
Current Intervention Treatments for Food Addiction: A Systematic Review



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Selection Criteria
2.2. Data Extraction and Synthesis
2.3. Study Quality
3. Results
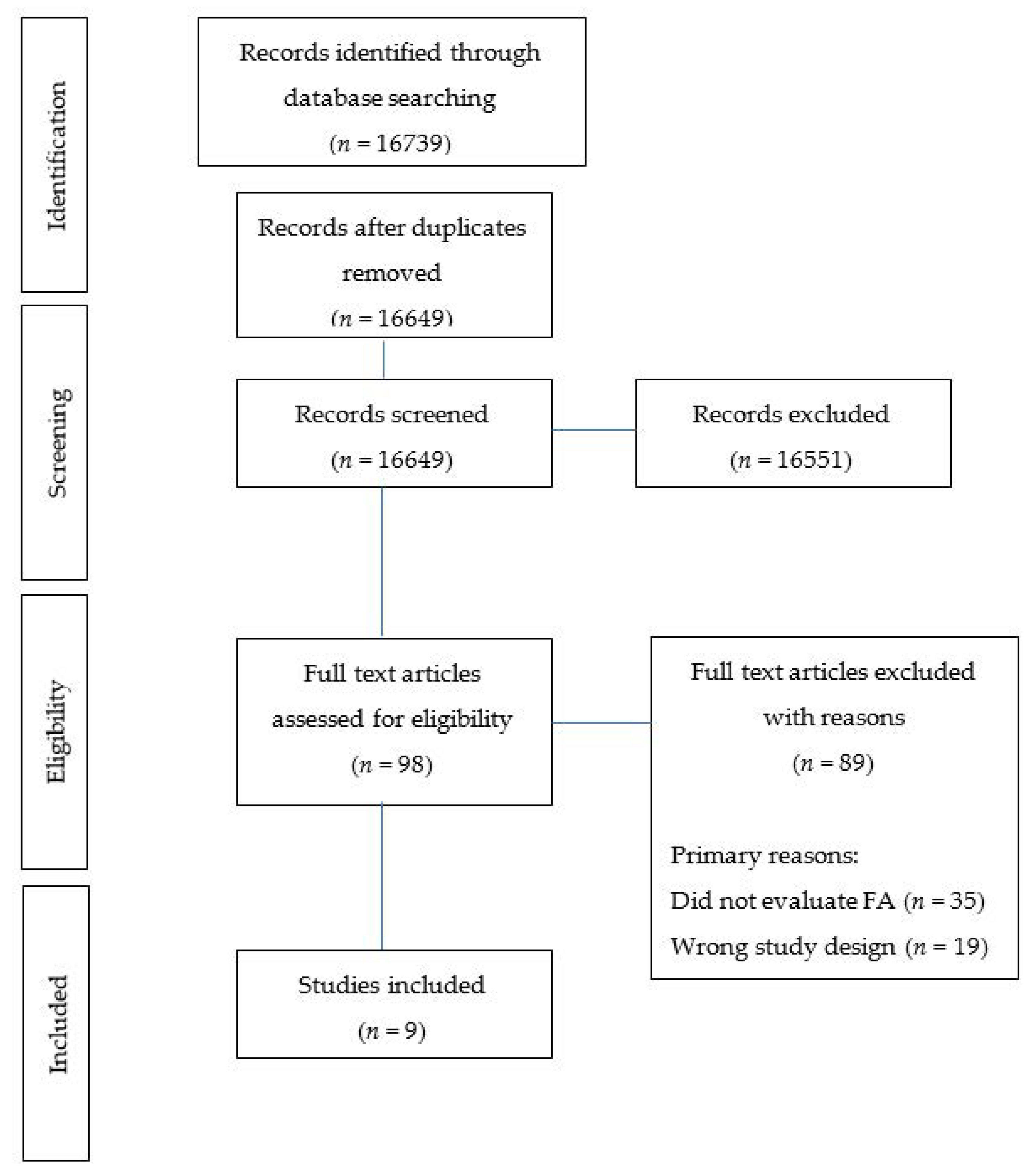
3.1. Search Results
3.2. Description of Included Studies
3.2.1. Participants
3.2.2. Interventions
3.3. Outcomes
Assessment of Outcomes
3.4. Effectiveness of Interventions
3.4.1. Changes Post-Intervention Diagnosis
3.4.2. Changes Post-Intervention Symptom Scores
3.5. Moderators
Changes Post-Intervention Symptom Scores between Sexes and Surgery Type
3.6. Quality Assessment/Risk of Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Study (1st Author, Year) | 1. Was the Research Question Clearly Stated? | 2. Was the Sample of Study Participants Free from Bias? | 3. Were Study Groups Comparable? | 4. Was Method of Handling Withdrawals Described? | 5. Was Blinding Used to Prevent Introduction of Bias? | 6. Were Intervention/Therapeutic Regimens/Exposure Factor or Procedure and Any Comparisons Described in Detail? | 7. Were Outcomes Clearly Defined and the Measurement Valid and Reliable? | 8. Was the Statistical Analysis Appropriate? | 9. Were Conclusions Supported by Results with Biases and Limitations Considered? | 10. Is Bias Due to Study’s Funding or Sponsorship Unlikely? | Overall Quality (+, ø, −) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Carbone E et al., 2020 [38] | Y | N | Y | Y | N | Y | Y | Y | Y | Y | ø |
| Chao A, et al. 2017 [33] | Y | Y | N/A | Y | N | Y | Y | Y | Y | Y | + |
| Epstein D et al., 2016 [31] | Y | U/C | Y | N | Y | Y | Y | Y | Y | Y | + |
| Giel K et al., 2017 [37] | Y | U/C | Y | Y | Y | Y | Y | Y | Y | U/C | + |
| Murray S et al., 2019 [39] | Y | N | Y | Y | U/C | N | Y | Y | Y | Y | ø |
| Nordin A et al., 2017 [36] | Y | U/C | U/C | N | N | N | Y | Y | Y | Y | ø |
| Sevincer G et al., 2016 [34] | Y | N/A | Y | N | N | Y | Y | Y | Y | Y | ø |
| Tompkins C et al., 2017 [35] | Y | N | N/A | N | N | N | Y | Y | Y | Y | ø |
| Vidmar A et al., 2019 [25] | Y | N | Y | N | N | Y | Y | Y | Y | Y | ø |
References
- Davis, C.; Loxton, N.J. A Psycho-Genetic Study of Hedonic Responsiveness in Relation to ‘Food Addiction’. Nutrients 2014, 6, 4338–4353. [Google Scholar] [CrossRef] [PubMed]
- Gearhardt, A.N.; White, M.A.; Masheb, R.M.; Grilo, C.M. An examination of food addiction in a racially diverse sample of obese patients with binge eating disorder in primary care settings. Comp. Psychiatry 2013, 54, 500–505. [Google Scholar] [CrossRef] [PubMed]
- Meule, A. Back by Popular Demand: A Narrative Review on the History of Food Addiction Research. Yale J. Biol. Med. 2015, 88, 295–302. [Google Scholar]
- Pursey, K.M.; Stanwell, P.; Gearhardt, A.N.; Collins, C.E.; Burrows, T.L. The Prevalence of Food Addiction as Assessed by the Yale Food Addiction Scale: A Systematic Review. Nutrients 2014, 6, 4552–4590. [Google Scholar] [CrossRef]
- Burrows, T.; Dayas, C.; Skinner, J.; Pursey, K.M.; Kay-Lambkin, F. Food Addiction and associations with mental health symptoms: A systematic review with meta-analysis. J. Hum. Nutr. Diet. 2018, 31, 544–572. [Google Scholar] [CrossRef]
- Gearhardt, A.N.; Corbin, W.R.; Brownell, K.D. Preliminary validation of the Yale Food Addiction Scale. Appetite 2009, 52, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Burrows, T.; Skinner, J.; McKenna, R.; Rollo, M. Food addiction, binge eating disorder, and obesity: Is there a relationship? Behav. Sci. 2017, 7, 54. [Google Scholar] [CrossRef] [PubMed]
- Meule, A.; Gearhardt, A. Five years of the Yale Food Addiction Survey: Taking stock and moving forward. Curr. Addict. Rep. 2014, 1, 193–205. [Google Scholar] [CrossRef]
- Burrows, T.L.; Hides, L.; Brown, R.; Dayas, C.; Kay-Lambkin, F. Differences in dietary preferences, personality and mental health in Australian adults with and without food addiction. Nutrients 2017, 9, 285. [Google Scholar] [CrossRef] [PubMed]
- Canan, F.; Karaca, S.; Sogucak, S.; Gecici, O.; Kuloglu, M. Eating disorders and food addiction in men with heroin use disorder: A controlled study. Eat. Weight Disord. 2017, 22, 249–257. [Google Scholar] [CrossRef]
- Mason, S.M.; Flint, A.J.; Roberts, A.L. Post-traumatic stress disorder symptoms and food addiction in women by timing and type of trauma exposure. JAMA Psychiatry 2014, 71, 1271–1278. [Google Scholar] [CrossRef] [PubMed]
- Gearhardt, A.N.; Roberto, C.A.; Seamans, M.J.; Corbin, W.R.; Brownell, K.D. Preliminary validation of the Yale Food Addiction Scale in children. Eat. Behav. 2013, 14, 508–512. [Google Scholar] [CrossRef] [PubMed]
- Lawson, J.L.; Wiedemann, A.A.; Carr, M.M.; Kerrigan, S.G. Considering Food Addiction through a cultural lens. Curr. Addict. Rep. 2020, 7, 387–394. [Google Scholar] [CrossRef]
- Meadows, A.; Nolan, L.J.; Higgs, S. Self-perceived food addiction: Prevalence, predictors, and prognosis. Appetite 2017, 114, 282–298. [Google Scholar] [CrossRef]
- McKenna, R.A.; Rollo, M.E.; Skinner, J.A.; Burrows, T.L. Food Addiction Support: Website content analysis. JMIR Cardio 2018, 2, e10. [Google Scholar] [CrossRef] [PubMed]
- Overeaters Anonymous. 2020. Available online: https://oa.org/app/uploads/2019/12/OAMembership-Survey-2017.pdf (accessed on 12 August 2020).
- Cassin, S.E.; Sijercic, I.; Montemarano, V. Psychosocial Interventions for Food Addiction: A Systematic Review. Curr. Addict. Rep. 2020, 7, 1–11. [Google Scholar] [CrossRef]
- Weinstein, A.; Zlatkes, M.; Gingis, A.; Lejoyeux, M. The effects of a 12-step self-help group for compulsive eating on measures of food addiction, anxiety, depression, and self-efficacy. J. Groups Addict. Recov. 2015, 10, 190–200. [Google Scholar] [CrossRef]
- Mount, R.; Neziroglu, F.; Taylor, C.J. An obsessive-compulsive view of obesity and its treatment. J. Clin. Psychol. 1990, 46, 68–78. [Google Scholar] [CrossRef]
- Miller-Matero, L.R.; Brescacin, C.; Clark, S.M.; Troncone, C.L.; Tobin, E.T. Why WAIT? Preliminary evaluation of the weight assistance and intervention techniques (WAIT) group. Psychol. Health Med. 2019, 24, 1029–1037. [Google Scholar] [CrossRef] [PubMed]
- Webber, K.H.; Mellin, L.; Mayes, L.; Mitrovic, I.; Saulnier, M. Pilot investigation of 2 nondiet approaches to improve weight and health. ALT Ther. Health Med. 2017, 24, 16–20. [Google Scholar]
- Sawamoto, R.; Nozaki, T.; Nishihara, T.; Furukawa, T.; Hata, T.; Komaki, G.; Sudo, N. Predictors of successful long-term weight loss maintenance: A two-year follow-up. Biopsychol. Med. 2017, 11, 14. [Google Scholar] [CrossRef]
- Mason, A.E.; Lustig, R.H.; Brown, R.R.; Acree, M.; Bacchetti, P.; Moran, P.J.; Dallman, M.; Laraia, B.; Adler, N.; Hecht, F.M.; et al. Acute responses to opioidergic blockade as a biomarker of hedonic eating among obese women enrolled in a mindfulness based weight loss intervention trial. Appetite 2015, 91, 311–320. [Google Scholar] [CrossRef] [PubMed]
- Hilker, I.; Sánchez, I.; Steward, T.; Jiménez-Murcia, S.; Granero, R.; Gearhardt, A.N.; Rodríguez-Muñoz, R.C.; Dieguez, C.; Crujeiras, A.B.; Tolosa-Sola, I.; et al. Food addiction in bulimia nervosa: Clinical correlates and association with response to a brief psychoeducational intervention. Eur. Eat. Disord. Rev. 2016, 24, 482–488. [Google Scholar] [CrossRef] [PubMed]
- Vidmar, A.P.; Pretlow, R.; Borzutzky., C.; Wee, C.P.; Fox, D.S.; Fink, C.; Mittelman, S.D. An addiction model-based mobile health weight loss intervention in adolescents with obesity. Pediatr. Obes. 2019, 14, e12464. [Google Scholar] [CrossRef] [PubMed]
- Teasdale, S.B.; Burrows, T.L.; Hayes, T.; Hsia, C.Y.; Watkins, A.; Curtis, J.; Ward, P.B. Dietary intake, food addiction and nutrition knowledge in young people with mental illness. Nutr. Diet. 2020, 77, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Barry, D.T.; Grilo, C.M.; Masheb, R.M. Gender Differences in Patients with Binge Eating Disorder. Int. J. Eat. Disord. 2002, 31, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef]
- Murphy, C.M.; Stojek, M.K.; MacKillop, J. Interrelationships among impulsive personality traits, food addiction, and Body Mass Index. Appetite 2014, 73, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Covidence Systematic Review Software. Veritas Health Innovation, Melbourne, Australia. Available online: www.covidence.org (accessed on 26 May 2020).
- Epstein, D.H.; Kennedy, A.P.; Furnari, M.; Heilig, M.; Shaham, Y.; Phillips, K.A.; Preston, K.L. Effect of the CRF1-receptor antagonist pexacerfont on stress-induced eating and food craving. Psychopharmacology 2016, 233, 3921–3932. [Google Scholar] [CrossRef] [PubMed]
- Dietetics AoNa. In Evidence Analysis Manual: Steps in the Academy Evidence Analysis Process; Academy of Nutrition and Dietetics: Chicago, IL, USA, 2016.
- Chao, A.M.; Wadden, T.A.; Tronieri, J.S.; Pearl, R.L.; Alamuddin, N.; Bakizada, Z.M.; Pinkasavage, E.; Leonard, S.M.; Alfaris, N.; Berkowitz, R.I. Effects of addictive-like eating behaviors on weight loss with behavioral obesity treatment. J. Behav. Med. 2019, 42, 246–255. [Google Scholar] [CrossRef]
- Sevincer, G.M.; Konuk, N.; Bozkurt, S.; Coskun, H. Food addiction and the outcome of bariatric surgery at 1-year: Prospective observational study. Psychiatry Res. 2016, 244, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Tompkins, C.L.; Laurent, J.; Brock, D.W. Food Addiction: A barrier for effective weight management for obese adolescents. Child. Obes. 2017, 13, 462–469. [Google Scholar] [CrossRef]
- Nordin, A.; Adamson, S.J.; Sellman, J.D. Food Addiction does not explain weight gain in smoking cessation. J. Smok. Cessat. 2017, 13, 59–62. [Google Scholar] [CrossRef]
- Giel, K.E.; Speer, E.; Schag, K.; Leehr, E.J.; Zipfel, S. Effects of a food-specific inhibition training in individuals with binge eating disorder-findings from a randomized controlled proof-of-concept study. Eat. Weight Disord. 2017, 22, 345–351. [Google Scholar] [CrossRef]
- Carbone, E.; Caroleo, M.; Rania, M.; Calabro, G.; Staltari, F.A.; Filippis, R.; Aloi, M.; Condoleo, F.; Arturi, F.; Segura-Garcia, C. An open-label trial on the efficacy and tolerability of naltrexone/bupropion SR for treating altered eating behaviours and weight loss in binge eating disorder. Eat. Weight Disord. 2020, 26, 779–788. [Google Scholar] [CrossRef] [PubMed]
- Murray, S.M.; Tweardy, S.; Geliebter, A.; Avena, N.M. A Longitudinal Preliminary Study of addiction-like responses to food and alcohol consumption among individuals undergoing weight loss surgery. Obes. Surg. 2019, 29, 2700–2703. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef]
- Wilfley, D.E.; Welch, R.R.; Stein, R.I.; Spurrell, E.B.; Cohen, L.R.; Saelens, B.E.; Dounchis, J.Z.; Frank, M.A.; Wiseman, C.V.; Matt, G.E. A randomized comparison of group cognitive-behavioral therapy and group interpersonal psychotherapy for the treatment of overweight individuals with binge-eating disorder. Arch. Gen. Psychiatry 2002, 59, 713–721. [Google Scholar] [CrossRef]
- Pursey, K.M.; Collins, C.E.; Stanwell, P.; Burrows, T.L. The stability of ‘food addiction’ as assessed by the Yale Food Addiction Scale in a non-clinical population over 18-months. Appetite 2016, 96, 533–538. [Google Scholar] [CrossRef]
- Burmeister, J.M.; Hinman, N.; Koball, A.; Hoffmann, D.A.; Carels, R.A. Food addiction in adults seeking weight loss treatment. Implications for psychosocial health and weight loss. Appetite 2013, 60, 103–110. [Google Scholar] [CrossRef]
- Lent, M.R.; Eichen, D.M.; Goldbacher, E.; Wadden, T.A.; Foster, G.D. Relationship of food addiction to weight loss and attrition during obesity treatment. Obesity 2014, 22, 52–55. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Chai, L.K.; Collins, R.; Leary, M.; Rollo, M.; Whatnall, M.; Burrows, T. Process evaluation of a personality targeted intervention for addictive eating in Australian adults. Behav. Sci. 2020, 10, 186. [Google Scholar] [CrossRef] [PubMed]
- Elfhag, K.; Rössner, S. Who succeeds in maintaining weight loss? A conceptual review of factors associated with weight loss maintenance and weight regain. Obes. Rev. 2005, 6, 67–85. [Google Scholar] [CrossRef] [PubMed]
- Moseley, I.; Roy, A.; Deluty, A.; Brewer, J.A. Evaluating the Quality of Smartphone Apps for Overeating, Stress, and Craving-Related Eating Using the Mobile Application Rating Scale. Curr. Addict. Rep. 2020, 7, 260–267. [Google Scholar] [CrossRef]
- Pretlow, R.A.; Stock, C.M.; Allison, S.; Roeger, L. Treatment of Child/Adolescent Obesity Using the Addiction Model: A Smartphone App Pilot Study. Child. Obes. 2015, 11, 248–259. [Google Scholar] [CrossRef]
- Grillot, C.L.; Keel, P.K. Barriers to seeking treatment for eating disorders: The role of self-recognition in understanding gender disparities in who seeks help. Int. J. Eat. Disord. 2018, 51, 1285–1289. [Google Scholar] [CrossRef]
- Yekaninejad, M.S.; Badrooj, N.; Vosouhghi, F.; Lin, C.Y.; Potenza, M.N.; Pakpour, A.H. Prevalence of food addiction in children and adolescents: A systematic review and meta-analysis. Obes. Rev. 2021, 1–12. [Google Scholar]
- Dhaliwal, J.; Nosworthy, N.; Holt, N.L.; Zwaigenbaum, L.; Avis, J.; Rasquinha, A.; Ball, G. Attrition and the Management of Pediatric Obesity: An Integrative Review. Child. Obes. 2014, 10, 461–473. [Google Scholar] [CrossRef]

| Author, Year, Country | Type of Study | Number of Participants (Including Sex) | Retention Rate | Population Studied | Participant Characteristics (Age) | Participant Characteristics (BMI) | Participant Characteristics (Ethnicity) | YFAS Details | Symptom/Diagnosis |
|---|---|---|---|---|---|---|---|---|---|
| Carbone, 2020, Italy [38] | Control Trial Control: Individuals with obesity and non-BED | n = 43 Sex: Group 1 (individuals with obesity and BED), F n = 17/23 (73.9%), Group 2 (Individuals with obesity and non-BED), F n = 10/20 (50%) | 79.1% (n = 34) Group 1, F n = 15/19 Group 2, F n = 8/15 | Individuals with obesity with/without BED | Group 1 (individuals with obesity and BED) 41.0 ± 13.2 years Group 2 (individuals with obesity and non-BED) 44.4 ± 14.0 years | Baseline BMI: Group 1 (individuals with obesity and BED) 39.0 ± 7.8 kg/m2 Group 2 (Individuals with obesity and non-BED) 43.8 ± 9.6 kg/m2 | Not Reported | YFAS 2.0 Italian version | Symptom |
| Chao, 2019, USA [33] | Pre/Post No control | n = 178 Sex: F n = 156 (87.6%) | 77.5% (n = 138) | Individuals that are OW/OB seeking WL | 44.2 ± 11.2 years | Baseline BMI: 40.9 ± 5.9 kg/m2 | Black, White, other | YFAS (original) | Symptom + Diagnosis |
| Epstein, 2016, USA [31] | RCT Control: placebo (medication unknown) | n = 31 Sex: Treatment group, F n = 10/13 (76.9%), Placebo group, F n = 15/18 (83.3%) | 74.2% (n = 23) Treatment group, n = 10/13Placebo group, n = 13/18 | Adults that scored ≥15 DRS for food craving | Treatment group 30.8 ± 8.3 years Placebo group 32.8 ± 10.7 years | Baseline BMI: Treatment group 33.0 ± 11.4 kg/m2 Placebo group 36.4 ± 8.3 kg/m2 | African American, European American, other | YFAS (original) recorded daily | Symptom |
| Giel, 2017, Germany [37] | RCT Control: no restrictions, control condition (CC group) | n = 22 Sex: F n = 22 (100%) | 90.1% (n = 20) | Patients diagnosed with BED | 36.6 ± 11.9 years | BMI: 29.6 ± 6.3 kg/m2 | Not Reported | YFAS (original) German version | Symptom |
| Murray, 2019, USA [39] | Control Trial Control: (no Treatment) | n = 55 Sex: F n = 25 (93%) | 49.1% (n = 27) Surgery n = 16 Diet n = 6 No treatment n =5 | Patients undergoing Bariatric Surgery | 32.7 ± 7.6 years | BMI: 44.3 ± 4.4 kg/m2 | Hispanic/Latino, Black/African American, White, Native American, Pacific Islander, other | YFAS (original) | Symptom + Diagnosis |
| Nordin, 2017, New Zealand [36] | RCT Control: placebo (oral spray unknown) | n = 256 Sex: F n = 140 (54.7%) | 54.7% (n = 140) attended at least 1 of the F/up visits, 48.4% (n = 124) attended at least 1 of the 1 or 3 month F/up visits, 36.7% (n = 94) attended at least 1 of the 6 or 12 month F/up visits | Adult smokers wishing to quit | 46.2 ± 12.2 years | BMI: 27.4 ± 6.2 kg/m2 (range 16.4–74.1 kg/m2) | Caucasian, Maori, other | YFAS (modified version) | Diagnosis |
| Sevincer, 2016, Turkey [34] | Pre/Post No control | n = 166 Sex: F n = 128 (77.1%) | 50% (n = 83) at 6 months, 30.7% (n = 51) at 12 months | Patients undergoing Bariatric Surgery | 35.6 ± 9.8 years | BMI pre-surgery: 47.0 ± 7.1 kg/m2 (range 36.4–69.4 kg/m2) | Not Reported | YFAS (original) Turkey version | Symptom + Diagnosis |
| Tompkins, 2017, USA [35] | Pre/Post No control | n = 26 Sex: F n = 14 (53.8%) | 50% (n = 13), F n = 6 | Adolescents that are OW/OB seeking WL | Age: 14.0 ± 1.9 years (range 11–18 years) | BMI: 33.0 ± 6.3 kg/m2 (range 24.3–47.3 kg/m2) | Caucasian | YFAS (children version) | Symptom + Diagnosis |
| Vidmar, 2019, USA [25] | Control Trial Control: Usual care (multidisciplinary weight management clinic = Empower group) | n = 35 Sex: Empower group, F n = 8/17 (47.1%) Application group, F n = 13/18 (72.2%) | Empower group 35% (n = 6) at 6 months Application group 100% (n = 18) at 6 months | Adolescents that are obese seeking WL | Empower group 14.4 ± 1.8 years Application group 14.4 ± 1.7 years | BMI: Not Reported | Ethnicity: Hispanic, Caucasian, Black, other | YFAS (children version) | Symptom |
| Author, Year, Country | Intervention Type | Prevalence of FA as per YFAS Diagnosis | YFAS Symptoms, Mean (SD) Pre Intervention | YFAS Symptoms, Mean (SD) Post-Intervention | Intervention Length | Follow Up (Post-Intervention) | Quality Rating |
|---|---|---|---|---|---|---|---|
| Carbone, 2020, Italy [38] | Medication: naltrexone + bupropion + Lifestyle modification: hypocaloric diet reducing daily cals of about 500 cal, behavioural counselling, physical activity | Not Reported | Group 1 (individuals with obesity and BED)—6.5 (3.5) (n = 23) Group 2 (individuals with obesity and non-BED)—3.4 (2.5) (n = 20) | Group 1 (individuals with obesity and BED) n = 19, 3.4 (3.6) Group 2 (individuals with obesity and non-BED) n = 15, 2.9 (3.0) | 16 weeks | Nil | Neutral |
| Chao, 2019, USA [33] | Lifestyle modification: 14 × 90 min lifestyle mod sessions led by registered dietitians or psychologists. Weeks 2–12 follow 1000–1200 cal/day diet (4 serves of choc/vanilla liquid shakes 160–170cal/shake, a pre-packaged/frozen food entrée 250–300 cal, 1–2 serve fruit and side salad. weeks 12–14 refeeding diet replacing shakes with conventional foods. week 6 > increase physical activity to reach 175 min/week by week 14 | FA diagnosis: baseline = 6.7% (n = 12) of 178 participants post = 1.4% (n = 2) of 138 participants | 2.24 (1.58) (n = 138) | 1.93 (1.24) from n = 138 | 14 weeks | Nil | Positive |
| Epstein, 2016, USA [31] | Medication: pexacerfont- corticotropin-releasing factor (CRF) antagonist vs placebo medication (unknown) | Not Reported | Treatment group 6.5 (4.3) (n = 13) Placebo group 7.8 (4.2) (n = 18) * Treatment group 2.4 (2.6) Placebo group 4.1 (2.3) | Reported as least-squares means: pexacerfont, 1.59 ± 0.30; placebo, 2.49 ± 0.27 * Treatment group 1.9 (2.9) Placebo group 2.0 (3.9) | 35 days | Nil | Positive |
| Giel, 2017, Germany [37] | Behavioural: food specific inhibition training | Not Reported | FIT group—3.4 (1.8) (n = 10) CC group—3.4 (1.4) (n = 10) | FIT group n = 10 3.4 (1.3) CC group n =10 3.5 (1.8) | 2 weeks | 4 weeks post-intervention Binge eating only, no YFAS | Positive |
| Murray, 2019, USA [39] | Surgical: (RYGB + SG) + Diet: weight loss (liquid meal replacement diet for 3 months) or no treatment (control) | FA diagnosis: baseline = 6.3% surgery group, 33.3% diet group, 40% no treatment group | Baseline surgery 1.9 (n = 16) diet 2.7 (n = 6) no treatment 3.2 (n = 5) (interpreted from graph) | 4 months Surgery 1.2 (n = 16) Diet 1.6 (n = 6) No treatment 3.5 (n = 5) 24 months Surgery 0.9 (n = 16) Diet 2.3 (n = 6) No treatment 2.8 (n = 5) (interpreted from graph) Sig diff between baseline and both f/up time points in surgery group only | Surgery | 4 months + 24 months | Neutral |
| Nordin, 2017, New Zealand [36] | Medication: oral nicotine spray vs oral placebo spray (unknown) | FA diagnosis: baseline = 0.8% (n = 2) 1 and 3 month = 0% 6 and 12 month = 1.1% (n = 1) | Not Reported | Not Reported | 6 months | 1 and 3 months (early F/up) 6 and 12 months (late F/up) | Neutral |
| Sevincer, 2016, Turkey [34] | Surgical: laparoscopic sleeve gastrectomy + omega loop gastric bypass | FA diagnosis: baseline = 57.8% (n = 96) 6 month = 7.2% (n = 6) 12 month = 13.7% (n = 7) | 3.75 (1.44) (n = 166) | 6 month 2.79 (1.00) (n = 83) 12 month 2.96 (1.25) (n = 51) | Surgery | 6 months + 12 months | Neutral |
| Tompkins, 2017, USA [35] | Lifestyle modification: 12 week multidisciplinary weight management program (consisting of physical activity and nutrition instruction, as well as behavioural instruction derived from SCT) in outpatient setting | FA diagnosis: Baseline = 30.7% (n = 8) FA diagnosis completers (n = 13) pre 23.1% (n = 3/13), post 7.7% (n = 1/13) | 2.35 (1.8) (n = 26) 2.08 (1.6) (n = 13) (completers) | 1.00 (0.9) (n = 13) (completers) | 12 weeks | Nil | Neutral |
| Vidmar, 2019, USA [25] | Lifestyle modification: mobile-health technology app (mHealth). Empowergroup—consists of a team of physicians, dietitians, physical therapists and psychologists. Individual behaviour change goals for healthy eating, physical activity, emotional well-being and family support F/up at monthly visits. Applicationgroup—2 × clinic visits at 2 + 6-month intervals + ongoing support via txt msg + weekly phone calls. Stage 1—Participants withdrew from 2 self-selected problem foods at a time, with goal of total abstinence for min 10 consecutive days. Stage 2—Eliminating snacking between meals. Stage 3—Excessive food amounts reduced through weighing and recording serves into the application | Not Reported | N=10/18 (55%) of Application group scored 4 or more on YFAS (children version) at baseline * 4.22 (1.35) | Reported as: no linear relationship between the change in zBMI and YFAS (children version) at baseline (coef = 0.01, 95%CI = −0.02, 0.04. p = 0.52) 17% (3/18) had negative YFAS (children version) scores upon completion of intervention * 3.78 (1.48) | 6 months | Nil | Neutral |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leary, M.; Pursey, K.M.; Verdejo-Garcia, A.; Burrows, T.L. Current Intervention Treatments for Food Addiction: A Systematic Review. Behav. Sci. 2021, 11, 80. https://doi.org/10.3390/bs11060080
Leary M, Pursey KM, Verdejo-Garcia A, Burrows TL. Current Intervention Treatments for Food Addiction: A Systematic Review. Behavioral Sciences. 2021; 11(6):80. https://doi.org/10.3390/bs11060080
Chicago/Turabian StyleLeary, Mark, Kirrilly M. Pursey, Antonio Verdejo-Garcia, and Tracy L. Burrows. 2021. "Current Intervention Treatments for Food Addiction: A Systematic Review" Behavioral Sciences 11, no. 6: 80. https://doi.org/10.3390/bs11060080
APA StyleLeary, M., Pursey, K. M., Verdejo-Garcia, A., & Burrows, T. L. (2021). Current Intervention Treatments for Food Addiction: A Systematic Review. Behavioral Sciences, 11(6), 80. https://doi.org/10.3390/bs11060080