

A Scoping Review of the Effects of Ambient Air Quality on Cognitive Frailty

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
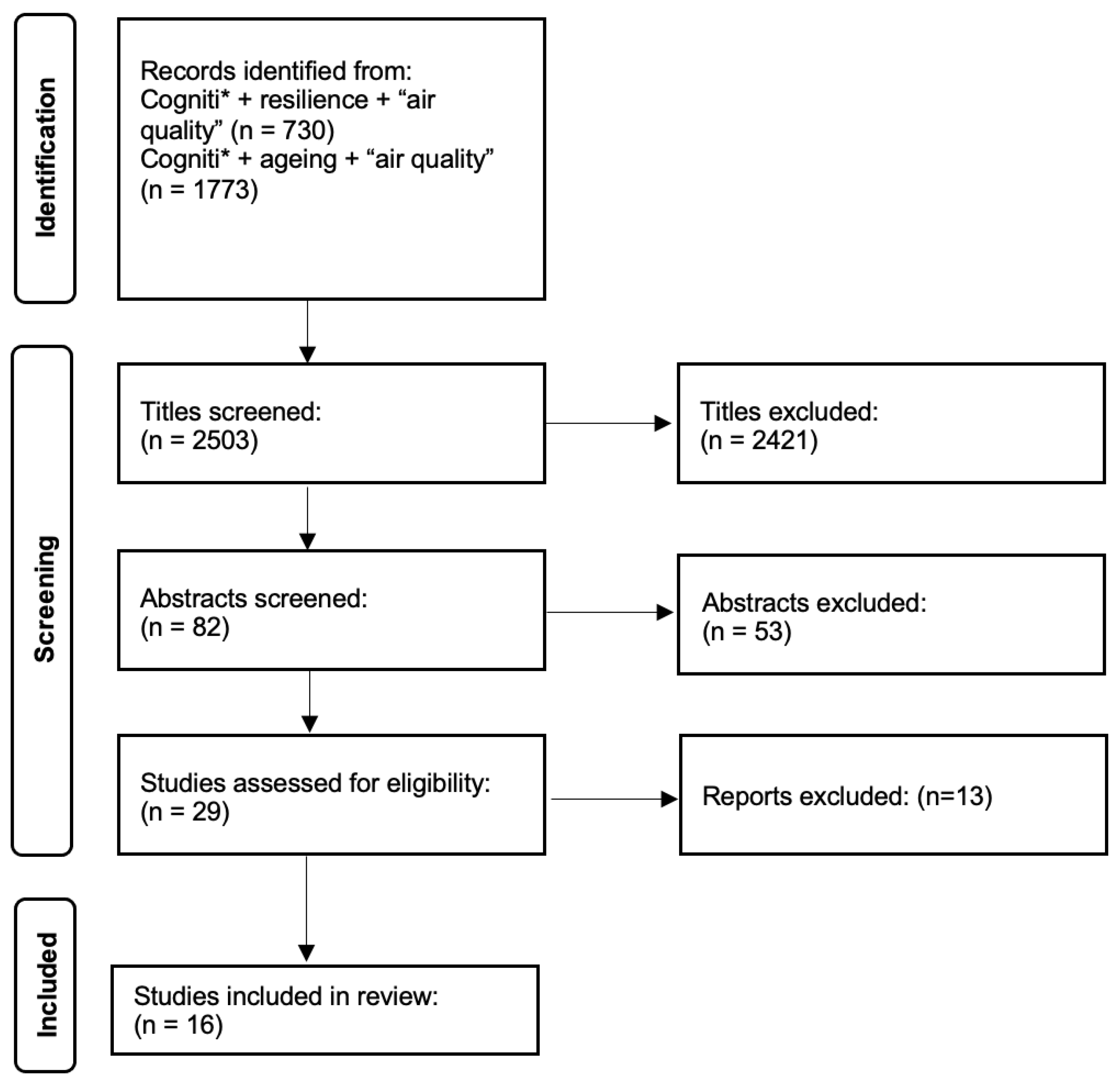
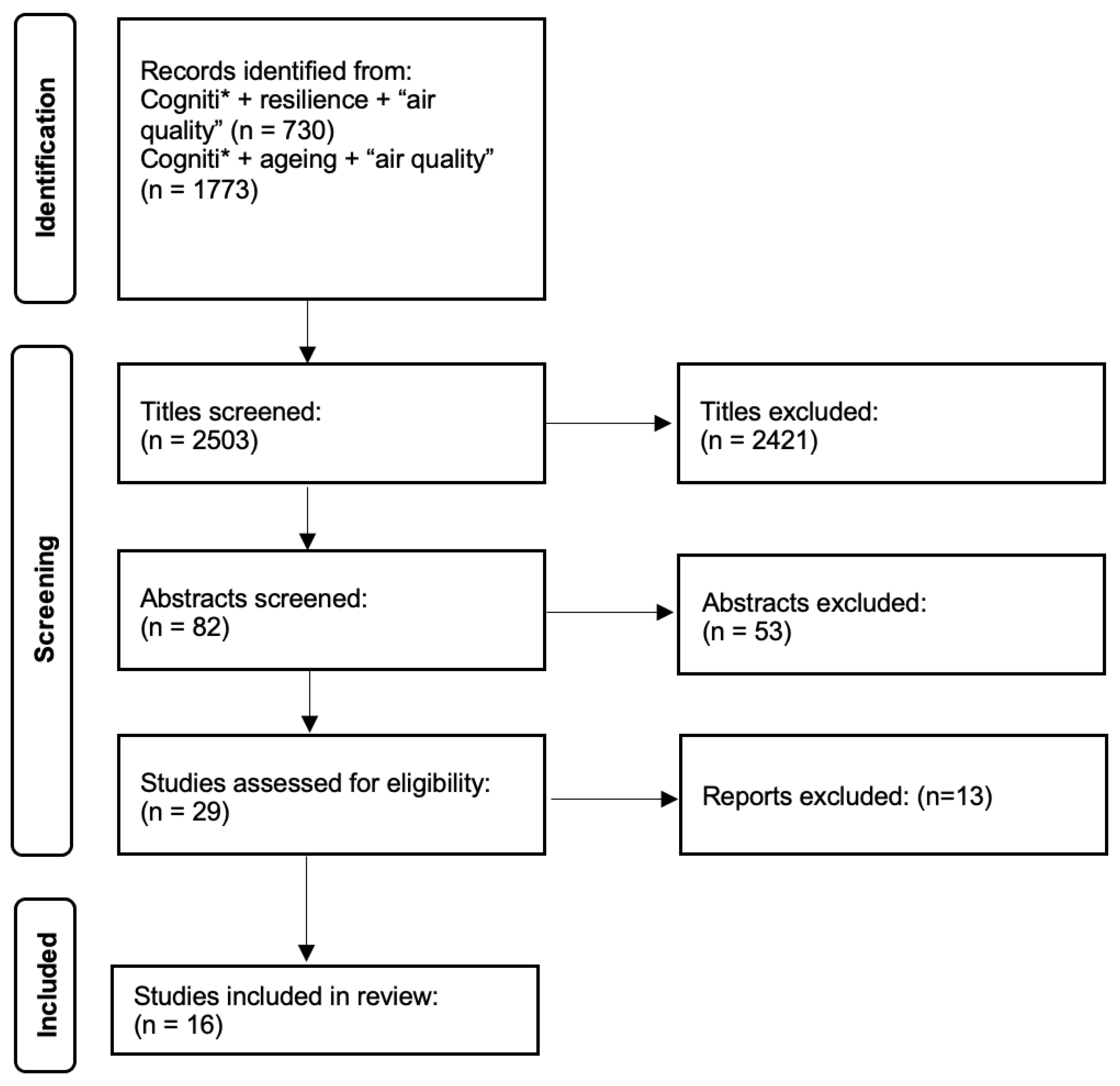
2.1. Scoping Review Approach
2.2. Protocol
3. Results
3.1. Scoping Review
3.2. Variations in Air Quality Assessment
3.3. Overall Results

{kind=link}
{kind=link}
| Authors | Title | Published | Country | OECD /UMIC | Maximum Cohort Number | Gender Male/Female (in %) | Reported Level of Education | Wealth |
|---|---|---|---|---|---|---|---|---|
| Ailshire and Walseman [32] | Education differences in the adverse impact of PM2.5 on incident cognitive impairment among U.S. older adults | 2021 | United States | OECD | 5636 | 46/54 | 59%, 12 years of education | Majority high paid workers |
| Ailshire and Crimmins [36] | Fine particulate matter air pollution and cognitive function among older US adults | 2014 | United States | OECD | 13,996 | 44/56 | Mean 14 years of education | No data |
| Chen et al. [30] | Long-Term exposure to air pollutants and cognitive function in Taiwanese community-dwelling older adults: A four-year cohort study | 2020 | Taiwan | OECD | 605 (305 at follow up) | 46/54 | Mean 14 years of education | No data |
| Kulick et al. [34] | Long-term exposure to ambient air pollution, APOE-ε4 status, and cognitive decline in a cohort of older adults in northern Manhattan | 2020 | United States | OECD | 4821 | 32/68 | Mean 9 years of education | No data |
| Lo et al. [35] | Air pollution associated with cognitive decline by the mediating effects of sleep cycle disruption and changes in brain structure in adults | 2022 | Taiwan | OECD | 4866 | 69/31 | Mean 10 years of education | No data |
| Lv et al. [5] | Long-term exposure to PM2.5 and incidence of disability in activities of daily living among oldest old | 2023 | China | OECD | 15,453 | 44/56 | 67% illiterate 33% literate | No data |
| Molina-Sotomayor et al. [37] | Effects of cardiorespiratory exercise on cognition in older women exposed to air pollution | 2019 | Chile | UMIC | 181 | All women | No data | No data |
| Petkus et al. [28] | Outdoor air pollution exposure and inter-relation of global cognitive performance and emotional distress in older women | 2021 | United States | OECD | 6118 | All women | 71% higher educated | Assumed wealthier |
| Qiu et al. [38] | Associations between air pollution and psychiatric symptoms in the Normative Aging Study | 2022 | United States | OECD | 570 | All men (veterans) | 13% higher educated | No data |
| Russ et al. [6] | Life course air pollution exposure and cognitive decline: Modelled historical air pollution data and the Lothian birth cohort 1936 | 2021 | Scotland UK | OECD | 572 | 53/47 | 28% higher educated | No data |
| Salinas-Rodríguez et al. [39] | Exposure to ambient PM2.5 concentrations and cognitive function among older Mexican adults | 2018 | Mexico | UMIC | 7986 | 46/54 | No data | No data |
| Tonne et al. [29] | Traffic-related air pollution in relation to cognitive function in older adults | 2014 | UK | OECD | 3414 | 65/35 | 39% higher educated | 41% high paid |
| Wang et al. [40] | Fine particulate matter and poor cognitive function among Chinese older adults: Evidence from a community-based, 12-year prospective cohort study | 2020 | China | 13,324 | 48/52 | 59% illiterate | No data | |
| Weuve et al. [27] | Exposure to particulate air pollution and cognitive decline in older women | 2012 | United States | OECD | 19,409 | All women | 100% graduate nurses | No data |
| Yao et al. [26] | The effect of China’s Clean Air Act on cognitive function in older adults: a population-based, quasi-experimental study | 2022 | China | OECD | 2812 | 50/50 | No data | No data |
| Zhu et al. [31] | Interaction between plant-based dietary pattern and air pollution on cognitive function: a prospective cohort analysis of older adults | 2022 | China | OECD | 6525 | 49/51 | 48% formal education | 35% ‘financially independent’ |
| Authors | Publication | Country | Monitoring Method | Modelling Method | Validation Method | Averaging Period (s) |
|---|---|---|---|---|---|---|
| Ailshire and Walseman [32] | 2021 | United States | United States Environmental Protection Agency (USEPA) monitoring stations | Gridded 12 km model | None stated—utilising USEAP model | Annual average concentration |
| Ailshire and Crimmins [36] | 2014 | United States | USEPA monitoring stations | Inverse distance weighting of monitoring stations to participant census tract | None stated | 24 h mean |
| Chen et al. [30] | 2020 | Taiwan | Taiwan Environmental Protection Administration monitoring stations | Bayesian maximum entropy | None stated | Annual mean concentration |
| Kulick et al. [34] | 2020 | United States | USEPA monitoring stations | Universal kriging | None stated | Annual Average |
| Lo et al. [35] | 2022 | Taiwan | Taiwan Environmental Protection Administration monitoring stations | Hybrid kriging-land-use regression | None stated | Daily concentrations aggregate to annual average |
| Lv et al. [5] | 2023 | China | Satellite, simulation and monitoring stations utilised to estimate resident exposure. | Not specified | Out-of-sample cross-validation with monitors | Annual concentration over 4 time points (2002, 2005, 2008, 2011) |
| Molina-Sotomayor et al. [37] | 2019 | Chile | Not specified | Not specified | Not specified | Annual average (2012, 2013, 2014) |
| Petkus et al. [28] | 2021 | United States | USEPA monitoring stations | Regionalised universal kriging | None stated | Annual mean concentration |
| Qiu et al. [38] | 2022 | United States | USEPA monitoring stations, satellite-derived measurements | Machine-learning algorithms using geographically weighted regression | Cross-validated to monitored values | Averages of 1 week, 4 weeks, 8 weeks and one year prior to the visit |
| Russ et al. [6] | 2021 | Scotland UK | N/A | EMEP4UK atmospheric chemistry transport model | Validated against UK monitoring stations | Annual mean PM2.5 concentration (1935, 1950, 1970, 1980, 1990, 2001) |
| Salinas-Rodríguez et al. [39] | 2018 | Mexico | N/A | Aerosol optical depth information retrieved from remote sensing data. Combination of observations from the Moderate Resolution Imaging Spectroradiometer and Multiangle Imaging Spectroradiometer instruments on the Terra satellite (NASA satellites), and simulations with the Goddard Earth Observing System (GEOS) chemical transport model. | None stated | Annual average |
| Tonne et al. [29] | 2014 | UK | N/A | KCLurban and CMAQ-Urban models | Validated against monitoring stations | 1-, 3- and 5-year average |
| Wang et al. [40] | 2020 | China | N/A | Utilised aerosol optical depth data with a land-use regression model. | Global ground-based stations and geographical weighted regression method. | Averaged for study period as well as 3 years prior to recruitment |
| Weuve et al. [27] | 2012 | United States | USEPA monitoring data | Geographic information system-based spatiotemporal smoothing | Not stated | 1 month and 7–14 year exposures |
| Yao et al. [26] | 2022 | China | N/A | Atmospheric chemical transport model. | Not stated | Annual average concentration |
| Zhu et al. [31] | 2022 | China | Remote sensing, Multiangle Imaging SpectroRadiometer and Sea-viewing Wide Field-of-view Sensor satellite instrument, vertical profiles derived from the GEOS-Chem chemical transport model | Utilised monitoring data previously described | Ground-based observations using geographically weighted regression | Annual mean from 1998 to 2014 |
3.4. Variations in Cognitive Assessments
3.5. Limitations of the Selected Studies
4. Discussion
4.1. Limitations of Scoping Review and Gaps in the Literature
4.2. Standardising Measures of Air Quality and Cognitive Frailty
4.3. Thinking about Policy and Practice
4.4. The Differential Impact of Air Quality, Even When Guidelines Are Met
4.5. Thinking about Co-Benefits
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Saborit, J.M.; Guercio, V.; Gowers, A.M.; Shaddick, G.; Fox, N.C.; Love, S. A critical review of the epidemiological evidence of effects of air pollution on dementia, cognitive function and cognitive decline in adult population. Sci. Total Environ. 2021, 757, 143734. [Google Scholar] [CrossRef] [PubMed]
- Chandra, M.; Rai, C.B.; Kumari, N.; Sandhu, V.K.; Chandra, K.; Krishna, M.; Kota, S.H.; Anand, K.S.; Oudin, A. Air pollution and cognitive impairment across the life course in humans: A systematic review with specific focus on income level of study Area. Int. J. Environ. Res. Public Health 2022, 19, 1405. [Google Scholar] [CrossRef] [PubMed]
- Lv, Y.; Yang, Z.; Ye, L.; Jiang, M.; Zhou, J.; Guo, Y.; Qiu, Y.; Li, X.; Chen, C.; Ju, A.; et al. Long-term fine particular exposure and incidence of frailty in older adults: Findings from the Chinese Longitudinal Healthy Longevity Survey. Age Ageing 2023, 52, afad009. [Google Scholar] [CrossRef] [PubMed]
- Russ, T.C.; Cherrie, M.P.; Dibben, C.; Tomlinson, S.; Reis, S.; Dragosits, U.; Vieno, M.; Beck, R.; Carnell, E.; Shortt, N.K.; et al. Life course air pollution exposure and cognitive decline: Modelled his-torical air pollution data and the Lothian birth cohort 1936. J. Alzheimer’s Dis. 2021, 79, 1063–1074. [Google Scholar] [CrossRef] [PubMed]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef]
- Kelaiditi, E.; Cesari, M.; Canevelli, M.; Abellan van Kan, G.; Ousset, P.J.; Gillette-Guyonnet, S.; Ritz, P.; Duveau, F.; Soto, M.E.; Provencher, V.; et al. Cognitive frailty: Rational and definition from an (IANA/IAGG) International Consensus Group. J. Nutr. Health Aging 2013, 17, 726–734. [Google Scholar] [CrossRef]
- Sugimoto, T.; Arai, H.; Sakurai, T. An update on cognitive frailty: Its definition, impact, associated factors and underlying mechanisms, and interventions. Geriatr. Gerontol. Int. 2022, 22, 99–109. [Google Scholar] [CrossRef]
- Ramnath, U.; Rauch, L.; Lambert, E.V.; Kolbe-Alexander, T.L. The relationship between functional status, physical fitness and cognitive performance in physically active older adults: A pilot study. PLoS ONE 2018, 13, e0194918. [Google Scholar] [CrossRef]
- WHO. Ambient (Outdoor) Air Pollution. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/ambient-(outdoor)-air-quality-and-health (accessed on 21 June 2023).
- Mannucci, P.M.; Harari, S.; Franchini, M. Novel evidence for a greater burden of ambient air pollution on cardiovascular disease. Haematologica 2019, 104, 2349–2357. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Zhu, D. Exposure to outdoor air pollution and its human health outcomes: A scoping review. PLoS ONE 2019, 14, e0216550. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Global Air Quality Guidelines: Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulphur Dioxide and Carbon Monoxide. 2021. Available online: https://apps.who.int/iris/handle/10665/345329 (accessed on 5 December 2023).
- Calderon-Garciduenas, L.; Maronpot, R.R.; Torres-Jardon, R.; Henriquez-Roldan, C.; Schoonhoven, R.; Acuna-Ayala, H.; Villarreal-Calderon, A.; Nakamura, J.; Fernando, R.; Reed, W.; et al. DNA damage in nasal and brain tissues of canines exposed to air pollutants is associated with evidence of chronic brain inflammation and neurodegeneration. Toxicol. Pathol. 2003, 31, 524–538. [Google Scholar] [CrossRef] [PubMed]
- Shou, Y.; Huang, Y.; Zhu, X.; Liu, C.; Hu, Y.; Wang, H. A review of the possible associations between ambient PM2.5 exposures and the development of Alzheimer’s disease. Ecotoxicol. Environ. Saf. 2019, 174, 344–352. [Google Scholar] [CrossRef] [PubMed]
- COMEAP. Air Pollution: Cognitive Decline and Dementia. A Report by the Committee on the Medical Effects of Air Pollutants (COMEAP). 2022. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1090376/COMEAP-dementia-report-2022.pdf (accessed on 5 December 2023).
- Castellani, B.; Bartington, S.; Wistow, J.; Heckels, N.; Ellison, A.; Van Tongeren, M.; Arnold, S.R.; Barbrook-Johnson, P.; Bicket, M.; Pope, F.D.; et al. Mitigating the impact of air pollution on dementia and brain health: Setting the policy agenda. Environ. Res. 2022, 215, 114362. [Google Scholar] [CrossRef] [PubMed]
- Oberdörster, G.; Sharp, Z.; Atudorei, V.; Elder, A.; Gelein, R.; Kreyling, W.; Cox, C. Translocation of inhaled ultrafine particles to the brain. Inhal. Toxicol. 2004, 16, 437–445. [Google Scholar] [CrossRef] [PubMed]
- Heusinkveld, H.J.; Wahle, T.; Campbell, A.; Westerink, R.H.S.; Tran, L.; Johnston, H.; Stone, V.; Cassee, F.R.; Schins, R.P.F. Neurodegenerative and neurological disorders by small inhaled particles. Neurotoxicology 2016, 56, 94–106. [Google Scholar] [CrossRef]
- Tian, L.; Shang, Y.; Chen, R.; Bai, R.; Chen, C.; Inthavong, K.; Tu, J. Correlation of regional deposition dosage for inhaled nanoparticles in human and rat olfactory. Part. Fibre Toxicol. 2019, 16, 6. [Google Scholar] [CrossRef]
- Tian, Q.; Bilgel, M.; Moghekar, A.R.; Ferrucci, L.; Resnick, S.M. Olfaction, cognitive impairment, and PET biomarkers in community-dwelling older adults. J. Alzheimer’s Dis. 2022, 86, 1275–1285. [Google Scholar] [CrossRef]
- Veronese, N.; Maniscalco, L.; Matranga, D.; Lacca, G.; Dominguez, L.J.; Barbagallo, M. Association between Pollution and Frailty in Older People: A Cross-Sectional Analysis of the UK Biobank. J. Am. Med. Dir. Assoc. 2023, 24, 475–481.e3. [Google Scholar] [CrossRef]
- Pun, V.C.; Manjourides, J.; Suh, H. Association of ambient air pollution with depressive and anxiety symptoms in older adults: Results from the NSHAP study. Environ. Health Perspect. 2017, 125, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Lockwood, C.; dos Santos, K.B.; Pap, R. Practical guidance for knowledge synthesis: Scoping review methods. Asian Nurs. Res. 2019, 13, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Lv, X.; Qiu, C.; Li, J.; Wu, X.; Zhang, H.; Yue, D.; Liu, K.; Eshak, E.S.; Lorenz, T.; et al. The effect of China’s Clean Air Act on cognitive function in older adults: A population-based, quasi-experimental study. Lancet Healthy Longev. 2022, 3, e98–e108. [Google Scholar] [CrossRef] [PubMed]
- Weuve, J.; Puett, R.C.; Schwartz, J.; Yanosky, J.D.; Laden, F.; Grodstein, F. Exposure to particulate air pollution and cognitive decline in older women. Arch. Intern. Med. 2012, 172, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Petkus, A.J.; Wang, X.; Beavers, D.P.; Chui, H.C.; Espeland, M.A.; Gatz, M.; Gruenewald, T.; Kaufman, J.D.; Manson, J.E.; Resnick, S.M.; et al. Outdoor air pollution exposure and inter-relation of global cognitive performance and emotional distress in older women. Environ. Pollut. 2021, 271, 116282. [Google Scholar] [CrossRef] [PubMed]
- Tonne, C.; Elbaz, A.; Beevers, S.; Singh-Manoux, A. Traffic-related air pollution in relation to cognitive function in older adults. Epidemiology 2014, 25, 674–681. [Google Scholar] [CrossRef]
- Chen, J.-H.; Kuo, T.-Y.; Yu, H.-L.; Wu, C.; Yeh, S.-L.; Chiou, J.-M.; Chen, T.-F.; Chen, Y.-C. Long-term exposure to air pollutants and cognitive function in taiwanese community-dwelling older adults: A four-year cohort study. J. Alzheimer’s Dis. 2020, 78, 1585–1600. [Google Scholar] [CrossRef]
- Zhu, A.; Chen, H.; Shen, J.; Wang, X.; Li, Z.; Zhao, A.; Shi, X.; Yan, L.; Zeng, Y.; Yuan, C.; et al. Interaction between plant-based dietary pattern and air pollution on cognitive function: A prospective cohort analysis of Chinese older adults. Lancet Reg. Health–West. Pac. 2022, 20, 100372. [Google Scholar] [CrossRef]
- Ailshire, J.; Walsemann, K.M. Education differences in the adverse impact of PM2.5 on incident cognitive impairment among US older adults. J. Alzheimer’s Dis. 2021, 79, 615–625. [Google Scholar] [CrossRef]
- Lv, Y.; Zhou, J.; Kraus, V.B.; Li, T.; Sarnat, J.A.; Wang, J.; Liu, Y.; Chen, H.; Brasher, M.S.; Mao, C.; et al. Long-term exposure to PM2.5 and incidence of disability in activities of daily living among oldest old. Environ. Pollut. 2020, 259, 113910. [Google Scholar] [CrossRef]
- Kulick, E.R.; Elkind, M.S.; Boehme, A.K.; Joyce, N.R.; Schupf, N.; Kaufman, J.D.; Mayeux, R.; Manly, J.J.; Wellenius, G.A. Long-term exposure to ambient air pollution, APOE-ε4 status, and cognitive decline in a cohort of older adults in northern Manhattan. Environ. Int. 2020, 136, 105440. [Google Scholar] [CrossRef]
- Lo, C.-C.; Liu, W.-T.; Lu, Y.-H.; Wu, D.; Wu, C.-D.; Chen, T.-C.; Fang, Y.-T.; Lo, Y.-C.; Chen, Y.-Y.; Kang, L.; et al. Air pollution associated with cognitive decline by the mediating effects of sleep cycle disruption and changes in brain structure in adults. Environ. Sci. Pollut. Res. 2022, 29, 52355–52366. [Google Scholar] [CrossRef] [PubMed]
- Ailshire, J.A.; Crimmins, E.M. Fine particulate matter air pollution and cognitive function among older US adults. Am. J. Epidemiology 2014, 180, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Molina-Sotomayor, E.; Orb, M.G.; de la Fuente, F.P.; Figueroa, G.C.; Sánchez-Oliver, A.J.; González-Jurado, J.A. Effects of cardiorespiratory exercise on cognition in older women exposed to air pollution. Int. J. Environ. Res. Public Health 2019, 16, 245. [Google Scholar] [CrossRef] [PubMed]
- Qiu, X.; Danesh-Yazdi, M.; Weisskopf, M.; Kosheleva, A.; Spiro, A.; Wang, C.; A Coull, B.; Koutrakis, P.; Schwartz, J.D. Associations between air pollution and psychiatric symptoms in the Normative Aging Study. Environ. Res. Lett. 2022, 17, 034004. [Google Scholar] [CrossRef] [PubMed]
- Salinas-Rodríguez, A.; Fernández-Niño, J.A.; Manrique-Espinoza, B.; Moreno-Banda, G.L.; Sosa-Ortiz, A.L.; Qian, Z.M.; Lin, H. Exposure to ambient PM2.5 concentrations and cognitive function among older Mexican adults. Environ. Int. 2018, 117, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Naghavi, M.; Allen, C.; Barber, R.M.; Bhutta, Z.A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; Coates, M.M.; et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Li, T.; Lv, Y.; Kraus, V.B.; Zhang, Y.; Mao, C.; Yin, Z.; Shi, W.; Zhou, J.; Zheng, T.; et al. Fine particulate matter and poor cognitive function among Chinese older adults: Evidence from a community-based, 12-year prospective cohort study. Environ. Health Perspect. 2020, 128, 067013. [Google Scholar] [CrossRef]
- Tsai, C.-F.; Lee, W.-J.; Wang, S.-J.; Shia, B.-C.; Nasreddine, Z.; Fuh, J.-L. Psychometrics of the Montreal Cognitive Assessment (MoCA) and its subscales: Validation of the Taiwanese version of the MoCA and an item response theory analysis. Int. Psychogeriatr. 2012, 24, 651–658. [Google Scholar] [CrossRef]
- Marmot, M. Health equity in England: The Marmot review 10 years on. BMJ 2020, 368, m693. [Google Scholar] [CrossRef]
- Al-Kindi, S.G.; Brook, R.D.; Biswal, S.; Rajagopalan, S. Environmental determinants of cardiovascular disease: Lessons learned from air pollution. Nat. Rev. Cardiol. 2020, 17, 656–672. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, B. Air Pollution in Cities: Urban and Transport Planning Determinants and Health in Cities; Integrating Human Health into Urban and Transport Planning: A framework; Springer: Cham, Switzerland, 2019; pp. 425–441. [Google Scholar]
- Koman, P.D.; Hogan, K.A.; Sampson, N.; Mandell, R.; Coombe, C.M.; Tetteh, M.M.; Hill-Ashford, Y.R.; Wilkins, D.; Zlatnik, M.G.; Loch-Caruso, R.; et al. Examining joint effects of air pollution exposure and social determinants of health in defining “at-risk” populations under the Clean Air Act: Susceptibility of pregnant women to hypertensive disorders of preg-nancy. World Med. Health Policy 2018, 10, 7–54. [Google Scholar] [CrossRef] [PubMed]
- Fairburn, J.; Schüle, S.A.; Dreger, S.; Hilz, L.K.; Bolte, G. social inequalities in exposure to ambient air pollution: A systematic review in the WHO European region. Int. J. Environ. Res. Public Health 2019, 16, 3127. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, L.; Taylor, J.; Zhou, K.; Shrubsole, C.; Symonds, P.; Davies, M.; Dimitroulopoulou, S. Systemic inequalities in indoor air pollution exposure in London, UK. Build. Cities 2021, 2, 425–448. [Google Scholar] [CrossRef] [PubMed]
- Callaghan, A.; McCombe, G.; Harrold, A.; McMeel, C.; Mills, G.; Moore-Cherry, N.; Cullen, W. The impact of green spaces on mental health in urban settings: A scoping review. J. Ment. Health 2021, 30, 179–193. [Google Scholar] [CrossRef] [PubMed]
- Marval, J.; Tronville, P. Ultrafine particles: A review about their health effects, presence, generation, and measurements in indoor environments. Build. Environ. 2022, 216, 108992. [Google Scholar] [CrossRef]
- Hajkowicz, S.A.; Cook, H.; Littleboy, A. Our Future World: Global Megatrends That Will Change the Way We Live; CSIRO: Canberra, Australia, 2012.
- Chew, N.W.; Ng, C.H.; Tan, D.J.H.; Kong, G.; Lin, C.; Chin, Y.H.; Lim, W.H.; Huang, D.Q.; Quek, J.; Fu, C.E.; et al. The global burden of metabolic disease: Data from 2000 to 2019. Cell Metab. 2023, 35, 414–428.e3. [Google Scholar] [CrossRef]
- Rechel, B.; Doyle, Y.; Grundy, E.; McKee, M. How Can Health Systems Respond to Population Ageing? Technical Report; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2009. [Google Scholar]
- Haq, G.; Gutman, G. Climate gerontology: Meeting the challenge of growing old in a changing climate. Z. Für Gerontol. Und Geriatr. 2014, 47, 462–467. [Google Scholar] [CrossRef]
- Meade, R.D.; Akerman, A.P.; Notley, S.R.; McGinn, R.; Poirier, P.; Gosselin, P.; Kenny, G.P. Physiological factors characterizing heat-vulnerable older adults: A narrative review. Environ. Int. 2020, 144, 105909. [Google Scholar] [CrossRef]
- GOV.UK. GOV £10.7 Million in Funding for Local AUTHORITIES to Improve Air Quality. 2023. Available online: https://www.gov.uk (accessed on 21 July 2023).
- GOV. Available online: https://www.gov.uk/guidance/driving-in-a-clean-air-zone (accessed on 24 July 2023).
- Chamberlain, R.C.; Fecht, D.; Davies, B.; Laverty, A.A. Health effects of low emission and congestion charging zones: A systematic review. Lancet Public Health 2023, 8, e559–e574. [Google Scholar] [CrossRef]
- GOV. New Legally Binding Environment Targets Set Out. 2022. Available online: https://www.gov.uk/government/news/new-legally-binding-environment-targets-set-out (accessed on 1 February 2023).
- Vandyck, T.; Keramidas, K.; Kitous, A.; Spadaro, J.V.; Van Dingenen, R.; Holland, M.; Saveyn, B. Air quality co-benefits for human health and agriculture counterbalance costs to meet Paris Agreement pledges. Nat. Commun. 2018, 9, 4939. [Google Scholar] [CrossRef] [PubMed]
- Ao, C.-K.; Dong, Y.; Kuo, P.-F. Industrialization, indoor and ambient air quality, and elderly mental health. China Econ. Rev. 2021, 69, 101676. [Google Scholar] [CrossRef]
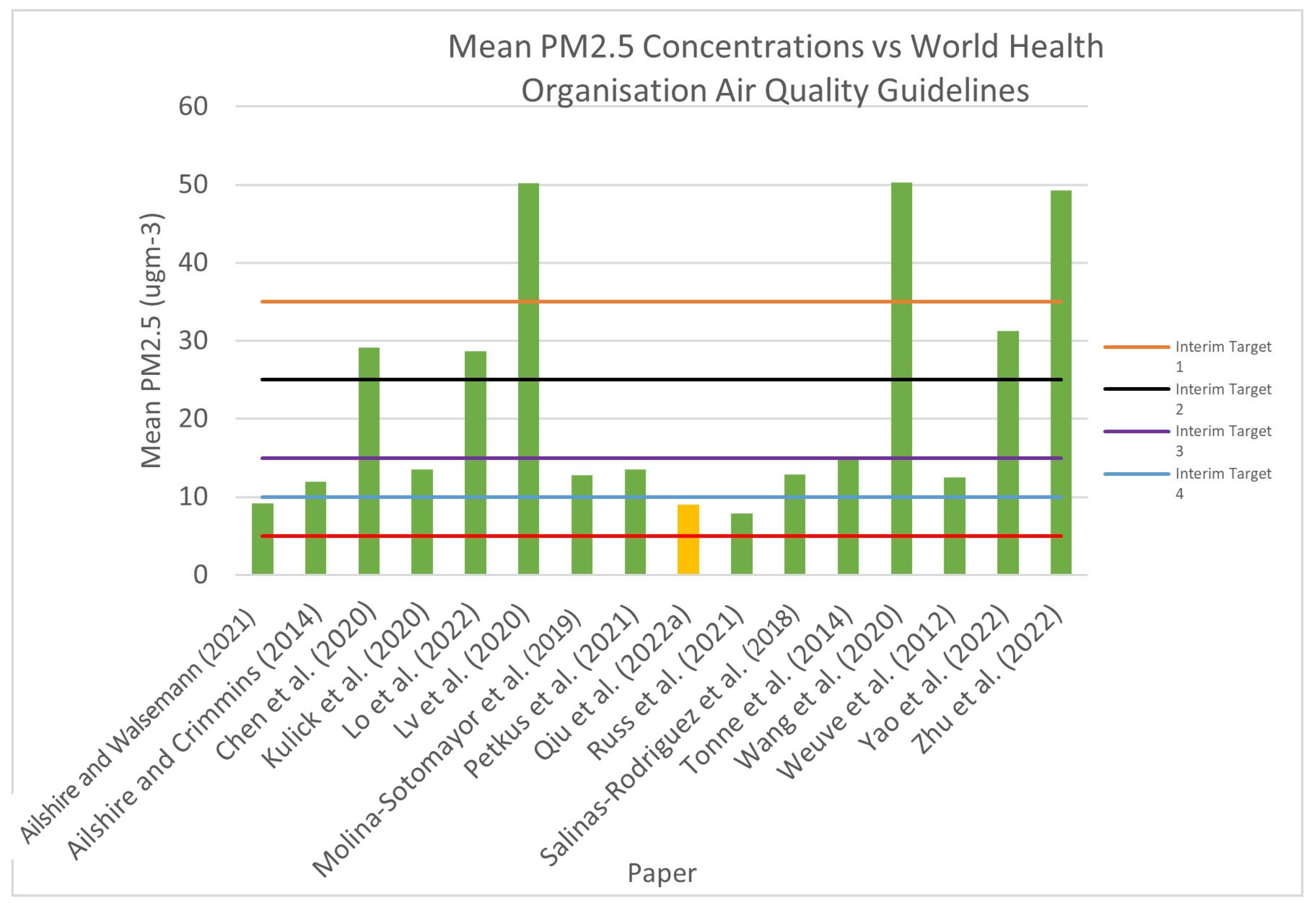
| Pollutant | Averaging Time | WHO 2005 Guideline | WHO 2021 Update | ||||
|---|---|---|---|---|---|---|---|
| Interim Targets | Guideline | ||||||
| 1 | 2 | 3 | 4 | ||||
| Fine Particles, PM2.5 | Daily (24 h) mean (μgm−3) | 10 | 35 | 25 | 15 | 10 | 5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hodgson, J.R.; Benkowitz, C.; Castellani, B.C.; Ellison, A.; Yassaie, R.; Twohig, H.; Bhudia, R.; Jutila, O.-E.I.; Fowler-Davis, S. A Scoping Review of the Effects of Ambient Air Quality on Cognitive Frailty. Environments 2024, 11, 4. https://doi.org/10.3390/environments11010004
Hodgson JR, Benkowitz C, Castellani BC, Ellison A, Yassaie R, Twohig H, Bhudia R, Jutila O-EI, Fowler-Davis S. A Scoping Review of the Effects of Ambient Air Quality on Cognitive Frailty. Environments. 2024; 11(1):4. https://doi.org/10.3390/environments11010004
Chicago/Turabian StyleHodgson, James Robert, Charlotte Benkowitz, Brian C. Castellani, Amanda Ellison, Rammina Yassaie, Helen Twohig, Roshni Bhudia, Otto-Emil Ilmari Jutila, and Sally Fowler-Davis. 2024. "A Scoping Review of the Effects of Ambient Air Quality on Cognitive Frailty" Environments 11, no. 1: 4. https://doi.org/10.3390/environments11010004
APA StyleHodgson, J. R., Benkowitz, C., Castellani, B. C., Ellison, A., Yassaie, R., Twohig, H., Bhudia, R., Jutila, O.-E. I., & Fowler-Davis, S. (2024). A Scoping Review of the Effects of Ambient Air Quality on Cognitive Frailty. Environments, 11(1), 4. https://doi.org/10.3390/environments11010004