
Motor Vehicle Collisions during Adolescence: The Role of Alexithymic Traits and Defense Strategies


 ,
, 
Abstract
1. Introduction
1.1. Literature Review
1.2. Current Study
2. Materials and Methods
2.1. Subjects, Recruitment and Procedure
2.2. Measures
2.3. Statistical Analyses
3. Results
3.1. Association between Adolescent’s Sex and Motor Vehicle Collisions
3.2. Alexithymic Traits and Defense Strategies Use in the Four Groups
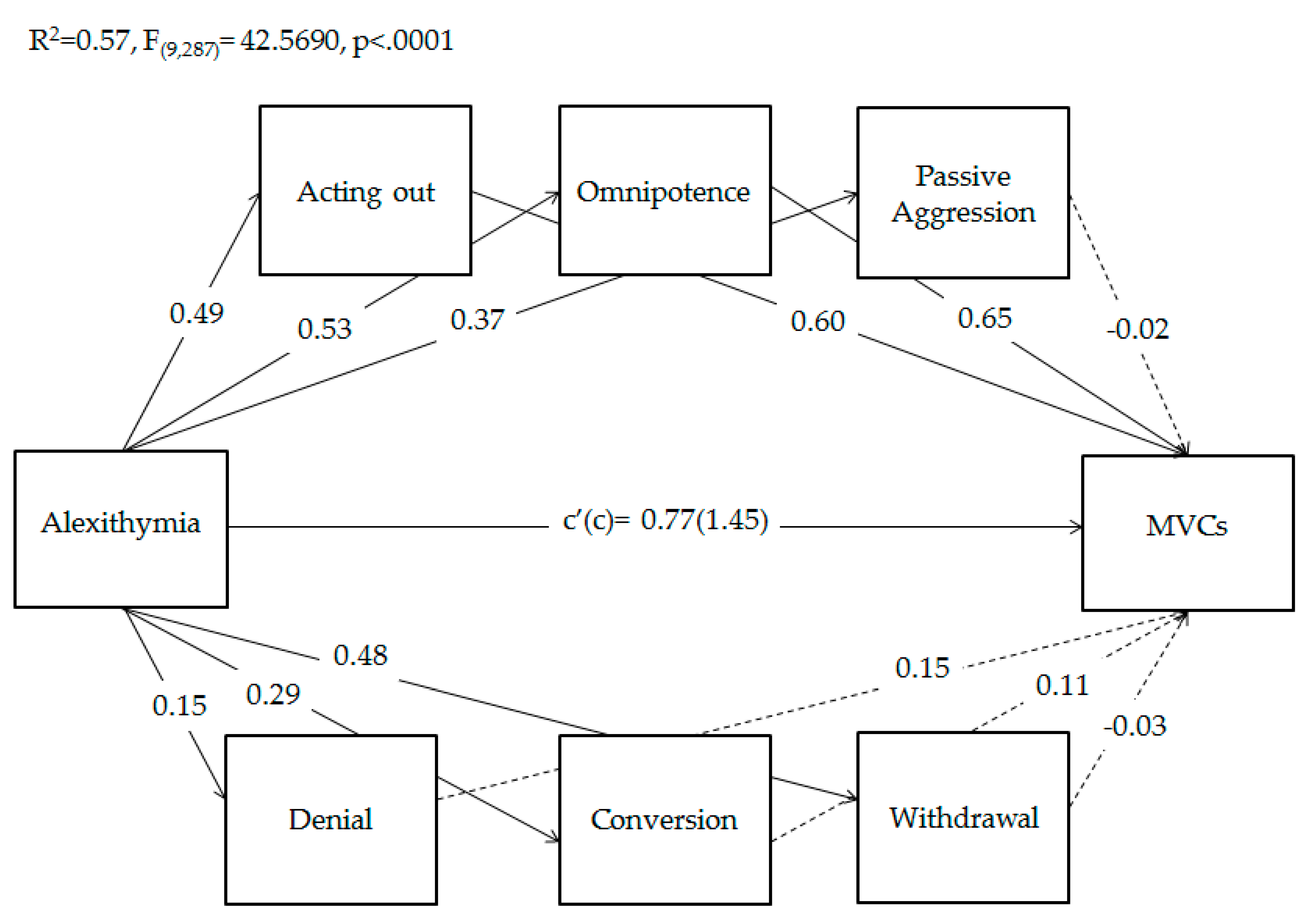
3.3. Adolescents’ Defense Strategies Use as Mediators of the Relationship between Alexithymia and MVCs
4. Discussion
4.1. Main Findings
4.2. The Mediation Role of Defense Strategies Use on the Relationship between Alexithymia and MVCs
4.3. Limitations and Strengths
4.4. Implications for Practice and Clinic Applications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Beck, N.I.; Arif, I.; Paumier, M.F.; Jacobsen, K.H. Adolescent injuries in Argentina, Bolivia, Chile, and Uruguay: Results from the 2012–2013 Global School-based Student Health Survey (GSHS). Injury 2016, 47, 2642–2649. [Google Scholar] [CrossRef] [PubMed]
- Gorios, C.; Souza, R.M.D.; Gerolla, V.; Maso, B.; Rodrigues, C.L.; Armond, J.D.E. Transport accidents among children and adolescents at the emergency service of a teaching hospital in the southern zone of the city of São Paulo. Rev. Bras. Ortop. 2014, 49, 391–395. [Google Scholar] [CrossRef]
- Kwan, K.; Wiebe, D.; Cerdá, M.; Goldman-Mellor, S. Repeat assault injury among adolescents utilizing emergency care: A statewide longitudinal study. J. Emerg. Med. 2019, 57, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Breen, J.M.; Naess, P.A.; Gjerde, H.; Gaarder, C.; Stray-Pedersen, A. The significance of preexisting medical conditions, alcohol/drug use and suicidal behavior for drivers in fatal motor vehicle crashes: A retrospective autopsy study. Forensic Sci. Med. Pathol. 2018, 14, 4–17. [Google Scholar] [CrossRef] [PubMed]
- Le, T.M.T.; Oleck, N.C.; Liu, F.C.; Halsey, J.N.; Hoppe, I.C.; Lee, E.S.; Granick, M.S. Motor vehicle collision injuries: An analysis of facial fractures in the urban pediatric population. J. Craniofac. Surg. 2020, 31, 1910–1913. [Google Scholar] [CrossRef] [PubMed]
- Rothman, L.; Macarthur, C.; Wilton, A.; Howard, A.W.; Macpherson, A.K. Recent trends in child and youth emergency department visits because of pedestrian motor vehicle collisions by socioeconomic status in Ontario, Canada. Inj. Prev. 2019, 25, 570–573. [Google Scholar] [CrossRef] [PubMed]
- McGarvey, C.; Hamilton, K.; Donnelly, J.; Nicholson, A.J. Trends in road transport collision deaths in the Irish paediatric population: A retrospective review of mortality data, 1991–2015. BMJ Paediatr. Open 2019, 3, e000361. [Google Scholar] [CrossRef]
- Peden, M.; Kayede, O.; Ozanne-Smith, J.; Hyder, A.A. World Report on Child Injury Prevention: World Health Organization. 2008, pp. 79–93. Available online: http://www.who.int/violence_injury_prevention/child/injury/world_report/en/ (accessed on 2 March 2021).
- Roberts, Z.; Collins, J.A.; James, D.; Bouamra, O.; Young, M.; Lyttle, M.D.; Roland, D.; Mullen, S.; PERUKI. Epidemiology of adolescent trauma in England: A review of TARN data 2008–2017. Emerg. Med. J. 2020, 37, 25–30. [Google Scholar] [CrossRef]
- Wu, X.; Kaminga, A.C.; Dai, W.; Deng, J.; Wang, Z.; Pan, X.; Liu, A. The prevalence of moderate-to-high posttraumatic growth: A systematic review and meta-analysis. J. Affect disord 2019, 243, 408–415. [Google Scholar] [CrossRef]
- Moreira, M.R.; Ribeiro, J.M.; Motta, C.T.; Motta, J.I.J. Mortality by road traffic accidents in adolescents and young people, Brazil, 1996–2015: Will we achieve SDG 3.6? Cien. Saude Colet. 2018, 23, 2785–2796. [Google Scholar] [CrossRef]
- Wang, H.; Zhou, Y.; Liu, J.; Ou, L.; Zhao, Y.; Han, J.; Xiang, L. Traumatic fractures as a result of motor vehicle collisions in children and adolescents. Int. Orthop. 2018, 42, 625–630. [Google Scholar] [CrossRef] [PubMed]
- Breen, J.M.; Næss, P.A.; Hansen, T.B.; Gaarder, C.; Stray-Pedersen, A. Serious motor vehicle collisions involving young drivers on Norwegian roads 2013–2016: Speeding and driver-related errors are the main challenge. Traffic Inj. Prev. 2020, 21, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Kar, I.N.; Guillaume, C.; Sita, K.R.; Gershon, P.; Simons-Morton, B.G. US adolescent street racing and other risky driving behaviors. J. Adolesc. Health 2018, 62, 626–629. [Google Scholar] [CrossRef] [PubMed]
- Shults, R.A.; Bergen, G.; Smith, T.J.; Cook, L.; Kindelberger, J.; West, B. Characteristics of single vehicle crashes with a teen driver in South Carolina, 2005–2008. Accid. Anal. Prev. 2019, 122, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Wu, M.; Cheng, X.; Schwebel, D.C. The road user behaviors of Chinese adolescents: Data from China and a comparison with adolescents in other countries. Ann. Glob. Health 2019, 85, 76. [Google Scholar] [CrossRef] [PubMed]
- WHO, U.; Mathers, C. Global strategy for women’s, children’s and adolescents’ health (2016–2030). Organization 2016, 201, 4–103. [Google Scholar]
- Roberts, S.E.; Vingilis, E.; Wilk, P.; Seeley, J. A comparison of self-reported motor vehicle collision injuries compared with official collision data: An analysis of age and sex trends using the Canadian National Population Health Survey and Transport Canada data. Accid. Anal. Prev. 2008, 40, 559–566. [Google Scholar] [CrossRef]
- Kahane, C.J. Injury Vulnerability and Effectiveness of Occupant Protection Technologies for Older Occupants and Women (No. DOT HS 811 766). 2013. Available online: https://crashstats.nhtsa.dot.gov/Api/Public/ViewPublication/811766 (accessed on 3 March 2021).
- Raphael, D. Adolescence as a gateway to adult health outcomes. Maturitas 2013, 752, 137–141. [Google Scholar] [CrossRef]
- Sawyer, S.M.; Afifi, R.A.; Bearinger, L.H.; Blakemore, S.J.; Dick, B.; Ezeh, A.C.; Patton, G.C. Adolescence: A foundation for future health. Lancet 2012, 379, 1630–1640. [Google Scholar] [CrossRef]
- Crone, E.A.; Dahl, R.E. Understanding adolescence as a period of social–affective engagement and goal flexibility. Nat. Rev. Neurosci. 2012, 13, 636–650. [Google Scholar] [CrossRef]
- Patton, G.C.; Sawyer, S.M.; Santelli, J.S.; Ross, D.A.; Afifi, R.; Allen, N.B.; Arora, M.; Azzopardi, P.; Baldwin, W.; Bonell, C.; et al. Our future: A Lancet commission on adolescent health and wellbeing. Lancet 2016, 387, 2423–2478. [Google Scholar] [CrossRef]
- van Duijvenvoorde, A.C.; Peters, S.; Braams, B.R.; Crone, E.A. What motivates adolescents? Neural responses to rewards and their influence on adolescents’ risk taking, learning, and cognitive control. Neurosci. Biobehav. Rev. 2016, 70, 135–147. [Google Scholar] [CrossRef] [PubMed]
- Lampropoulou, A. The role of the family in adolescents’ subjective well-being. Psychiatriki 2018, 29, 172–182. [Google Scholar] [CrossRef]
- Roach, A. Supportive peer relationships and mental health in adolescence: An integrative review. Issues Ment. Health Nurs. 2018, 39, 723–737. [Google Scholar] [CrossRef]
- Casey, B.J.; Jones, R.M.; Hare, T.A. The adolescent brain. Ann. N. Y. Acad. Sci. 2008, 1124, 111–126. [Google Scholar] [CrossRef]
- Petanjek, Z.; Kostović, I. Epigenetic regulation of fetal brain development and neurocognitive outcome. Proc. Natl. Acad. Sci. USA 2012, 109, 11062–11063. [Google Scholar] [CrossRef] [PubMed]
- Vijayakumar, N.; Op de Macks, Z.; Shirtcliff, E.A.; Pfeifer, J.H. Puberty and the human brain: Insights into adolescent development. Neurosci Biobehav Rev. 2018, 92, 417–436. [Google Scholar] [CrossRef]
- Blakemore, S.J.; Robbins, T.W. Decision-making in the adolescent brain. Nat. Neurosci. 2012, 15, 1184–1191. [Google Scholar] [CrossRef] [PubMed]
- Bludau, A.; Royer, M.; Meister, G.; Neumann, I.D.; Menon, R. Regulation of the Social Brain. Trends Neurosci. 2019, 42, 471–484. [Google Scholar] [CrossRef] [PubMed]
- Casey, B.J.; Heller, A.S.; Gee, D.G.; Cohen, A.O. Development of the emotional brain. Neurosci Lett. 2019, 693, 29–34. [Google Scholar] [CrossRef]
- Bos, M.; Wierenga, L.M.; Blankenstein, N.E.; Schreuders, E.; Tamnes, C.K.; Crone, E.A. Longitudinal structural brain development and externalizing behavior in adolescence. J. Child. Psychol. Psychiatry 2018, 59, 1061–1072. [Google Scholar] [CrossRef]
- Dow-Edwards, D.; MacMaster, F.P.; Peterson, B.S.; Niesink, R.; Andersen, S.; Braams, B.R. Experience during adolescence shapes brain development: From synapses and networks to normal and pathological behavior. Neurotoxicol. Teratol. 2019, 76, 106834. [Google Scholar] [CrossRef]
- van Hoorn, J.; McCormick, E.M.; Telzer, E.H. Moderate social sensitivity in a risky context supports adaptive decision making in adolescence: Evidence from brain and behavior. Soc. Cogn. Affect. Neurosci. 2018, 13, 546–556. [Google Scholar] [CrossRef]
- Chong, S.L.; Tyebally, A.; Chew, S.Y.; Lim, Y.C.; Feng, X.Y.; Chin, S.T.; Lee, L.K. Road traffic injuries among children and adolescents in Singapore—Who is at greatest risk? Accid. Anal. Prev. 2017, 100, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Mokdad, A.H.; Forouzanfar, M.H.; Daoud, F.; Mokdad, A.A.; El Bcheraoui, C.; Moradi-Lakeh, M.; Kyu, H.H.; Barber, R.M.; Wagner, J.; Cercy, K.; et al. Global burden of diseases, injuries, and risk factors for young people’s health during 1990-2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2016, 387, 2383–2401. [Google Scholar] [CrossRef]
- Ramisetty-Mikler, S.; Almakadma, A. Attitudes and behaviors towards risky driving among adolescents in Saudi Arabia. Int. J. Pediatr. Adolesc. Med. 2016, 3, 55–63. [Google Scholar] [CrossRef]
- Varnaccia, G.; Saß, A.C.; Rommel, A. Unintentional injuries among children and adolescents in Germany. Data sources and results]. Bundesgesundheitsblatt Gesundh. Gesundh. 2014, 57, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Braitman, K.A.; Kirley, B.B.; McCartt, A.T.; Chaudhary, N.K. Crashes of novice teenage drivers: Characteristics and contributing factors. J. Saf. Res. 2008, 39, 47–54. [Google Scholar] [CrossRef]
- Curry, A.E.; Hafetz, J.; Kallan, M.J.; Winston, F.K.; Durbin, D.R. Prevalence of teen driver errors leading to serious motor vehicle crashes. Accid. Anal. Prev. 2011, 43, 1285–1290. [Google Scholar] [CrossRef] [PubMed]
- Bingham, C.R.; Shope, J.T. Adolescent developmental antecedents of risky driving among young adults. J. Stud. Alcohol. 2004, 65, 84–94. [Google Scholar] [CrossRef] [PubMed]
- Behnood, A.; Mannering, F.L. The effects of drug and alcohol consumption on driver injury severities in single-vehicle crashes. Traffic Inj. Prev. 2017, 18, 456–462. [Google Scholar] [CrossRef]
- Hingson, R.; Zha, W.; Simons-Morton, B.; White, A. Alcohol-Induced Blackouts as Predictors of Other Drinking Related Harms Among Emerging Young Adults. Alcohol. Clin. Exp. Res. 2016, 40, 776–784. [Google Scholar] [CrossRef] [PubMed]
- Awaluddin, S.M.; Ahmad, F.H.; Jeevananthan, C.; Ganapathy, S.S.; Sooryanarayana, R.; Mohamad Anuar, M.F.; Alias, N.; Saminathan, T.A.; Mohd Yusoff, M.F.; Rosman, A. Prevalence of Nonfatal Serious Injury Due to Motor Vehicle Accidents Among Malaysian School-Going Adolescents: Findings from the Adolescent Health Survey 2017. Asia Pac. J. Public Health. 2019, 31, 65S–72S. [Google Scholar] [CrossRef] [PubMed]
- Mirman, J.H. Agency, Adolescence, and Motor Vehicle Crash Risk. J. Adolesc. Health. 2018, 62, 509–510. [Google Scholar] [CrossRef] [PubMed]
- Banz, B.C.; Fell, J.C.; Vaca, F.E. Complexities of Young Driver Injury and Fatal Motor Vehicle Crashes. Yale J. Biol. Med. 2019, 92, 725–731. [Google Scholar] [PubMed]
- Hayashi, Y.; Rivera, E.A.; Modico, J.G.; Foreman, A.M.; Wirth, O. Texting while driving, executive function, and impulsivity in college students. Accid. Anal. Prev. 2017, 102, 72–80. [Google Scholar] [CrossRef] [PubMed]
- MacArthur, G.; Caldwell, D.M.; Redmore, J.; Watkins, S.H.; Kipping, R.; White, J.; Chittleborough, C.; Langford, R.; Er, V.; Lingam, R.; et al. Individual-, family-, and school-level interventions targeting multiple risk behaviours in young people. Cochrane Database Syst. Rev. 2018, 2012, 10. [Google Scholar] [CrossRef] [PubMed]
- Ehsani, J.P.; Gershon, P.; Grant, B.; Zhu, C.; Klauer, S.G.; Dingus, T.A.; Simons-Morton, B.G. Learner Driver Experience and Teenagers’ Crash Risk During the First Year of Independent Driving. JAMA Pediatr. 2020, 174, 573–580. [Google Scholar] [CrossRef]
- Marengo, D.; Settanni, M.; Vidotto, G. Drivers’ subtypes in a sample of Italian adolescents: Relationship between personality measures and driving behaviors. Transp. Res. Part F Traffic Psychol. Behav. 2012, 15, 480–490. [Google Scholar] [CrossRef]
- Zhu, D.; Sze, N.N.; Bai, L. Roles of personal and environmental factors in the red light running propensity of pedestrian: Case study at the urban crosswalks. Transp. Res. Part F Traffic Psychol. Behav. 2021, 76, 47–58. [Google Scholar] [CrossRef]
- Zhu, D.; Sze, N.N. Propensities of red light running of pedestrians at the two-stage crossings with split pedestrian signal phases. Accid. Anal. Prev. 2021, 151, 105958. [Google Scholar] [CrossRef] [PubMed]
- Cavalcanti, A.L.; Lino, T.H.; de Oliveira, T.B.; de Oliveira, T.S.; Cardoso, A.M.; de Macedo, R.F.; Padilha, W.W.; Xavier, A.F. Head and maxillofacial injuries in child and adolescent victims of automotive accidents. Sci. World J. 2014, 632720. [Google Scholar] [CrossRef] [PubMed]
- Papadatou, D.; Bellali, T.; Tselepi, K.; Giannopoulou, I. Adolescents’ trajectory through peer loss after a road traffic accident. Death Stud. 2018, 42, 383–391. [Google Scholar] [CrossRef]
- Horvath, C.; Lewis, I.; Watson, B. The beliefs which motivate young male and female drivers to speed: A comparison of low and high intenders. Accid. Anal. Prev. 2012, 45, 334–341. [Google Scholar] [CrossRef] [PubMed]
- McDonald, C.C.; Sommers, M.S.; Fargo, J.D. Risky driving, mental health, and health-compromising behaviours: Risk clustering in late adolescents and adults. Inj. Prev. 2014, 20, 365–372. [Google Scholar] [CrossRef]
- Steinberger, F.; Moeller, A.; Schroeter, R. The antecedents, experience, and coping strategies of driver boredom in young adult males. J. Saf. Res. 2016, 59, 69–82. [Google Scholar] [CrossRef]
- Kumar, S.; Mahima; Srivastava, D.K.; Kharya, P.; Sachan, N.; Kiran, K. Analysis of risk factors contributing to road traffic accidents in a tertiary care hospital. A hospital based cross-sectional study. Chin. J. Traumatol. 2020, 23, 159–162. [Google Scholar] [CrossRef]
- Cicchetti, D.A.N.T.E.; Beauchaine, T.P.; Hinshaw, S.P. A multiple-levels-of-analysis perspective on research in development and psychopathology. Child. Adolesc. Psychol. 2008, 1, 27–57. [Google Scholar]
- Sroufe, L.A.; Rutter, M. The domain of developmental psychopathology. Child. Dev. 1984, 55, 17–29. [Google Scholar] [CrossRef]
- Cerniglia, L.; Cimino, S.; Ballarotto, G.; Casini, E.; Ferrari, A.; Carbone, P.; Cersosimo, M. Motor vehicle accidents and adolescents: An empirical study on their emotional and behavioral profiles, defense strategies and parental support. Transp. Res. Part. F Traffic Psychol. Behav. 2015, 35, 28–36. [Google Scholar] [CrossRef]
- Cimino, S.; Simonelli, A.; Parolin, M.; Ballarotto, G.; Carbone, P.; Cerniglia, L. Theoretical and Empirical Linkage between Road Accidents and Binge Eating Behaviors in Adolescence. Int. J. Environ. Res. Public Health 2018, 15, 355. [Google Scholar] [CrossRef]
- M’bailara, K.; Atzeni, T.; Contrand, B.; Derguy, C.; Bouvard, M.P.; Lagarde, E.; Galéra, C. Emotional reactivity: Beware its involvement in traffic accidents. Psychiatry Res. 2018, 262, 290–294. [Google Scholar] [CrossRef]
- Carbone, P. Le Ali di Lcaro; Capire e Prevenire Gli Incidenti dei Giovani; Bollati Boringhieri: Torino, Italy, 2009. [Google Scholar]
- Carbone, P.; Casini, E.; Ferrari, A. Pronto Soccorso. In Adolescenze Itinerari Psicoanalitici; Carbone, P., Cimino, S., Eds.; Edizione Magi: Roma, Italy, 2017. [Google Scholar]
- Scott-Parker, B.; Watson, B.; King, M.J.; Hyde, M.K. The psychological distress of the young driver: A brief report. Inj. Prev. 2011, 17, 275–277. [Google Scholar] [CrossRef]
- Aduen, P.A.; Day, T.N.; Kofler, M.J.; Harmon, S.L.; Wells, E.L.; Sarver, D.E. Social Problems in ADHD: Is it a Skills Acquisition or Performance Problem? J. Psychopathol. Behav. Assess. 2018, 40, 440–451. [Google Scholar] [CrossRef] [PubMed]
- Aduen, P.A.; Kofler, M.J.; Cox, D.J.; Sarver, D.E.; Lunsford, E. Motor vehicle driving in high incidence psychiatric disability: Comparison of drivers with ADHD, depression, and no known psychopathology. J. Psychiatr. Res. 2015, 64, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Räisänen, T.; Hakko, H.; Riipinen, P.; Räty, E.; Kantojärvi, L. Personality disorders of drivers killed in fatal motor vehicle accidents in Finland during 1990-2011. Acta Psychiatr. Scand. 2019, 140, 39–49. [Google Scholar] [CrossRef]
- Wachs, S.; Vazsonyi, A.T.; Wright, M.F.; Ksinan Jiskrova, G. Cross-National Associations Among Cyberbullying Victimization, Self-Esteem, and Internet Addiction: Direct and Indirect Effects of Alexithymia. Front. Psychol. 2020, 11, 1368. [Google Scholar] [CrossRef] [PubMed]
- Cerniglia, L.; Guicciardi, M.; Sinatra, M.; Monacis, L.; Simonelli, A.; Cimino, S. The Use of Digital Technologies, Impulsivity and Psychopathological Symptoms in Adolescence. Behav. Sci. 2019, 9, 82. [Google Scholar] [CrossRef]
- Parolin, M.; Miscioscia, M.; De Carli, P.; Cristofalo, P.; Gatta, M.; Simonelli, A. Alexithymia in Young Adults With Substance Use Disorders: Critical Issues About Specificity and Treatment Predictivity. Front. Psychol. 2018, 9, 645. [Google Scholar] [CrossRef]
- Gonzales, N.A.; Liu, Y.; Jensen, M.; Tein, J.Y.; White, R.; Deardorff, J. Externalizing and internalizing pathways to Mexican American adolescents’ risk taking. Dev. Psychopathol. 2017, 29, 1371–1390. [Google Scholar] [CrossRef]
- Fang, S.; Chung, M.C.; Wang, Y. The impact of past trauma on psychological distress: The roles of defense mechanisms and alexithymia. Front. Psychol. 2020, 11, 992. [Google Scholar] [CrossRef]
- Ziadni, M.S.; Jasinski, M.J.; Labouvie-Vief, G.; Lumley, M.A. Alexithymia, Defenses, and Ego Strength: Cross-sectional and Longitudinal Relationships with Psychological Well-Being and Depression. J. Happiness Stud. 2017, 18, 1799–1813. [Google Scholar] [CrossRef] [PubMed]
- Helmes, E.; McNeill, P.D.; Holden, R.R.; Jackson, C. The construct of alexithymia: Associations with defense mechanisms. J. Clin. Psychol. 2008, 64, 318–331. [Google Scholar] [CrossRef]
- Lenzo, V.; Barberis, N.; Cannavò, M.; Filastro, A.; Verrastro, V.; Quattropani, M.C. The relationship between alexithymia, defense strategies, eating disorders, anxiety and depression. Riv. Psichiatr. 2020, 55, 24–30. [Google Scholar] [PubMed]
- Chung, M.C.; Di, X.; Wan, K.H. Exploring the interrelationship between alexithymia, defense style, emotional suppression, homicide-related posttraumatic stress disorder and psychiatric co-morbidity. Psychiatry Res. 2016, 243, 373–381. [Google Scholar] [CrossRef]
- Khademi, M.; Hajiahmadi, M.; Faramarzi, M. The role of long-term psychodynamic psychotherapy in improving attachment patterns, defense styles, and alexithymia in patients with depressive/anxiety disorders. Trends Psychiatry Psychother. 2019, 41, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Besharat, M.A.; Shahidi, S. What is the relationship between alexithymia and ego defense styles? A correlational study with Iranian students. Asian J. Psychiatr. 2011, 4, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Nikmanesh, Z.; Darvish Molla, M.; Mehranfard, M. The Mediating Role of Alexithymia in the Relationship Between Defense Mechanisms and Tendency to High-risk Behaviors Among Adolescents. J. Res. Health 2021, 11, 29–36. [Google Scholar] [CrossRef]
- Desapriya, E.B.; Iwase, N.; Shimizu, S. Adolescents alcohol related traffic accidents and mortality in 1999–2000—Problem and solutions. Nihon Arukoru Yakubutsu Igakkai Zasshi 2002, 37, 168–178. [Google Scholar]
- Marzilli, E.; Ballarotto, G.; Cimino, S.; Cerniglia, L. Motor vehicle collisions in adolescence: The role of family support. [Incidenti stradali in adolescenza: Il ruolo del supporto genitoriale]. Rass. Psicol. 2018, 34, 17–28. [Google Scholar]
- Lund, J.; Aarø, L.E. Accident prevention. Presentation of a model placing emphasis on human, structural and cultural factors. Saf. Sci. 2004, 42, 271–324. [Google Scholar] [CrossRef]
- Hole, G. Predictors of motor vehicle collisions. In Motor Vehicle Collisions; Academic Press: Cambridge, MA, USA, 2008; pp. 13–43. [Google Scholar]
- Marcelli, D.; Ingrand, P.; Ingrand, I.; Delamour, M. Scale for the Evaluation of Circumstances Surrounding an Accident and the Risk of Recurrence (ECARR): A Prospective Validation Study of Accident Repetition. Psychiatr. Enfant. 2011, 54, 253–299. [Google Scholar] [CrossRef]
- Bagby, R.M.; Parker, J.D.; Taylor, G.J. The twenty-item Toronto Alexithymia Scale--I. Item selection and cross-validation of the factor structure. J. Psychosom. Res. 1994, 38, 23–32. [Google Scholar] [CrossRef]
- La Ferlita, V.; Bonadies, M.; Solano, L.; De Gennaro, L.; Gonini, P. Alessitimia e adolescenza: Studio preliminare di validazione della TAS-20 su un campione di 360 adolescenti italiani. Infanz. E Adolesc. 2007, 6, 131–144. [Google Scholar]
- Steiner, H.; Araujo, K.B.; Koopman, C. The response evaluation measure (REM-71): A new instrument for the measurement of defenses in adults and adolescents. Am. J. Psychiatry 2001, 158, 467–473. [Google Scholar] [CrossRef]
- Prunas, A.; Madeddu, F.; Pozzoli, S.; Gatti, C.; Shaw, R.J.; Steiner, H. The Italian version of the response evaluation measure-71. Compr. Psychiatry 2009, 50, 369–377. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Publications: London, UK, 2017. [Google Scholar]
- Lee, C.W.; Lee, J.; Jun, J.Y.; Lee, S.H.; Yu, S.Y.; Park, J.; Kim, S.J. Associations between defense mechanisms and life satisfaction among North Korean refugees. Ann. Gen. Psychiatry 2021, 20, 18. [Google Scholar] [CrossRef] [PubMed]
- Cordellieri, P.; Baralla, F.; Ferlazzo, F.; Sgalla, R.; Piccardi, L.; Giannini, A.M. Gender effects in young road users on road safety attitudes, behaviors and risk perception. Front. Psychol. 2016, 7, 1412. [Google Scholar] [CrossRef] [PubMed]
- Gardner, M.; Steinberg, L. Peer influence on risk taking, risk preference, and risky decision making in adolescence and adulthood: An experimental study. Dev. Psychol. 2005, 41, 625–635. [Google Scholar] [CrossRef]
- Reniers, R.L.; Murphy, L.; Lin, A.; Bartolomé, S.P.; Wood, S.J. Risk Perception and Risk-Taking Behaviour during Adolescence: The Influence of Personality and Gender. PLoS ONE 2016, 11, e0153842. [Google Scholar] [CrossRef]
- Kim, Y.; Park, I.; Kang, S. Age and gender differences in health risk perception. Cent. Eur. J. Public Health 2018, 26, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Walshe, E.A.; Ward McIntosh, C.; Romer, D.; Winston, F.K. Executive Function Capacities, Negative Driving Behavior and Crashes in Young Drivers. Int. J. Environ. Res. Public Health 2017, 14, 1314. [Google Scholar] [CrossRef] [PubMed]
- Oviedo-Trespalacios, O.; Scott-Parker, B. The sex disparity in risky driving: A survey of Colombian young drivers. Traffic Inj. Prev. 2018, 19, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.M.; Chan, C.C.; Leung, A.W.; Fox, P.T.; Gao, J.H. Sex-related differences in neural activity during risk taking: An fMRI study. Cereb. Cortex. 2009, 19, 1303–1312. [Google Scholar] [CrossRef]
- van den Bos, R.; Homberg, J.; de Visser, L. A critical review of sex differences in decision-making tasks: Focus on the Iowa Gambling Task. Behav. Brain Res. 2013, 238, 95–108. [Google Scholar] [CrossRef] [PubMed]
- Van Leijenhorst, L.; Westenberg, P.M.; Crone, E.A. A developmental study of risky decisions on the cake gambling task: Age and gender analyses of probability estimation and reward evaluation. Dev. Neuropsychol. 2008, 33, 179–196. [Google Scholar] [CrossRef] [PubMed]
- Glendon, A.I.; Dorn, L.; Davies, R.; Matthews, G.; Taylor, R.G. Age and gender differences in perceived accident likelihood and driver competences. Risk Anal. 1996, 16, 755–762. [Google Scholar] [CrossRef]
- Gonzales, J.; Field, T.; Yando, R.; Gonzales, K. Adolescents’ perception of their risk-taking behavior. Adolescence 1994, 29, 701–709. [Google Scholar]
- Quadrel, M.J.; Fischhoff, B.; Davis, W. Adolescent (in)vulnerability. Am. Psychol. 1993, 48, 102–116. [Google Scholar] [CrossRef]
- Harré, N.; Field, J.; Kirkwood, B. Gender differences and areas of common concern in the driving behaviors and attitudes of adolescents. J. Saf. Res. 1996, 27, 163–173. [Google Scholar] [CrossRef]
- Erriu, M. Emotional–Behavioral Profiles and Parental Support in Adolescents with Motor Vehicle Accidents. Eur. Proc. Soc. Behav. Sci. EpSBS 2016, 13, 303–312. [Google Scholar]
- Craparo, G.; Ardino, V.; Gori, A.; Caretti, V. The Relationships between Early Trauma, Dissociation, and Alexithymia in Alcohol Addiction. Psychiatry Investig. 2014, 11, 330–335. [Google Scholar] [CrossRef] [PubMed]
- Gori, A.; Craparo, G.; Caretti, V.; Giannini, M.; Iraci-Sareri, G.; Bruschi, A.; Janiri, L.; Ponti, L.; Tani, F. Impulsivity, alexithymia and dissociation among pathological gamblers in different therapeutic settings: A multisample comparison study. Psychiatry Res. 2016, 246, 789–795. [Google Scholar] [CrossRef] [PubMed]
- Schimmenti, A.; Passanisi, A.; Caretti, V.; La Marca, L.; Granieri, A.; Iacolino, C.; Gervasi, A.M.; Maganuco, N.R.; Billieux, J. Traumatic experiences, alexithymia, and Internet addiction symptoms among late adolescents: A moderated mediation analysis. Addict. Behav. 2017, 64, 314–320. [Google Scholar] [CrossRef]
- Carbone, P. L’Adolescente Prende Corpo; II Pensiero Scientifico Editore: Roma, Italy, 2010. [Google Scholar]
- Berger, S.S.; Elliott, C.; Ranzenhofer, L.M.; Shomaker, L.B.; Hannallah, L.; Field, S.E.; Young, J.F.; Sbrocco, T.; Wilfley, D.E.; Yanovski, J.A.; et al. Interpersonal problem areas and alexithymia in adolescent girls with loss of control eating. Compr. Psychiatry. 2014, 55, 170–178. [Google Scholar] [CrossRef]
- Raffagnato, A.; Angelico, C.; Valentini, P.; Miscioscia, M.; Gatta, M. Using the Body When There Are No Words for Feelings: Alexithymia and Somatization in Self-Harming Adolescents. Front. Psychiatry 2020, 11, 262. [Google Scholar] [CrossRef]
- Shank, L.M.; Tanofsky-Kraff, M.; Kelly, N.R.; Jaramillo, M.; Rubin, S.G.; Altman, D.R.; Byrne, M.E.; LeMay-Russell, S.; Schvey, N.A.; Broadney, M.M.; et al. The association between alexithymia and eating behavior in children and adolescents. Appetite 2019, 142, 104381. [Google Scholar] [CrossRef]
- Fukunishi, I.; Maeda, K.; Kubota, M.; Tomino, Y. Association of alexithymia with low utilization and perception on a measure of social support in patients on peritoneal dialysis. Psychol. Rep. 1997, 80, 127–130. [Google Scholar] [CrossRef]
- Thome, A. Alexithymia and acquired immune deficiency syndrome. Psychother. Psychosom. 1990, 54, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Boogar, I.; Moazedian, A. Improvement of borderline personality disorder at different time frames of transference focused psychotherapy: A case report. J. Med. Sci. 2020, 31, 255–266. [Google Scholar]
- Gross, J.J. Emotion regulation. Handb. Emot. 2008, 3, 497–513. [Google Scholar]
- Greene, D.; Boyes, M.; Hasking, P. he associations between alexithymia and both non-suicidal self-injury and risky drinking: A systematic review and meta-analysis. J. Affect. Disord. 2020, 260, 140–166. [Google Scholar] [CrossRef]
- Lyvers, M.; Jamieson, R.; Thorberg, F.A. Risky cannabis use is associated with alexithymia, frontal lobe dysfunction, and impulsivity in young adult cannabis users. J. Psychoact. Drugs. 2013, 45, 394–403. [Google Scholar] [CrossRef]
- Rachão, I.; Campos, R.C. Personality styles and defense mechanisms in a community sample of adolescents: An exploratory study. Bull. Menn. Clin. 2015, 79, 14–40. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Tozzi, E.; Andrisani, G.; Maiorani, D.; Pezzi, L.; Leopardi, R.; Fiorentini, N.; Sechi, E. Alexithymia in headache sufferers: A psychosomatic symptom or comorbidity in adolescents? Educ. Res. 2013, 4, 289–293. [Google Scholar]
- Manciaux, M.R.G. Accidents in childhood: From epidemiology to prevention. Acta Paediatr. 1985, 74, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Turz, A. Adolescence et Risque; Syros: Paris, France, 1993. [Google Scholar]
- Marcelli, D. La position autistique: Hypotheses psychopathologiques et ontoge-nethiques [The autistic position: Psychopathological and ontogenetic hypothesis]. Psychiatr. Enfant. 1983, 24, 5–55. [Google Scholar]
- Cerniglia, L.; Cimino, S.; Marzilli, E.; Pascale, E.; Tambelli, R. Associations Among Internet Addiction, Genetic Polymorphisms, Family Functioning, and Psychopathological Risk: Cross-Sectional Exploratory Study. JMIR Ment. Health. 2020, 7, e17341. [Google Scholar] [CrossRef]
- Van Hoorn, J.; McCormick, E.M.; Rogers, C.R.; Ivory, S.L.; Telzer, E.H. Differential effects of parent and peer presence on neural correlates of risk taking in adolescence. Soc. Cogn. Affect. Neurosci. 2018, 13, 945–955. [Google Scholar] [CrossRef]
- Marzilli, E.; Cerniglia, L.; Ballarotto, G.; Cimino, S. Internet Addiction among Young Adult University Students: The Complex Interplay between Family Functioning, Impulsivity, Depression, and Anxiety. Int. J. Environ. Res. Public Health 2020, 17, 8231. [Google Scholar] [CrossRef]
- Sherman, L.E.; Greenfield, P.M.; Hernandez, L.M.; Dapretto, M. Peer Influence Via Instagram: Effects on Brain and Behavior in Adolescence and Young Adulthood. Child. Dev. 2018, 89, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Tafà, M.; Marzilli, E.; Cimino, S.; Cerniglia, L.; Bracaglia, F. Anorexic families and bulimic families: Psychopathological risk and family functioning [Famiglie anoressiche e bulimiche: Rischio psicopatologico e funzionamento familiare]. Rass. Psicol. 2017, 34, 5–23. [Google Scholar]
- Weston, L.; Hellier, E. Designing road safety interventions for young drivers–The power of peer influence. Transp. Res. Part F Traffic Psychol. Behav. 2018, 55, 262–271. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Group 1 (n = 117) | Group 2 (n = 84) | Group 3 (n = 47) | Group 4 (n = 49) | |
|---|---|---|---|---|
| Age in years, M(SD) | 16.30(1.77) | 16.01(1.63) | 17.28(1.75) | 17.02(1.80) |
| Sex, n(%) | ||||
| Male | 59(50.4) | 55(65.5) | 39(83.8) | 38(77.6) |
| Female | 58(49.6) | 29(34.5) | 8(17) | 11(22.4) |
| Race, n(%) | ||||
| Caucasian | 115(98.3) | 76(90.5) | 44(93.6) | 44(89.8) |
| Other | 2(1.7) | 8(9.5) | 3(6.4) | 5(10.2) |
| Household income (EUR/year) | ||||
| 0–15,000 | 12(10.2) | 14(16.6) | 5(10.6) | 4(8) |
| 15,001–28,000 | 8(6.8) | 6(7.1) | 4(8.6) | 28(4) |
| 28,001–55,000 | 75(64.1) | 47(55.9) | 35(74.4) | 39(79.6) |
| 55,001–75,000 | 19(16.2) | 15(17.8) | 3(6.4) | 4(8) |
| >75,000 | 3(2.5) | 2(2.3) | 0 | 0 |
| Family structure, n(%) | ||||
| Intact | 84(71.8) | 63(75) | 41(87.2) | 44(89.8) |
| Broken | 33(28.2) | 21(25) | 6(12.8) | 5(10.2) |
| Number of siblings, n(%) | ||||
| 0 | 23(19.5) | 31(37) | 16(3) | 21(42.8) |
| 1–2 | 68(58.1) | 37(44) | 19(40.4) | 15(30.6) |
| 3–5 | 21(17.9) | 15(17.8) | 12(24.3) | 13(26.6) |
| >5 | 5(4.2) | 1(1.2) | 0 | 0 |
| Birth order, n(%) | ||||
| First position | 102(87.1) | 39(46.4) | 27(57.4) | 19(38.8) |
| Other positions | 15(12.8) | 45(53.6) | 20(42.6) | 30(61.2) |
| Adolescent’s Group | Total | |||||
|---|---|---|---|---|---|---|
| Sex | Group 1 | Group 2 | Group 3 | Group 4 | ||
| Male | n | 59 | 55 | 39 | 38 | 191 |
| Exp. Val. | 75.2 | 54.0 | 30.2 | 31.5 | ||
| % within sex | 30.9% | 28.8% | 20.4% | 19.9% | ||
| % within group | 50.4% | 65.5% | 83.0% | 77.6% | ||
| St. R | −4.0 | 0.30 | 2.9 | 2.1 | ||
| Female | n | 58 | 29 | 8 | 11 | 106 |
| Exp. Val. | 41.8 | 30.0 | 16.8 | 17.5 | ||
| % within sex | 54.7% | 27.4% | 7.5% | 10.4% | ||
| % within group | 49.6% | 34.5% | 17.0% | 22.4% | ||
| St. R | 4.0 | −0.30 | −2.9 | −2.1 | ||
| Total | n | 117 | 84 | 47 | 49 | 297 |
| Adolescent’s Group | |||||||
|---|---|---|---|---|---|---|---|
| Group 1 M(SD) | Group 2 M(SD) | Group 3 M(SD) | Group 4 M(SD) | F3293 | p-Value | ||
| TAS-20 | Factor 1 | 7.12(1.72) a | 14.60(3.96) b | 17.44(4.37) c | 19.44(4.18) d | 208.94 | <0.001 |
| Factor 2 | 15.81(5.37) a | 17.58(6.13) a | 16.31(4.98) a | 16.79(6.94) a | 1.56 | 0.19 | |
| Factor 3 | 11.36(3.51) a | 20.86(4.57) b | 21.51(4.99) c | 25.46(5.65) d | 152.86 | <0.001 | |
| Total | 34.30(7.27) a | 53.05(9.02) b | 55.27(7.78) b | 61.71(10.85) c | 163.35 | <0.001 | |
| REM-71 | Acting out | 2.93(1.36) a | 4.28(1.41) b | 5.20(1.69) c | 6.28(1.92) d | 62.93 | <0.001 |
| Splitting | 6.08(1.70) a | 6.11(1.56) a | 5.79(1.86) a | 5.72(1.89) a | 0.83 | 0.47 | |
| Displacement | 4.31(2.02) a | 4.10(1.80) a | 4.34(1.86) a | 4.95(4.81) a | 1.10 | 0.34 | |
| Dissociation | 4.16(1.83) a | 4.42(1.77) a | 4.21(1.54) a | 3.90(1.88) a | 0.91 | 0.43 | |
| Fantasy | 4.05(2.06) a | 4.96(4.03) a | 4.55(2.11) a | 4.25(2.05) a | 1.84 | 0.14 | |
| Omnipotence | 3.45(1.26) a | 5.36(1.09) b | 5.56(1.64) c | 7.27(1.75) d | 97.86 | <0.001 | |
| PassiveAggression | 4.20(1.74) a | 5.13(1.88) b | 5.08(1.73) c | 6.46(1.71) d | 18.96 | <0.001 | |
| Projection | 3.08(1.80) a | 3.17(1.74) a | 3.16(1.91) a | 3.29(2.13) a | 0.15 | 0.92 | |
| Suppression | 4.18(1.85) a | 4.32(1.78) a | 4.35(1.89) a | 4.66(1.89) a | 0.79 | 0.49 | |
| Undoing | 5.13(1.85) a | 5.30(1.63) a | 4.84(1.92) a | 4.76(1.75) a | 1.29 | 0.27 | |
| Sublimation | 5.19(1.61) a | 5.20(1.55) a | 5.15(1.56) a | 5.34(1.68) a | 0.12 | 0.94 | |
| Altruism | 7.13(1.41) a | 7.13(1.44) a | 7.38(1.64) a | 6.75(1.83) a | 1.41 | 0.23 | |
| Denial | 4.39(1.94) a | 4.21(1.73) b | 5.43(1.46) b | 5.85(1.90) c | 12.19 | <0.001 | |
| Humor | 5.07(1.71) a | 5.57(1.82) a | 5.35(1.56) a | 5.66(1.76) a | 1.97 | 0.11 | |
| Idealization | 6.11(1.74) a | 6.40(1.93) a | 6.35(1.96) a | 6.42(1.68) a | 0.54 | 0.65 | |
| Intellectualization | 5.42(1.55) a | 5.30(1.91) a | 4.89(1.56) a | 5.15(1.71) a | 1.19 | 0.31 | |
| Reactive Formation | 4.44(2.57) a | 4.48(1.84) a | 3.78(1.75) a | 4.14(1.64) a | 1.38 | 0.24 | |
| Repression | 4.92(1.60) a | 4.75(1.53) a | 4.83(1.48) a | 4.95(1.79) a | 0.24 | 0.86 | |
| Conversion | 1.33(.79) a | 1.61(1.11) a | 1.86(1.61) a | 2.25(2.06) b | 6.18 | <0.001 | |
| Somatization | 3.42(1.85) a | 3.58(1.93) a | 3.63(1.80) a | 3.92(2.05) a | 0.80 | 0.49 | |
| Withdrawal | 3.76(2.24) a | 5.21(2.18) b | 5.86(1.85) b | 6.55(1.60) c | 26.05 | <0.001 | |
| Indirect Effect | Effect(BootSE) | LLCI | ULCI |
|---|---|---|---|
| Alexithymia→Acting out→MVCs | 0.29(0.05) | 0.16 | 0.46 |
| Alexithymia→Omnipotence→MVCs | 0.34(0.08) | 0.19 | 0.52 |
| Alexithymia→Passive Aggression→MVCs | −0.01(0.05) | −0.12 | 0.09 |
| Alexithymia→Denial→MVCs | 0.02(0.01) | −0.01 | 0.06 |
| Alexithymia→Conversion→MVCs | 0.03(0.04) | −0.04 | 0.12 |
| Alexithymia→ Withdrawal→MVCs | −0.01(0.06) | −0.15 | 0.09 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cimino, S.; Marzilli, E.; Erriu, M.; Carbone, P.; Casini, E.; Cerniglia, L. Motor Vehicle Collisions during Adolescence: The Role of Alexithymic Traits and Defense Strategies. Behav. Sci. 2021, 11, 79. https://doi.org/10.3390/bs11060079
Cimino S, Marzilli E, Erriu M, Carbone P, Casini E, Cerniglia L. Motor Vehicle Collisions during Adolescence: The Role of Alexithymic Traits and Defense Strategies. Behavioral Sciences. 2021; 11(6):79. https://doi.org/10.3390/bs11060079
Chicago/Turabian StyleCimino, Silvia, Eleonora Marzilli, Michela Erriu, Paola Carbone, Elisa Casini, and Luca Cerniglia. 2021. "Motor Vehicle Collisions during Adolescence: The Role of Alexithymic Traits and Defense Strategies" Behavioral Sciences 11, no. 6: 79. https://doi.org/10.3390/bs11060079
APA StyleCimino, S., Marzilli, E., Erriu, M., Carbone, P., Casini, E., & Cerniglia, L. (2021). Motor Vehicle Collisions during Adolescence: The Role of Alexithymic Traits and Defense Strategies. Behavioral Sciences, 11(6), 79. https://doi.org/10.3390/bs11060079