Case Report of a Mare Diagnosed with a Metastatic Mammary Carcinoma after the Excision of a Recurrent Intraocular Neuroepithelial Tumor

 , , , and
, , , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials, Methods, and Results
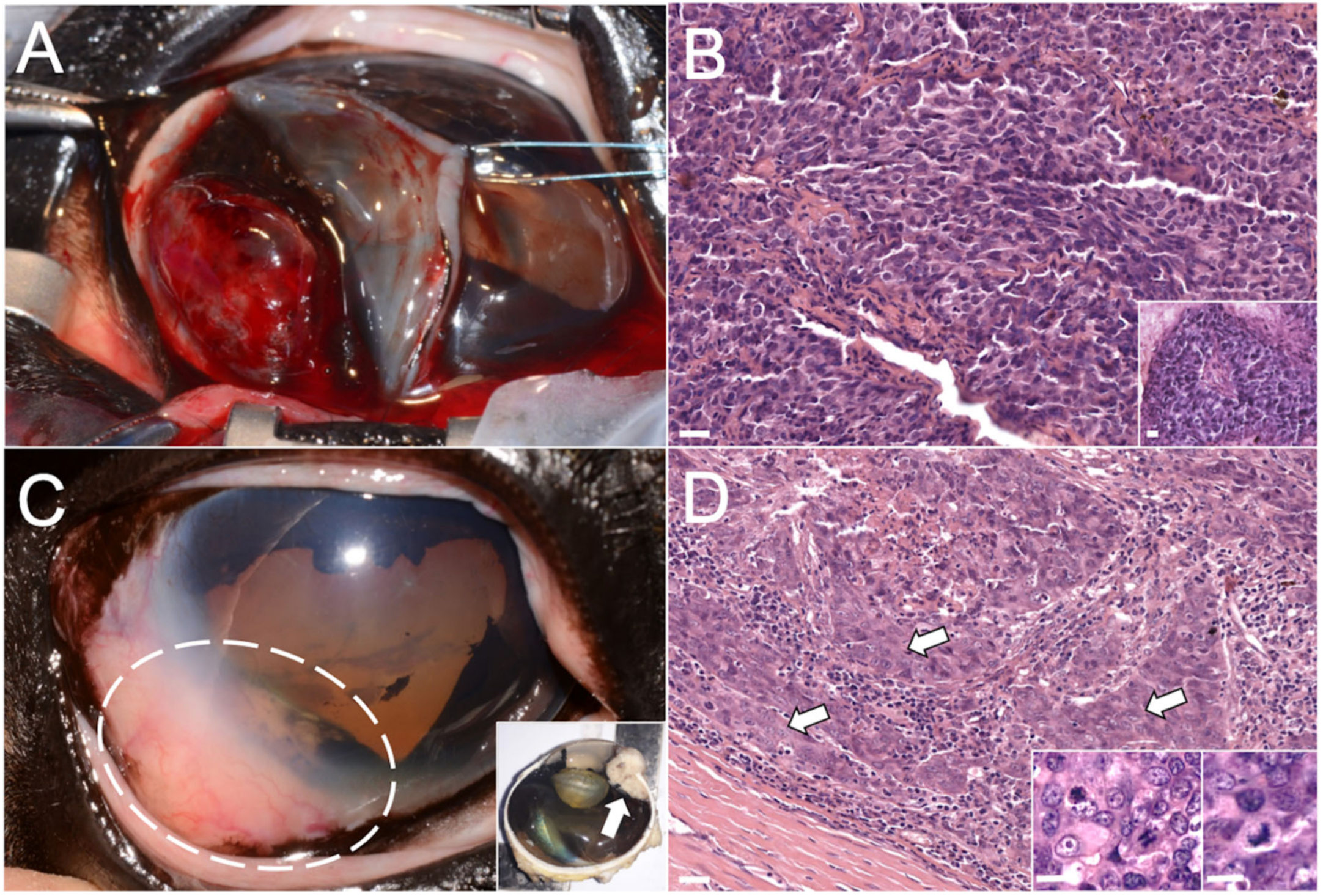
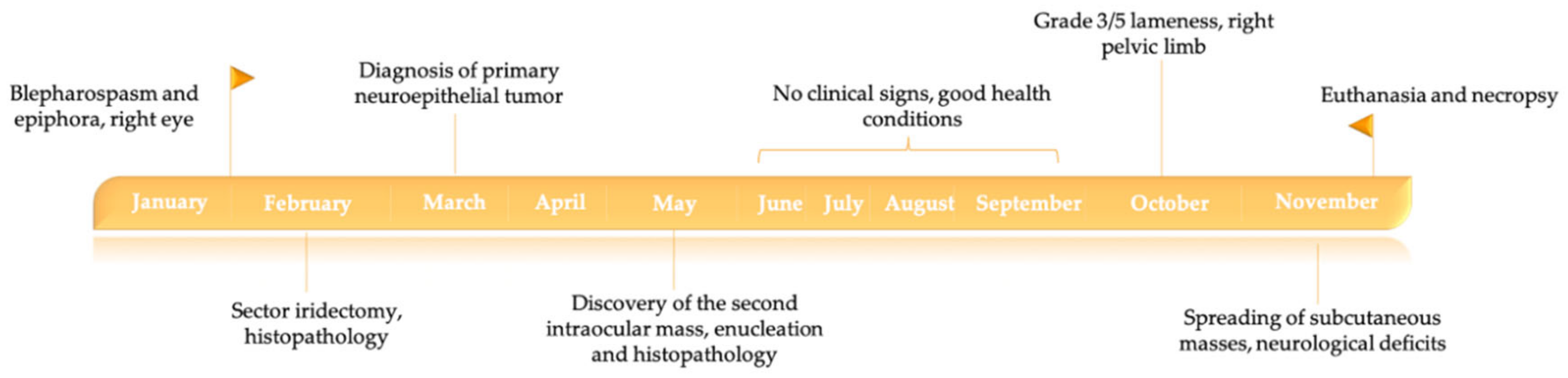
2.1. Case Description and In Vivo Investigations
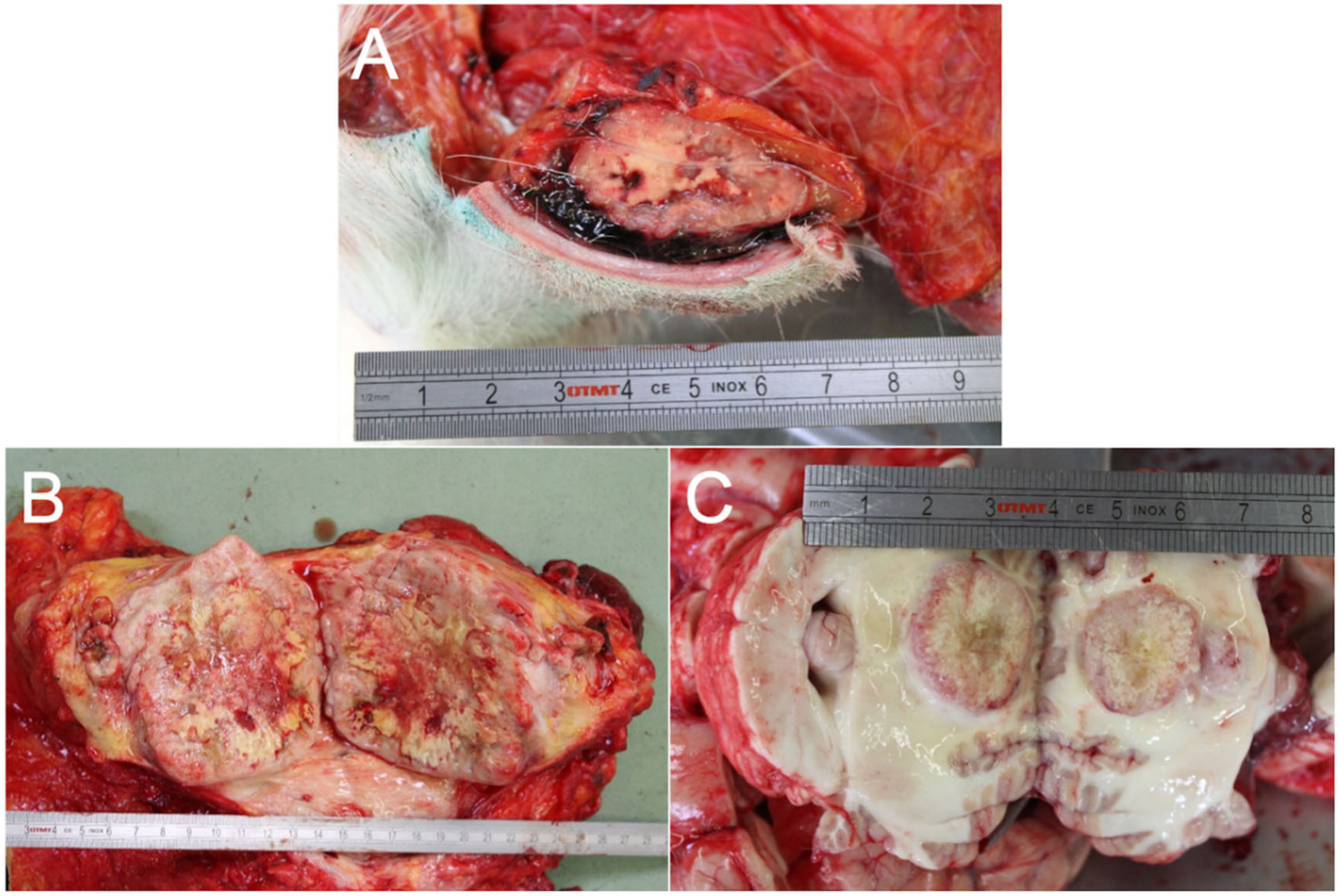
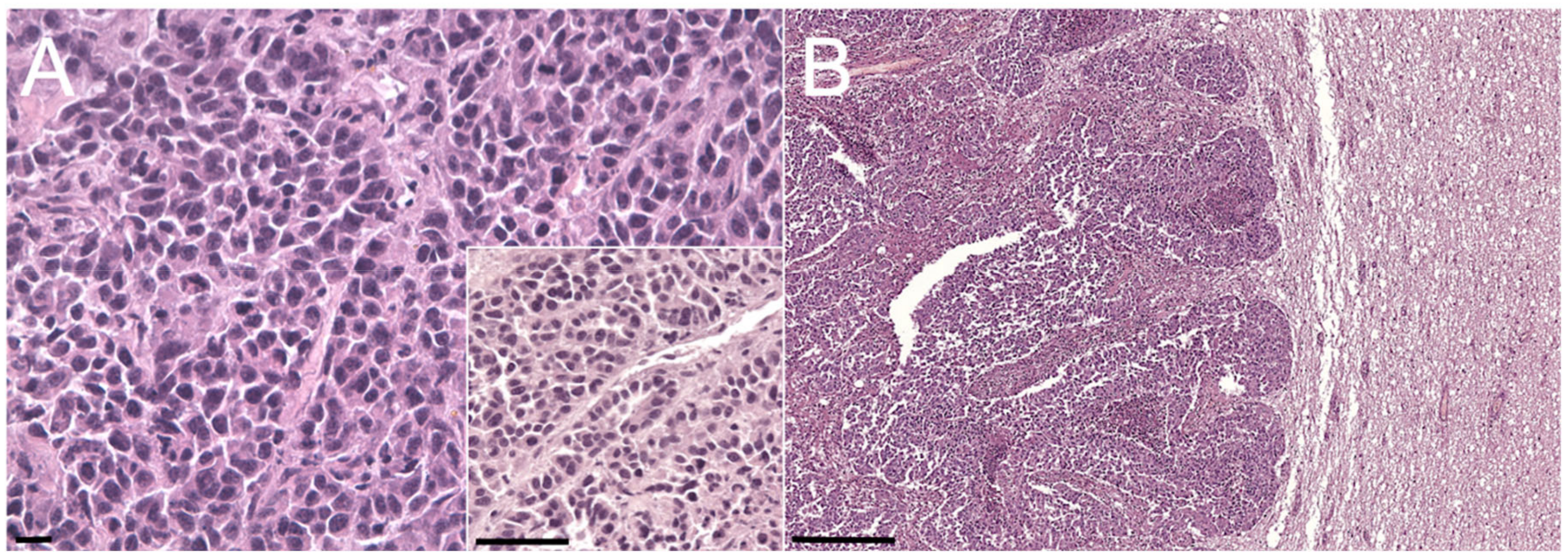
2.2. Post Mortem Examinations
3. Discussion
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Jena, A.; Patnayak, R.; Lakshmi, A.Y.; Manilal, B.; Reddy, M.K. Multiple primary cancers: An enigma. South Asian J. Cancer 2016, 5, 29–32. [Google Scholar] [CrossRef] [PubMed]
- Priester, W.A. Multiple primary tumors in domestic animals: A preliminary view with particular emphasis on tumors in dogs. Cancer 1977, 40, 1845–1848. [Google Scholar] [CrossRef]
- Veterinary Practice—Detecting Tumours in Horses. Available online: https://veterinary-practice.com/article/detecting-tumours-in-horses (accessed on 14 September 2020).
- Montgomery, K.W. Equine ocular neoplasia: A review. Equine Vet. Educ. 2014, 26, 372–380. [Google Scholar] [CrossRef]
- Goldschmidt, M.; Peña, L.; Rasotto, R.; Zappulli, V. Classification and grading of canine mammary tumors. Vet. Pathol. 2011, 48, 117–131. [Google Scholar] [CrossRef] [PubMed]
- Peña, L.; Gama, A.; Goldschmidt, M.H.; Abadie, J.; Benazzi, C.; Castagnaro, M.; Díez, L.; Gärtner, F.; Hellmén, E.; Kiupel, M.; et al. Canine mammary tumors: A review and consensus of standard guidelines on epithelial and myoepithelial phenotype markers, HER2, and hormone receptor assessment using immunohistochemistry. Vet. Pathol. 2014, 51, 127–145. [Google Scholar] [CrossRef]
- Acland, H.M.; Gillette, D.M. Mammary carcinoma in a mare. Vet. Pathol. 1982, 19, 93–95. [Google Scholar] [CrossRef]
- Gamba, C.O.; Araújo, M.R.; Palhares, M.S.; Garbin, L.C.; Maranhão, R.P.A.; Cassali, G.D.; Ecco, R. Invasive micropapillary carcinoma of the mammary glands in a mare. Vet. Q. 2011, 31, 207–210. [Google Scholar] [CrossRef]
- Hirayama, K.; Honda, Y.; Sako, T.; Okamoto, M.; Tsunoda, N.; Tagami, M.; Taniyama, H. Invasive ductal carcinoma of the mammary gland in a mare. Vet. Pathol. 2003, 40, 86–91. [Google Scholar] [CrossRef]
- Hughes, K.; Scase, T.J.; Foote, A.K. Estrogen receptor and signal transducer and activator of transcription 3 expression in equine mammary tumors. Vet. Pathol. 2015, 52, 631–634. [Google Scholar] [CrossRef]
- Feldmann, W.H. Malignant growths in domestic animals. J. Am. Vet. Med Assoc. 1929, 75, 192–200. [Google Scholar]
- Spadari, A.; Valentini, S.; Sarli, G.; Spinella, G.; Millanta, F.R. Mammary adenoma in a mare: Clinical, histopathological and immunohistochemical findings. Equine Vet. Educ. 2008, 20, 4–7. [Google Scholar] [CrossRef]
- Boyce, S.D.; Goodwin, S.L. Mammary gland neoplasia in a Canadian mare: Challenges of diagnosis and treatment in a rural setting. Can. Vet. J. 2017, 58, 628–630. [Google Scholar] [PubMed]
- Reppas, G.P. Papillary ductal adenocarcinoma in the mammary glands of two horses. Vet. Rec. 1999, 138, 518–519. [Google Scholar] [CrossRef] [PubMed]
- Shank, A.M. Mare mammary neoplasia: Difficulties in diagnosis and treatment. Equine Vet. Educ. 2009, 20, 475–477. [Google Scholar] [CrossRef]
- Munson, L. Carcinoma of the mammary gland in a mare. J. Am. Vet. Med. Assoc. 1987, 191, 71–72. [Google Scholar] [PubMed]
- Schmahl, V.W. Solides Karzinom der Mamma bei einem Pferd [Solid mammary carcinoma in a horse]. Berl. Munch. Tierarztl. Wochenschr. 1972, 85, 141–142. (In German) [Google Scholar]
- Seahorn, T.L.; Hall, G.; Brumbaugh, G.W.; Honnas, C.M.; Lovering, S.L.; Snyder, J.R. Mammary adenocarcinoma in four mares. J. Am. Vet. Med. Assoc. 1992, 200, 1675–1677. [Google Scholar]
- Foreman, J.H.; Weidner, J.P.; Parry, B.W.; Hargis, A. Pleural effusion secondary to thoracic metastatic mammary adenocarcinoma in a mare. J. Am. Vet. Med. Assoc. 1990, 197, 1193–1195. [Google Scholar]
- Prendergast, M.; Bassett, H.; Larkin, H.A. Mammary carcinoma in three mares. Vet. Rec. 1999, 144, 731–732. [Google Scholar] [CrossRef]
- Kato, M.; Higuchi, T.; Hata, H.; Ishikawa, Y.; Kadota, K. Lactalbumin-positive mammary carcinoma in a mare. Equine Vet. J. 1998, 30, 358–360. [Google Scholar] [CrossRef]
- Tomassini, L.; Pettinari, I.; Lepri, E.; Gialletti, R.; Bellezza, E.; Leonardi, L. A case of orbital extra-adrenal paraganglioma in a quarter horse. Braz. J. Vet. Pathol. 2019, 12, 53–57. [Google Scholar] [CrossRef]
- Komsta, R.; Lopuszynski, W. Multiple primary tumors in a dog. A case report. Bull. Vet. Inst. Pulawy 2008, 52, 481–484. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antibody | Features | Clone | Dilution | Localization | Tumor Positivity | Metastases Positivity | First Intraocular Mass | Second Intraocular Mass |
|---|---|---|---|---|---|---|---|---|
| PanCK | Dako® (Santa Clara, CA, USA) monoclonal | AE1/AE3 | 1:100 | Cytoplasm | 75% | 60% | 15–20% | 100% |
| mouse anti-human | (strong) | (strong) | (strong) | (strong) | ||||
| CK 14 | Novocastra® (Newcastle, UK) monoclonal | LL002 | 1:20 | Cytoplasm | negative | 10% | / | 30% |
| mouse anti-human | (strong) | (strong) | ||||||
| CK 5/6 | Dako® monoclonal | D5/16 B4 | 1:50 | Cytoplasm | 15% | 19% | / | 5% |
| mouse anti-human | (strong) | (strong) | (strong) | |||||
| p63 | GeneTex® (Irvine, CA, USA) polyclonal | N2C1 | 1:200 | Nucleus | negative | negative | / | negative |
| mouse anti-human | ||||||||
| Vimentin | Dako® monoclonal | V9 | 1:150 | Cytoplasm | stromal | 15–20% | 100% | |
| mouse anti-vimentin | (strong) | (strong) | ||||||
| Calponin | Dako® monoclonal | CALP | 1:200 | Cytoplasm | stromal | / | negative | |
| mouse anti-human | ||||||||
| ER | Novocastra® monoclonal | 6F11 | 1:40 | Cytoplasm | not cross-reactive | |||
| mouse anti-human | ||||||||
| PR | Ventana® (Tucson, AZ, USA) monoclonal rabbit anti-human | 1E2 | 1:80 | Nucleus | negative | 16% | / | negative |
| (mild) | ||||||||
| NSE | Dako® monoclonal | BBS/NC/VI-H14 | 1:250 | Cytoplasm | negative | 15–20% | 100% | |
| mouse anti-human | (strong) | (strong) | ||||||
| PNL2 | Santa Cruz Biotech® (Dallas, TX, USA) | sc-59306 | 1:100 | Cytoplasm | / | negative | / | |
| monoclonal | ||||||||
| mouse anti-human | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brocca, G.; Centelleghe, C.; Padoan, E.; Stoppini, R.; Giudice, C.; Castagnaro, M.; Zappulli, V. Case Report of a Mare Diagnosed with a Metastatic Mammary Carcinoma after the Excision of a Recurrent Intraocular Neuroepithelial Tumor. Animals 2020, 10, 2409. https://doi.org/10.3390/ani10122409
Brocca G, Centelleghe C, Padoan E, Stoppini R, Giudice C, Castagnaro M, Zappulli V. Case Report of a Mare Diagnosed with a Metastatic Mammary Carcinoma after the Excision of a Recurrent Intraocular Neuroepithelial Tumor. Animals. 2020; 10(12):2409. https://doi.org/10.3390/ani10122409
Chicago/Turabian StyleBrocca, Ginevra, Cinzia Centelleghe, Elisa Padoan, Riccardo Stoppini, Chiara Giudice, Massimo Castagnaro, and Valentina Zappulli. 2020. "Case Report of a Mare Diagnosed with a Metastatic Mammary Carcinoma after the Excision of a Recurrent Intraocular Neuroepithelial Tumor" Animals 10, no. 12: 2409. https://doi.org/10.3390/ani10122409
APA StyleBrocca, G., Centelleghe, C., Padoan, E., Stoppini, R., Giudice, C., Castagnaro, M., & Zappulli, V. (2020). Case Report of a Mare Diagnosed with a Metastatic Mammary Carcinoma after the Excision of a Recurrent Intraocular Neuroepithelial Tumor. Animals, 10(12), 2409. https://doi.org/10.3390/ani10122409