
A Critical Review of Effective Child Mass Trauma Interventions: What We Know and Do Not Know from the Evidence


Abstract
1. Introduction
Child Mass Trauma Intervention Studies
2. Materials and Methods
3. Results
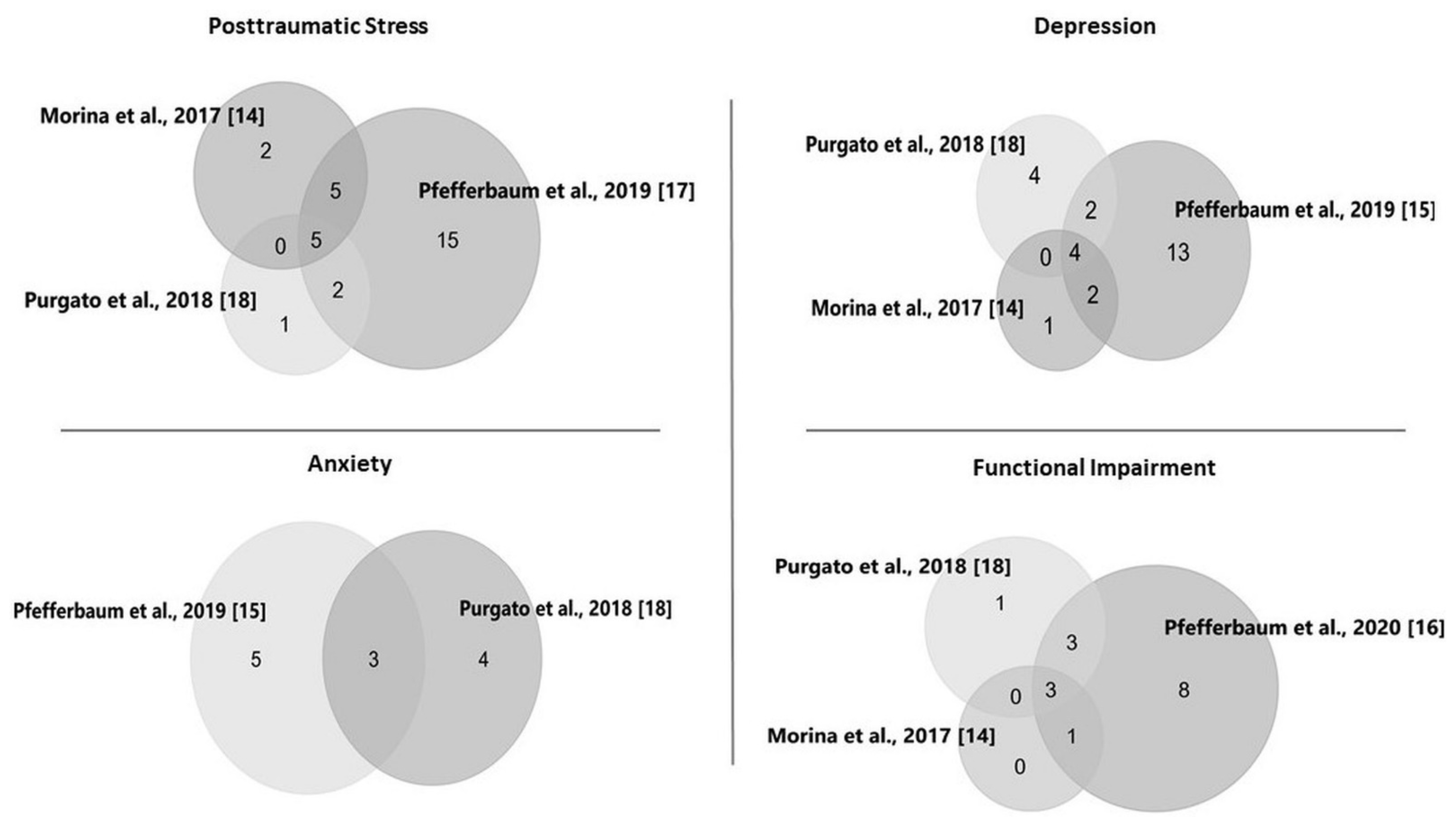
3.1. Differences across Meta-Analyses
3.2. Effectiveness of Interventions
3.3. Follow-Up Findings
3.4. Moderator and Subgroup Analyses
4. Discussion
4.1. Moderator and Subgroup Findings
4.1.1. Characteristics of the Event
4.1.2. Child Characteristics
Sociodemographics
Population Exposure
4.1.3. Contextual Factors
4.1.4. Intervention Features
Trauma Focus
Individual versus Group Application
4.1.5. Aspects of Intervention Delivery
4.2. Implications for Practice
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Commission on Children and Disasters (NCCD). 2010 Report to the President and Congress. 2010. Available online: https://www.acf.hhs.gov/sites/default/files/ohsepr/nccdreport.pdf (accessed on 13 November 2020).
- United Nations Children’s Fund (UNICEF). Machel Study 10-Year Strategic Review. Children and Conflict in a Changing World. 2009. Available online: https://www.unicef.org/publications/index_49985.html (accessed on 23 November 2020).
- Bonanno, G.A.; Brewin, C.R.; Kaniasty, K.; La Greca, A.M. Weighing the costs of disaster: Consequences, risks, and resilience in individuals, families, and communities. Psychol. Sci. 2010, 11, 1–49. [Google Scholar] [CrossRef]
- Furr, J.M.; Comer, J.S.; Edmunds, J.M.; Kendall, P.C. Disasters and youth: A meta-analytic examination of posttraumatic stress. J. Consult. Clin. Psychol. 2010, 78, 765–780. [Google Scholar] [CrossRef]
- Alisic, E.; Zalta, A.K.; van Wesel, F.; Larsen, S.E.; Hafstad, G.S.; Hassanpour, K.; Smid, G.E. Rates of post-traumatic stress disorder in trauma-exposed children and adolescents: Meta-analysis. Br. J. Psychiatry 2014, 204, 335–340. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, K.A.; Koenen, K.C.; Hill, E.D.; Petukhova, M.; Sampson, N.A.; Zaslavsky, A.M.; Kessler, R.C. Trauma exposure and posttraumatic stress disorder in a national sample of adolescents. J. Am. Acad. Child. Adolesc. Psychiatry 2013, 52, 815–830. [Google Scholar] [CrossRef]
- Wang, C.W.; Chan, C.L.W.; Ho, R.T.H. Prevalence and trajectory of psychopathology among child and adolescent survivors of disasters: A systematic review of epidemiological studies across 1987–2011. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 1697–1720. [Google Scholar] [CrossRef] [PubMed]
- Sagi-Schwartz, A. The well being of children living in chronic war zones: The Palestinian-Israeli case. Int. J. Behav. Dev. 2008, 32, 322–336. [Google Scholar] [CrossRef]
- Pfefferbaum, B.; Sweeton, J.L.; Newman, E.; Varma, V.; Nitiéma, P.; Shaw, J.A.; Chrisman, A.K.; Noffsinger, M.A. Child disaster mental health interventions, part I. Techniques, outcomes, and methodological considerations. Disaster Health 2014, 2, 46–57. [Google Scholar] [CrossRef] [PubMed]
- Pfefferbaum, B.; Sweeton, J.L.; Newman, E.; Varma, V.; Noffsinger, M.A.; Shaw, J.A.; Chrisman, A.K.; Nitiéma, P. Child disaster mental health interventions, part II. Timing of implementation, delivery settings and providers, and therapeutic approaches. Disaster Health 2014, 2, 58–67. [Google Scholar] [CrossRef]
- Forman-Hoffman, V.L.; Zolotor, A.J.; McKeeman, J.L.; Blanco, R.; Knauer, S.R.; Lloyd, S.W.; Fraser, J.G.; Viswanathan, M. Comparative effectiveness of interventions for children exposed to nonrelational traumatic events. Pediatrics 2013, 131, 526–539. [Google Scholar] [CrossRef] [PubMed]
- Jordans, M.J.D.; Pigott, H.; Tol, W.A. Interventions for children affected by armed conflict: A systematic review of mental health and psychosocial support in low- and middle-income countries. Curr. Psychiatry Rep. 2016, 18, 9. [Google Scholar] [CrossRef]
- Pfefferbaum, B.; Newman, E.; Nelson, S.D.; Liles, B.D.; Tett, R.P.; Varma, V.; Nitiéma, P. Research methodology used in studies of child disaster mental health interventions for posttraumatic stress. Compr. Psychiatry 2014, 55, 11–24. [Google Scholar] [CrossRef]
- Morina, N.; Malek, M.; Nickerson, A.; Bryant, R.A. Psychological interventions for post-traumatic stress disorders and depression in young survivors of mass violence in low- and middle-income countries: Meta-analysis. Br. J. Psychiatry 2017, 210, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Pfefferbaum, B.; Nitiéma, P.; Newman, E. A meta-analysis of intervention effects on depression and/or anxiety in youth exposed to political violence or natural disasters. Child. Youth Care Forum 2019, 48, 449–477. [Google Scholar] [CrossRef]
- Pfefferbaum, B.; Nitiéma, P.; Newman, E. The effect of interventions on functional impairment in youth exposed to mass trauma: A meta-analysis. J. Child. Adolesc. Trauma 2020, 13, 127–140. [Google Scholar] [CrossRef]
- Pfefferbaum, B.; Nitiéma, P.; Newman, E.; Patel, A. The benefit of interventions to reduce posttraumatic stress in youth exposed to mass trauma: A review and meta-analysis. Prehosp. Disaster Med. 2019, 34, 540–551. [Google Scholar] [CrossRef]
- Purgato, M.; Gross, A.L.; Betancourt, T.; Bolton, P.; Bonetto, C.; Gastaldon, C.; Gordon, J.; O’Callaghan, P.; Papola, D.; Peltonen, K.; et al. Focused psychosocial interventions for children in low-resource humanitarian settings: A systematic review and individual participant data meta-analysis. Lancet Glob. Health 2018, 6, e390–e400. [Google Scholar] [CrossRef]
- Tol, W.A.; Barbui, C.; Galappatti, A.; Silove, D.; Betancourt, T.S.; Souza, R.; Golaz, A.; van Ommeren, M. Mental health and psychosocial support in humanitarian settings: Linking practice and research. Lancet 2011, 378, 1581–1591. [Google Scholar] [CrossRef]
- Brown, R.C.; Witt, A.; Fegert, J.M.; Keller, F.; Rassenhofer, M.; Plener, P.L. Psychosocial interventions for children and adolescents after man-made and natural disasters: A meta-analysis and systematic review. Psycholog. Med. 2017, 47, 1893–1905. [Google Scholar] [CrossRef]
- Newman, E.; Pfefferbaum, B.; Kirlic, N.; Tett, R.; Nelson, S.; Liles, B. Meta-analytic review of psychological interventions for children survivors of natural and man-made disasters. Curr. Psychiatry Rep. 2014, 16, 462. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.; van Ommeren, M.; Belfer, M.; Saxena, S.; Saraceno, B. Children and the Sphere standard on mental and social aspects of health. Disasters 2007, 31, 71–90. [Google Scholar] [CrossRef] [PubMed]
- Summerfield, D. A critique of seven assumptions behind psychological programmes in war-affected areas. Soc. Sci. Med. 1999, 48, 1449–1462. [Google Scholar] [CrossRef]
- Moss, W.J.; Ramakrishnan, M.; Storms, D.; Siegel, A.H.; Weiss, W.M.; Lejnev, I.; Muhe, L. Child health in complex emergencies. Bull. World Health Org. 2006, 84, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Bolton, P.; Bass, J.; Betancourt, T.; Speelman, L.; Onyango, G.; Clougherty, K.F.; Neugebauer, R.; Murray, L.; Verdeli, H. Interventions for depression symptoms among adolescent survivors of war and displacement in Northern Uganda. JAMA 2007, 298, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Brown, F.L.; de Graaff, A.M.; Annan, J.; Betancourt, T.S. Annual research review: Breaking cycles of violence—A systematic review and common practice elements analysis of psychosocial interventions for children and youth affected by armed conflict. J. Child. Psychol. Psychiatry 2017, 58, 507–524. [Google Scholar] [CrossRef]
- Pfefferbaum, B.; Newman, E.; Nelson, S.D. Mental health interventions for children exposed to disasters and terrorism. J. Child. Adolesc. Psychopharmacol. 2014, 24, 24–31. [Google Scholar] [CrossRef]
- Barenbaum, J.; Ruchkin, V.; Schwab-Stone, M. The psychosocial aspects of children exposed to war: Practice and policy initiatives. J. Child. Psychol. Psychiatry 2004, 45, 41–62. [Google Scholar] [CrossRef] [PubMed]
- Williams, R. The psychosocial consequences for children and young people who are exposed to terrorism, war, conflict, and natural disasters. Curr. Opin. Psychiatry 2006, 19, 337–349. [Google Scholar] [CrossRef]
- Jacobson, N.S.; Truax, P. Clinical significance: A statistical approach to defining meaningful change in psychotherapy research. J. Consult. Clin. Psychol. 1991, 59, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Jensen, S.A.; Carralejo, S.M. Measurement issues: Large effect sizes do not mean most people get better—Clinical significance and the importance of individual results. Child. Adolesc. Ment. Health 2017, 22, 163–166. [Google Scholar] [CrossRef]
- Ertl, V.; Neuner, F. Are school-based mental health interventions for war-affected children effective and harmless? BMC Med. 2014, 12, 84. [Google Scholar] [CrossRef]
- Williams, D.D.R.; Garner, J. The case against ‘the evidence’: A different perspective on evidence-based medicine. Br. J. Psychiatry 2002, 180, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D. for the CONSORT Group. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Publication | Number of Trials (k)/Participants (N) a | Summary Effect Size Post-Intervention b | HeterogeneityAmong Studies | Subgroup Analysis | Summary Effect Size at Follow-Up |
|---|---|---|---|---|---|
| Posttraumatic Stress | |||||
| Morina et al. 2017 [14] | k = 12 | g = 0.53 (0.25; 0.81) | Not provided | Not conducted | Unclear |
| Pfefferbaum et al. 2019 [17] | k = 27 N = 4662 | g = 0.57 (0.33; 0.81); p < 0.0001 | Q(26) = 151.21; p < 0.0001; I2 = 83% | - Traumatic event - Population exposure - Country income | Not conducted |
| Purgato et al. 2018 [18] | k = 8 N = 2355 | SMD = 0.33 (0.14; 0.52); p = 0.0006 | Q(7) = 35.52; p < 0.0001; I2 = 80% | - Age - Gender - Household size - Geographic region - Displacement status | 6 weeks or later: 0.21 (0.01; 0.42) (k = 6; N = 1808) |
| Tol et al. 2011 [19] | k = 5 N = 1558 | SMD = 0.36 (−0.10; 0.83); p = 0.12) | Q(4) = 80.99; p < 0.0001; I2 = 95% | Not conducted | Not conducted |
| Depression | |||||
| Morina et al. 2017 [14] | k = 7 | g = 0.25 (0.06; 0.45) | Not provided | Not conducted | Unclear |
| Pfefferbaum et al. 2019 [15] | k = 21 | g = 0.14 (−0.01; 0.28); p = 0.0581 | Q (20) = 42.63; p = 0.0023; I2 = 53%; 95% CI = (23%; 71%) | - Traumatic event - Population exposure - Country income - Trauma-focused intervention component - Intervention application (individual vs. group) - Number of sessions | Not conducted |
| Purgato et al. 2018 [18] | k = 10 N = 2672 | SMD = 0.06 (−0.09; 0.21); p = 0.44 | Q(9) = 32.96; (p = 0.0001); I2 = 73% | - Age - Gender - Household size - Geographic region - Displacement status | 6 weeks or later: 0.09 (0.00; 0.19) (k = 6; N = 1808) |
| Anxiety | |||||
| Pfefferbaum et al. 2019 [15] | k = 8 | g = 0.39 (−0.07; 0.85); p = 0.0855 | Q (7) = 27.91; p = 0.0002; I2 = 75%; 95% CI = (49%; 88%) | - Traumatic event - Population exposure - Country income - Trauma-focused intervention component - Intervention application (individual vs. group) - Number of sessions | Not conducted |
| Purgato et al. 2018 [18] | k = 7 N = 1969 | SMD = 0.03 (−0.13; 0.20); p = 0.70 | Q(6) = 20.14; p = 0.0030; I2 = 70% | - Age - Gender - Household size - Geographic region - Displacement status | 6 weeks or later: 0.08 (−0.04; 0.19) (k = 4; N = 1264) |
| Functional Impairment | |||||
| Morina et al. 2017 [14] | k = 4 | g = 0.36 (0.26; 0.49) | Not provided | Not conducted | g = 0.18, 95% CI (0.06; 0.30) (k = 4) |
| Pfefferbaum et al. 2020 [16] | k = 15 N = 3092 | g = 0.33 (0.16; 0.50); p = 0.0011 | Q(14) = 31.04; p = 0.0055; I2 = 55% (18%; 75%) | - Traumatic event - Population exposure - Country income - Number of sessions | Not conducted |
| Purgato et al. 2018 [18] | k = 7 N = 1895 | SMD = 0.29 (0.14; 0.43) | I2 = 57% | - Age - Gender - Household size - Geographic region - Displacement status | 6 weeks or later: 0.09 (−0.05; 0.23) (k = 5; N = 1404) |
| Publication | Subgroups with Statistically Significant Effect Size | Subgroups with Non-Statistically Significant Effect Size | Subgroups with Statistically Significant Difference |
|---|---|---|---|
| Posttraumatic Stress | |||
| Morina et al. 2017 [14] | Not conducted | Not conducted | Not conducted |
| Pfefferbaum et al. 2019 [17] |
| None | None |
| Purgato et al. 2018 [18] |
|
|
|
| Tol et al. 2011 [19] | Not conducted | Not conducted | Not conducted |
| Depression | |||
| Morina et al. 2017 [14] | Not conducted | Not conducted | Not conducted |
| Pfefferbaum et al. 2019 [15] |
|
| None |
| Purgato et al. 2018 [18] | None |
| None |
| Anxiety | |||
| Pfefferbaum et al. 2019 [15] a |
|
|
|
| Purgato et al. 2018 [18] |
|
| None |
| Functional Impairment | |||
| Morina et al. 2017 [14] | Not conducted | Not conducted | Not conducted |
| Pfefferbaum et al. 2020 [16] |
|
| None |
| Purgato et al. 2018 [18] |
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pfefferbaum, B.; Nitiéma, P.; Newman, E. A Critical Review of Effective Child Mass Trauma Interventions: What We Know and Do Not Know from the Evidence. Behav. Sci. 2021, 11, 25. https://doi.org/10.3390/bs11020025
Pfefferbaum B, Nitiéma P, Newman E. A Critical Review of Effective Child Mass Trauma Interventions: What We Know and Do Not Know from the Evidence. Behavioral Sciences. 2021; 11(2):25. https://doi.org/10.3390/bs11020025
Chicago/Turabian StylePfefferbaum, Betty, Pascal Nitiéma, and Elana Newman. 2021. "A Critical Review of Effective Child Mass Trauma Interventions: What We Know and Do Not Know from the Evidence" Behavioral Sciences 11, no. 2: 25. https://doi.org/10.3390/bs11020025
APA StylePfefferbaum, B., Nitiéma, P., & Newman, E. (2021). A Critical Review of Effective Child Mass Trauma Interventions: What We Know and Do Not Know from the Evidence. Behavioral Sciences, 11(2), 25. https://doi.org/10.3390/bs11020025