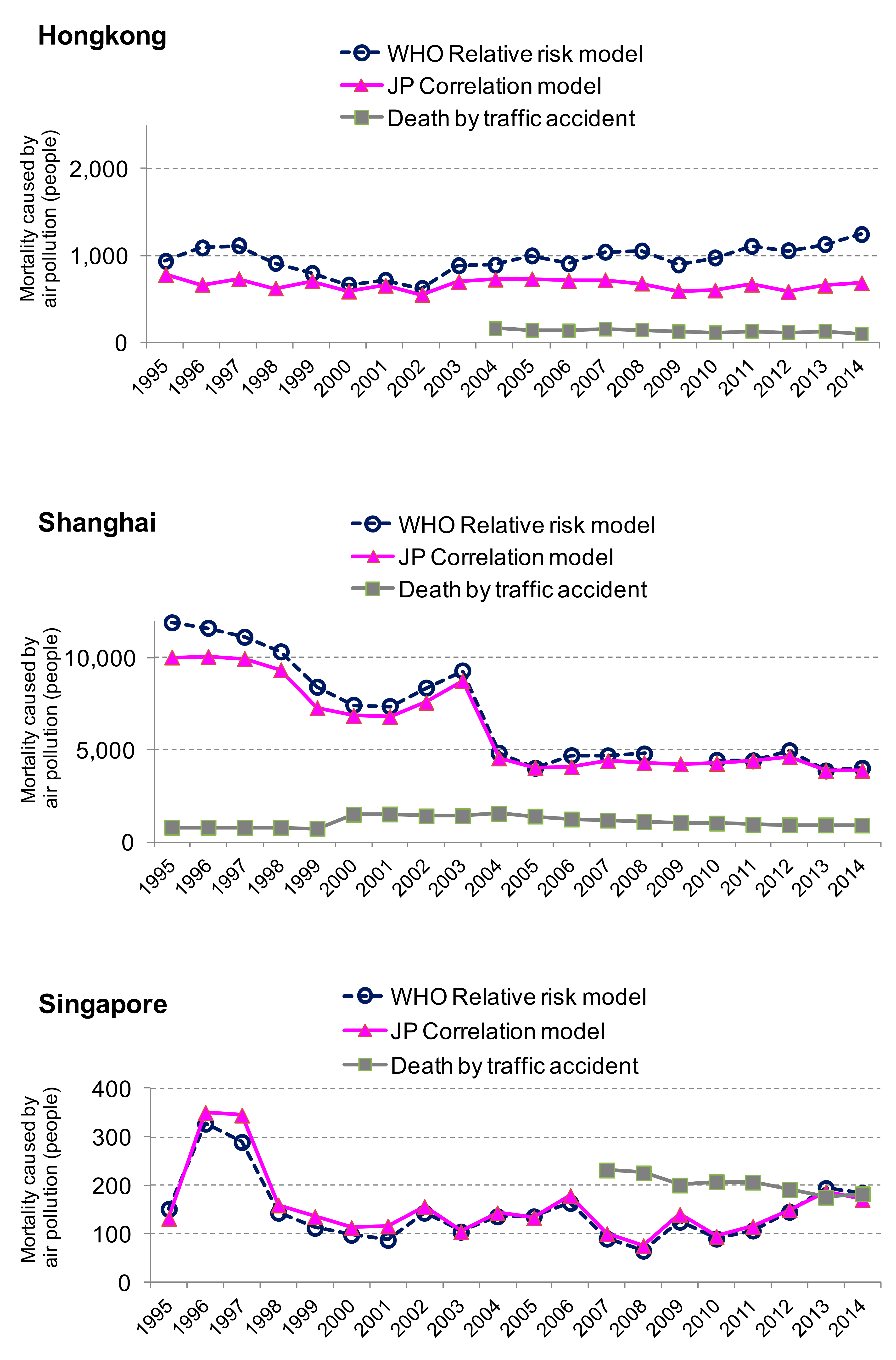
4.2. Comparison by City and by Time Series
5. Conclusions and Further Improvements
- ▪
- This “one fit for all” model should be adjusted by local conditions. Mortality rates will be influenced by the availability of medical treatments/medical care systems in Asia. The correlation model should include indicators of these medical facilities.
- ▪
- The application of the Japanese coefficients for Asia could be improved. The coefficient β should be estimated from all of Japan to increase accuracy. The definition of respiratory disease mortality in statistical yearbooks from each country should be verified.
- ▪
- Due to uncertainty, factors which affect the results should be identified as a next step.
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| Compensation system | Pollution-related Health Damage Compensation and Prevention System |
| COPD | Chronic obstructive pulmonary disease |
| GBD | Global Burden of Disease |
| ICD | International statistical Classification of Disease |
| NO2 | Nitrogen Dioxide |
| PM | Particulate Matter According to the US EPA, particulate matter includes PM10 and PM2.5. |
| SO2 | Sulphur dioxide |
| SPM | Suspended Particulate Matter |
| TSP | Total Suspended Matter |
| USEPA | Environmental Protection Agency in the USA |
| WHO | World Health Organization |
References
- Anderson, H.R. Air pollution and mortality: A history. Atmos. Environ. 2009, 43, 142–152. [Google Scholar] [CrossRef]
- Daly, C. Air pollution and causes of death. Br. J. Pre. Soc. Med. 1959, 13, 14–27. [Google Scholar] [CrossRef]
- Dockery, D.W.; Pope, C.A., III; Xu, X.; Spengler, J.D.; Ware, J.H.; Fay, M.E.; Ferris, B.G., Jr.; Speizer, F.E. An association between air pollution and mortality in six U.S. cities. N. Engl. J. Med. 1993, 329, 1753–1759. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A., III; Brunett, R.T.; Thun, M.J. Lung cancer, cardiopulmonary mortality, and long term exposure to fine particulate air pollution. J. Am. Med. Assoc. 2002, 287, 1132–1141. [Google Scholar] [CrossRef]
- Bonita, R.; Beaglehole, R.; Kjellström, T. Basic Epidemiology, 2nd ed.; WHO: Geneve, Switzerland, 2006. [Google Scholar]
- Health Effect Institute. Health Effects of Outdoor Air Pollution in Developing Countries: A Literature Review. Available online: https://www.healtheffects.org/publication/health-effects-outdoor-air-pollution-developing-countries-asia-literature-review (accessed on 2 December 2006).
- WHO. World Health Report 2002. Available online: //www.who.int/whr/2002/en/whr02_annex_en.pdf (accessed on 9 January 2011).
- WHO. The Global Burden of Disease (GBD): 2004 Update. Available online: http://www.who.int/healthinfo/global_burden_disease/2004_report_update/en/index.html (accessed on 9 January 2011).
- Ostro, B. Outdoor air pollution. In Environmental Burden of Disease Series No.5; WHO: Geneve, Switzerland, 2004. [Google Scholar]
- Cohen, A.J.; Anderson, H.R.; Ostro, B.; Pandey, K.D.; Krzyzanowski, M.; Kunzli, N.; Gutschmidt, K.; Pope, C.A., III; Romieu, I.; Samet, J.M.; et al. Urban air pollution. In Comparative Quantification of Health Risks; Ezzati, M.E., Lopez, A.D., Murray, C.J.L., Eds.; WHO: Geneve, Switzerland, 2004. [Google Scholar]
- Vimercati, L.; Gatti, M.F.; Gagliardi, T.; Cuccaro, F.; Maria, D.L.; Caputi, A.; Quarato, M.; Baldassarre, A. Environmental exposure to arsenic and chromium in an industrial area. Environ. Sci. Pollut. Res. Int. 2017, 24, 11528–11535. [Google Scholar] [CrossRef] [PubMed]
- Vimercati, L.; Baldassarre, A.; Gatti, M.F.; Gagliardi, T.; Serinelli, M.; Maria, D.L.; Caputi, A.; Dirodi, A.A.; Galise, I.; Cuccaro, F.; et al. Non-occupational exposure to heavy metals of the residents of an industrial area and biomonitoring. Environ. Monit. Assess. 2016, 188, 673. [Google Scholar] [CrossRef] [PubMed]
- Nasari, M.M.; Szyszkowicz, M.; Chen, H.; Crouse, D.; Turner, M.C.; Jerrett, M.; Pope, C.A., III; Hubbell, B.; Fann, N.; Cohen, A.; et al. A class of non-linear exposure-response models suitable for health impact assessment applicable to large cohort studies of ambient air pollution. Air Qual. Atmos. Health 2016, 9, 961–972. [Google Scholar] [CrossRef] [PubMed]
- Anenberg, S.C.; Miller, J.; Minjares, R.; Du, L.; Henze, D.K.; Lacey, F.; Malley, C.S.; Emberson, L.; Franco, V.; Klimont, Z.; et al. Impacts and Mitigation of Excess Diesel-related NOx Emissions in 11 Major Vehicle Markets. Nature. 2017, 545, 467. [Google Scholar] [CrossRef] [PubMed]
- Osaka City Government. Osaka City White Paper; Osaka City Government: Osaka, Japan, 1984 and 1990. (In Japanese)
- Osaka Prefecture Government. Osaka Prefecture White Paper; Osaka Prefecture Government: Osaka, Japan, 1980 and 1990. (In Japanese)
- Sakamoto, S.; Shibuya, S.; Hirota, K.; Kashima, S. Estimation of exposure-response function considered cumulative and composite air pollution concentration. In Proceedings of the 26th Conference on Environmental Information Science, Tokyo, Japan, November 2012. [Google Scholar]
- Hirota, K.; Shibuya, S.; Sakamoto, S.; Kashima, S. A methodology of estimation on air pollution and its health effects in large Japanese cities. In Air Quality; Sunil, K., Ed.; InTech Open Access: Rijeka, Croatia, 2012; pp. 145–166. ISBN 979-953-307-220-2. [Google Scholar]
- Hirota, K.; Kashima, S. Emission volume, air quality and health effect in Japan: The cases of Tokyo, Kawasaki, Amagasaki and Kita Kyusyu. In Proceedings of the Seventh International Conference on Traffic & Transportation Studies (ICTTS 2010), Kunming, China, 3–5 August 2010. [Google Scholar]
- WHO. Reference Table 1. GBD 2000. Cause Groups and ICD Codes. Available online: http://www.who.int/healthinfo/bodreferencecausecategories.pdf (accessed on 5 February 2011).
- Ministry of Health, Labor and Welfare Government of Japan (MHLW). Available online: http://www.mhlw.go.jp/toukei/sippei/icd.html (accessed on 4 February 2011).
- Trends in Vital Statistics by prefecture in Japan (1974–1988). Available online: http://www.mhlw.go.jp/english/database/db-hw/vs_8/index.html (accessed on 29 June 2017).
- Kishimoto, A. Quantification and economic valuation of the health of particulate matter. Resour. Environ. 2000, 9, 42. (In Japanese) [Google Scholar]
- Quian, Z.; Zhang, J.; Wei, F.; Wilson, W.E.; Chapman, R.S. Long-term ambient air pollution levels in four Chinese cities: Inter-city and intra-city concentration gradients for epidemiological studies. J. Expo. Anal. Environ. Epidemiol. 2001, 11, 341–351. [Google Scholar] [CrossRef] [PubMed]
- Alpha Research Co.; Tera International Co. Thailand in Figures; Tera International Co.: Bangkok, Thailand, 2002–2006, 2015–2016. [Google Scholar]
- Alfa Research. Thailand Health Data; Alfa Research Co., Ltd: Bangkok, Thailand, 2015–2016. [Google Scholar]
- Asian Development Bank (ADB) and Clean Air Initiative for Asian Cities (CAI-Asia) Center. Country Synthesis Report on Urban Air Quality Management. Bangladesh, Cambodia, Hong Kong, India, Indonesia, Lao PDR, Malaysia, Mongolia, Nepal, Pakistan, Philippines, PRC, Singapore, Sri Lanka, Thailand, Viet Nam; ADB: Manila, The Philippines, 2006. [Google Scholar]
- Clean Air Initiative for Asian Cities (CAI-Asia). Clean Air Management Profile: India, Indonesia, Philippines, Thailand and Viet Nam: Air Quality Profile 2010 Edition; CAI-Asia Center: Pasig City, The Philippines, 2010. [Google Scholar]
- Badan Pusat Statistik (BPS). Statistics of Indonesia; BPS: Jakarta, Indonesia, 2008, 2015.
- Badan Pusat Statistik (BPS), Environmental Statistics of Indonesia; BPS: Jakarta, Indonesia, 2001, 2004, 2006, 2008.
- Bangladesh Bureau of Statistics. Statistical Yearbook of Bangladesh; Bangladesh Bureau of Statistics: Dhaka, Bangladesh, 2005, 2008.
- Beijing Municipal Bureau of Statistics. Beijing Statistical Yearbook; China Statistics Press: Beijing, China, 2003–2015.
- Census and Statistics Department. Hong Kong Annual Digest of Statistics; The Government of Hong Kong Special Administration Region: Hong Kong, 2000, 2007, 2008, 2015.
- Central Statistical Organization. Myanmar Statistical Yearbook; Ministry of Planning and Finance: Nay Pyi Taw, Myanmar, 2005, 2011, 2015.
- Chongqing Municipal Bureau of Statistics. Chongqing Statistical Yearbook; China Statistics Press: Beijing, China, 2004–2007, 2011, 2013 and 2015.
- Dalian Municipal Bureau of Statistics. Dalian Statistical Yearbook; China Statistics Press: Dalian, China, 2012–2015.
- Department of Census and Statistics Sri Lanka. Statistical Abstract; Department of Census and Statistics: Battaramulla, Sri Lanka, 1999, 2005–2007, 2009 and 2015.
- Department of Census and Statistics Sri Lanka. Statistical Pocket Book of Republic of Sri Lanka; Department of Census and Statistics: Battaramulla, Sri Lanka, 2004.
- Department of Environment Malaysia. Malaysia Environmental Quality Report; Department of Environment Malaysia: Putrajaya, Malaysia, 2004, 2007.
- Department of Statistics Malaysia. State/district Databank; Department of Statistics: Putrajaya, Malaysia, 2012.
- Department of Statistics Malaysia. Social Statistics Bulletin; Department of Statistics: Putrajaya, Malaysia, 2006, 2012, 2014, 2015.
- The Energy and Resources Institute (TERI). TERI Energy and Environment Data Diary and Yearbook (TEDDY); TERI: New Delhi, India, 2013/2014, 2015/2016. [Google Scholar]
- Department of Environment and Natural Resources. National Air Quality Report; Department of Environment and Natural Resources: Quezon City, The Philippines, 2002–2004.
- Government of Karnakata and WilburSmith Associates. Bangalore Mobility Indicators 2008; Directorate of urban land transport, Government of Karnakata and WilburSmith Associates: Bangalore, India, 2009.
- Government of Karnakata. Annual Report 2008–2009; Government of Karnakata: Bangalore, India, 2010.
- The Government of National Capital Territory of Delhi. Delhi Statistical Handbook; The Government of National Capital Territory of Delhi: Delhi, India, 2008.
- Guangzhou Municipal Bureau of Statistics. Guangzhou Statistical Yearbook; China Statistics Press: Beijing, China, 2000–2004, 2007, 2008, 2015.
- Hanoi Statistical Office. Statistical Yearbook of Hanoi; General Statistical Office of Viet Nam: Hanoi, Viet Nam, 2002, 2004–2006, 2015.
- Ho Chi Minh City Statistical Office. Statistics Yearbook of Ho Chi Minh City; General Statistics Office of Viet Nam: Ho Chi Minh City, Viet Nam, 2006, 2008, 2013.
- Lao Statistics Bureau. Lao PDR Statistical Yearbook; Lao Statistics Bureau: Vientiane, Laos, 2015.
- The Ministry of Environment. Korea Environmental Statistics; The Ministry of Environment: Seoul, Korea, 2006.
- Ministry of Statistics & Programme Implementation. Statistical Abstract of India; New Delhi Govt. of India: New Delhi, India, 2000–2004, 2007.
- National Bureau of Statistics of China. China National Statistical Yearbook; National Bureau of Statistics of China: Beijing, China, 1999–2005.
- National Institute of Statistics. Ministry of Planning. Cambodia Statistical Yearbook; National Institute of Statistics, Ministry of Planning: Phnom Penh, Cambodia, 2006.
- National Institute of Statistics, Ministry of Planning. A Compendium on Environment Statistics; Ministry of Planning: Phnom Penh, Cambodia, 2003.
- National Statistical Office, Ministry of Information and Communication Technology. Thailand Environment Statistics; National Statistical Office Publication: Bangkok, Thailand, 2004.
- National Statistical Office of Mongolia. Mongolian Statistical Yearbook; National Statistical Office of Mongolia: Ulaanbaatar, Mongolia, 2006, 2013.
- Pakistan Bureau of Statistics. Pakistan Statistical Yearbook; Pakistan Bureau of Statistics: Islamabad, Pakistan, 2007, 2014.
- Pakistan Bureau of Statistics. Statistical Pocket Book of Pakistan; Pakistan Bureau of Statistics: Islamabad, Pakistan, 2007.
- Philippines Statistics Authority. Philippine Statistical Yearbook; The Philippines Statistics Authority: Quezon City, The Philippines, 2009.
- Philippines Statistics Authority. Compendium of Environmental Statistics; Philippines Statistics Authority: Quezon City, The Philippines, 2014.
- Qingdao Municipal Bureau of Statistics. Qingdao Statistical Yearbook; China Statistics Press: Beijing, China, 2006, 2008, 2015.
- Shanghai Municipal Bureau of Statistics. Shanghai Statistical Yearbook; China Statistics Press: Beijing, China, 1997, 1998, 2004, 2005, 2009, 2011, 2014, 2015.
- Shenzhen Municipal Bureau of Statistics. Shenzhen Statistical Yearbook; China Statistics Press: Beijing, China, 2008, 2015.
- Shenyang Municipal Bureau of Statistics. Shenyang Statistical Yearbook; China Statistics Press: Beijing, China, 2007, 2015.
- Singapore Department of Statistics. Yearbook of Statistics Singapore; Singapore Department of Statistics: High Street, Singapore, 2000, 2008, 2015.
- Statistical Forecasting Bureau. Statistical Yearbook Thailand; National Statistical Office: Bangkok, Thailand, 2007, 2014.
- The Yearbook of China’s Cities Press. The China's Cities Yearbook; The Yearbook of China’s Cities Press: Beijing, China, 2008. [Google Scholar]
- Transport Research Wing, Ministry of Shipping, Road Transport and Highway. Road Transport Yearbook; Ministry of Road Transport and Highway: Delhi, India, 2009, 2010.
- The World Bank Indonesia Office. Indonesia Environmental Monitor 2003; The World Bank Group: Jakarta, Indonesia, 2003. [Google Scholar]
- The World Bank Manila Office. Philippines Environmental Monitor 2002; The World Bank Group: Pasig City, The Philippines, 2002. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Rate | City | Urban Population | TSP/PM2.5/PM10 | Cause of Death for Respiratory Disease (J00–J99) | km2/ Monitoring Site |
|---|---|---|---|---|---|---|
| 1 | △ | Bangalore | 1990, 1995, 1996, 2000, 2001, 2005 | 1995, 1999–2007, 2012, 2013 | NA | 89 |
| 2 | ○ | Bangkok | 1990, 1995–2014 | 1990, 1995–2013 | 1995, 1996, 2000, 2011, 2013 | 143 |
| 3 | ○ | Beijing | 1990, 1995–2014 | 1990, 1995,1999–2014 | 1995–2014 | 73 |
| 4 | △ | Chongqing | 1995–2014 | 1997–2014 | NA | 37 |
| 5 | ○ | Colombo | 1995–2014 | 1998–2012 | 1995, 2003–2006, 2009 | NA |
| 6 | △ | Dalian | 1995, 1998, 2000–2014 | 2003–2008, 2012 | NA | 26 |
| 7 | △ | Delhi | 1990, 1995–2005 | 1990, 1995–2007 | NA | 66 |
| 8 | × | Dhaka | 1995, 1997–2005 | 1997–2007 | NA | 581 |
| 9 | △ | Guangzhou | 1995–2014 | 1995, 1998–2014 | NA | 81 |
| 10 | △ | Hanoi | 1995, 1999–2014 | 1996, 1998–2003 | NA | 117 |
| 11 | △ | Ho Chi Minh City | 1995, 1998–2008, 2010–2012 | 1995–2007 | NA | 210 |
| 12 | ○ | Hong Kong | 1995–2014 | 1995–2014 | 1995–2014 | 100 |
| 13 | △ | Jakarta | 1995, 1998–2006, 2010, 2013–2014 | 1990, 1995, 1999–2003, 2007, 2009 | NA | 111 |
| 14 | × | Karachi | 1990, 1998 | 1990, 2000, 2001, 2003 | NA | 14,091 |
| 15 | × | Kathmandu | 1995, 2000, 2001, 2005 | 2003–2007 | NA | 25 |
| 16 | △ | Kuala Lumpur | 1995, 1996, 1998–2012 | 1995–2007, 2010, 2012, 2013 | NA | 77 |
| 17 | △ | Manila | 2000, 2005–2007 | 1990, 1995–2007 | 1996–1999 | 53 |
| 18 | △ | Mumbai | 1990, 1995, 2000, 2001, 2005 | 1995–2007 | NA | NA |
| 19 | × | Okinawa Naha-City | NA | NA | NA | 40 |
| 20 | △ | Phnom Penh | 1995, 1998–2006, 2008, 2013 | 1995, 2001, 2002 | NA | 21 |
| 21 | △ | Qingdao | 1996–2012 | NA | NA | 45 |
| 22 | △ | Seoul | 1995, 2000, 2005, 2007 | 1990, 1995–2005, 2007 | NA | 30 |
| 23 | ○ | Shanghai | 1990, 1995–2014 | 1990, 1995–2014 | 1990, 1995–2008, 2010–2014 | 81 |
| 24 | △ | Shenyang | 1995, 1998, 2000–2007, 2010–2012 | 2003–2007 | 1998 | 22 |
| 25 | △ | Shenzen | 1995–2014 | 1996–2014 | 1996–1998 | NA |
| 26 | ○ | Singapore | 1990, 1995–2014 | 1990, 1995–2014 | 1995–2014 | 140 |
| 27 | × | Taipei | 1995, 2000, 2002–2005, 2007 | 1995–2008 | NA | NA |
| 28 | × | Ulaanbaater | 1995, 2000–2006 | 2008 | NA | 588 |
| 29 | × | Vientiane | 1995, 1998, 2000–2006, 2014, 2015 | 2002–2004, 2007, 2008 | NA | NA |
| 30 | △ | Yangon | 1995, 1998, 2000–2010, 2014 | 2007 | 1990, 1995, 1998–2007, 2010–2013 | 518 |
| 31 | × | Yokohama | 1995–1999 | NA | NA | 16 |
| Items of Results | Equation (2) α | Equation (5) β |
|---|---|---|
| Coefficient | 0.0291 (16.30) | 0.0062 (4.31) |
| Adjusted R2 | 0.856 | 0.499 |
| The number of observations | 10 | 15 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hirota, K.; Sakamoto, S.; Shibuya, S.; Kashima, S. A Methodology of Health Effects Estimation from Air Pollution in Large Asian Cities. Environments 2017, 4, 60. https://doi.org/10.3390/environments4030060
Hirota K, Sakamoto S, Shibuya S, Kashima S. A Methodology of Health Effects Estimation from Air Pollution in Large Asian Cities. Environments. 2017; 4(3):60. https://doi.org/10.3390/environments4030060
Chicago/Turabian StyleHirota, Keiko, Shogo Sakamoto, Satoshi Shibuya, and Shigeru Kashima. 2017. "A Methodology of Health Effects Estimation from Air Pollution in Large Asian Cities" Environments 4, no. 3: 60. https://doi.org/10.3390/environments4030060
APA StyleHirota, K., Sakamoto, S., Shibuya, S., & Kashima, S. (2017). A Methodology of Health Effects Estimation from Air Pollution in Large Asian Cities. Environments, 4(3), 60. https://doi.org/10.3390/environments4030060