

Intensity of Physical Activity in Young People: Focus on Emotional, Cognitive, and Healthy Lifestyle-Related Variables

 , , and
, , and 
Abstract

1. Introduction
2. Method
2.1. Participants
2.2. Procedure
- -
- d2 test [48]: In this test, participants must cross out any letter “d” with two marks around, above, or below in any order. There are also surrounding distractors that are similar to the target stimulus, e.g., a p with two marks or a d with one or three marks. The time limit per line of the test is 20 s.
- -
- Digit span test [49]: This is used to measure the working memory’s number storage capacity. Participants hear a sequence of numbers and are required to recall the sequence correctly, with increasingly longer sequences being tested in each trial. Digit span tasks are given forward or backward, meaning that once the sequence is presented, the participant is asked to recall the sequence in either normal or reverse order.
2.3. Statistical Analysis
3. Results
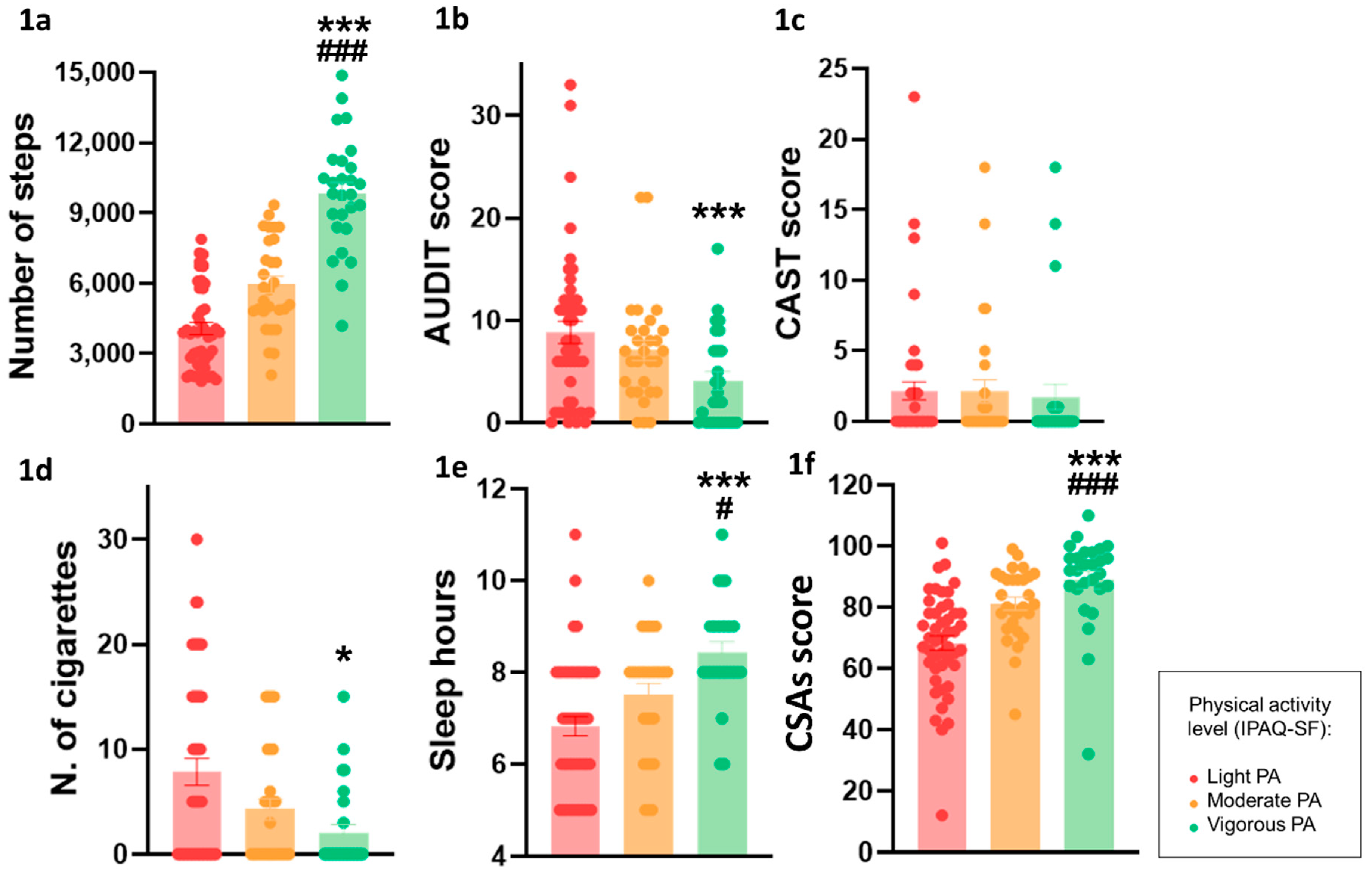
3.1. Health- and Lifestyle-Related Variables
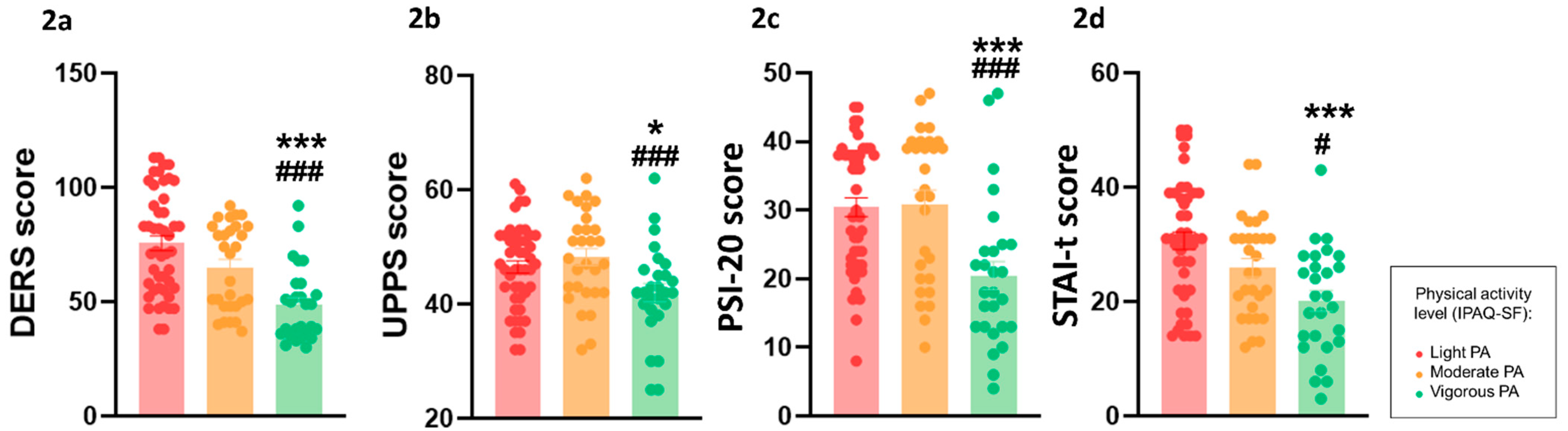
3.2. Psychological Variables
3.3. Cognitive Variables
3.4. Multiple Linear Regression
4. Discussion
4.1. A Higher Intensity of PA Was Related to Healthy Behaviors
4.2. Higher Intensity of PA Was Associated with Better Emotional and Impulse Control Skills
4.3. Prefrontal-Related Functions Were Not Affected by Different Intensities of PA
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arnett, J.J. Emerging adulthood. A theory of development from the late teens through the twenties. Am. Psychol. 2000, 55, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Bruffaerts, R.; Mortier, P.; Kiekens, G.; Auerbach, R.P.; Cuijpers, P.; Demyttenaere, K.; Green, J.G.; Nock, M.K.; Kessler, R.C. Mental health problems in college freshmen: Prevalence and academic functioning. J. Affect. Disord. 2018, 225, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Erickson, E.H. Identity Youth Crisis New York; W.W. Norton Company: New York, NY, USA, 1968. [Google Scholar]
- Limone, P.; Toto, G.A. Factors That Predispose Undergraduates to Mental Issues: A Cumulative Literature Review for Future Research Perspectives. Front. Public Health 2022, 10, 831349. [Google Scholar] [CrossRef] [PubMed]
- Pedrelli, P.; Nyer, M.; Yeung, A.; Zulauf, C.; Wilens, T. College Students: Mental Health Problems and Treatment Considerations. Acad. Psychiatry 2015, 39, 503–511. [Google Scholar] [CrossRef]
- Bewick, B.; Koutsopoulou, G.; Miles, J.; Slaa, E.; Barkham, M. Changes in undergraduate students’ psychological well-being as they progress through university. Stud. High. Educ. 2010, 35, 633–645. [Google Scholar] [CrossRef]
- Snedden, T.R.; Scerpella, J.; Kliethermes, S.A.; Norman, R.S.; Blyholder, L.; Sanfilippo, J.; McGuine, T.A.; Heiderscheit, B. Sport and physical activity level impacts health-related quality of life among collegiate students. Am. J. Health Promot. 2019, 33, 675–682. [Google Scholar] [CrossRef] [PubMed]
- Schlack, R.; Peerenboom, N.; Neuperdt, L.; Junker, S.; Beyer, A.K. The effects of mental health problems in childhood and adolescence in young adults: Results of the KiGGS cohort. J. Health Monit. 2021, 6, 3–19. [Google Scholar] [CrossRef]
- Leach, L.S.; Butterworth, P. Depression and anxiety in early adulthood: Consequences for finding a partner, and relationship support and conflict. Epidemiol. Psychiatr. Sci. 2020, 29, e141. [Google Scholar] [CrossRef]
- Daros, A.R.; Daniel, K.E.; Boukhechba, M.; Chow, P.I.; Barnes, L.E.; Teachman, B.A. Relationships between trait emotion dysregulation and emotional experiences in daily life: An experience sampling study. Cogn. Emot. 2020, 34, 743–755. [Google Scholar] [CrossRef]
- Zeman, J.; Cassano, M.; Perry-Parrish, C.; Stegall, S. Emotion regulation in children and adolescents. J. Dev. Behav. Pediatr. 2006, 27, 155–168. [Google Scholar] [CrossRef]
- Berg, J.M.; Latzman, R.D.; Bliwise, N.G.; Lilienfeld, S.O. Parsing the heterogeneity of impulsivity: A meta-analytic review of the behavioral implications of the UPPS for psychopathology. Psychol. Assess. 2015, 27, 1129–1146. [Google Scholar] [CrossRef] [PubMed]
- Bos, J.; Hayden, M.J.; Lum, J.A.G.; Staiger, P.K. UPPS-P impulsive personality traits and adolescent cigarette smoking: A meta-analysis. Drug Alcohol. Depend. 2019, 197, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Stautz, K.; Cooper, A. Impulsivity-related personality traits and adolescent alcohol use: A meta-analytic review. Clin. Psychol. Rev. 2013, 33, 574–592. [Google Scholar] [CrossRef]
- Arias-De la Torre, J.; Fernández-Villa, T.; Molina, A.J.; Amezcua-Prieto, C.; Mateos, R.; Cancela, J.M.; Delgado-Rodríguez, M.; Ortíz-Moncada, R.; Alguacil, J.; Almaraz, A.; et al. Drug use, family support and related factors in university students. A cross-sectional study based on the uniHcos Project data. Gac. Sanit. 2019, 33, 141–147. [Google Scholar] [CrossRef]
- Abrantes, L.C.S.; de Souza de Morais, N.; Gonçalves, V.S.S.; Ribeiro, S.A.V.; de Oliveira Sediyama, C.M.N.; do Carmo Castro Franceschini, S.; dos Santos Amorim, P.R.; Priore, S.E. Physical activity and quality of life among college students without comorbidities for cardiometabolic diseases: Systematic review and meta-analysis. Qual. Life Res. 2022, 31, 1933–1962. [Google Scholar] [CrossRef]
- Steptoe, A.; Wardle, J.; Cui, W.; Bellisle, F.; Zotti, A.M.; Baranyai, R.; Sanderman, R. Trends in smoking, diet, physical exercise, and attitudes toward health in European university students from 13 countries, 1990–2000. Prev. Med. 2002, 35, 97–104. [Google Scholar] [CrossRef]
- Patrick, M.E.; Schulenberg, J.E.; O’Malley, P.M.; Johnston, L.D.; Bachman, J.G. Adolescents’ reported reasons for alcohol and marijuana use as predictors of substance use and problems in adulthood. J. Stud. Alcohol Drugs 2011, 72, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The Physical Activity Guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef]
- Penedo, F.J.; Dahn, J.R. Exercise and well-being: A review of mental and physical health benefits associated with physical activity. Curr. Opin. Psychiatry 2005, 18, 189–193. [Google Scholar] [CrossRef]
- Li, J.; Huang, Z.; Si, W.; Shao, T. The Effects of Physical Activity on Positive Emotions in Children and Adolescents: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 14185. [Google Scholar] [CrossRef]
- Gmmash, A.; Alonazi, A.; Almaddah, M.; Alkhateeb, A.; Sabir, O.; Alqabbani, S. Influence of an 8-week exercise program on physical, emotional, and mental health in saudi adolescents: A pilot study. Medicina 2023, 59, 883. [Google Scholar] [CrossRef] [PubMed]
- Clemente, F.M.; Nikolaidis, P.T.; Martins, F.M.; Mendes, R.S. Physical activity patterns in university students: Do they follow the public health guidelines? PLoS ONE 2016, 11, e0152516. [Google Scholar] [CrossRef] [PubMed]
- Dishman, R.K.; McIver, K.L.; Dowda, M.; Pate, R.R. Declining physical activity and motivation from middle school to high school. Med. Sci. Sports Exerc. 2018, 50, 1206–1215. [Google Scholar] [CrossRef] [PubMed]
- Martens, M.P.; Buscemi, J.; Smith, A.E.; Murphy, J.G. The short-term efficacy of a brief motivational intervention designed to increase physical activity among college students. J. Phys. Act. Health 2012, 9, 525–532. [Google Scholar] [CrossRef]
- Bernstein, E.E.; McNally, R.J. Acute aerobic exercise helps overcome emotion regulation deficits. Cogn. Emot. 2017, 31, 834–843. [Google Scholar] [CrossRef]
- Giles, G.E.; Cantelon, J.A.; Eddy, M.D.; Brunyé, T.T.; Urry, H.L.; Mahoney, C.R.; Kanarek, R.B. Habitual exercise is associated with cognitive control and cognitive reappraisal success. Exp. Brain Res. 2017, 235, 3785–3797. [Google Scholar] [CrossRef]
- Belcher, B.R.; Zink, J.; Azad, A.; Campbell, C.E.; Chakravartti, S.P.; Herting, M.M. The roles of physical activity, exercise, and fitness in promoting resilience during adolescence: Effects on mental well-being and brain development. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2021, 6, 225–237. [Google Scholar] [CrossRef]
- Alves, A.R.; Dias, R.; Neiva, H.P.; Marinho, D.A.; Marques, M.C.; Sousa, A.C.; Loureiro, V.; Loureiro, N. High-Intensity Interval Training upon Cognitive and Psychological Outcomes in Youth: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 5344. [Google Scholar] [CrossRef]
- Soler, C.T.; Kanders, S.H.; Olofsdotter, S.; Vadlin, S.; Åslund, C.; Nilsson, K.W. Exploration of the Moderating Effects of Physical Activity and Early Life Stress on the Relation between Brain-Derived Neurotrophic Factor (BDNF) rs6265 Variants and Depressive Symptoms among Adolescents. Genes 2022, 13, 1236. [Google Scholar] [CrossRef]
- Ruotsalainen, I.; Gorbach, T.; Perkola, J.; Renvall, V.; Syväoja, H.J.; Tammelin, T.H.; Karvanen, J.; Parviainen, T. Physical activity, aerobic fitness, and brain white matter: Their role for executive functions in adolescence. Dev. Cogn. Neurosci. 2020, 42, 100765. [Google Scholar] [CrossRef]
- Talbot, J.S.; Perkins, D.R.; Tallon, C.M.; Dawkins, T.G.; Douglas, A.J.M.; Beckerleg, R.; Crofts, A.; Wright, M.E.; Davies, S.; Steventon, J.J.; et al. Cerebral blood flow and cerebrovascular reactivity are modified by maturational stage and exercise training status during youth. Exp. Physiol. 2023, 108, 1500–1515. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Muro Franco, A.; Beamonte San Agustín, A.; Marqueta, A.; Gargallo Valero, P.; Nerín de la Puerta, I. Addictive substance use among first-year university students. Adicciones 2009, 21, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Molina, A.J.; Varela, V.; Fernández, T.; Martín, V.; Ayán, C.; Cancela, J.M. Unhealthy habits and practice of physical activity in Spanish college students: The role of gender, academic profile and living situation. Adicciones 2012, 24, 319–327. [Google Scholar] [CrossRef]
- Vázquez, F.L.; Torres, Á.; Otero, P.; Díaz, O. Prevalence, comorbidity, and correlates of DSM-IV axis I mental disorders among female university students. J. Nerv. Ment. Dis. 2011, 199, 379–383. [Google Scholar] [CrossRef] [PubMed]
- Ballester, L.; Alayo, I.; Vilagut, G.; Almenara, J.; Cebrià, A.I.; Echeburúa, E.; Gabilondo, A.; Gili, M.; Lagares, C.; Piqueras, J.A.; et al. Mental disorders in Spanish university students: Prevalence, age-of-onset, severe role impairment and mental health treatment. J. Affect. Disord. 2020, 273, 604–613. [Google Scholar] [CrossRef]
- Sicilia, Á.; Alías-García, A.; Ferriz, R.; Moreno-Murcia, J.A. Spanish adaptation and validation of the Exercise Addiction Inventory (EAI). Psicothema 2013, 25, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Contel Guillamon, M.; Gual Solé, A.; Colom Farran, J. Test para la identificación de trastornos por uso de alcohol (AUDIT): Traducción y validación del AUDIT al catalán y castellano. Adicciones 1999, 11, 337–347. [Google Scholar] [CrossRef]
- Legleye, S.; Karila, L.; Beck, F.; Reynaud, M. Validation of the CAST, a general population Cannabis Abuse Screening Test. J. Subst. Use 2007, 12, 233–242. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Gorsuchm, R.L.; Lushene, R.E. Manual for the State-Trait Anxiety Inventory; Consulting Psychologist Press: Palo Alto, CA, USA, 1970. [Google Scholar]
- Hervas, G.; Jódar, R. Adaptación al castellano de la escala de dificultades en regulación emocional. Clínica Y Salud 2008, 19, 139–156. [Google Scholar]
- Cándido, A.; Orduña, E.; Perales, J.C.; Verdejo-García, A.; Billeux, J. Validation of a short Spanish version of the UPPS-P impulsive behaviour scale. Trastor. Adict. 2012, 14, 73–78. [Google Scholar] [CrossRef]
- Pedrero-Perez, E.J.; Ruiz-Sanchez de Leon, J.M.; Rojo-Mota, G.; Morales-Alonso, S.; Pedrero-Aguilar, J.; Lorenzo, I.; Gonzalez, A. Prefrontal Symptoms Inventory (PSI): Ecological validity and convergence with neuropsychological measures. Rev. De Neurol. 2016, 63, 241–251. [Google Scholar]
- Martínez-Molina, A.; Arias, V.B. Balanced and positively worded personality short-forms: Mini-IPIP validity and cross-cultural invariance. PeerJ 2018, 6, e5542. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R., Jr.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. Compendium of Physical Activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [PubMed]
- León-Estrada, I.; García-García, J.; Roldán-Tapia, L. Escala de reserva cognitiva: Ajuste del modelo teórico y baremación. Rev. De Neurol. 2017, 64, 7–16. [Google Scholar] [CrossRef]
- Brickenkamp, R.; Cubero, N.S. D2: Test de Atención; TEA Ediciones: Madrid, Spain, 2002. [Google Scholar]
- Wechsler, D. WMS-III Escala de memoria de Wechsler-III; TEA: Madrid, Spain, 2004. [Google Scholar]
- Lardier, D.T.; Coakley, K.E.; Holladay, K.R.; Amorim, F.T.; Zuhl, M.N. Exercise as a useful intervention to reduce alcohol consumption and improve physical fitness in individuals with alcohol use disorder: A systematic review and meta-analysis. Front. Psychol. 2021, 12, 675285. [Google Scholar] [CrossRef]
- Leasure, J.L.; Neighbors, C.; Henderson, C.E.; Young, C.M. Exercise and alcohol consumption: What we know, what we need to know, and why it is important. Front. Psychiatry 2015, 6, 156. [Google Scholar] [CrossRef]
- Buscemi, J.; Martens, M.P.; Murphy, J.G.; Yurasek, A.M.; Smith, A.E. Moderators of the relationship between physical activity and alcohol consumption in college students. J. Am. Coll. Health 2011, 59, 503–509. [Google Scholar] [CrossRef]
- Allen, M.S.; Vella, S.A.; Laborde, S. Health-related behaviour and personality trait development in adulthood. J. Res. Personal. 2015, 59, 104–110. [Google Scholar] [CrossRef]
- Boland, J.K.; Henderson, C.E. The impact of personality on the physical activity and alcohol use relationship. Clin. Psychol. Spec. Educ. 2020, 9, 62–75. [Google Scholar] [CrossRef]
- Sanz-Martín, D.; Zurita-Ortega, F.; Melguizo-Ibáñez, E.; Alonso-Vargas, J.M.; Caracuel-Cáliz, R.; Ubago-Jiménez, J.L. Physical Activity Time, Alcohol Consumption, Mediterranean Diet, and Anxiety in Education Science Students. Eur. J. Investig. Health Psychol. Educ. 2024, 14, 87–102. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Boros, S. The effect of physical activity on sleep quality: A systematic review. Eur. J. Physiother. 2021, 23, 11–18. [Google Scholar] [CrossRef]
- Curcio, G.; Ferrara, M.; De Gennaro, L. Sleep loss, learning capacity and academic performance. Sleep Med. Rev. 2006, 10, 323–337. [Google Scholar] [CrossRef] [PubMed]
- Lang, C.; Brand, S.; Feldmeth, A.K.; Holsboer-Trachsler, E.; Pühse, U.; Gerber, M. Increased self-reported and objectively assessed physical activity predict sleep quality among adolescents. Physiol. Behav. 2013, 120, 46–53. [Google Scholar] [CrossRef]
- Eime, R.M.; Young, J.A.; Harvey, J.T.; Charity, M.J.; Payne, W.R. A systematic review of the psychological and social benefits of participation in sport for children and adolescents: Informing development of a conceptual model of health through sport. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 98. [Google Scholar] [CrossRef]
- Timonen, J.; Niemelä, M.; Hakko, H.; Alakokkare, A.; Räsänen, S. Associations between adolescents’ social leisure activities and the onset of mental disorders in young adulthood. J. Youth Adolesc. 2021, 50, 1757–1765. [Google Scholar] [CrossRef]
- Perchtold-Stefan, C.M.; Fink, A.; Rominger, C.; Weiss, E.M.; Papousek, I. More habitual physical activity is linked to the use of specific, more adaptive cognitive reappraisal strategies in dealing with stressful events. Stress Health 2020, 36, 274–286. [Google Scholar] [CrossRef] [PubMed]
- Kalisch, R.; Müller, M.B.; Tüscher, O. A conceptual framework for the neurobiological study of resilience. Behav. Brain Sci. 2015, 38, e92. [Google Scholar] [CrossRef]
- Gerber, M.; Pühse, U. Review article: Do exercise and fitness protect against stress-induced health complaints? A review of the literature. Scand. J. Public Health 2009, 37, 801–819. [Google Scholar] [CrossRef]
- Ekelund, U.; Sanchez-Lastra, M.A.; Dalene, K.E.; Tarp, J. Dose-response associations, physical activity intensity and mortality risk: A narrative review. J. Sport Health Sci. 2024, 13, 24–29. [Google Scholar] [CrossRef]
- Williams, R.A.; Hatch, L.; Cooper, S.B. A review of factors affecting the acute exercise-cognition relationship in children and adolescents. OBM Integr. Complement. Med. 2019, 4, 24. [Google Scholar] [CrossRef]
- Browne, R.A.; Costa, E.C.; Sales, M.M.; Fonteles, A.I.; Moraes, J.F.; Barros, J. Acute effect of vigorous aerobic exercise on the inhibitory control in adolescents. Rev. Paul. De Pediatr. 2016, 34, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Soga, K.; Shishido, T.; Nagatomi, R. Executive function during and after acute moderate aerobic exercise in adolescents. Psychol. Sport Exerc. 2015, 16, 7–17. [Google Scholar] [CrossRef]
- Hötting, K.; Röder, B. Beneficial effects of physical exercise on neuroplasticity and cognition. Neurosci. Biobehav. Rev. 2013, 37, 2243–2257. [Google Scholar] [CrossRef] [PubMed]
- Müller, P.; Duderstadt, Y.; Lessmann, V.; Müller, N.G. Lactate and BDNF: Key Mediators of Exercise Induced Neuroplasticity? J. Clin. Med. 2020, 9, 1136. [Google Scholar] [CrossRef]
- Jacob, N.; So, I.; Sharma, B.; Marzolini, S.; Tartaglia, M.C.; Oh, P.; Green, R. Effects of High-Intensity Interval Training Protocols on Blood Lactate Levels and Cognition in Healthy Adults: Systematic Review and Meta-Regression. Sports Med. 2023, 53, 977–991. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Light PA (n = 47) | Moderate PA (n = 29) | Vigorous PA (n = 27) | p | |
|---|---|---|---|---|
| Age | 20.19 ± 0.41 | 19.55 ± 0.33 | 19.59 ± 0.52 | 0.47 |
| AUDIT | 8.83 ± 1.08 | 7.07 ± 0.98 | 4.07 ± 0.89 | 0.008 ** |
| Age at onset for alcohol use | 15.23 ± 0.27 | 15.41 ± 0.37 | 16.04 ± 0.30 | 0.18 |
| CAST | 2.17 ± 0.65 | 2.14 ± 0.83 | 1.74 ± 0.90 | 0.92 |
| Cannabis use (YES %) | 23.4% | 20.7% | 11.1% | |
| Nicotine (YES %) | 55.3% | 48.3% | 25.9% | |
| Cigarettes/day | 7.83 ± 1.29 | 4.28 ± 1.02 | 2.04 ± 0.77 | <0.001 * |
| Sleep hours | 6.83 ± 0.21 | 7.52 ± 0.25 | 8.44 ± 0.22 | <0.001 ***# |
| Sleep difficulties | 51.1% | 41.4% | 11.1% | |
| IPAQ-SF | 436.58 ± 48.47 | 2062.69 ± 75.31 | 3994.04 ± 172.29 | <0.001 ***### |
| EAI | 6.12 ± 0.45 | 7.87 ± 0.98 | 7.02 ± 1.03 | 0.69 |
| Type of PA (individual %) | 100% | 100% | 74.1% | |
| Steps/week | 4075.06 ± 253.31 | 5938.72 ± 361.67 | 9832.81 ± 461.56 | <0.001 ***### |
| Sitting hours/day | ||||
| 6–8 h | 29.8% | 62.1% | 22.2% | |
| 8–10 h | 59.6% | 37.9% | 70.4% | |
| >10 h | 10.6% | - | 7.4% | |
| CSAs | 68.38 ± 2.38 | 81.21 ± 2.17 | 88.96 ± 2.88 | <0.001 ***### |
| STAI trait | 30.66 ± 1.53 | 25.93 ± 1.61 | 20.15 ± 1.81 | <0.001 ***# |
| DERS | 75.66 ± 3.27 | 65.07 ± 3.47 | 48.70 ± 3.12 | <0.001 ***### |
| Emotional neglect | 12.70 ± 0.59 | 10.69 ± 0.58 | 9.93 ± 0.62 | 0.004 ***### |
| Emotional confusion | 7.57 ± 0.49 | 6.79 ± 0.36 | 4.67 ± 0.31 | <0.001 ***### |
| Emotional interference | 13.81 ± 0.54 | 12.03 ± 0.65 | 8.56 ± 0.61 | <0.001 ***### |
| Emotional dysregulation | 22.77 ± 1.32 | 18.79 ± 1.33 | 12.52 ± 0.90 | <0.001 ***### |
| Emotional rejection | 18.81 ± 1.06 | 16.76 ± 1.57 | 13.04 ± 1.43 | 0.007 ** |
| UPPS-P | 46.51 ± 1.06 | 48.24 ± 1.48 | 42.04 ± 1.59 | 0.01 *### |
| Negative urgency | 9.64 ± 0.40 | 9.90 ± 0.42 | 8.04 ± 0.54 | 0.03 * |
| Lack of perseverance | 8.49 ± 0.32 | 8.07 ± 0.51 | 6.52 ± 0.45 | 0.003 ** |
| Lack of premeditation | 7.72 ± 0.28 | 7.90 ± 0.40 | 7.33 ± 0.39 | 0.56 |
| Sensation seeking | 10.62 ± 0.44 | 11.86 ± 0.50 | 10.85 ± 0.65 | 0.21 |
| Positive urgency | 10.04 ± 0.45 | 10.52 ± 0.51 | 9.30 ± 0.62 | 0.32 |
| PSI-20 | 30.43 ± 1.37 | 30.90 ± 2.03 | 20.48 ± 2.06 | <0.001 ***### |
| Emotional behavior | 6.32 ± 0.60 | 7.31 ± 0.71 | 4.81 ± 0.61 | 0.06 |
| Social behavior | 3.74 ± 0.47 | 5.24 ± 0.56 | 2.89 ± 0.62 | 0.02 * |
| Behavioral control | 20.36 ± 0.92 | 18.34 ± 1.38 | 12.78 ± 1.35 | <0.001 ***### |
| Mini-IPIP | 65.43 ± 1.06 | 65.76 ± 1.01 | 67.26 ± 1.14 | 0.49 |
| Openness | 10.87 ± 0.23 | 11.17 ± 0.33 | 11.63 ± 0.41 | 0.23 |
| Conscientiousness | 13.85 ± 0.36 | 12.62 ± 0.53 | 12.37 ± 0.55 | 0.11 |
| Extraversion | 13.34 ± 0.52 | 14.83 ± 0.55 | 16.22 ± 0.49 | 0.08 |
| Agreeableness | 15.34 ± 0.38 | 14.62 ± 0.55 | 15.52 ± 0.44 | 0.39 |
| Neuroticism | 12.02 ± 0.42 | 12.52 ± 0.43 | 11.19 ± 0.41 | 0.15 |
| COGNITIVE VARIABLES | ||||
| d2–correct | 158.62 ± 6.68 | 158.14 ± 7.65 | 178.59 ± 6.01 | 0.09 |
| d2–omissions | 21.87 ± 3.07 | 21.03 ± 4.10 | 13.41 ± 2.73 | 0.19 |
| d2–commissions | 2.66 ± 0.70 | 4.17 ± 1.17 | 1.30 ± 0.58 | 0.10 |
| d2–TOT | 414.13 ± 12.61 | 407.86 ± 15.14 | 436.52 ± 11.96 | 0.36 |
| d2–VAR | 12.13 ± 0.61 | 12.10 ± 1.10 | 11.41 ± 0.78 | 0.80 |
| d2–CON | 155.98 ± 7.07 | 153.93 ± 8.37 | 176.59 ± 6.41 | 0.09 |
| Forward digits | 9.36 ± 0.38 | 9.69 ± 0.42 | 10.22 ± 0.36 | 0.32 |
| Backward digits | 7.19 ± 0.39 | 7.38 ± 0.43 | 7.56 ± 0.39 | 0.82 |
| Total digits | 16.47 ± 0.74 | 17.21 ± 0.82 | 17.78 ± 0.70 | 0.48 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elliott, A.S.; Moreno-Fernández, R.D.; Cordellat-Marzal, A.; Sampedro-Piquero, P. Intensity of Physical Activity in Young People: Focus on Emotional, Cognitive, and Healthy Lifestyle-Related Variables. Behav. Sci. 2024, 14, 935. https://doi.org/10.3390/bs14100935
Elliott AS, Moreno-Fernández RD, Cordellat-Marzal A, Sampedro-Piquero P. Intensity of Physical Activity in Young People: Focus on Emotional, Cognitive, and Healthy Lifestyle-Related Variables. Behavioral Sciences. 2024; 14(10):935. https://doi.org/10.3390/bs14100935
Chicago/Turabian StyleElliott, Adrián S., Román D. Moreno-Fernández, Ana Cordellat-Marzal, and Patricia Sampedro-Piquero. 2024. "Intensity of Physical Activity in Young People: Focus on Emotional, Cognitive, and Healthy Lifestyle-Related Variables" Behavioral Sciences 14, no. 10: 935. https://doi.org/10.3390/bs14100935
APA StyleElliott, A. S., Moreno-Fernández, R. D., Cordellat-Marzal, A., & Sampedro-Piquero, P. (2024). Intensity of Physical Activity in Young People: Focus on Emotional, Cognitive, and Healthy Lifestyle-Related Variables. Behavioral Sciences, 14(10), 935. https://doi.org/10.3390/bs14100935