
Exploring the Experiences and Current Support of Children and Young People with Selective Mutism Within Mainstream Secondary Schools

Abstract
1. Introduction
1.1. Selective Mutism
1.2. Presentation
1.3. Support and Intervention
1.4. Views of CYP with SM
1.5. Research Questions
- How do secondary school-aged young people with SM experience school?
- Can we define and identify effective support for young people with selective mutism within secondary school?
2. Materials and Methods
2.1. Epistemological Position
2.2. Design
2.3. Participants and Sampling
2.4. Data Collection Methods
- Phase 1: Gathering informed assent and building rapport
- Phase 2: Gathering young people’s experiences
- Phase 3: Gathering information from key stakeholders
2.5. Data Analysis
3. Results
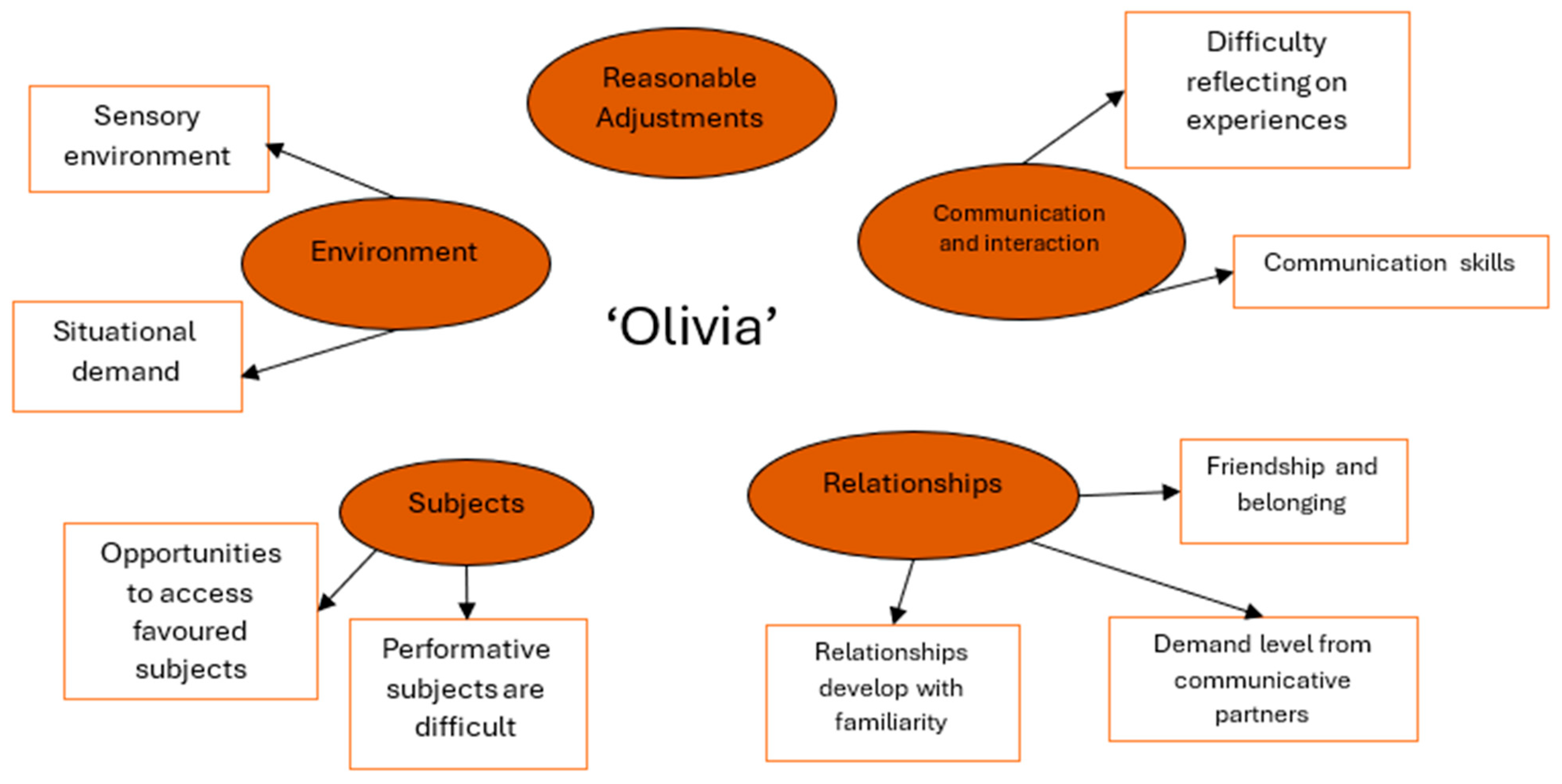
3.1. ‘Olivia’
3.1.1. Context
3.1.2. Interview Process
3.1.3. Environment
3.1.4. Subjects
3.1.5. Relationships
3.1.6. Communication and Interaction
3.1.7. Reasonable Adjustments
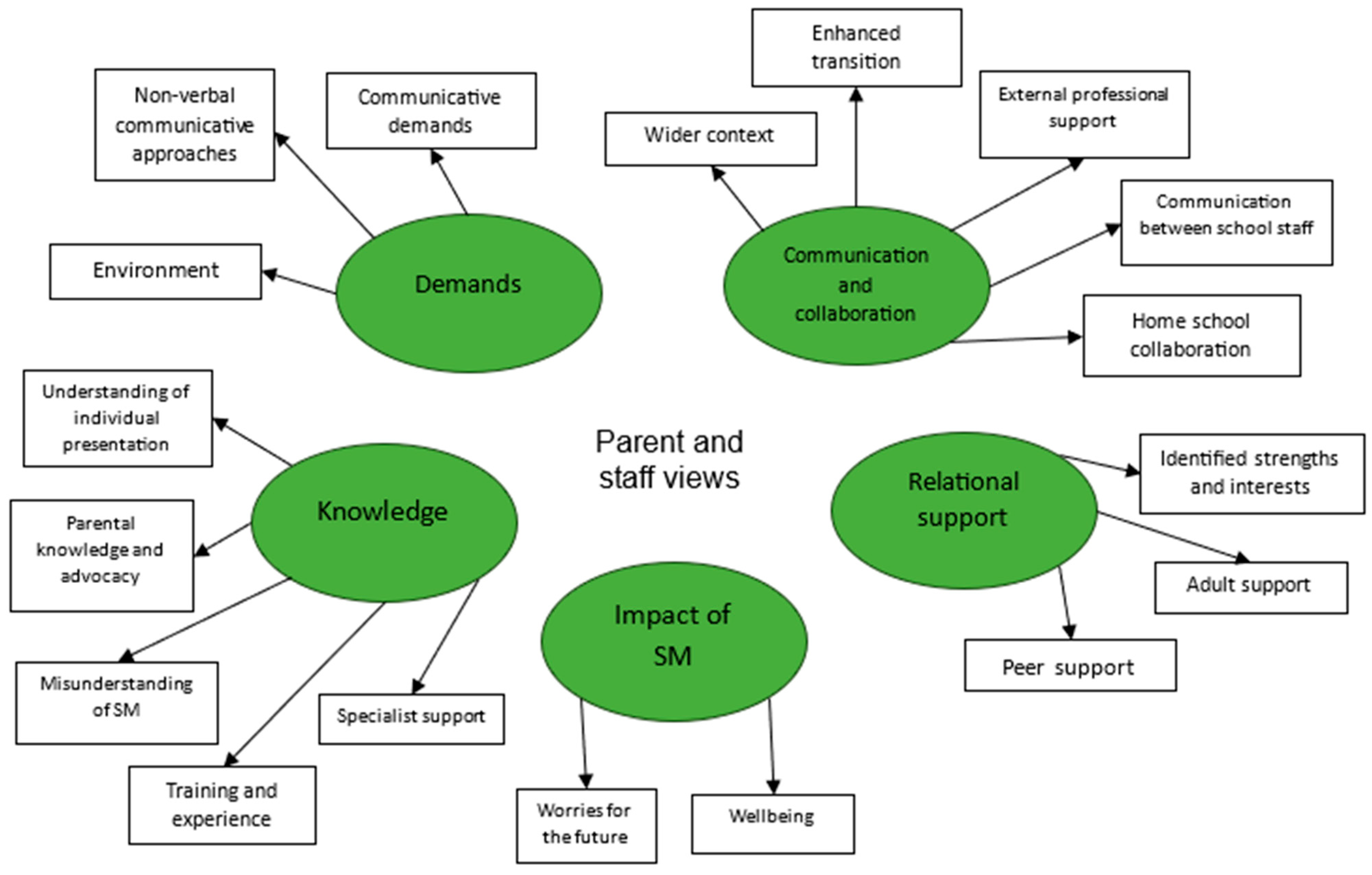
3.1.8. Parent and Staff Perspectives
3.2. ‘Catherine’
3.2.1. Context
3.2.2. Interview Process
3.2.3. Relationships
3.2.4. Difficulty with Communication Skills
3.2.5. Communicative Demand
3.2.6. Consistent Support
3.2.7. Parent and Staff Perspectives
3.3. ‘Michael’
3.3.1. Context
3.3.2. Interview Process
3.3.3. Themes
3.3.4. Building and Developing Relationships
3.3.5. Strengths in Skills for Communication
3.3.6. The Need for Further Support
Parent and Staff Perspectives
3.4. Cross-Case Analysis
4. Discussion
4.1. Key Findings and Implications for Practice
4.2. Knowledge and Understanding
4.3. Relationships
4.4. Communication and Collaboration
4.5. Individual Experience and Support
4.6. Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| APA | American Psychological Association |
| ASD | Autism Spectrum Disorder |
| CYP | Children and young people |
| DFE | Department for Education |
| DSM | Diagnostic and Statistical manual of mental disorders |
| EHCP | Education, health and care plan |
| ICD | International classification of diseases |
| NHS | National Health Service |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| RCSLT | Royal College of Speech and Language Therapists |
| RTA | Reflexive thematic analysis |
| SAD | Social anxiety disorder |
| SALT | Speech and language therapist |
| SEN | Special educational needs |
| SENDCO | Special educational needs and disabilities coordinator |
| SM | Selective mutism |
| SMIRA | Selective mutism information and research association |
| UK | United Kingdom |
| YP | Young person |
References
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatry Publishing. [Google Scholar]
- Beidel, D. C., Alfano, C. A., Kofler, M. J., Rao, P. A., & Scharfstein, L. A. (2014). The impact of social skills training for social anxiety disorder: A randomized controlled trial. Journal of Anxiety Disorders, 28(8), 908–918. [Google Scholar] [CrossRef] [PubMed]
- Bergman, R. L., Gonzalez, A., Piacentini, J., & Keller, M. L. (2013). Integrated behavior therapy for selective mutism: A randomized controlled pilot study. Behaviour Research and Therapy, 51(10), 680–689. [Google Scholar] [CrossRef]
- Berko, Z. (2013). “Psychic Twins”: A psycho-dynamically informed treatment of a selectively mute adolescent and her mother. Journal of Infant, Child, and Adolescent Psychotherapy, 12(4), 307–320. [Google Scholar] [CrossRef]
- Blanchard, B. L. (2021). CommuniTeen: A group treatment program for adolescents with selective mutism [Doctoral dissertation, Widener University]. [Google Scholar]
- Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. [Google Scholar] [CrossRef]
- Braun, V., & Clarke, V. (2019). Reflecting on reflexive thematic analysis. Qualitative Research in Sport, Exercise and Health, 11(4), 589–597. [Google Scholar] [CrossRef]
- Chavira, D. A., Shipon-Blum, E., Hitchcock, C., Cohan, S., & Stein, M. B. (2007). Selective mutism and social anxiety disorder: All in the family? Journal of the American Academy of Child & Adolescent Psychiatry, 46, 1464–1472. [Google Scholar]
- Children Act. (1989). Children Act 1989, c. 41 (UK). Available online: https://www.legislation.gov.uk/ukpga/1989/41/contents (accessed on 18 June 2025).
- Cline, T., & Baldwin, S. (1994). Selective mutism in children. Whurr. [Google Scholar]
- Cohen, L., Manion, L., & Morrison, K. (2013). Research methods in education (6th ed.). Routledge. [Google Scholar]
- Cox, P., & McDonald, J. M. (2018). Analysis and critique of ‘Transforming children and young people’s mental health provision: A green paper’: Some implications for refugee children and young people. Journal of Child Health Care, 24(3), 338–350. [Google Scholar] [CrossRef]
- Cummings, L. (2021). Handbook of pragmatic language disorders: Complex and underserved populations. Springer Nature. [Google Scholar]
- Davidson, M. (2012). Selective mutism: Exploring the knowledge and needs of teachers [Doctoral dissertation, Rutgers The State University of New Jersey]. [Google Scholar]
- Easton, G. (2010). Critical realism in case study research. Industrial Marketing Management, 39(1), 118–128. [Google Scholar] [CrossRef]
- Giddens, A. (1986). Sociology: A brief but critical introduction. Bloomsbury Publishing. [Google Scholar]
- Hipolito, G., Pagnamenta, E., Stacey, H., Wright, E., Joffe, V., Murayama, K., & Creswell, C. (2023). A systematic review and meta-analysis of nonpharmacological interventions for children and adolescents with selective mutism. JCPP Advances, 3(3), e12166. [Google Scholar] [CrossRef]
- Johnson, M., & Wintgens, A. (2012). Can I tell you about selective mutism?: A guide for friends, family and professionals. Jessica Kingsley Publishers. [Google Scholar]
- Johnson, M., & Wintgens, A. (2016). The selective mutism resource manual (2nd ed.). Routledge. [Google Scholar]
- Manassis, K. (2009). Silent suffering: Understanding and treating children with selective mutism. Expert Review of Neurotherapeutics, 9(2), 235–243. [Google Scholar] [CrossRef]
- Mulligan, C. A., Hale, J. B., & Shipon-Blum, E. (2015). Selective mutism: Identification of subtypes and implications for treatment. Journal of Education and Human Development, 4(1), 79–96. [Google Scholar] [CrossRef]
- Muris, P., Monait, N., Weijsters, L., & Ollendick, T. H. (2021). Symptoms of selective mutism in non-clinical 3-to 6-year-old children: Relations with social anxiety, autistic features, and behavioral inhibition. Frontiers in Psychology, 12, 669907. [Google Scholar] [CrossRef]
- Muris, P., & Ollendick, T. H. (2021a). Current challenges in the diagnosis and management of selective mutism in children. Psychology Research and Behavior Management, 14, 159–167. [Google Scholar] [CrossRef]
- Muris, P., & Ollendick, T. H. (2021b). Selective mutism and its relations to social anxiety disorder and autism spectrum disorder. Clinical Child and Family Psychology Review, 24(2), 294–325. [Google Scholar] [CrossRef] [PubMed]
- NHS. (2019). Selective mutism. Available online: https://www.nhs.uk/conditions/selective-mutism/.
- Oerbeck, B., Overgaard, K. R., Bergman, R. L., Pripp, A. H., & Kristensen, H. (2020). The selective mutism questionnaire: Data from typically developing children and children with selective mutism. Clinical Child Psychology and Psychiatry, 25(4), 754–765. [Google Scholar] [CrossRef]
- Omdal, H. (2007). Can adults who have recovered from selective mutism in childhood and adolescence tell us anything about the nature of the condition and/or recovery from it? European Journal of Special Needs Education, 22(3), 237–253. [Google Scholar] [CrossRef]
- Omdal, H. (2008). Including children with selective mutism in mainstream schools and kindergartens: Problems and possibilities. International Journal of Inclusive Education, 12(3), 301–315. [Google Scholar] [CrossRef]
- Omdal, H., & Galloway, D. (2007). Interviews with selectively mute children. Emotional and Behavioural Difficulties, 12(3), 205–214. [Google Scholar] [CrossRef]
- Ponzurick, J. M. (2012). Selective mutism: A team approach to assessment and treatment in the school setting. The Journal of School Nursing, 28(1), 31–37. [Google Scholar] [CrossRef]
- Reuther, E. T., Davis, T. E., Moree, B. N., & Matson, J. L. (2011). Treating selective mutism using modular CBT for child anxiety: A case study. Journal of Clinical Child and Adolescent Psychology, 40(1), 156–163. [Google Scholar] [CrossRef]
- Robson, C. (2011). Real world research (3rd ed.). John Wiley & Sons Ltd. [Google Scholar]
- Roe, V., & Phil, B. (2011, September 6–8). Silent voices: Listening to young people with selective mutism. British Educational Research Association Annual Conference, London, UK. [Google Scholar]
- Royal College of Speech and Language Therapists. (2019). Selective mutism—Overview. Available online: https://www.rcslt.org/speech-and-language-therapy/clinicalinforma3on/selective-mutism (accessed on 18 June 2025).
- Schwenck, C., Gensthaler, A., & Vogel, F. (2021). Anxiety levels in children with selective mutism and social anxiety disorder. Current Psychology, 40(12), 6006–6013. [Google Scholar] [CrossRef]
- Selective Mutism Information & Research Association. (2019). Available online: http://www.selectivemutism.org.uk (accessed on 18 June 2025).
- Sharkey, L., & McNicholas, F. (2012). Selective mutism: A prevalence study of primary school children in the Republic of Ireland. Irish Journal of Psychological Medicine, 29(1), 36–40. [Google Scholar] [CrossRef]
- Shimoni, H. N., Alon, T., Zalsman, G., Apter, A., & Gothelf, D. (2025). The clinical phenotype of early selective mutism and later autism spectrum disorder in girls: A case series. Children, 12(2), 267. [Google Scholar] [CrossRef] [PubMed]
- Smillie, I., & Newton, M. (2020). Educational psychologists’ practice: Obtaining and representing young people’s views. Educational Psychology in Practice, 36(3), 328–344. [Google Scholar] [CrossRef]
- Sutton, C. (2013). Selective mutism in adults: An exploratory study [Unpublished Master’s thesis, University of Chester]. Available online: http://www.ispeak.org.uk/Download.ashx (accessed on 18 June 2025).
- United Nations. (2006). United Nations convention on the rights of the child (UNCRC). UN. [Google Scholar]
- Vygotsky, L. S. (1978). Mind in society: The development of higher psychological processes. Harvard University Press. [Google Scholar]
- Wade, R. (2022). My ideal school: Using a personal construct psychology technique to explore and understand the school constructs of children and young people identified as having selective mutism [Doctoral dissertation, University of East Anglia]. [Google Scholar]
- White, J., & Bond, C. (2022). The role that schools hold in supporting young people with selective mutism: A systematic literature review. Journal of Research in Special Educational Needs, 22(3), 232–242. [Google Scholar] [CrossRef]
- White, J., Bond, C., & Carroll, C. (2022). An exploration of how selective mutism training informs teachers’ understanding and practice. Support for Learning, 37(1), 3–20. [Google Scholar] [CrossRef]
- Yin, R. (2014). Case study research: Design and methods (5th ed.). Sage Publications, Inc. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case Study | Young Person Characteristics | School Characteristics | Stakeholders Recruited |
|---|---|---|---|
| Case study 1, Pseudonym Olivia | Female 13 years old Diagnosed with low-profile SM Co-occurring diagnoses of ASD and SAD (social anxiety disorder) No education, health and care plan in place in school | Elective grammar school Smaller than average number of pupils Average to higher levels of SEN in school | Special educational needs coordinator Parents (mother and father) Key worker Assistant Psychologist |
| Case study 2, Pseudonym Catherine Case study 3, Pseudonym Michael | Female 12 years old Diagnosed with SM Co-occurring diagnoses of ASD, anxiety, and medical needs Education, health and care plan in place Male 12 years old Diagnosed with selective mutism Education, health and care plan in place | School within a lower socioeconomic area Smaller than average number of pupils Significantly higher than average levels of SEN Rural area Average number of pupils Lower than average level of SEN in school | Special educational needs coordinator Mother Form tutor Special educational needs coordinator Mother Key worker |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Walker, S.; Bond, C. Exploring the Experiences and Current Support of Children and Young People with Selective Mutism Within Mainstream Secondary Schools. Behav. Sci. 2025, 15, 947. https://doi.org/10.3390/bs15070947
Walker S, Bond C. Exploring the Experiences and Current Support of Children and Young People with Selective Mutism Within Mainstream Secondary Schools. Behavioral Sciences. 2025; 15(7):947. https://doi.org/10.3390/bs15070947
Chicago/Turabian StyleWalker, Sophie, and Caroline Bond. 2025. "Exploring the Experiences and Current Support of Children and Young People with Selective Mutism Within Mainstream Secondary Schools" Behavioral Sciences 15, no. 7: 947. https://doi.org/10.3390/bs15070947
APA StyleWalker, S., & Bond, C. (2025). Exploring the Experiences and Current Support of Children and Young People with Selective Mutism Within Mainstream Secondary Schools. Behavioral Sciences, 15(7), 947. https://doi.org/10.3390/bs15070947