Empathy Mediates the Relations between Working Memory and Perpetration of Intimate Partner Violence and Aggression


Abstract
1. Introduction
2. Materials and Methods
2.1. Measures
2.2. Procedures
2.3. Data Analytic Strategy
3. Results
3.1. Demographics and Descriptive Statistics
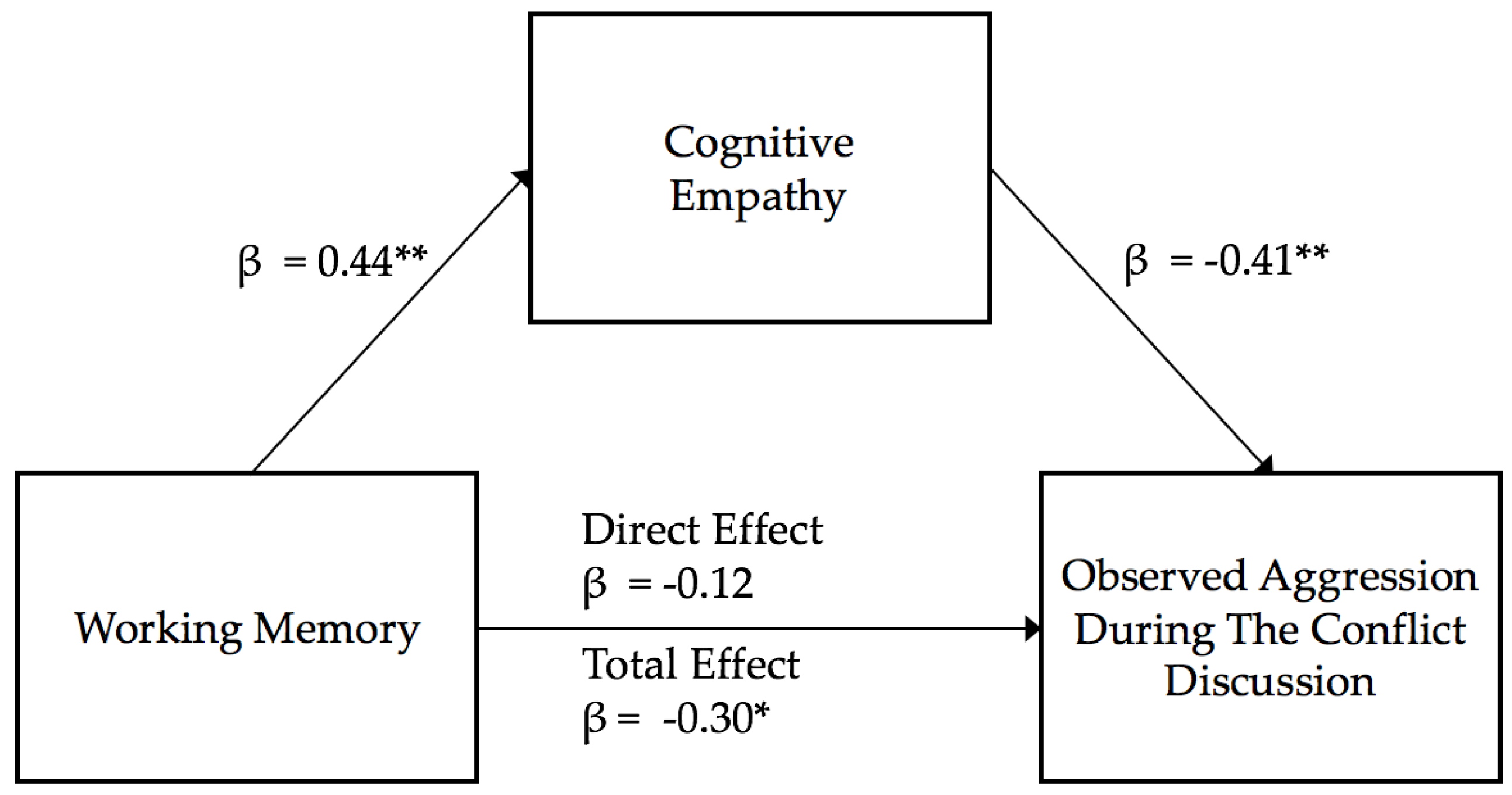
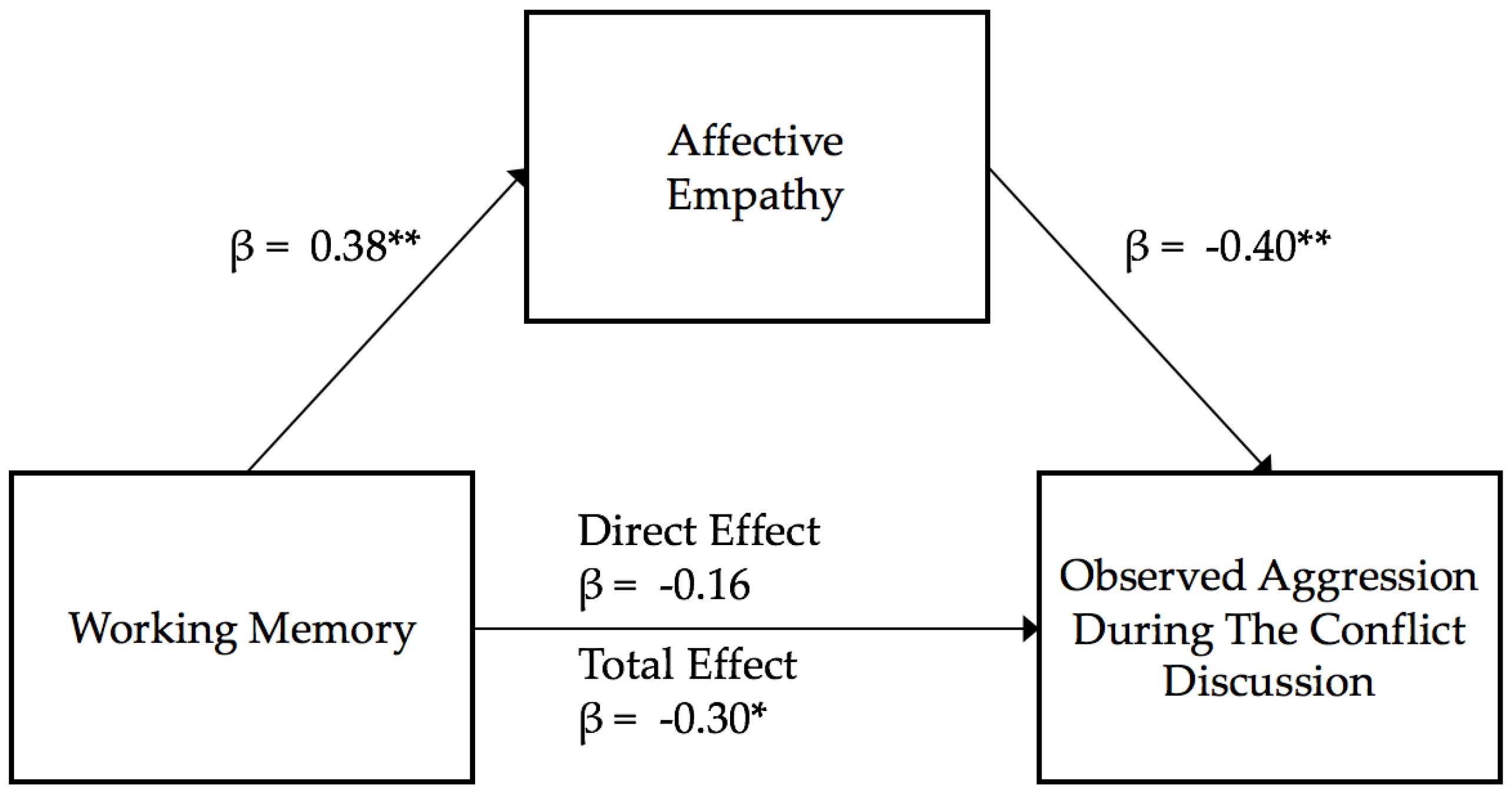
3.2. Estimating Observed Aggression During Interpersonal Conflict
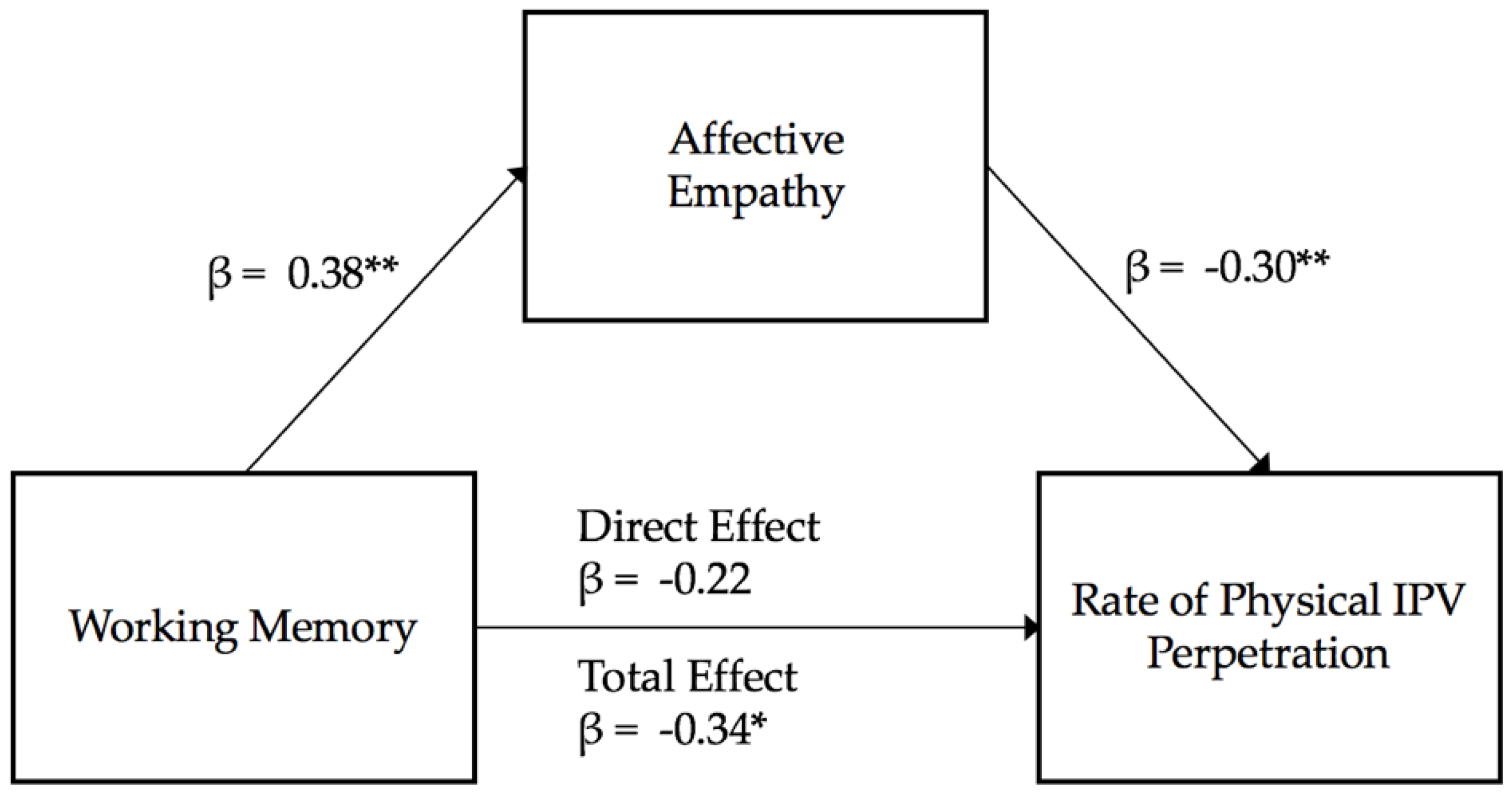
3.3. Estimating Frequency of Male Physical IPV Perpetration
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Breiding, M.J.; Smith, S.G.; Basile, K.C.; Walters, M.L.; Chen, J.; Merrick, M.T. Prevalence and characteristics of sexual violence, stalking, and intimate partner violence victimization—National intimate partner and sexual violence survey, United States, 2011. Morb. Mortal. Wkly. Report. Surveill. Summ. 2014, 63, 1. [Google Scholar]
- National Center for Injury Prevention and Control. Costs of Intimate Partner Violence Against Women in the United States. Atlanta (GA). In Centers for Disease Control and Prevention; 2003. Available online: https://www.cdc.gov/violenceprevention/pdf/ipvbook-a.pdf (accessed on 19 August 2019).
- Coker, A.L.; Davis, K.E.; Arias, I.; Desai, S.; Sanderson, M.; Brandt, H.M.; Smith, P.H. Physical and mental health effects of intimate partner violence for men and women. Am. J. Prev. Med. 2002, 23, 260–268. [Google Scholar] [CrossRef]
- Babcock, J.C.; Green, C.E.; Robie, C. Does batterers’ treatment work? A meta-analytic review of domestic violence treatment. Clin. Psychol. Rev. 2004, 23, 1023–1053. [Google Scholar] [CrossRef] [PubMed]
- Farrer, T.J.; Frost, R.B.; Hedges, D.W. Prevalence of Traumatic Brain Injury in Intimate Partner Violence Offenders Compared to the General Population: A Meta-Analysis. Trauma Violence Abus. 2012, 13, 77–82. [Google Scholar] [CrossRef]
- Rosenbaum, A.; Hoge, S.K. Head injury and marital aggression. Am. J. Psychiatry 1989, 146, 1048–1051. [Google Scholar] [CrossRef]
- Rosenbaum, A.; Hoge, S.K.; Adelman, S.A.; Warnken, W.J.; Fletcher, K.E.; Kane, R.L. Head injury in partner-abusive men. J. Consult. Clin. Psychol. 1984, 62, 1187–1193. [Google Scholar] [CrossRef]
- Walling, S.M.; Meehan, J.C.; Marshall, A.D.; Holtzworth-Munroe, A.; Taft, C.T. The Relationship of Intimate Partner Aggression to Head Injury, Executive Functioning, and Intelligence. J. Marital Fam. Ther. 2012, 38, 471–485. [Google Scholar] [CrossRef]
- Marsh, N.V.; Martinovich, W.M. Executive dysfunction and domestic violence. Brain inj. 2006, 20, 61–66. [Google Scholar] [CrossRef]
- Romero-Martínez, A.; Moya-Albiol, L. Neuropsychology of perpetrators of domestic violence: The role of traumatic brain injury and alcohol abuse and/or dependence. Rev. Neurol. 2013, 57, 515–522. [Google Scholar]
- Bueso-Izquierdo, N.; Hart, S.D.; Hidalgo-Ruzzante, N.; Kropp, P.R.; Pérez-García, M. The mind of the male batterer: A neuroscience perspective. Aggress. Violent Behav. 2015, 25, 243–251. [Google Scholar] [CrossRef]
- Corvo, K. The Role of Executive Function Deficits in Domestic Violence Perpetration. Partn. Abus. 2014, 5, 342–356. [Google Scholar] [CrossRef]
- Cohen, R.A.; Rosenbaum, A.; Kane, R.L.; Warnken, W.J.; Benjamin, S. Neuropsychological Correlates of Domestic Violence. Violence Vict. 1999, 14, 397–411. [Google Scholar] [CrossRef] [PubMed]
- Howard, C.J. Neurobiological correlates of partner abusive men: Equifinality in perpetrators of intimate partner violence. Psychol. Trauma Theory Res. Pract. Policy 2012, 4, 330–337. [Google Scholar] [CrossRef]
- Channon, S.; Pellijeff, A.; Rule, A. Social cognition after head injury: Sarcasm and theory of mind. Brain Lang. 2005, 93, 123–134. [Google Scholar] [CrossRef]
- McDonald, S. Impairments in Social Cognition Following Severe Traumatic Brain Injury. J. Int. Neuropsychol. Soc. 2013, 19, 231–246. [Google Scholar] [CrossRef]
- Eslinger, P.J.; Moore, P.; Anderson, C.; Grossman, M. Social cognition, executive functioning, and neuroimaging correlates of empathic deficits in frontotemporal dementia. J. Neuropsychiatry Clin. Neurosci. 2011, 23, 74–82. [Google Scholar] [CrossRef]
- Spikman, J.M.; Timmerman, M.E.; Milders, M.V.; Veenstra, W.S.; van der Naalt, J. Social Cognition Impairments in Relation to General Cognitive Deficits, Injury Severity, and Prefrontal Lesions in Traumatic Brain Injury Patients. J. Neurotrauma 2011, 29, 101–111. [Google Scholar] [CrossRef]
- Gao, Z.; Ye, T.; Shen, M.; Perry, A. Working memory capacity of biological movements predicts empathy traits. Psychon. Bull. Rev. 2016, 23, 468–475. [Google Scholar] [CrossRef]
- Gu, X.; Eilam-Stock, T.; Zhou, T.; Anagnostou, E.; Kolevzon, A.; Soorya, L.; Hof, P.R.; Friston, K.J.; Fan, J. Autonomic and brain responses associated with empathy deficits in autism spectrum disorder. Hum. Brain Mapp. 2015, 36, 3323–3338. [Google Scholar] [CrossRef]
- Xin, F.; Lei, X. Competition between frontoparietal control and default networks supports social working memory and empathy. Soc. Cogn. Affect. Neurosci. 2015, 10, 1144–1152. [Google Scholar] [CrossRef]
- McLaren, V.; Vanwoerden, S.; Sharp, C. The Basic Empathy Scale: Factor structure and validity in a sample of inpatient adolescents. Psychol. Assess. 2019, 31, 1208–1219. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.-L.; Chou, T.-L. A Dual Route Model of Empathy: A Neurobiological Prospective. Front. Psychol. 2018, 9. [Google Scholar] [CrossRef]
- Ulloa, E.C.; Hammett, J.F.; Meda, N.A.; Rubalcaba, S.J. Empathy and romantic relationship quality among cohabitating couples: An actor–partner interdependence model. Fam. J. 2017, 25, 208–214. [Google Scholar] [CrossRef]
- Ulloa, E.C.; Hammett, J.F. The role of empathy in violent intimate relationships. Partn. Abus. 2016, 7, 140–156. [Google Scholar] [CrossRef]
- Armenti, N.A.; Babcock, J.C. Psychophysiological Reactivity Profiles of Partner-Violent Men With Borderline or Psychopathic Personality Features: The Role of Empathy. Int. J. Offender Ther. Comp. Criminol. 2018, 62, 3337–3354. [Google Scholar] [CrossRef]
- Hildebran, D.; Pithers, W.D. Enhancing offender empathy for sexual-abuse victims. In Relapse Prevention with Sex Offenders; Laws, D.R., Ed.; The Guilford Press: New York, NY, USA, 1989; pp. 236–243. Available online: http://search.ebscohost.com.ezproxy.lib.uh.edu/login.aspx?direct=true&db=psyh&AN=1989-98239-021&site=ehost-live (accessed on 3 January 2020).
- Day, A.; Casey, S.; Gerace, A. Interventions to improve empathy awareness in sexual and violent offenders: Conceptual, empirical, and clinical issues. Aggress. Violent Behav. 2010, 15, 201–208. [Google Scholar] [CrossRef]
- Corsi, P.M. Human memory and the medial temporal region of the brain. Proquest Inf. Learning. 1973, 34, 891. [Google Scholar]
- Brunetti, R.; Del Gatto, C.; Delogu, F. eCorsi: Implementation and testing of the Corsi block-tapping task for digital tablets. Front. Psychol. 2014, 5. [Google Scholar] [CrossRef]
- Straus, M.A.; Hamby, S.L.; Boney-McCoy, S.; Sugarman, D.B. The revised Conflict Tactics Scales (CTS2): Development and preliminary psychometric data. J. Fam. Issues 1996, 17, 283–316. [Google Scholar] [CrossRef]
- Coan, J.A.; Gottman, J.M. The Specific Affect Coding System (SPAFF). In Handbook of Emotion Elicitation and Assessment; Series in affective science; Oxford University Press: New York, NY, USA, 2007; pp. 267–285. [Google Scholar]
- Sommer, J.; Iyican, S.; Babcock, J. The relation between contempt, anger, and intimate partner violence: A dyadic approach. J. Interpers. Violence 2016, 3059–3079. [Google Scholar] [CrossRef]
- Johnson, M.D. The observation of specific affect in marital interactions: Psychometric properties of a coding system and a rating system. Psychol. Assess. 2002, 14, 423–438. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Davis, M.H. A multidimensional approach to individual differences in empathy. JSAS Cat. Sel. Doc. Psychol. 1980, 10, 85. [Google Scholar]
- Ze, O.; Thoma, P.; Suchan, B. Cognitive and affective empathy in younger and older individuals. Aging Ment. Health 2014, 18, 929–935. [Google Scholar] [CrossRef]
- World Health Organization. Ethical and Safety Recommendations for Intervention Research on Violence Against Women: Building on Lessons from the WHO Publication Putting Women First: Ethical and Safety Recommendations for Research on Domestic Violence Against Women; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Hooven, C.; Rushe, R.; Gottman, J.M. The Play-by-Play Interview; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1996. [Google Scholar]
- Curran, P.J.; West, S.G.; Finch, J.F. The robustness of test statistics to nonnormality and specification error in confirmatory factor analysis. Psychol. Methods 1996, 1, 16–29. [Google Scholar] [CrossRef]
- Cohen, J.; Cohen, P.; West, S.G.; Aiken, L.S. Applied Multiple Regression-Correlation Analysis for the Behavioral Sciences. 2002. Available online: http://gen.lib.rus.ec/book/index.php?md5=81DC71AF3E2AFE6145339F1EE1754054 (accessed on 20 October 2019).
- MacKinnon, D.P.; Fairchild, A.J.; Fritz, M.S. Mediation Analysis. Annu. Rev. Psychol. 2007, 58, 593. [Google Scholar] [CrossRef]
- Hudson, S.M.; Marshall, W.L.; Ward, T.; Johnston, P.W.; Jones, R.L. Kia Marama: A cognitive—Behavioural program for incarcerated child molesters. Behav. Chang. 1995, 12, 69–80. [Google Scholar] [CrossRef]
- Bosco, A.; Longoni, A.M.; Vecchi, T. Gender effects in spatial orientation: Cognitive profiles and mental strategies. Appl. Cogn. Psychol. 2004, 18, 519–532. [Google Scholar] [CrossRef]
- Toussaint, L.; Webb, J.R. Gender differences in the relationship between empathy and forgiveness. J. Soc. Psychol. 2005, 145, 673–685. [Google Scholar] [CrossRef]
- Landsberger, H.A. Hawthorne Revisited; Cornell University: Ithaca, NY, USA, 1958. [Google Scholar] [CrossRef]
- Babcock, J.C.; Armenti, N.; Cannon, C.; Lauve-Moon, K.; Buttell, F.; Ferreira, R.; Cantos, A.; Hamel, J.; Kelly, D.R.; Catheleen, J.; et al. Domestic violence perpetrator programs: A proposal for evidence-based standards in the United States. Partn. Abus. 2016, 7, 2–107. [Google Scholar] [CrossRef]
- Redick, T. Working memory training and interpreting interactions in intelligence interventions. Intelligence 2015, 50, 14–20. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1 | 2 | 3 | 4 | 5 | 6 | ||
|---|---|---|---|---|---|---|---|
| 1. Working Memory | |||||||
| 2. Cognitive Empathy | 0.44 ** | ||||||
| 3. Affective Empathy | 0.38 ** | 0.60 *** | |||||
| 4. Observed Aggression | −0.30 * | −0.47 *** | −0.46 ** | ||||
| 5. Physical IPV Perpetration | −0.34 ** | −0.29 * | −0.38 ** | 0.23 | |||
| 6. Psychological IPV Perpetration | −0.22 | −0.17 | −0.34 ** | 0.44 ** | 0.53 *** | ||
| Mean Standard Deviation | Concussion | 60.49 | 16.53 | 18.13 | 16.60 | 3.60 | 31.53 |
| 5.21 | 1.13 | 0.80 | 5.65 | 2.62 | 4.19 | ||
| Mean | No Concussion | 53.32 | 16.00 | 17.52 | 22.44 | 8.37 | 23.98 |
| Standard Deviation | 3.46 | 0.75 | 0.53 | 3.76 | 1.74 | 24.71 | |
| F Statistic (p value) | 1.13 (0.26) | 0.15 (0.70) | 0.41 (0.53) | 0.39 (0.14) | 2.30 (0.14) | 2.07 (0.16) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Godfrey, D.A.; Kehoe, C.M.; Bastardas-Albero, A.; Babcock, J.C. Empathy Mediates the Relations between Working Memory and Perpetration of Intimate Partner Violence and Aggression. Behav. Sci. 2020, 10, 63. https://doi.org/10.3390/bs10030063
Godfrey DA, Kehoe CM, Bastardas-Albero A, Babcock JC. Empathy Mediates the Relations between Working Memory and Perpetration of Intimate Partner Violence and Aggression. Behavioral Sciences. 2020; 10(3):63. https://doi.org/10.3390/bs10030063
Chicago/Turabian StyleGodfrey, Donald A., Caitlin M. Kehoe, Adriana Bastardas-Albero, and Julia C. Babcock. 2020. "Empathy Mediates the Relations between Working Memory and Perpetration of Intimate Partner Violence and Aggression" Behavioral Sciences 10, no. 3: 63. https://doi.org/10.3390/bs10030063
APA StyleGodfrey, D. A., Kehoe, C. M., Bastardas-Albero, A., & Babcock, J. C. (2020). Empathy Mediates the Relations between Working Memory and Perpetration of Intimate Partner Violence and Aggression. Behavioral Sciences, 10(3), 63. https://doi.org/10.3390/bs10030063