
Physical Activity and Depression in Adolescents: Evidence from China Family Panel Studies


Abstract
:1. Introduction
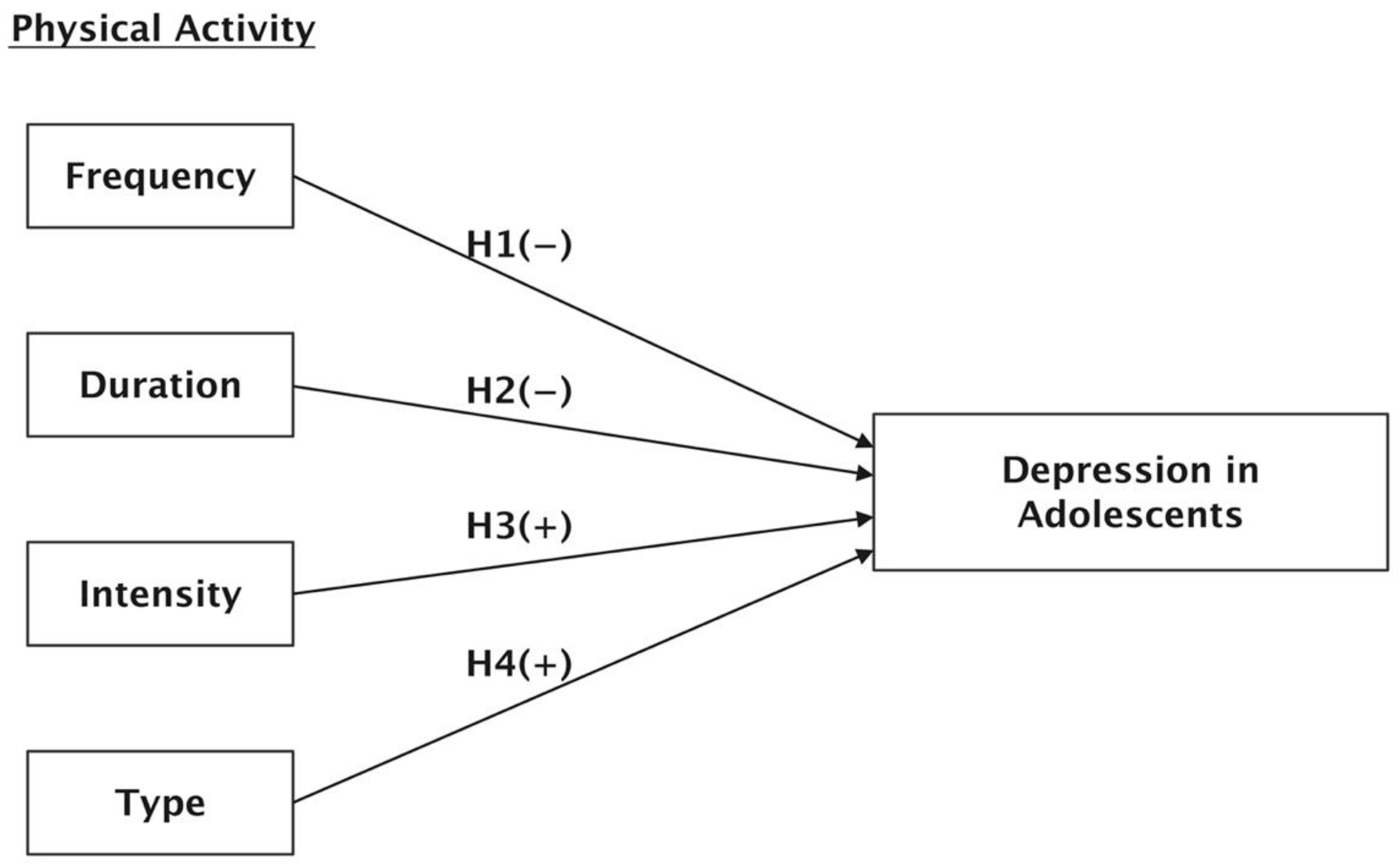
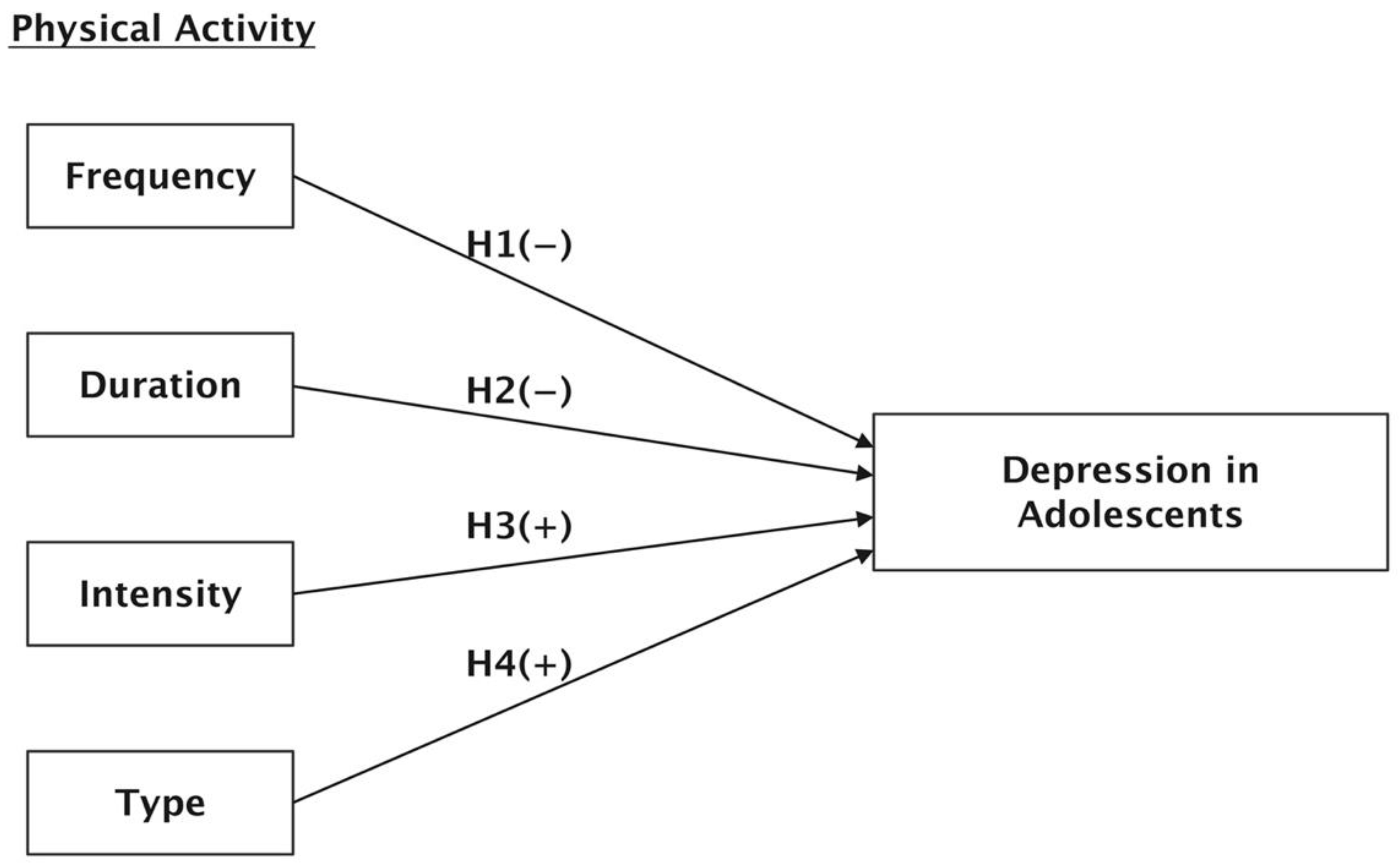
2. Literature Review and Hypothesis Development
3. Methods
3.1. Sample
3.2. Measures
3.2.1. Dependent Variables of Depression
3.2.2. Physical Activity
3.2.3. Control Variables
3.3. Statistical Modeling
4. Results
5. Discussion
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Diener, M.J.; Gottdiener, W.H.; Keefe, J.R.; Levy, K.N.; Midgley, N. Treatment of depression in children and adolescents. Lancet Psychiatry 2021, 8, 97. [Google Scholar] [CrossRef]
- Kroning, M.; Kroning, K. Teen Depression and Suicide: A Silent Crisis. J. Christ. Nurs. 2016, 33, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Villafaina, S.; Tapia-Serrano, M.Á.; Vaquero-Solís, M.; León-Llamas, J.L.; Sánchez-Miguel, P.A. The Role of Physical Activity in the Relationship between Satisfaction with Life and Health-Related Quality of Life in School-Age Adolescents. Behav. Sci. 2021, 11, 121. [Google Scholar] [CrossRef] [PubMed]
- Rose, L.T.; Soundy, A. The Positive Impact and Associated Mechanisms of Physical Activity on Mental Health in Underprivileged Children and Adolescents: An Integrative Review. Behav. Sci. 2020, 10, 171. [Google Scholar] [CrossRef]
- Graf, C.; Beneke, R.; Bloch, W.; Bucksch, J.; Dordel, S.; Eiser, S.; Ferrari, N.; Koch, B.; Krug, S.; Lawrenz, W.; et al. Recommendations for promoting physical activity for children and adolescents in Germany. A consensus statement. Obes. Facts 2014, 7, 178–190. [Google Scholar] [CrossRef] [Green Version]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef]
- Li, M.; Dibley, M.J.; Sibbritt, D.; Yan, H. Factors Associated with Adolescents’ Physical Inactivity in Xi’an City, China. Med. Sci. Sports Exerc. 2007, 38, 2075–2085. [Google Scholar] [CrossRef]
- Fu, X.; Zhang, K.; Chen, X. Report on the Development of Chinese National Mental Health (2019–2020); Social Science Literature Press: Beijing, China, 2020. [Google Scholar]
- Alghadir, A.H.; Gabr, S.A.; Iqbal, Z.A. Effect of Gender, Physical Activity and Stress-Related Hormones on Adolescent’s Academic Achievements. Int. J. Environ. Res. Public Health 2020, 17, 4143. [Google Scholar] [CrossRef]
- Murri, M.B.; Ekkekakis, P.; Menchetti, M.; Neviani, F.; Trevisani, F.; Tedeschi, S.; Latessa, P.M.; Nerozzi, E.; Ermini, G.; Zocchi, D.; et al. Physical exercise for late-life depression: Effects on symptom dimensions and time course. J. Affect. Disord. 2018, 230, 65–70. [Google Scholar] [CrossRef]
- Mayer, J.S.; Hees, K.; Medda, J.; Grimm, O.; Asherson, P.; Bellina, M.; Colla, M.; Ibáñez, P.; Koch, E.; Martinez-Nicolas, A. Bright light therapy versus physical exercise to prevent co-morbid depression and obesity in adolescents and young adults with attention-deficit/hyperactivity disorder: Study protocol for a randomized controlled trial. Trials 2018, 19, 140. [Google Scholar] [CrossRef] [PubMed]
- Rimer, J.; Dwan, K.; Lawlor, D.A.; Greig, C.A.; McMurdo, M.; Morley, W.; Mead, G.E. Exercise for depression. Cochrane Database Syst. Rev. 2013, 9, CD004366. [Google Scholar]
- Krogh, J.; Saltin, B.; Gluud, C.; Nordentoft, M. The DEMO trial: A randomized, parallel-group, observer-blinded clinical trial of strength versus aerobic versus relaxation training for patients with mild to moderate depression. J. Clin. Psychiatry 2009, 70, 790–800. [Google Scholar] [CrossRef] [PubMed]
- Chalder, M.; Wiles, N.; Campbell, J.; Hollinghurst, S.; Searle, A.; Haase, A.; Taylor, A.; Fox, K.; Baxter, H.; Davis, M.; et al. A pragmatic randomised controlled trial to evaluate the cost-effectiveness of a physical activity intervention as a treatment for depression: The treating depression with physical activity (TREAD) trial. Health Technol. Assess. 2012, 16, 1–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reichert, M.; Braun, U.; Gan, G.; Reinhard, I.; Giurgiu, M.; Ma, R.; Zang, Z.; Hennig, O.; Koch, E.D.; Wieland, L.; et al. A neural mechanism for affective well-being: Subgenual cingulate cortex mediates real-life effects of nonexercise activity on energy. Sci. Adv. 2020, 6, eaaz8934. [Google Scholar] [CrossRef]
- Mahmood, H.; Waqar, A.; Rana, S.; Yaqoob, M.; Qureshi, E. Physical Exercise Activity, Cognitive Functions and Its Relationship to Quality of Life in the Senior Citizens of Lahore. Am. J. Biomed. Life Sci. 2021, 8, 143–155. [Google Scholar] [CrossRef]
- Jung, W.S.; Park, H.Y.; Kim, S.W.; Kim, J.; Lim, K. Prediction of non-exercise activity thermogenesis (NEAT) using multiple linear regression in healthy Korean adults: A preliminary study. Phys. Act. Nutr. 2021, 25, 23–29. [Google Scholar] [CrossRef]
- Nabkasorn, C.; Miyai, N.; Sootmongkol, A.; Junprasert, S.; Yamamoto, H.; Arita, M.; Miyashita, K. Effects of physical exercise on depression, neuroendocrine stress hormones and physiological fitness in adolescent females with depressive symptoms. Eur. J. Public Health 2006, 16, 179–184. [Google Scholar] [CrossRef]
- Motta, R.W.; McWilliams, M.E.; Schwartz, J.T.; Cavera, S.R. The Role of Exercise in Reducing Childhood and Adolescent PTSD, Anxiety, and Depression. J. Appl. Sch. Psychol. 2012, 28, 224–238. [Google Scholar] [CrossRef]
- Stella, S.G.; Vilar, A.P.; Lacroix, C.; Isberg, F.M.; Santos, R.F.; Mello, M.T.; Tufik, S. Effects of type of physical exercise and leisure activities on the depression scores of obese Brazilian adolescent girls. Braz. J. Med. Biol. Res. 2005, 38, 1683–1689. [Google Scholar] [CrossRef] [Green Version]
- Ivarsson, T.; Spetz, A.C.; Hammar, M. Physical exercise and vasomotor symptoms in postmenopausal women. Maturitas 1998, 29, 139–146. [Google Scholar] [CrossRef]
- Jóźków, P.; Mędraś, M. Psychological stress and the function of male gonads. Endokrynol. Pol. 2012, 63, 44–49. [Google Scholar] [PubMed]
- Wright, A.; Cattan, M. Physical activity and the management of depression. Work. Older People 2009, 13, 15–18. [Google Scholar] [CrossRef]
- Hedlund, E.R.; Ljungberg, H.; Söderström, L.; Lundell, B.; Sjöberg, G. Physical exercise may improve sleep quality in children and adolescents with Fontan circulation. Cardiol. Young 2019, 29, 922–929. [Google Scholar] [CrossRef] [PubMed]
- Vigil, P.; Orellana, R.F.; Cortés, M.; Molina, C.T.; Switzer, B.E.; Klaus, H. Endocrine Modulation of the Adolescent Brain: A Review. J. Pediatr. Adolesc. Gynecol. 2011, 24, 330–337. [Google Scholar] [CrossRef]
- Farooqui, A.A. Effect of Exercise on Neurodegeneration in Neurological Disorders. In Inflammation and Oxidative Stress in Neurological Disorders: Effect of Lifestyle, Genes, and Age; Farooqui, A.A., Ed.; Springer: Cham, Switzerland, 2014; pp. 143–173. [Google Scholar]
- Schuch, F.B.; Vancampfort, D.; Richards, J.; Rosenbaum, S.; Ward, P.B.; Stubbs, B. Exercise as a treatment for depression: A meta-analysis adjusting for publication bias. J. Psychiatr. Res. 2016, 77, 42–51. [Google Scholar] [CrossRef] [Green Version]
- Gergelyfi, M.; Sanz-Arigit, E.J.; Solopchuk, O.; Dricot, L.; Jacob, B.; Zénon, A. Mental fatigue correlates with depression of task-related network and augmented DMN activity but spares the reward circuit. NeuroImage 2021, 243, 118532. [Google Scholar] [CrossRef]
- Paluska, S.A.; Schwenk, T.L. Physical Activity and Mental Health: Current Concepts. Sports Med. 2000, 29, 167–180. [Google Scholar] [CrossRef]
- Sim, M.; Peeling, P.; Dawson, B.; Trinder, D. Exercise-Induced Anemia. In Encyclopedia of Exercise Medicine in Health and Disease; Mooren, F.C., Ed.; Springer: Berlin/Heidelberg, Germany, 2012; p. 28. [Google Scholar]
- Kamada, M.; Kitayuguchi, J.; Lee, I.M.; Hamano, T.; Imamura, F.; Inoue, S.; Miyachi, M.; Shiwaku, K. Relationship Between Physical Activity and Chronic Musculoskeletal Pain Among Community-dwelling Japanese Adults. J. Epidemiol. 2014, 24, 474–483. [Google Scholar] [CrossRef] [Green Version]
- Colley, R.C.; Janssen, I.; Tremblay, M.S. Daily step target to measure adherence to physical activity guidelines in children. Med. Sci. Sports Exerc. 2012, 44, 977–982. [Google Scholar] [CrossRef]
- Tudor-Locke, C.; Craig, C.L.; Beets, M.W.; Belton, S.; Cardon, G.M.; Duncan, S.; Hatano, Y.; Lubans, D.R.; Olds, T.S.; Raustorp, A.; et al. How many steps/day are enough? for children and adolescents. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 78. [Google Scholar] [CrossRef] [Green Version]
- Schuch, F.B.; Fleck, M.P. Is exercise an efficacious treatment for depression? A comment upon recent negative findings. Front. Psychiatry 2013, 4, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGuigan, K.; McGuigan, C.J. Moderate-to-vigorous exercise is beneficial and can improve symptoms of fatigue and depression in young people with paediatric-onset multiple sclerosis and other demyelinating conditions. Evid. Based Nurs. 2019, 209, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Lawlor, D.A.; Taylor, M.; Bedford, C.; Ebrahim, S. Is housework good for health? Levels of physical activity and factors associated with activity in elderly women. Results from the British Women’s Heart and Health Study. J. Epidemiol. Community Health 2002, 56, 473–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoshino, A.; Amano, S.; Suzuki, K.; Suwa, M. Relationships Between Depression and Stress Factors in Housework and Paid Work Among Japanese Women. Hong Kong J. Occup. Ther. 2016, 27, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.-S. Housework and Subjective Well-Being for Adolescents in Middle-Class Dual-Earner Families. Korean Popul. Stud. 2013, 3, 75–99. [Google Scholar]
- Lam, C.B.; Greene, K.M.; Mchale, S.M. Housework time from middle childhood through adolescence: Links to parental work hours and youth adjustment. Dev. Psychol. 2016, 52, 2071–2084. [Google Scholar] [CrossRef]
- Bianchi, S.M.; Sayer, L.C.; Milkie, M.A.; Robinson, J.P. Housework: Who Did, Does or Will Do It, and How Much Does It Matter? Soc. Forces 2012, 91, 55–63. [Google Scholar] [CrossRef] [Green Version]
- Gu, J.; Ming, X. Perceived Social Discrimination, Socioeconomic Status, and Alcohol Consumption among Chinese Adults: A Nationally Representative Study. Int. J. Environ. Res. Public Health 2020, 17, 6043. [Google Scholar] [CrossRef]
- Gu, J.; Zhu, R. Social Capital and Self-Rated Health: Empirical Evidence from China. Int. J. Environ. Res. Public Health 2020, 17, 9108. [Google Scholar] [CrossRef]
- Gu, J.; Ming, X. The Effects of Life Stress on Men’s Alcohol Use: A Reassessment of Data from the 2012 China Family Panel Studies. Int. J. Ment. Health Addict. 2021, 1–12. [Google Scholar] [CrossRef]
- Gu, J.; Ming, X. Daily Social Pressure and Alcohol Consumption Among Chinese Women: A Cross-Sectional Study. Asia Pac. J. Public Health 2021, 33, 396–403. [Google Scholar] [CrossRef]
- Xiang, Z.; Xiaoning, S. Family depression profiles among adolescents and their parents: A group-based multitrajectory modeling. J. Fam. Psychol. 2021, 35, 886–896. [Google Scholar]
- Paunesku, D.; Ellis, J.; Fogel, J.; Kuwabara, S.A.; Gollan, J.; Gladstone, T.; Reinecke, M.; Voorhees, B.W.V. Clusters of Behaviors and Beliefs Predicting Adolescent Depression: Implications for Prevention. J. Cogn. Behav. Psychother. 2008, 8, 147–168. [Google Scholar]
- Gijzen, M.W.M.; Rasing, S.P.A.; Creemers, D.H.M.; Smita, F.; Engels, R.C.M.E.; Beurs, D.D. Suicide ideation as a symptom of adolescent depression. A network analysis. J. Affect. Disord. 2020, 278, 68–77. [Google Scholar] [CrossRef]
- Rao, U.; Daley, S.E.; Hammen, C. Relationship Between Depression and Substance Use Disorders in Adolescent Women During the Transition to Adulthood. J. Am. Acad. Child Adolesc. Psychiatry 2000, 3, 215–222. [Google Scholar] [CrossRef]
- Chopra, R.; Sangwan, S. Differences in Depression Level among Rural and Urban Adolescents of Haryana, India. Int. J. Curr. Microbiol. Appl. Sci. 2020, 9, 3391–3398. [Google Scholar] [CrossRef]
- Ajaero, C.K.; Nzeadibe, C.T.; Igboeli, E.E. Rural-urban differences in the prevalence and predictors of depression among adolescents in South Africa. S. Afr. J. Child Health 2018, 12, s71–s74. [Google Scholar] [CrossRef] [Green Version]
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- Song, M.; Carroll, D.D.; Fulton, J.E. Meeting the 2008 Physical Activity Guidelines for Americans Among U.S. Youth. Am. J. Prev. Med. 2013, 44, 216–222. [Google Scholar] [CrossRef]
- Huaxia. China Reiterates Implementation of “Double Reduction” Policy. Xinhua, Beijing, 7 January 2021. [Google Scholar]
- Goh, E. China’s One-Child Policy and Multiple Caregiving: Raising Little Suns in Xiamen; Routledge: London, UK, 2011. [Google Scholar]

{kind=link}
| Number of Participants (n = 11,547) | Drinking | ||||
|---|---|---|---|---|---|
| Classification | N (%) | Yes N (%) | No N (%) | ||
| Exercise intensity | Non-intense | 119 (13.28) | 50 (16.56) | 69 (11.62) | 9.473 *** (0.009) |
| A little intense | 460 (51.34) | 164 (54.3) | 296 (49.83) | ||
| Intense | 317 (35.38) | 88 (29.14) | 229 (38.55) | ||
| Gender | Female | 385 (42.97) | 131 (43.38) | 254 (42.97) | 0.031 (0.86) |
| Male | 511 (57.03) | 171 (56.62) | 340 (57.24) | ||
| Health status | Average or unhealthy | 21 (2.34) | 1 (0.33) | 20 (3.37) | 29.147 *** (0.000) |
| Relatively healthy | 272 (30.36) | 74 (24.5) | 198 (33.33) | ||
| Very healthy | 295 (32.92) | 91 (30.13) | 204 (34.34) | ||
| Great healthy | 308 (34.38) | 136 (45.03) | 172 (28.96) | ||
| Changes in health | No change | 469 (51.34) | 169 (55.96) | 300 (50.51) | 15.387 *** (0.000) |
| Got better | 369 (41.18) | 127 (42.05) | 242 (40.74) | ||
| Got worse | 58 (6.47) | 6 (1.99) | 52 (8.75) | ||
| Education | Primary school | 248 (27.68) | 76 (25.17) | 172 (28.96) | 2.592 (0.459) |
| Junior high school | 280 (31.25) | 103 (34.11) | 177 (29.8) | ||
| High School | 241 (26.9) | 78 (25.83) | 163 (27.44) | ||
| College | 127 (14.17) | 45 (14.9) | 82 (13.8) | ||
| Type of residence | Rural | 468 (55.45) | 149 (52.65) | 319 (55.45) | 1.351 (0.245) |
| Urban | 376 (44.55) | 134 (47.35) | 242 (43.14) | ||
| Family type | non-MHNW families | 781 (87.17) | 255 (84.44) | 526 (88.55) | 3.031 * (0.082) |
| MHNW families | 115 (12.83) | 47 (15.56) | 68 (11.45) | ||
| City type | first-tier cities | 35 (3.91) | 18 (5.96) | 17 (2.86) | 5.14 (0.162) |
| Second-tier cities | 56 (6.25) | 18 (5.96) | 38 (6.4) | ||
| Third-tier cities | 30 (3.35) | 10 (3.31) | 20 (3.37) | ||
| Others | 775 (86.5) | 256 (84.77) | 519 (87.37) | ||
| Depression | Yes | 238 (26.56) | |||
| No | 658 (73.44) | ||||
| Characteristics | Odds Ratio | Drink_Y_18 95% CI | p Value |
|---|---|---|---|
| Frequency of exercise | 0.892 ** | 0.799–0.995 | 0.04 |
| Exercise duration | 0.997 * | 0.993–1.001 | 0.093 |
| Exercise intensity (Re: non- intense) | |||
| A little intense | 1.208 | 0.765–1.908 | 0.417 |
| Intense | 1.723 ** | 1.059–2.804 | 0.028 |
| Housework time | 1.187 ** | 1.018–1.385 | 0.029 |
| Gender (Re: female) | |||
| Male | 1.022 | 0.738–1.417 | 0.894 |
| Happiness | 0.801 *** | 0.731–0.876 | 0.001 |
| Age | 1.062 | 0.922–1.224 | 0.83 |
| Health status (Re: average or unhealthy) | |||
| Relatively healthy | 0.18 | 0.023–1.406 | 0.102 |
| Very healthy | 0.175 * | 0.022–1.367 | 0.096 |
| Great healthy | 0.114 ** | 0.015–0.886 | 0.038 |
| Changes in health (Re: no change) | |||
| Got better | 1.066 | 0.772–1.47 | 0.698 |
| Got worse | 3.065 ** | 1.22–7.698 | 0.017 |
| Education (Re: illiterate/semi-literate) | |||
| Primary school | 0.538 ** | 0.308–0.942 | 0.03 |
| Junior high school | 0.521 | 0.211–1.285 | 0.157 |
| High School | 0.406 | 0.125–1.322 | 0.134 |
| Type of residence (Re: rural) | |||
| Urban | 0.923 | 0.654–1.304 | 0.651 |
| Family type (Re: non-MHNW families) | |||
| MHNW families | 0.805 | 0.501–1.295 | 0.372 |
| City type (Re: first-tier cities) | |||
| Second-tier cities | 2.206 * | 0.873–5.579 | 0.095 |
| Third-tier cities | 2.074 | 0.716–6.007 | 0.179 |
| Others | 1.812 | 0.842–3.901 | 0.129 |
| Constant | 33.794 ** | 1.874–609.313 | 0.017 |
| LR chi-squared | 95.974 (0.000) | ||
| −2Log likelihood | 980.758 | ||
| Cox and Snell R square | 0.107 | ||
| MacFadden square | 0.089 | ||
| Nagelkerke square | 0.183 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gu, J. Physical Activity and Depression in Adolescents: Evidence from China Family Panel Studies. Behav. Sci. 2022, 12, 71. https://doi.org/10.3390/bs12030071
Gu J. Physical Activity and Depression in Adolescents: Evidence from China Family Panel Studies. Behavioral Sciences. 2022; 12(3):71. https://doi.org/10.3390/bs12030071
Chicago/Turabian StyleGu, Jiafeng. 2022. "Physical Activity and Depression in Adolescents: Evidence from China Family Panel Studies" Behavioral Sciences 12, no. 3: 71. https://doi.org/10.3390/bs12030071
APA StyleGu, J. (2022). Physical Activity and Depression in Adolescents: Evidence from China Family Panel Studies. Behavioral Sciences, 12(3), 71. https://doi.org/10.3390/bs12030071