
Coxiella burnetii Femoro-Popliteal Bypass Infection: A Case Report

 ,
,
Abstract
1. Introduction
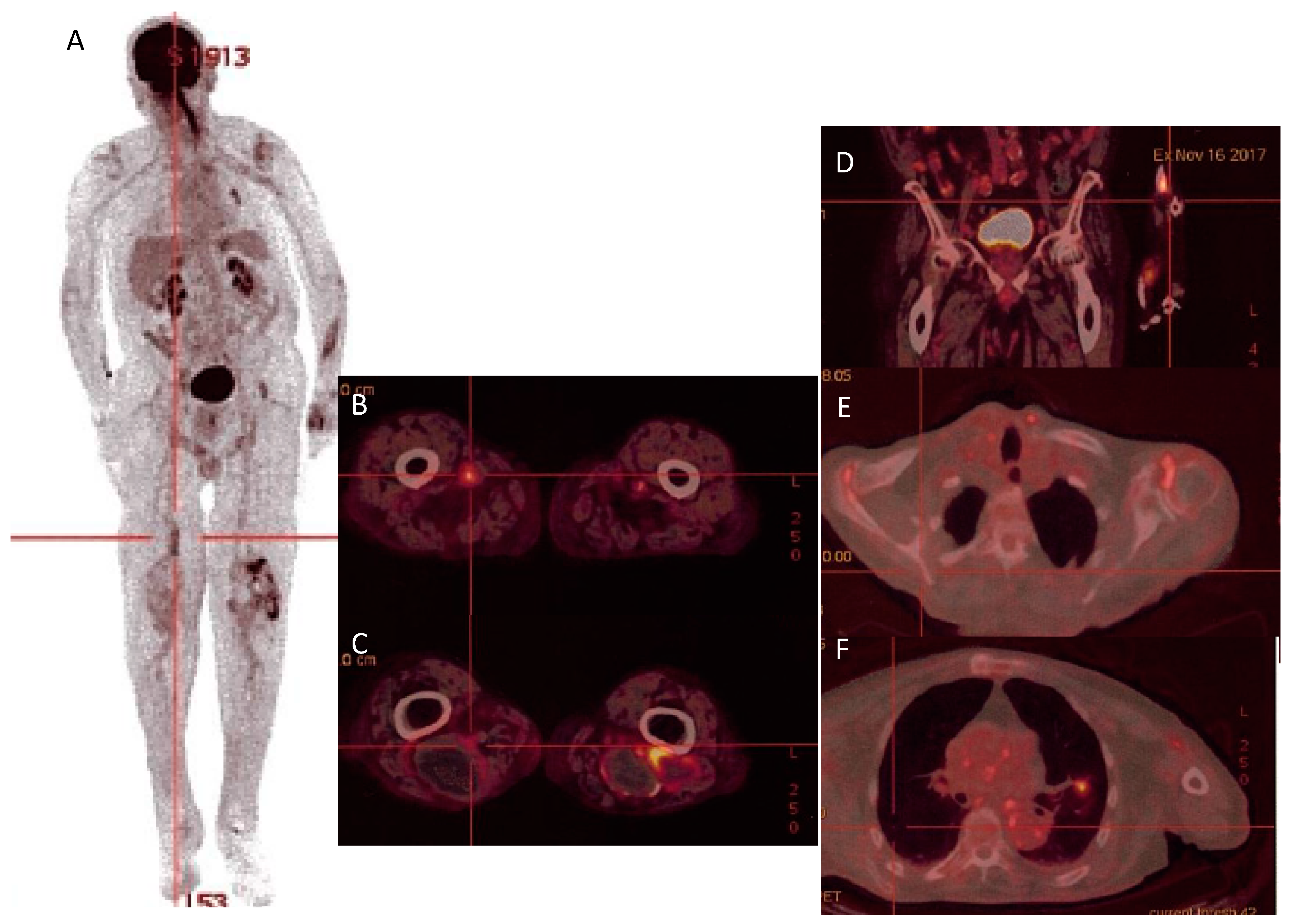
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Wegdam-Blans, M.; Vainas, T.; van Sambeek, M.R.; Cuypers, P.; Tjhie, H.; van Straten, A.; Teijink, J. Vascular Complications of Q-fever Infections. Eur. J. Vasc. Endovasc. Surg. 2011, 42, 384–392. [Google Scholar] [CrossRef] [PubMed]
- Maurin, M.; Raoult, D. Q Fever. Clin. Microbiol. Rev. 1999, 12, 518–553. [Google Scholar] [CrossRef]
- Million, M.; Walter, G.; Thuny, F.; Habib, G.; Raoult, D. Evolution from Acute Q Fever to Endocarditis Is Associated With Underlying Valvulopathy and Age and Can Be Prevented by Prolonged Antibiotic Treatment. Clin. Infect. Dis. 2013, 57, 836–844. [Google Scholar] [CrossRef] [PubMed]
- Fournier, P.; Casalta, J.; Piquet, P.; Tournigand, P.; Branchereau, A.; Raoult, D. Coxiella burnetii Infection of Aneurysms or Vascular Grafts: Report of Seven Cases and Review. Clin. Infect. Dis. 1998, 26, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Eldin, C.; Mélenotte, C.; Mediannikov, O.; Ghigo, E.; Million, M.; Edouard, S.; Mege, J.-L.; Maurin, M.; Raoult, D. From Q Fever to Coxiella burnetii Infection: A Paradigm Change. Clin. Microbiol. Rev. 2017, 30, 115–190. [Google Scholar] [CrossRef]
- Hamon, A.; El Sayed, F.; Bouchand, F.; Davido, B.; Duran, C.; Coggia, M.; Javerliat, I.; Dinh, A. Infection d’endoprothèse aortique à Coxiella burnetii. Med. Mal. Infect. 2020, 50, 620–623. [Google Scholar] [CrossRef]
- Senn, L.; Franciolli, M.; Raoult, D.; Moulin, A.; Von Segesser, L.; Calandra, T.; Greub, G. Coxiella burnetii vascular graft infection. BMC Infect. Dis. 2005, 5, 109. [Google Scholar] [CrossRef]
- O’Donnell, M.E.; Manshani, N.; McCaughey, C.; Soong, C.; Lee, B. Coxiella burnetii infection of an aortic graft with multiple vertebral body erosion. J. Vasc. Surg. 2007, 45, 399–403. [Google Scholar] [CrossRef]
- Merhej, V.; Cammilleri, S.; Piquet, P.; Casalta, J.-P.; Raoult, D. Relevance of the positron emission tomography in the diagnosis of vascular graft infection with Coxiella burnetii. Comp. Immunol. Microbiol. Infect. Dis. 2012, 35, 45–49. [Google Scholar] [CrossRef]
- Piquet, P.; Raoult, D.; Tranier, P.; Mercier, C. Coxiella burnetii infection of pseudoaneurysm of an aortic bypass graft with contiguous vertebral osteomyelitis. J. Vasc. Surg. 1994, 19, 165–168. [Google Scholar] [CrossRef]
- Dutasta, F.; Richaud, C.; Michon, A.; Ragone, E.; Podglajen, I.; Mainardi, J.-L. Use of 18F-FDG PET/CT for diagnosis of vascular graft infection with spread to sternum caused by Coxiella burnetii. Infect. Dis. 2016, 48, 769–771. [Google Scholar] [CrossRef] [PubMed]
- van Assen, S.; Houwerzijl, E.J.; van den Dungen, J.J.; Koopmans, K.-P. Vascular graft infection due to chronic Q fever diagnosed with fusion positron emission tomography/computed tomography. J. Vasc. Surg. 2007, 46, 372. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Stokes, W.; Janvier, J.; Vaughan, S. Chronic Q Fever in Alberta: A Case of Coxiella burnetii Mycotic Aneurysm and Concomitant Vertebral Osteomyelitis. Can. J. Infect. Dis. Med Microbiol. 2016, 2016, 7456157. [Google Scholar] [CrossRef]
- Waelbers, V.; Desmet, S.; De Munter, P.; Van Loon, J.; Fourneau, I. Vertebral Osteomyelitis or Infected Abdominal Aortic Endograft? A Rare Case of Q Fever. Ann. Vasc. Surg. 2020, 67, 568.e9–568.e12. [Google Scholar] [CrossRef]
- Kloppenburg, G.T.; van de Pavoordt, E.D.; de Vries, J.-P.P. Endograft-preserving therapy of a patient with Coxiella burnetii-infected abdominal aortic aneurysm: A case report. J. Med. Case Rep. 2011, 5, 565. [Google Scholar] [CrossRef] [PubMed]
- Wegdam-Blans, M.C.; ter Woorst, J.F.; Klompenhouwer, E.G.; Teijink, J.A. David procedure during a reoperation for ongoing chronic Q fever infection of an ascending aortic prosthesis. Eur. J. Cardio-Thoracic. Surg. 2012, 42, e19–e20. [Google Scholar] [CrossRef] [PubMed]
- Dvorak, S.; Bizzini, A. Streptococcus anginosus and Coxiella burnetii vascular graft co-infection. IDCases 2020, 19, e00697. [Google Scholar] [CrossRef] [PubMed]
- Vecchio, M.G.-D.; Vena, A.; Valerio, M.; Marin, M.; Verde, E.; Muñóz, P.; Bouza, E. Coxiella burnetii Infection in Hemodialysis and Other Vascular Grafts. Medicine 2014, 93, 364–371, Correction in Medicine 2014, 93, 414. [Google Scholar] [CrossRef]
- Ernest, V.; Cammilleri, S.; Amabile, P.; Fedi, M.; Burtey, S.; Von Kotze, C.; Pelletier, M.; Moal, V.; Guedj, E.; Perron, C.; et al. Hemodialysis vascular graft as a focus of persistent Q fever. Infection 2018, 46, 881–884. [Google Scholar] [CrossRef] [PubMed]
- Hagenaars, J.C.; Wever, P.C.; van Petersen, A.S.; Lestrade, P.J.; de Jager-Leclercq, M.G.; Hermans, M.H.; Moll, F.L.; Koning, O.H.; Renders, N.H. Estimated prevalence of chronic Q fever among Coxiella burnetii seropositive patients with an abdominal aortic/iliac aneurysm or aorto-iliac reconstruction after a large Dutch Q fever outbreak. J. Infect. 2014, 69, 154–160. [Google Scholar] [CrossRef]
- Melenotte, C.; Protopopescu, C.; Million, M.; Edouard, S.; Carrieri, M.P.; Eldin, C.; Angelakis, E.; Djossou, F.; Bardin, N.; Fournier, P.-E.; et al. Clinical Features and Complications of Coxiella burnetii Infections from the French National Reference Center for Q Fever. JAMA Netw. Open 2018, 1, e181580. [Google Scholar] [CrossRef] [PubMed]
- Million, M.; Raoult, D. Recent advances in the study of Q fever epidemiology, diagnosis and management. J. Infect. 2015, 71 (Suppl. 1), S2–S9. [Google Scholar] [CrossRef] [PubMed]
- Fenollar, F.; Fournier, P.; Carrieri, M.P.; Habib, G.; Messana, T.; Raoult, D. Risks Factors and Prevention of Q Fever Endocarditis. Clin. Infect. Dis. 2001, 33, 312–316. [Google Scholar] [CrossRef] [PubMed]
- Eldin, C.; Mailhe, M.; Lions, C.; Carrieri, P.; Safi, H.; Brouqui, P.; Raoult, D. Treatment and Prophylactic Strategy for Coxiella burnetii Infection of Aneurysms and Vascular Grafts: A Retrospective Cohort Study. Medicine 2016, 95, e2810. [Google Scholar] [CrossRef]
- Kampschreur, L.M.; Delsing, C.E.; Groenwold, R.H.H.; Wegdam-Blans, M.C.A.; Bleeker-Rovers, C.P.; de Jager-Leclercq, M.G.L.; Hoepelman, A.I.M.; van Kasteren, M.E.; Buijs, J.; Renders, N.H.M.; et al. Chronic Q Fever in the Netherlands 5 Years after the Start of the Q Fever Epidemic: Results from the Dutch Chronic Q Fever Database. J. Clin. Microbiol. 2014, 52, 1637–1643. [Google Scholar] [CrossRef]
- Botelho-Nevers, E.; Fournier, P.-E.; Richet, H.; Fenollar, F.; Lepidi, H.; Foucault, C.; Branchereau, A.; Piquet, P.; Maurin, M.; Raoult, D. Coxiella burnetii infection of aortic aneurysms or vascular grafts: Report of 30 new cases and evaluation of outcome. Eur. J. Clin. Microbiol. Infect. Dis. 2007, 26, 635–640. [Google Scholar] [CrossRef]
- Million, M.; Thuny, F.; Richet, H.; Raoult, D. Long-term outcome of Q fever endocarditis: A 26-year personal survey. Lancet Infect. Dis. 2010, 10, 527–535. [Google Scholar] [CrossRef]
- Frankel, D.; Richet, H.; Renvoisé, A.; Raoult, D. Q Fever in France, 1985–2009—Volume 17, Number 3—March 2011—Emerging Infectious Diseases Journal—CDC. Available online: https://wwwnc.cdc.gov/eid/article/17/3/10-0882_article (accessed on 12 July 2023).
- Prudent, E.; Lepidi, H.; Angelakis, E.; Raoult, D. Fluorescence In Situ Hybridization (FISH) and Peptide Nucleic Acid Probe-Based FISH for Diagnosis of Q Fever Endocarditis and Vascular Infections. J. Clin. Microbiol. 2018, 56, e00542-18. [Google Scholar] [CrossRef]
- Melenotte, C.; Million, M.; Raoult, D. New insights in Coxiella burnetii infection: Diagnosis and therapeutic update. Expert Rev. Anti-Infect. Ther. 2020, 18, 75–86. [Google Scholar] [CrossRef]
- Hagenaars, J.C.; Wever, P.C.; Vlake, A.W.; Renders, N.H.M.; Van Petersen, A.S.; Hilbink, M.; De Jager-Leclercq, M.G.L.; Moll, F.L.; Koning, O.H.J.; Hoekstra, C.J. Value of 18F-FDG PET/CT in diagnosing chronic Q fever in patients with central vascular disease. Neth. J. Med. 2016, 74, 301–308. [Google Scholar]
- Eldin, C.; Melenotte, C.; Million, M.; Cammilleri, S.; Sotto, A.; Elsendoorn, A.; Thuny, F.; Lepidi, H.; Roblot, F.; Weitten, T.; et al. 18F-FDG PET/CT as a central tool in the shift from chronic Q fever to Coxiella burnetii persistent focalized infection: A consecutive case series. Medicine 2016, 95, e4287. [Google Scholar] [CrossRef]
- Melenotte, C.; Million, M.; Hartung, O.; Botelho-Nevers, E.; Claudel, M.; Craighero, F.; Brouqui, P.; Raoult, D. Query rectal bleeding. Lancet 2012, 380, 446. [Google Scholar] [CrossRef]
- Melenotte, C.; Million, M.; Audoly, G.; Gorse, A.; Dutronc, H.; Roland, G.; Dekel, M.; Moreno, A.; Cammilleri, S.; Carrieri, M.P.; et al. B-cell non-Hodgkin lymphoma linked to Coxiella burnetii. Blood 2016, 127, 113–121. [Google Scholar] [CrossRef]
- van de Weijer, M.A.; Kruse, R.R.; Schamp, K.; Zeebregts, C.J.; Reijnen, M.M. Morbidity of femoropopliteal bypass surgery. Semin. Vasc. Surg. 2015, 28, 112–121. [Google Scholar] [CrossRef] [PubMed]
- Szilagyi, D.E.; Smith, R.F.; Elliott, J.P.; Vrandecic, M.P. Infection in Arterial Reconstruction with Synthetic Grafts. Ann. Surg. 1972, 176, 321–323. [Google Scholar] [CrossRef]
- Mege, J.-L.; Maurin, M.; Capo, C.; Raoult, D. Coxiella burnetii: The ‘query’ fever bacterium: A model of immune subversion by a strictly intracellular microorganism. FEMS Microbiol. Rev. 1997, 19, 209–217. [Google Scholar] [CrossRef]
- Raoult, D.; Marrie, T.; Mege, J. Natural history and pathophysiology of Q fever. Lancet Infect. Dis. 2005, 5, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Revest, M.; Camou, F.; Senneville, E.; Caillon, J.; Laurent, F.; Calvet, B.; Feugier, P.; Batt, M.; Chidiac, C. Medical treatment of prosthetic vascular graft infections: Review of the literature and proposals of a Working Group. Int. J. Antimicrob. Agents 2015, 46, 254–265. [Google Scholar] [CrossRef] [PubMed]
- Mandell, J.B.; Orr, S.; Koch, J.; Nourie, B.; Ma, D.; Bonar, D.D.; Shah, N.; Urish, K.L. Large variations in clinical antibiotic activity against Staphylococcus aureus biofilms of periprosthetic joint infection isolates. J. Orthop. Res. 2019, 37, 1604–1609. [Google Scholar] [CrossRef]
- van Asseldonk, M.; Prins, J.; Bergevoet, R. Economic assessment of Q fever in the Netherlands. Prev. Vet. Med. 2013, 112, 27–34. [Google Scholar] [CrossRef]
- Rahaman, R.; Milazzo, A.; Marshall, H.; Bi, P. Is a One Health Approach Utilized for Q Fever Control? A Comprehensive Literature Review. Int. J. Environ. Res. Public Health 2019, 16, 730. [Google Scholar] [CrossRef] [PubMed]
- Espí, A.; del Cerro, A.; Oleaga, Á.; Rodríguez-Pérez, M.; López, C.M.; Hurtado, A.; Rodríguez-Martínez, L.D.; Barandika, J.F.; García-Pérez, A.L. One Health Approach: An Overview of Q Fever in Livestock, Wildlife and Humans in Asturias (Northwestern Spain). Animals 2021, 11, 1395. [Google Scholar] [CrossRef] [PubMed]
- Million, M.; Walter, G.; Bardin, N.; Camoin, L.; Giorgi, R.; Bongrand, P.; Gouriet, F.; Casalta, J.-P.; Thuny, F.; Habib, G.; et al. Immunoglobulin G Anticardiolipin Antibodies and Progression to Q Fever Endocarditis. Clin. Infect. Dis. 2013, 57, 57–64. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Cases | Sex/Age | C. burnetii Infection Documentation (Serology, PCR, Culture…) | Vascular Infection Localization (Imaging Tool) | Treatment (Antibiotherapy and Surgery) | Outcome (at Time of Publication) | Country/Ref |
|---|---|---|---|---|---|---|
| Aortic vascular prosthesis infection | ||||||
| 1 | Man/78 years old | -Serology (IF 1) Phase I: IgG: 1:25,600, IgM: 1:400, Phase II IgG: 1:25,600, IgM: 1:400. -Positive PCR on serum | Abdominal under-renal aortic graft (TDM, PET-scan) | -DH 2 for 18 months -Surgery after 3 months | Recovery (three years follow-up) | France [6] |
| 2 | Man/63 years old | -Positive 16S rRNA PCR + sequencing on fragment of the para-iliac mass -Serology (IF) IgGI: 1:1,600, IgGII: 1:3,200 | Dacron aorto-bifemoral graft (CT-scan) | -partial removal of the prosthetic graft -DH | after 18 months: -Asymptomatic -IgG I:1600 and IgGII: 3200 | Switzerland [7] |
| 3 | Man/66 years old | -Complement Fixation Assay: CFT phase I antibody Titer: 1:1,280; CFT phase II antibody titer: 1:1,280 | Aorto-bifemoral bypass (MRI, CT-scan) | -oral doxycycline (200 mg/d) and ciprofloxacin (1000 mg/d) -graft excision | Recovery (21 months follow-up) | United Kingdom [8] |
| 4 | Man/70 years old | -Serology (IF) IgGI: 1:25,600; IgAI: 1:3200; IgGII: 1:51,200; IgAII: 1:6,400 -Positive real-time PCR (IS30a sequence) on a fragment of the aortic mass and the puncture liquid | Aortobiiliac endoprosthesis (CT-scan, PET-scan) | -DH -surgery three months later | Recovery (six months follow-up) | France [9] |
| 5 | Man/67 years old | -Serology (IF) IgGI: 1:800, IgMI: 0, IgAI: 1:800, IgGII: 1:1,600, IgMII: 0, IgAII: 1:800 -Positive aortic graft culture | Pseudoaneurysm of an aortic graft (CT-scan, MRI) | Doxycycline 200 mg/day and ofloxacine 600 mg/day Surgical excision of the aortic graft three weeks later | Recovery (three years follow-up) | France [10] |
| 6 | Man/46 years old | -Serology: IgGI: 1:51,200, IgMI: 1:25, IgAI: 1:200, IgGII: 1:102,400, IgMII: 1:50, IgAII: 1:400 -Positive specific PCR in sternal effusion | Aortic vascular graft (Bentall) (CT-scan, PET-scan) | DH | Recovery (21 months follow-up) | France [11] |
| 7 | Man/58 years old | Serology IgGI: 1:10,000 | Abdominal aortic prosthetic graft (FDG-PET-scan) | Antibiotics (not detailed) Surgical graft removal | Recovery (9 months follow-up) | The Netherlands [12] |
| 8 | Man/67 years old | -Serology IgGI: 1:2,048, IgGII: 1:1,024, IgM: 0 -Positive PCR on vascular tissue (post mortem) | Perirenal abdominal aortic graft (CT angiogram, MRI) | DH Surgical repair of abdominal aortic aneurysm and bilateral renal artery reconstruction | Died from acute pulmonary embolism 22 months since admission | Canada [13] |
| 9 | Woman/69 years old | -Positive panbacterial PCR on interlaminar L3-L4 biopsy and purulent fluid. -Serology: IgGI: 1:4,096, IgMI > 1:2,048 IgGII: 1:16,348, IgMII: 1:1,024 | Aortic endoprosthesis (CT-scan, MRI, PET-scan) | DH Aortic endoprosthesis removal | Recovery (5 months follow-up) | Belgium [14] |
| 10 | Man/62 years old | -Positive specific PCR on blood, thrombus and tissue culture -Serology IgGI: 1:2,048, IgGII: 1:4,096 | Infrarenal aortic bifurcated endograft (CT-scan) | Doxycycline 200 mg/day and cirprofloxacin 1500 mg/day abdominal wall of aneurysmal sac (including abscesses) removal endograft left in place | Recovery (six months follow-up) | The Netherlands [15] |
| 11 | Woman/55 years old | -Serology IgGI: 1:4,096, IgII: 1:4,096 -Positive specific PCR on blood, fluid material and prosthesis | Supracoronary tube graft repair of the ascending thoracic aorta (CT-scan, FDG PET-scan) | DH One year later (non-responsiveness to conservative treatment), aortic graft removal + Moxifloxacin | Recovery (six months follow-up) | The Netherlands [16] |
| 12 | Man/71 years old | -Serology IgGI: 1:8,192, IgGII: 1:8,192 -Positive specific real-time PCR on graft material | Aorto-bi-iliac graft (PET-scan) | DH Graft replacement and cure of the false aneurysm | Not mentioned | Switzerland [17] |
| Non-aortic vascular prosthesis infection | ||||||
| 13 | Man/61 years old | -Serology Phase I: IgG: 1:6,400, IgM: 1:50, IgA: 0 Phase II: IgG: 1:6,400, IgM: 0, IgAII: 0 -Positive 16S rRNA PCR+ sequencing and positive specific PCR (real-time PCR of the regions IS1111 and IS630) on periprosthetic biopsies and vascular arteriovenous grafts | Left humeral-axillary arteriovenous graft (CT-scan with tagged white blood cells of the left arm) | -DH -Surgery: partial removal of the infected prosthetic AV grafts | Recovery (undergoing treatment) | Spain [18] |
| 14 | Woman/50 years old | -Serology (IF) IgGI: 1:3,200, IgAI: 1:1,400, IgMI: 0 IgGII: 1:1,600, IgAII: 1:1,400, IgMII: 0 -Positive 16S rRNA PCR in the prosthetic valvular material -Positive specific PCR of the regions IS1111 and IS30a in the blood and vascular graft | Hemodialysis vascular graft (PET-scan) | Complete surgical removal of the infected vascular graft DH | Recovery (three months follow-up) | France [19] |
| 15 | Man/81 years old | -Serology (IF) IgGI: 1:800, IgMI: 0, IgAI: 1:100 IgGII: 1:200, IgMII: 0, IgAII: 0. | Femoro-popliteal bypass (PET-scan) | DH | -Clinical improvement -multiple hypermetabolisc foci persistence | Our case |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Azouzi, F.; Olagne, L.; Edouard, S.; Cammilleri, S.; Magnan, P.-E.; Fournier, P.-E.; Million, M. Coxiella burnetii Femoro-Popliteal Bypass Infection: A Case Report. Microorganisms 2023, 11, 2146. https://doi.org/10.3390/microorganisms11092146
Azouzi F, Olagne L, Edouard S, Cammilleri S, Magnan P-E, Fournier P-E, Million M. Coxiella burnetii Femoro-Popliteal Bypass Infection: A Case Report. Microorganisms. 2023; 11(9):2146. https://doi.org/10.3390/microorganisms11092146
Chicago/Turabian StyleAzouzi, Farah, Louis Olagne, Sophie Edouard, Serge Cammilleri, Pierre-Edouard Magnan, Pierre-Edouard Fournier, and Matthieu Million. 2023. "Coxiella burnetii Femoro-Popliteal Bypass Infection: A Case Report" Microorganisms 11, no. 9: 2146. https://doi.org/10.3390/microorganisms11092146
APA StyleAzouzi, F., Olagne, L., Edouard, S., Cammilleri, S., Magnan, P.-E., Fournier, P.-E., & Million, M. (2023). Coxiella burnetii Femoro-Popliteal Bypass Infection: A Case Report. Microorganisms, 11(9), 2146. https://doi.org/10.3390/microorganisms11092146