
What Works for Whom? The Influence of Problem Severity, Maladaptive Perfectionism, and Perceived Parental Pressure on the Effectiveness of a School-Based Performance Anxiety Program


Abstract
1. Introduction
2. Methods
2.1. Design and Procedure
2.2. Participants
2.3. Performance Anxiety Program
2.4. Instruments
2.4.1. Performance Anxiety
2.4.2. Moderators
2.5. Data Analysis
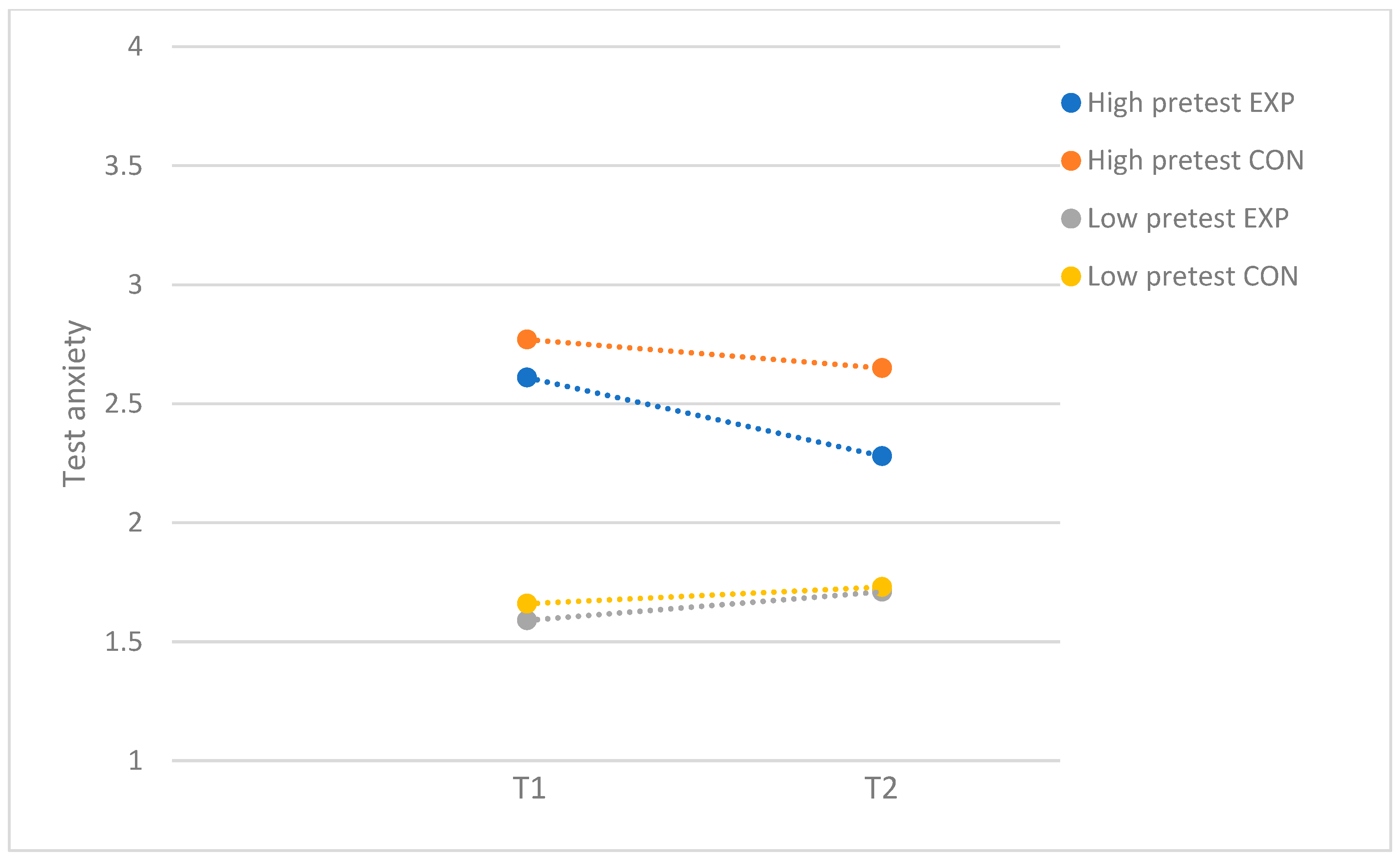
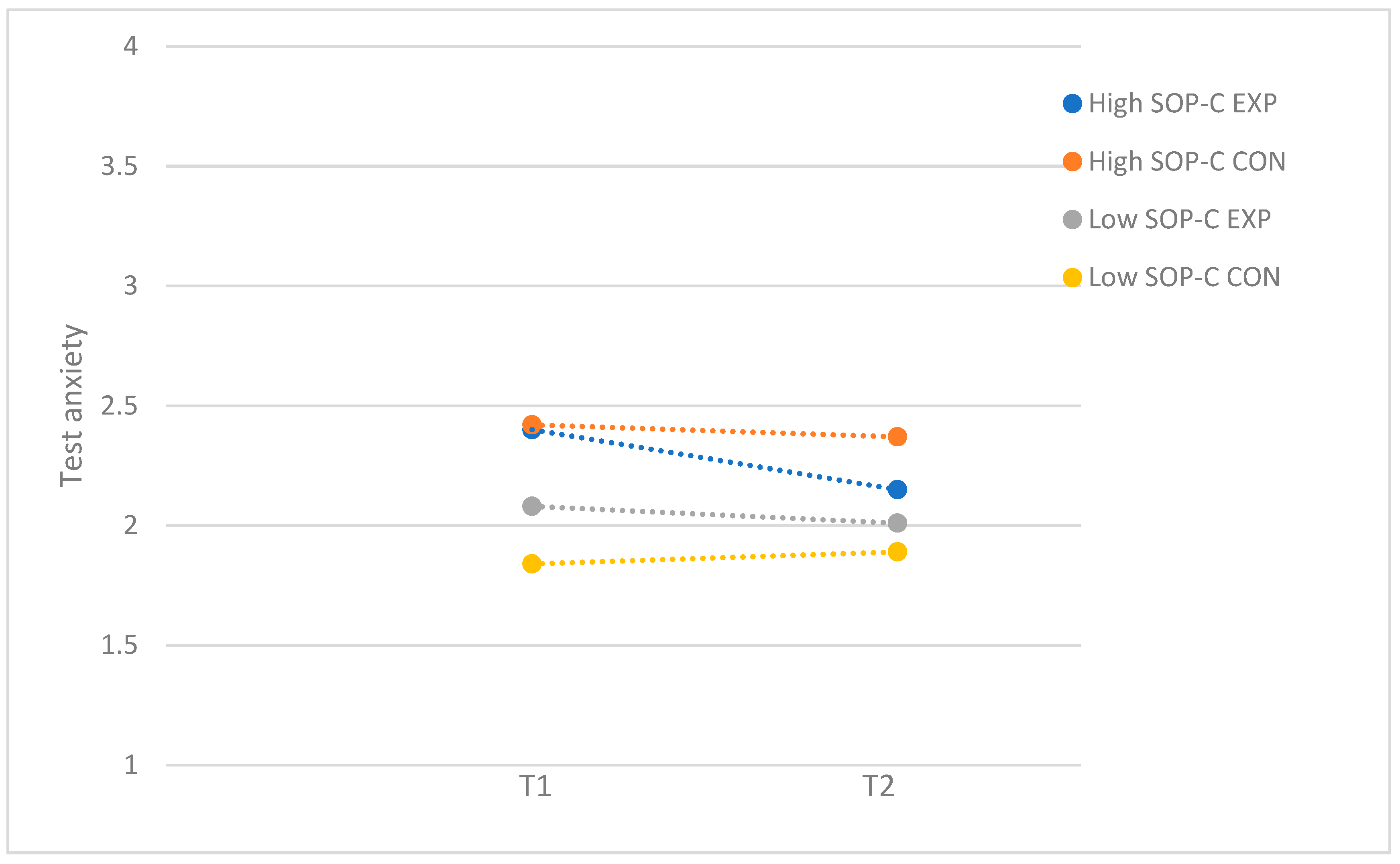
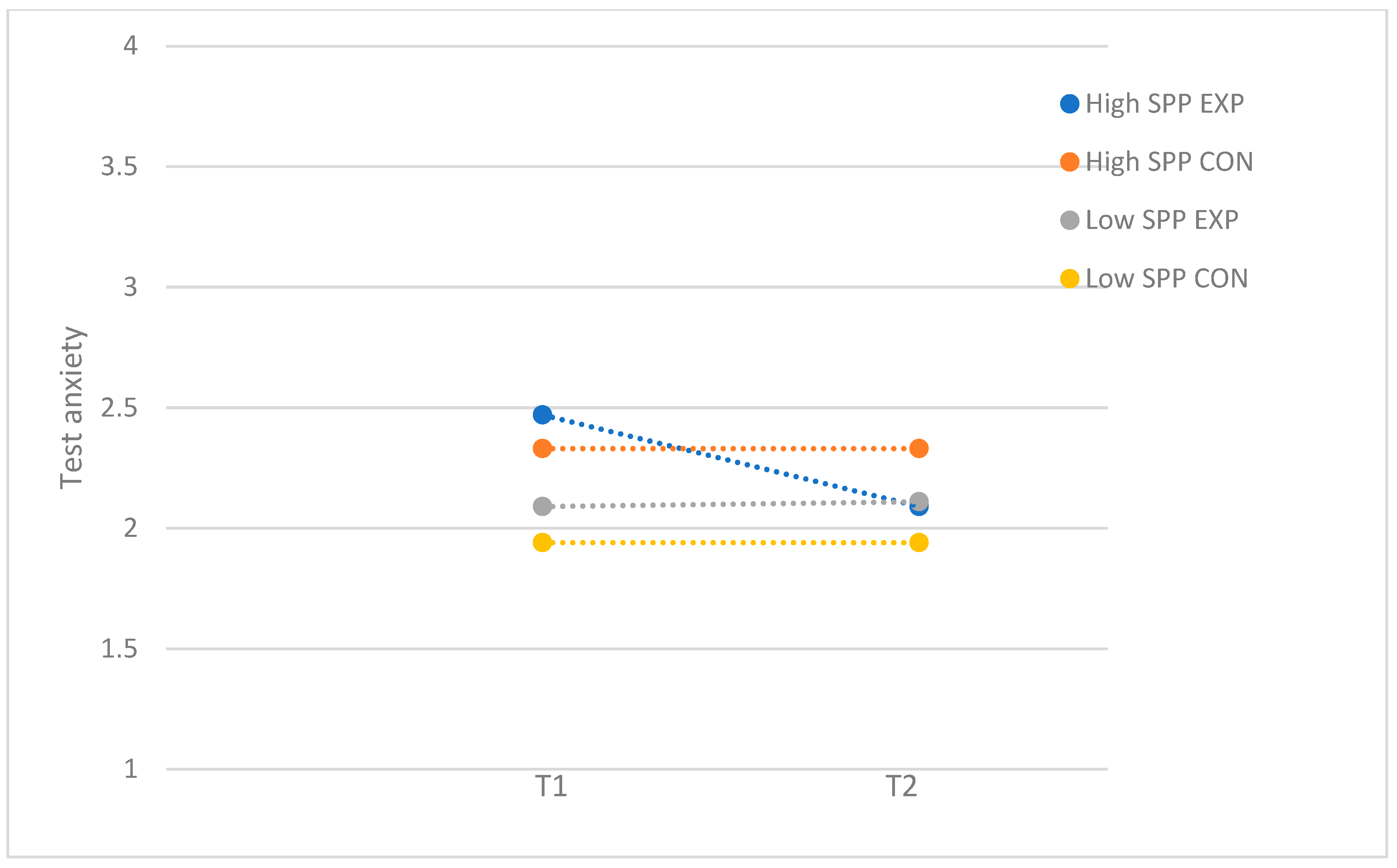
3. Results
3.1. Full Sample
3.2. Subsample with Higher Program Attendance
4. Discussion
Strengths and Limitations
5. Conclusions and Implications
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| RCT | Randomized controlled trial |
| SOP | Self-oriented perfectionism |
| SPP | Socially prescribed perfectionism |
| CBT | Cognitive behavioral therapy |
| SOP-C | Self-oriented critical perfectionism or self-criticism |
References
- Andersen, S. L., & Teicher, M. H. (2008). Stress, sensitive periods and maturational events in adolescent depression. Trends in Neurosciences, 31(4), 183–191. [Google Scholar] [CrossRef] [PubMed]
- Anniko, M. K., Boersma, K., & Tillfors, M. (2019). Sources of stress and worry in the development of stress-related mental health problems: A longitudinal investigation from early-to mid-adolescence. Anxiety, Stress and Coping, 32(2), 155–167. [Google Scholar] [CrossRef] [PubMed]
- Boer, M., van Dorsselaer, S., de Looze, M., de Roos, S., Brons, H., van den Eijnden, R., Monshouwer, K., Huijnk, W., ter Bogt, T., Vollebergh, W., & Stevens, G. (2021). HBSC 2021 Gezondheid en welzijn van jongeren in Nederland. Universiteit Utrecht. [Google Scholar]
- Branje, S., de Moor, E. L., Spitzer, J., & Becht, A. I. (2021). Dynamics of identity development in adolescence: A decade in review. Journal of Research on Adolescence, 31(4), 908–927. [Google Scholar] [CrossRef] [PubMed]
- Brière, F. N., Rohde, P., Shaw, H., & Stice, E. (2014). Moderators of two indicated cognitive-behavioral depression prevention approaches for adolescents in a school-based effectiveness trial. Behaviour Research and Therapy, 53(1), 55–62. [Google Scholar] [CrossRef]
- Brown, B. B. (2004). Adolescents’ relationships with peers. In Handbook of adolescent psychology (pp. 363–394). John Wiley & Sons Inc. [Google Scholar]
- Chappel, A. M., Suldo, S. M., & Ogg, J. A. (2014). Associations between adolescents’ family stressors and life satisfaction. Journal of Child and Family Studies, 23(1), 76–84. [Google Scholar] [CrossRef]
- Cohen, J. (1988). Statistical power analysis for the social sciences. Erlbaum. [Google Scholar]
- Conroy, D. E., Willow, J. P., & Metzler, J. N. (2002). Multidimensional fear of failure measurement: The Performance Failure Appraisal Inventory. Journal of Applied Sport Psychology, 14, 76–90. [Google Scholar] [CrossRef]
- Correia, M. C., Rosado, A. F., & Serpa, S. (2018). Fear of failure and perfectionism in sport miedo a fallar y perfeccionismo en el deporte medo de falhar e perfeccionismo no desporto. Faculty of Human Kinetics, University of Lisbon, Portugal, 18, 161–172. [Google Scholar]
- Cosma, A., Stevens, G. W. J. M., Martin, G., Duinhof, E. L., Walsh, S. D., Garcia-Moya, I., Költő, A., Gobina, I., Canale, N., Catunda, C., Inchley, J., & de Looze, M. (2020). Cross-national time trends in adolescent mental well-being from 2002 to 2018 and the explanatory role of schoolwork pressure. Journal of Adolescent Health, 66(6), S50–S58. [Google Scholar] [CrossRef]
- Cosma, A., Stevens, G. W. J. M., Vollebergh, W. A. M., & De Looze, M. (2021). Time trends in schoolwork pressure among Dutch adolescents, 2001–2017: Gender and educational differences. Scandinavian Journal of Public Health, 50, 538–541. [Google Scholar] [CrossRef]
- Creswell, C., Willetts, L., Murray, L., Singhal, M., & Cooper, P. (2008). Treatment of child anxiety: An exploratory study of the role of maternal anxiety and behaviours in treatment outcome. Clinical Psychology and Psychotherapy, 15(1), 38–44. [Google Scholar] [CrossRef]
- Curran, T., & Hill, A. P. (2019). Perfectionism is increasing over time: A meta-analysis of birth cohort differences from 1989 to 2016. Psychological Bulletin, 145(4), 410–429. [Google Scholar] [CrossRef] [PubMed]
- de Mooij, B., Fekkes, M., Scholte, R. H. J., & Overbeek, G. (2020). Effective components of social skills training programs for children and adolescents in nonclinical samples: A multilevel meta-analysis. Clinical Child and Family Psychology Review, 23(2), 250–264. [Google Scholar] [CrossRef] [PubMed]
- Dunn, J. G. H., Gotwals, J. K., Causgrove Dunn, J., & Lizmore, M. R. (2022). Perceived parental pressure and perceived coach pressure in adolescent and adult sport. Psychology of Sport and Exercise, 59, 102100. [Google Scholar] [CrossRef]
- Durlak, J. A., Weissberg, R. P., Dymnicki, A. B., Taylor, R. D., & Schellinger, K. B. (2011). The impact of enhancing students’ social and emotional learning: A meta-analysis of school-based universal interventions. Child Development, 82(1), 405–432. [Google Scholar] [CrossRef]
- Essau, C. A., Conradt, J., Sasagawa, S., & Ollendick, T. H. (2012). Prevention of anxiety symptoms in children: Results from a universal school-based trial. Behavior Therapy, 43(2), 450–464. [Google Scholar] [CrossRef]
- Festen, H., Hartman, C. A., Hogendoorn, S., de Haan, E., Prins, P. J. M., Reichart, C. G., Moorlag, H., & Nauta, M. H. (2013). Temperament and parenting predicting anxiety change in cognitive behavioral therapy: The role of mothers, fathers, and children. Journal of Anxiety Disorders, 27(3), 289–297. [Google Scholar] [CrossRef]
- Flett, G. L., & Hewitt, P. L. (2002). Perfectionism and maladjustment: An overview of theoretical, definitional, and treatment issues (pp. 5–31). American Psychological Association. [Google Scholar] [CrossRef]
- Flett, G. L., Hewitt, P. L., Besser, A., Su, C., Vaillancourt, T., Boucher, D., Munro, Y., Davidson, L. A., & Gale, O. (2016). The Child–Adolescent Perfectionism Scale: Development, psychometric properties, and associations with stress, distress, and psychiatric symptos. Journal of Psychoeducational Assessment, 34(7), 634–652. [Google Scholar] [CrossRef]
- Frost, R. O., Marten, P., Lahart, C., & Rosenblate, R. (1990). The dimensions of perfectionism. Cognitive Therapy and Research, 14(5), 449–468. [Google Scholar] [CrossRef]
- Hewitt, P. L., Smith, M. M., Deng, X., Chen, C., Ko, A., Flett, G. L., & Patterson, R. J. (2020). The perniciousness of perfectionism in group therapy for depression: A test of the perfectionism social disconnection model. Psychotherapy, 57(2), 206. [Google Scholar] [CrossRef]
- Horowitz, J. L., & Garber, J. (2006). The prevention of depressive symptoms in children and adolescents: A meta-analytic review. Journal of Consulting and Clinical Psychology, 74(3), 401–415. [Google Scholar] [CrossRef]
- Jacobsen, B., & Nørup, I. (2020). Young people’s mental health: Exploring the gap between expectation and experience. Educational Research, 62(3), 249–265. [Google Scholar] [CrossRef]
- Kleinjan, M., Pieper, I., Stevens, G., van de Klundert, N., Rombouts, M., Boer, M., & Lammers, J. (2020). Geluk onder druk? Onderzoek naar het mentaal welbevinden van jongeren in Nederland. UNICEF Netherlands. [Google Scholar]
- Limburg, K., Watson, H. J., Hagger, M. S., & Egan, S. J. (2017). The relationship between perfectionism and psychopathology: A meta-analysis. Journal of Clinical Psychology, 73(10), 1301–1326. [Google Scholar] [CrossRef] [PubMed]
- Menting, A. T. A., Orobio de Castro, B., & Matthys, W. (2013). Effectiveness of the incredible years parent training to modify disruptive and prosocial child behavior: A meta-analytic review. Clinical Psychology Review, 33(8), 901–913. [Google Scholar] [CrossRef] [PubMed]
- Miller, R., Hilsenroth, M. J., & Hewitt, P. L. (2017). Perfectionism and therapeutic alliance: A review of the clinical research. Research in Psychotherapy: Psychopathology, Process and Outcome, 20(1), 19–26. [Google Scholar] [CrossRef]
- Mitchell, J. H., Newall, C., Broeren, S., & Hudson, J. L. (2013). The role of perfectionism in cognitive behaviour therapy outcomes for clinically anxious children. Behaviour Research and Therapy, 51(9), 547–554. [Google Scholar] [CrossRef]
- Morris, L., & Lomax, C. (2014). Review: Assessment, development, and treatment of childhood perfectionism: A systematic review. Child and Adolescent Mental Health, 19(4), 225–234. [Google Scholar] [CrossRef]
- Nobel, R., Manassis, K., & Wilansky-Traynor, P. (2012). The role of perfectionism in relation to an intervention to reduce anxious and depressive symptoms in children. Journal of Rational—Emotive and Cognitive—Behavior Therapy, 30(2), 77–90. [Google Scholar] [CrossRef]
- Noble, C. M., Gnilka, P. B., Ashby, J. S., & McLaulin, S. E. (2017). Perfectionism, shame, and trichotillomania symptoms in clinical and nonclinical samples. Journal of Mental Health Counseling, 39(4), 335–350. [Google Scholar] [CrossRef]
- Nordahl, H. M., Wells, A., Olsson, C. A., & Bjerkeset, O. (2010). Association between abnormal psychosocial situations in childhood, generalized anxiety disorder and oppositional defiant disorder. Australian and New Zealand Journal of Psychiatry, 44(9), 852–858. [Google Scholar] [CrossRef]
- Núñez-Regueiro, F., & Núñez-Regueiro, S. (2021). Identifying salient stressors of adolescence: A systematic review and content analysis. Journal of Youth and Adolescence, 50, 2533–2556. [Google Scholar] [CrossRef]
- O’Connor, R. C., Dixon, D., & Rasmussen, S. (2009). The structure and temporal stability of the Child and Adolescent Perfectionism Scale. Psychological Assessment, 21(3), 437–443. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, R. C., Rasmussen, S., & Hawton, K. (2010). Predicting depression, anxiety and self-harm in adolescents: The role of perfectionism and acute life stress. Behaviour Research and Therapy, 48(1), 52–59. [Google Scholar] [CrossRef] [PubMed]
- O’Rourke, D. J., Smith, R. E., Smoll, F. L., & Cumming, S. P. (2011). Trait anxiety in young athletes as a function of parental pressure and motivational climate: Is parental pressure always harmful? Journal of Applied Sport Psychology, 23(4), 398–412. [Google Scholar] [CrossRef]
- Psychometrica. (n.d.). Computation of effect sizes. Available online: https://www.psychometrica.de/effect_size.html (accessed on 20 December 2024).
- Romeo, R. D. (2013). The teenage brain: The stress response and the adolescent brain. Current Directions in Psychological Science, 22(2), 140–145. [Google Scholar] [CrossRef]
- Smith, M. M., Sherry, S. B., Ge, S. Y. J., Hewitt, P. L., Flett, G. L., & Baggley, D. L. (2022). Multidimensional perfectionism turns 30: A review of known knowns and known unknowns. Canadian Psychology, 63(1), 16–31. [Google Scholar] [CrossRef]
- Snyder, H. R., Young, J. F., & Hankin, B. L. (2017). Chronic stress exposure and generation are related to the P-factor and externalizing specific psychopathology in youth. Journal of Clinical Child and Adolescent Psychology, 48(2), 306–315. [Google Scholar] [CrossRef]
- Soares, D., & Woods, K. (2020). An international systematic literature review of test anxiety interventions 2011–2018. Pastoral Care in Education, 38(4), 311–334. [Google Scholar] [CrossRef]
- Spielberger, C. D. (1980). Test anxiety inventory: Sampler set: Manual, test scoring:” test attitude inventory”: Preliminary professional manual. Mind Garden. [Google Scholar]
- Stevens, G., van Dorsselaer, S., Boer, M., De Roos, S., Duinhof, E., ter Bogt, T., van den Eijnden, R., Kuyper, L., Visser, D., Vollebergh, W., & de Looze, M. (2018). HBSC 2017: Gezondheid en welzijn van jongeren in Nederland. Utrecht University. [Google Scholar]
- Stice, E., & Shaw, H. (2004). Eating disorder prevention programs: A meta-analytic review. Psychological Bulletin, 130(2), 206–227. [Google Scholar] [CrossRef]
- Stice, E., Shaw, H., Bohon, C., Marti, C. N., & Rohde, P. (2009). A meta-analytic review of depression prevention programs for children and adolescents: Factors that predict magnitude of intervention effects. Journal of Consulting and Clinical Psychology, 77(3), 486–503. [Google Scholar] [CrossRef]
- Stoeber, J., Otto, K., & Stoll, O. (2006). Multidimensional inventory of perfectionism in sport (MIPS): English version (Unpublised). School of Psychology, University of Kent. Available online: https://core.ac.uk/download/pdf/20524039.pdf (accessed on 20 December 2024).
- Stoeber, J., & Rambow, A. (2007). Perfectionism in adolescent school students: Relations with motivation, achievement, and well-being. Personality and Individual Differences, 42(7), 1379–1389. [Google Scholar] [CrossRef]
- Stricker, J., Schneider, M., & Preckel, F. (2023). Concurrent and predictive relations of multidimensional perfectionism with test anxiety in secondary school students. Anxiety, Stress and Coping, 36(2), 137–146. [Google Scholar] [CrossRef] [PubMed]
- Van der Ploeg, H. M. (1984). The development and validation of the Dutch form of the test anxiety inventory. Applied Psychology, 33(2), 243–254. [Google Scholar] [CrossRef]
- Van Loon, A. W. G., Creemers, H. E., Beumer, W. Y., Okorn, A., Vogelaar, S., Saab, N., Miers, A. C., Westenberg, P. M., & Asscher, J. J. (2020). Can schools reduce adolescent psychological stress? A multilevel meta-analysis of the effectiveness of school-based intervention programs. Journal of Youth and Adolescence, 49, 1127–1145. [Google Scholar] [CrossRef] [PubMed]
- Van Loon, A. W. G., Creemers, H. E., Vogelaar, S., Miers, A. C., Saab, N., Westenberg, P. M., & Asscher, J. J. (2023). The effectiveness of school-based skills-training programs reducing performance or social anxiety: Two randomized controlled trials. Child and Youth Care Forum, 52(6), 1323–1347. [Google Scholar] [CrossRef]
- Van Loon, A. W. G., Creemers, H. E., Vogelaar, S., Saab, N., Miers, A. C., Westenberg, P. M., & Asscher, J. J. (2019). The effectiveness of school-based skills-training programs promoting mental health in adolescents: A study protocol for a randomized controlled study. BMC Public Health, 19(1), 712. [Google Scholar] [CrossRef]
- Vicent, M., Rubio-aparicio, M., Sánchez-meca, J., & Gonzálvez, C. (2019). A reliability generalization meta-analysis of the child and adolescent perfectionism scale. Journal of Affective Disorders, 245, 533–544. [Google Scholar] [CrossRef]
- Vogelaar, S., Miers, A. C., Saab, N., Dusseldorp, E., van Loon, A. W. G., Creemers, H. E., Asscher, J. J., & Westenberg, P. M. (2024). Teaching Adolescents about stress using a universal school-based psychoeducation program: A cluster randomised controlled trial. School Mental Health, 16(2), 467–482. [Google Scholar] [CrossRef]
- Von der Embse, N., Jester, D., Roy, D., & Post, J. (2017). Test anxiety effects, predictors, and correlates: A 30-year meta-analytic review. Journal of Affective Disorders, 227, 483–493. [Google Scholar] [CrossRef]
- Yin, Z., Moore, J. B., Johnson, M. H., Barbeau, P., Cavnar, M., Thornburg, J., & Gutin, B. (2005). The Medical College of Georgia FitKid Project: The relations between program attendance and changes in outcomes in year 1. International Journal of Obesity, 29, S40–S45. [Google Scholar] [CrossRef]
- Zuroff, D. C., Blatt, S. J., Sotsky, S. M., Krupnick, J. L., Martin, D. J., Sanislow, C. A., & Simmens, S. (2000). Relation of therapeutic alliance and perfectionism to outcome in brief outpatient treatment of depression. Journal of Consulting and Clinical Psychology, 68(1), 114–124. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1 a | 2 | 3 | 4 | 5 | 6 | 7 | M | SD | Range | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Gender b | - | - | - | - | ||||||
| 2. Test anxiety (T1) | 0.15 * | - | 2.08 | 0.62 | 1.00–3.90 | |||||
| 3. Test anxiety (T2) | 0.11 | 0.78 *** | - | 2.03 | 0.59 | 1.00–3.55 | ||||
| 4. Fear of failure (T1) | 0.23 ** | 0.65 *** | 0.53 *** | - | 2.16 | 0.91 | 1.00–4.40 | |||
| 5. Fear of failure (T2) | 0.26 *** | 0.60 *** | 0.67 *** | 0.62 *** | - | 2.20 | 0.94 | 1.00–4.80 | ||
| 6. Self-oriented perfectionism-critical (T1) | 0.08 | 0.51 *** | 0.34 *** | 0.49 *** | 0.42 *** | - | 2.43 | 0.99 | 1.00–5.00 | |
| 7. Socially prescribed perfectionism (T1) | −0.02 | 0.42 *** | 0.33 *** | 0.37 *** | 0.28 *** | 0.43 *** | - | 2.59 | 0.93 | 1.00–4.71 |
| 8. Perceived parental pressure (T2) | −0.10 | 0.24 *** | 0.36 *** | 0.22 ** | 0.26 *** | 0.38 *** | 0.50 *** | 2.34 | 1.11 | 1.00–6.00 |
| Test Anxiety (T2) | Fear of Failure (T2) | |||
|---|---|---|---|---|
| F (p) | η2 | F (p) | η2 | |
| Problem severity (pretest levels; T1) | 7.02 (0.01) | 0.04 | 0.36 (0.55) | 0.00 |
| Self-oriented perfectionism-criticism (SOP-C; T1) | 0.85 (0.36) | 0.00 | 0.30 (0.58) | 0.00 |
| Socially prescribed perfectionism (SPP; T1) | 2.80 (0.10) | 0.02 | 0.49 (0.49) | 0.00 |
| Perceived parental pressure (T2) | 1.14 (0.29) | 0.01 | 0.86 (0.36) | 0.01 |
| Test Anxiety (T2) | Fear of Failure (T2) | |||
|---|---|---|---|---|
| F (p) | η2 | F (p) | η2 | |
| Problem severity (pretest levels; T1) | 6.48 (0.01) | 0.04 | 2.19 (0.14) | 0.02 |
| Self-oriented perfectionism-criticism (SOP-C; T1) | 4.04 (0.05) | 0.03 | 0.00 (0.98) | 0.00 |
| Socially prescribed perfectionism (SPP; T1) | 6.15 (0.01) | 0.04 | 0.09 (0.77) | 0.00 |
| Perceived parental pressure (T2) | 0.91 (0.34) | 0.01 | 1.23 (0.27) | 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Loon, A.W.G.; Creemers, H.E.; Vogelaar, S.; Asscher, J.J. What Works for Whom? The Influence of Problem Severity, Maladaptive Perfectionism, and Perceived Parental Pressure on the Effectiveness of a School-Based Performance Anxiety Program. Behav. Sci. 2025, 15, 436. https://doi.org/10.3390/bs15040436
van Loon AWG, Creemers HE, Vogelaar S, Asscher JJ. What Works for Whom? The Influence of Problem Severity, Maladaptive Perfectionism, and Perceived Parental Pressure on the Effectiveness of a School-Based Performance Anxiety Program. Behavioral Sciences. 2025; 15(4):436. https://doi.org/10.3390/bs15040436
Chicago/Turabian Stylevan Loon, Amanda W. G., Hanneke E. Creemers, Simone Vogelaar, and Jessica J. Asscher. 2025. "What Works for Whom? The Influence of Problem Severity, Maladaptive Perfectionism, and Perceived Parental Pressure on the Effectiveness of a School-Based Performance Anxiety Program" Behavioral Sciences 15, no. 4: 436. https://doi.org/10.3390/bs15040436
APA Stylevan Loon, A. W. G., Creemers, H. E., Vogelaar, S., & Asscher, J. J. (2025). What Works for Whom? The Influence of Problem Severity, Maladaptive Perfectionism, and Perceived Parental Pressure on the Effectiveness of a School-Based Performance Anxiety Program. Behavioral Sciences, 15(4), 436. https://doi.org/10.3390/bs15040436