

Association between Helicobacter pylori Infection and Nasal Polyps: A Systematic Review and Meta-Analysis

 , , , , , , and
, , , , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Eligibility Criteria
2.2. Information Sources and Search Strategy
2.3. Data Extraction and Quality Assessment
2.4. Outcomes
2.5. Statistical Analysis and Data Synthesis
2.6. Quality of Evidence
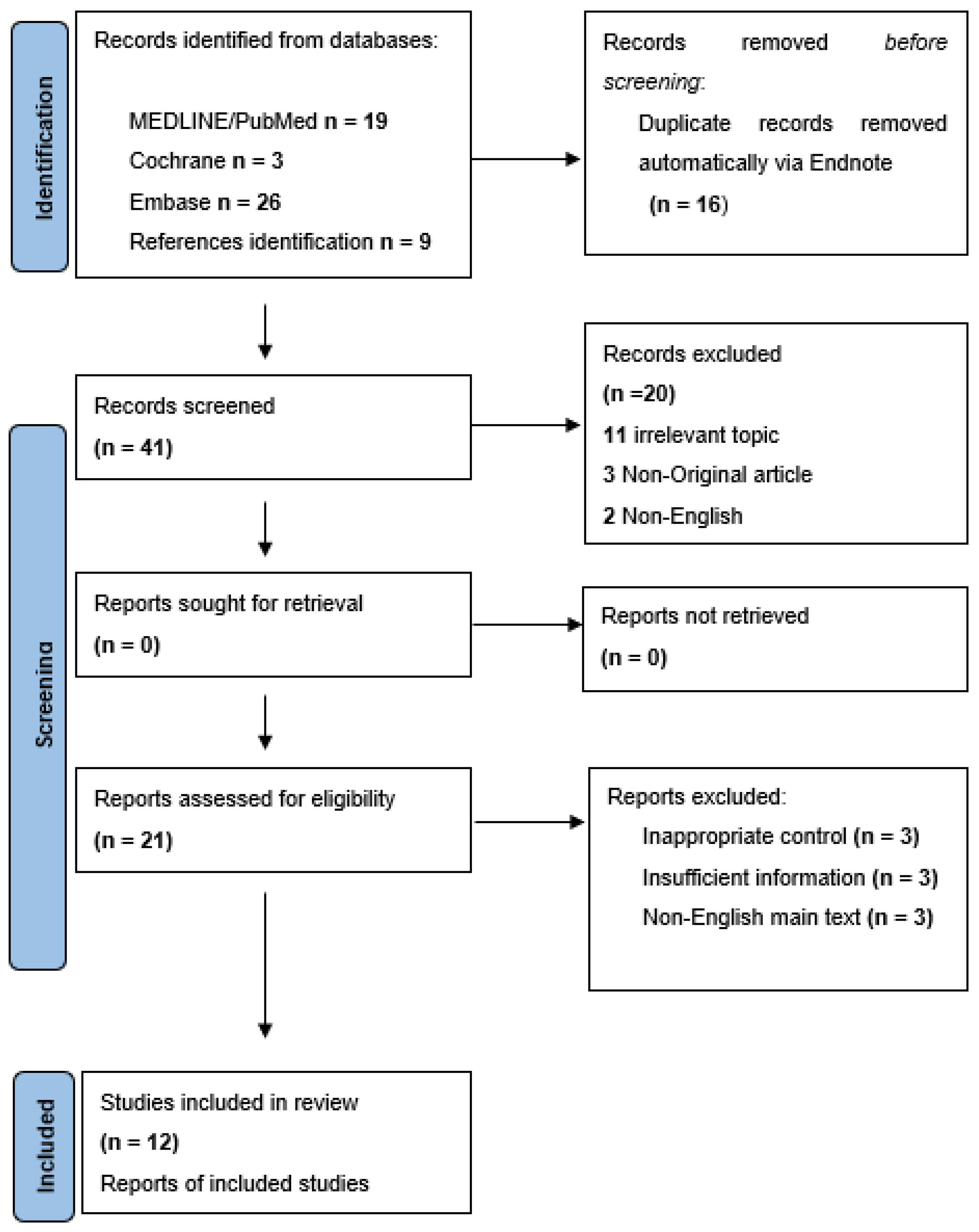
3. Results
3.1. Characteristics of Included Studies
3.2. Quality Assessment
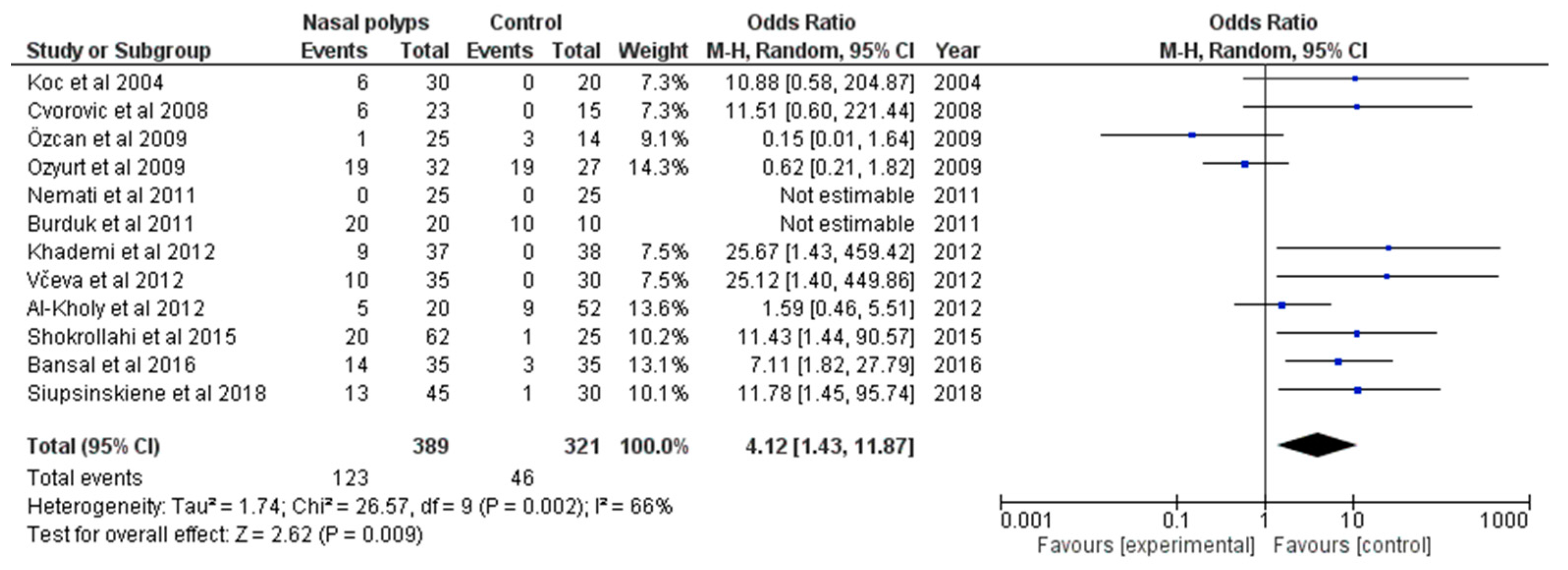
3.3. Primary Outcome
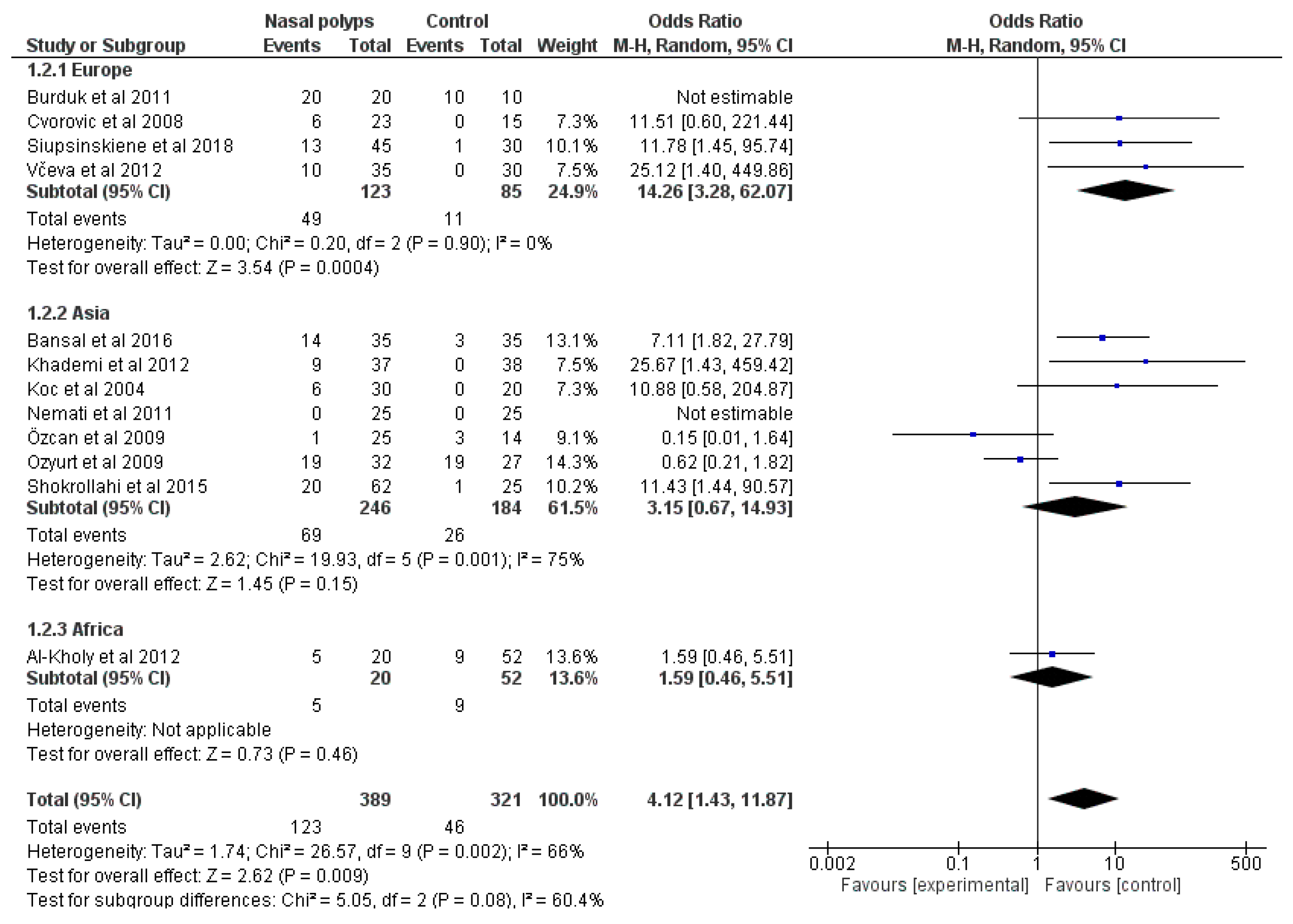
3.4. Subgroup Analysis
3.5. Quality of Evidence
3.6. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Doulberis, M.; Srivastava, S.; Polyzos, S.A.; Kountouras, J.; Papaefthymiou, A.; Klukowska-Rotzler, J.; Blank, A.; Exadaktylos, A.K.; Srivastava, D.S. Active Helicobacter pylori Infection is Independently Associated with Nonalcoholic Steatohepatitis in Morbidly Obese Patients. J. Clin. Med. 2020, 9, 933. [Google Scholar] [CrossRef] [PubMed]
- Kountouras, J.; Doulberis, M.; Polyzos, S.A.; Tzitiridou, M.; Chatzopoulos, D.; Gialamprinou, D.; Kotronis, G.; Vardaka, E.; Liatsos, C.; Papaefthymiou, A. A potential impact of Helicobacter pylori-related metabolic syndrome on early and long-term outcomes of bariatric surgery. Gastrointest. Endosc. 2022, 96, 1088–1089. [Google Scholar] [CrossRef] [PubMed]
- Malfertheiner, P.; Megraud, F.; Rokkas, T.; Gisbert, J.P.; Liou, J.M.; Schulz, C.; Gasbarrini, A.; Hunt, R.H.; Leja, M.; O’Morain, C.; et al. Management of Helicobacter pylori infection: The Maastricht VI/Florence consensus report. Gut 2022, 71, 1724–1762. [Google Scholar] [CrossRef] [PubMed]
- Doulberis, M.; Pierre, N.T.; Manzini, G.; Papaefthymiou, A.; Kountouras, J.; Klukowska-Rotzler, J.; Polyzos, S.A.; Srivastava, S.; Exadaktylos, A.K.; Knuchel, J.; et al. Helicobacter pylori-Related Metabolic Parameters and Premalignant Gastric Mucosa Histological Lesions in Swiss Bariatric Patients. Microorganisms 2021, 9, 1361. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Gravina, A.G.; Priadko, K.; Ciamarra, P.; Granata, L.; Facchiano, A.; Miranda, A.; Dallio, M.; Federico, A.; Romano, M. Extra-Gastric Manifestations of Helicobacter pylori Infection. J. Clin. Med. 2020, 9, 3887. [Google Scholar] [CrossRef]
- Rupp, S.; Papaefthymiou, A.; Chatzimichael, E.; Polyzos, S.A.; Spreitzer, S.; Doulberis, M.; Kuntzen, T.; Kountouras, J. Diagnostic approach to Helicobacter pylori-related gastric oncogenesis. Ann. Gastroenterol. 2022, 35, 333–344. [Google Scholar] [CrossRef]
- Doulberis, M.; Kotronis, G.; Thomann, R.; Polyzos, S.A.; Boziki, M.; Gialamprinou, D.; Deretzi, G.; Katsinelos, P.; Kountouras, J. Review: Impact of Helicobacter pylori on Alzheimer’s disease: What do we know so far? Helicobacter 2018, 23, e12454. [Google Scholar] [CrossRef]
- Kountouras, J.; Polyzos, S.A.; Katsinelos, P.; Zeglinas, C.; Artemaki, F.; Tzivras, D.; Vardaka, E.; Gavalas, E.; Romiopoulos, I.; Simeonidou, C.; et al. Cardio-cerebrovascular disease and Helicobacter pylori-related metabolic syndrome: We consider eradication therapy as a potential cardio-cerebrovascular prevention strategy. Int. J. Cardiol. 2017, 229, 17–18. [Google Scholar] [CrossRef]
- Kountouras, J.; Doulberis, M.; Polyzos, S.A.; Katsinelos, T.; Vardaka, E.; Kountouras, C.; Arapoglou, S.; Exadaktylos, A.K.; Deretzi, G.; Tsolaki, M.; et al. Impact of Helicobacter pylori and/or Helicobacter pylori-related metabolic syndrome on incidence of all-cause and Alzheimer’s dementia. Alzheimers Dement. 2019, 15, 723–725. [Google Scholar] [CrossRef]
- Kountouras, J.; Papaefthymiou, A.; Doulberis, M.; Polyzos, S.A. Influence of Helicobacter pylori-connected metabolic syndrome on non-alcoholic fatty liver disease and its related colorectal neoplasm high risk. Liver Int. 2020, 40, 475–476. [Google Scholar] [CrossRef]
- Kountouras, J.; Papaefthymiou, A.; Polyzos, S.A.; Liatsos, C.; Tzitiridou-Chatzopoulou, M.; Chatzopoulos, D.; Vardaka, E.; Gialambrinou, D.; Kotronis, G.; Doulberis, M. Potential impact of Helicobacter pylori and metabolic syndrome-related non-alcoholic fatty liver disease on cardio-cerebrovascular disease. Metabolism 2022, 135, 155276. [Google Scholar] [CrossRef]
- Zavos, C.; Kountouras, J.; Sakkias, G.; Venizelos, I.; Deretzi, G.; Arapoglou, S. Histological presence of Helicobacter pylori bacteria in the trabeculum and iris of patients with primary open-angle glaucoma. Ophthalmic Res. 2012, 47, 150–156. [Google Scholar] [CrossRef]
- Testerman, T.L.; Morris, J. Beyond the stomach: An updated view of Helicobacter pylori pathogenesis, diagnosis, and treatment. World J. Gastroenterol. 2014, 20, 12781–12808. [Google Scholar] [CrossRef]
- Doulberis, M.; Papaefthymiou, A.; Polyzos, S.A.; Bargiotas, P.; Liatsos, C.; Srivastava, D.S.; Zavos, C.; Katsinelos, P.; Kountouras, J. Association between Active Helicobacter pylori Infection and Glaucoma: A Systematic Review and Meta-Analysis. Microorganisms 2020, 8, 894. [Google Scholar] [CrossRef]
- Bansal, D.; Sharma, S.; Agarwal, S.; Saha, R.; Gupta, N. Detection of Helicobacter pylori in nasal polyps. Head Neck Pathol. 2016, 10, 306–313. [Google Scholar] [CrossRef]
- Kountouras, J.; Polyzos, S.A.; Doulberis, M.; Zeglinas, C.; Artemaki, F.; Vardaka, E.; Deretzi, G.; Giartza-Taxidou, E.; Tzivras, D.; Vlachaki, E.; et al. Potential impact of Helicobacter pylori-related metabolic syndrome on upper and lower gastrointestinal tract oncogenesis. Metabolism 2018, 87, 18–24. [Google Scholar] [CrossRef]
- Polyzos, S.A.; Zeglinas, C.; Artemaki, F.; Doulberis, M.; Kazakos, E.; Katsinelos, P.; Kountouras, J. Helicobacter pylori infection and esophageal adenocarcinoma: A review and a personal view. Ann. Gastroenterol. 2018, 31, 8–13. [Google Scholar] [CrossRef]
- Kountouras, J.; Doulberis, M.; Polyzos, S.A.; Zeglinas, C.; Vardaka, E.; Kountouras, C.; Tzivras, D.; Dardiotis, E.; Exadaktylos, A.; Katsinelos, P. Helicobacter pylori Infection and Gastroesophageal Reflux Disease-Barrett’s Esophagus-Esophageal Adenocarcinoma Sequence. Am. J. Gastroenterol. 2018, 113, 1723–1724. [Google Scholar] [CrossRef]
- Kountouras, J.; Zavos, C.; Chatzopoulos, D. The role of gastric Helicobacter pylori infection in laryngopharyngeal reflux disease. Otolaryngol. Head Neck Surg 2007, 136, 334. [Google Scholar] [CrossRef]
- Leason, S.R.; Barham, H.P.; Oakley, G.; Rimmer, J.; DelGaudio, J.M.; Christensen, J.M.; Sacks, R.; Harvey, R.J. Association of gastro-oesophageal reflux and chronic rhinosinusitis: Systematic review and meta-analysis. Rhinology 2017, 55, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Siupsinskiene, N.; Katutiene, I.; Jonikiene, V.; Janciauskas, D.; Vaitkus, S. Intranasal Helicobacter pylori infection in patients with chronic rhinosinusitis with polyposis. J. Laryngol. Otol. 2018, 132, 816–821. [Google Scholar] [CrossRef] [PubMed]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology 2020, 58, 1–464. [Google Scholar] [CrossRef] [PubMed]
- Van der Lans, R.J.L.; Hopkins, C.; Senior, B.A.; Lund, V.J.; Reitsma, S. Biologicals and Endoscopic Sinus Surgery for Severe Uncontrolled Chronic Rhinosinusitis with Nasal Polyps: An Economic Perspective. J. Allergy Clin. Immunol. Pract. 2022, 10, 1454–1461. [Google Scholar] [CrossRef]
- Včeva, A.; Đanić, D.; Včev, A.; Birtić, D.; Mihalj, H.; Zubčić, Ž.; Kotromanović, Ž.; Hadžibegović Đanić, A. The significance of Helicobacter pylori in patients with nasal polyposis. Med. Glas. 2012, 9, 281–286. [Google Scholar]
- Shokrollahi, M.R.; Tabatabaei, A.; Farhadi, M.; Noorbakhsh, S.; Movahedi, Z. Role of Helicobacter pylori in Nasal Polyp Formation: A Case-Control Study in Tehran, Iran. J. Otolaryngol. Adv. 2016, 1, 21–27. [Google Scholar] [CrossRef]
- Ozyurt, M.; Gungor, A.; Ergunay, K.; Cekin, E.; Erkul, E.; Haznedaroglu, T. Real-time PCR detection of Helicobacter pylori and virulence-associated cag A in nasal polyps and laryngeal disorders. Otolaryngol.-Head Neck Surg. 2009, 141, 131–135. [Google Scholar] [CrossRef]
- Özcan, C.; Polat, A.; Otağ, F.; Görür, K. Does Helicobacter pylori play a role in etiology of nasal polyposis? Auris Nasus Larynx 2009, 36, 427–430. [Google Scholar] [CrossRef]
- Nemati, S.; Mojtahedi, A.; Naghavi, S.E.; Banan, R.; Zia, F. Investigating Helicobacter pylori in nasal polyposis using polymerase chain reaction, urease test and culture. Eur. Arch. Oto-Rhino-Laryngol. 2012, 269, 1457–1461. [Google Scholar] [CrossRef]
- Morinaka, S.; Ichimiya, M.; Nakamura, H. Detection of Helicobacter pylori in nasal and maxillary sinus specimens from patients with chronic sinusitis. Laryngoscope 2003, 113, 1557–1563. [Google Scholar] [CrossRef]
- Koc, C.; Arikan, O.K.; Atasoy, P.; Aksoy, A. Prevalence of Helicobacter pylori in patients with nasal polyps: A preliminary report. Laryngoscope 2004, 114, 1941–1944. [Google Scholar] [CrossRef]
- Khajeh, F.; Motazedain, M.H.; Safarpoor, Z.; Meshkibaf, M.H.; Miladpoor, B. Prevalence of H. pylori in patients with nasal polyposis in Vali Asr hospital, Southern Iran. Iran. Red Crescent Med. J. 2011, 13, 436. [Google Scholar]
- Cvorovic, L.; Brajovic, D.; Strbac, M.; Milutinovic, Z.; Cvorovic, V. Detection of Helicobacter pylori in nasal polyps: Preliminary report. J. Otolaryngol.-Head Neck Surg. 2008, 37, 192–195. [Google Scholar]
- Khademi, B.; Kaviani, M.; Moosavi, S.A.; Pira, N.A.; Ashraf, M.J.; Chohedri, A.H. Helicobacter pylori in nasal polyposis. Prof. Med. J. 2012, 19, 455–461. [Google Scholar] [CrossRef]
- Al-Kholy, A.F.; Abadier, M.Z.; Hassaan, M.M.; Rageh, E.M.; Shindy, M.F. Screening for Helicobacter pylori Infection among Patients with Otorhinolaryngological Diseases May Spare Need for Surgical Interference: A PCR Confirmed Study. J. Am. Sci. 2012, 8, 83–88. [Google Scholar]
- Al-Abbasi, A.M.; Saeed, Z.K. Investigation of association of Helicobacter pylori and simple nasal polyps. Sudan J. Med. Sci. 2008, 3, 95–98. [Google Scholar] [CrossRef]
- Al-Abbasi, A.M.; Jasim, A.H. Association of Helicobacter pylori and Nasal polyposis. Iraqi Postgrad. Med. J. 2012, 11, 92–96. [Google Scholar]
- Sarhan, N.A.; Elhabashy, H.S.E. Frequency of H. pylori Infection among Patients with Varied Otorhinolaryngological Diseases: A PCR Controlled Study for Urea-Breath Test as A Screening Test. Tanta Med. J. 2009, 37, 927–934. [Google Scholar]
- Konstantinou, A.; Banos, G.; Sakelaridis, A. Helicobacter pylori Colonization in Nasal Polyps. Skull Base 2006, 16, A058. [Google Scholar] [CrossRef]
- Kaviani, M.; Khademi, B.; Mousavi, S.A.; Azarpira, N.; Ashraf, M.J. Detection of Helicobacter pylori in Nasal Polyps Using Rapid Urease Test and ELISA. Iran. J. Otorhinolaryngol. 2009, 20, 189–196. [Google Scholar]
- Čvorović, L.; Brajović, D.; Štrbac, M.; Burg, M.; Milutinović, Z.; Đukić, N.; Kiurski, M. Investigation of Helicobacter pylori colonization in nasal polyps. Mater. Med. 2004, 20, 11–14. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Booth, A.; Clarke, M.; Ghersi, D.; Moher, D.; Petticrew, M.; Stewart, L. An international registry of systematic-review protocols. Lancet 2011, 377, 108–109. [Google Scholar] [CrossRef] [PubMed]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Park, J.E.; Lee, Y.J.; Seo, H.J.; Sheen, S.S.; Hahn, S.; Jang, B.H.; Son, H.J. Testing a tool for assessing the risk of bias for nonrandomized studies showed moderate reliability and promising validity. J. Clin. Epidemiol. 2013, 66, 408–414. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Collaboration NCCTC. Review Manager (RevMan) [Computer Program], Version 5.3; The Nordic Cochrane Centre: Copenhagen, Denmark, 2014.
- Brozek, J.L.; Canelo-Aybar, C.; Akl, E.A.; Bowen, J.M.; Bucher, J.; Chiu, W.A.; Cronin, M.; Djulbegovic, B.; Falavigna, M.; Guyatt, G.H.; et al. GRADE Guidelines 30: The GRADE approach to assessing the certainty of modeled evidence-An overview in the context of health decision-making. J. Clin. Epidemiol. 2021, 129, 138–150. [Google Scholar] [CrossRef]
- Burduk, P.K.; Kaczmarek, A.; Budzynska, A.; Kazmierczak, W.; Gospodarek, E. Detection of Helicobacter pylori and cagA gene in nasal polyps and benign laryngeal diseases. Arch. Med. Res. 2011, 42, 686–689. [Google Scholar] [CrossRef]
- Jelavic, B.; Grgić, M.; Čupić, H.; Kordić, M.; Vasilj, M.; Baudoin, T. Prognostic value of Helicobacter pylori sinonasal colonization for efficacy of endoscopic sinus surgery. Eur. Arch. Oto-Rhino-Laryngol. 2012, 269, 2197–2202. [Google Scholar] [CrossRef]
- Hooi, J.K.Y.; Lai, W.Y.; Ng, W.K.; Suen, M.M.Y.; Underwood, F.E.; Tanyingoh, D.; Malfertheiner, P.; Graham, D.Y.; Wong, V.W.S.; Wu, J.C.Y.; et al. Global Prevalence of Helicobacter pylori Infection: Systematic Review and Meta-Analysis. Gastroenterology 2017, 153, 420–429. [Google Scholar] [CrossRef]
- Kaplan, M.; Tanoglu, A.; Duzenli, T.; Tozun, A.N. Helicobacter pylori treatment in Turkey: Current status and rational treatment options. North Clin. Istanb. 2020, 7, 87–94. [Google Scholar] [CrossRef]
- Ayas, M.; Gurol, Y. Antibiotic Resistance of Helicobacter pylori in Turkey: A Systematic Review and Meta-Analysis. Microb. Drug Resist 2023, 29, 96–103. [Google Scholar] [CrossRef]
- Sabbagh, P.; Mohammadnia-Afrouzi, M.; Javanian, M.; Babazadeh, A.; Koppolu, V.; Vasigala, V.R.; Nouri, H.R.; Ebrahimpour, S. Diagnostic methods for Helicobacter pylori infection: Ideals, options, and limitations. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 55–66. [Google Scholar] [CrossRef]
- Riba, A.K.; Ingeneri, T.J.; Strand, C.L. Improved Histologic Identification of Helicobacter pylori by Immunohistochemistry Using a New Novocastra Monoclonal Antibody. Lab. Med. 2011, 42, 35–39. [Google Scholar] [CrossRef]
- Shah, S.C.; Iyer, P.G.; Moss, S.F. AGA Clinical Practice Update on the Management of Refractory Helicobacter pylori Infection: Expert Review. Gastroenterology 2021, 160, 1831–1841. [Google Scholar] [CrossRef]
- Tutelyan, A.V.; Gaponov, A.M.; Pisarev, V.M.; El-Registan, G.I. Microbial dormancy and prevention of healthcare-associated infections. Ter. Arkh. 2015, 87, 103–108. [Google Scholar] [CrossRef]
- Reshetnyak, V.I.; Reshetnyak, T.M. Significance of dormant forms of Helicobacter pylori in ulcerogenesis. World J. Gastroenterol. 2017, 23, 4867–4878. [Google Scholar] [CrossRef]
- Ragab, S.M.; Lund, V.J.; Scadding, G. Evaluation of the medical and surgical treatment of chronic rhinosinusitis: A prospective, randomised, controlled trial. Laryngoscope 2004, 114, 923–930. [Google Scholar] [CrossRef]
- Anand, V.K. Epidemiology and economic impact of rhinosinusitis. Ann. Otol. Rhinol. Laryngol. Suppl. 2004, 193, 3–5. [Google Scholar] [CrossRef]
- Cho, S.H.; Hamilos, D.L.; Han, D.H.; Laidlaw, T.M. Phenotypes of Chronic Rhinosinusitis. J. Allergy Clin. Immunol. Pract. 2020, 8, 1505–1511. [Google Scholar] [CrossRef]
- Kucuksezer, U.C.; Ozdemir, C.; Akdis, M.; Akdis, C.A. Chronic rhinosinusitis: Pathogenesis, therapy options, and more. Expert Opin. Pharmacother. 2018, 19, 1805–1815. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Reitsma, S.; Wang, Y.; Fokkens, W.J. Highlights in the advances of chronic rhinosinusitis. Allergy 2021, 76, 3349–3358. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, N. The economic burden and symptom manifestations of chronic rhinosinusitis. Am. J. Rhinol. 2003, 17, 27–32. [Google Scholar] [CrossRef]
- Al Awady, M.K.; Alahmer, M.M.H.; El-Morsy, M.A.; Mostafa, O.M. Detection of Helicobacter pylori in paranasal sinus specimens from chronic rhinosinusitis patients. Al-Azhar Assiut Med. J. 2022, 20, 273. [Google Scholar] [CrossRef]
- Radenne, F.; Lamblin, C.; Vandezande, L.M.; Tillie-Leblond, I.; Darras, J.; Tonnel, A.B.; Wallaert, B. Quality of life in nasal polyposis. J. Allergy Clin. Immunol. 1999, 104, 79–84. [Google Scholar] [CrossRef]
- Diamantopoulos, I.I.; Jones, N.S.; Lowe, J. All nasal polyps need histological examination: An audit-based appraisal of clinical practice. J. Laryngol. Otol. 2000, 114, 755–759. [Google Scholar] [CrossRef]
- Dagli, M.; Eryilmaz, A.; Besler, T.; Akmansu, H.; Acar, A.; Korkmaz, H. Role of free radicals and antioxidants in nasal polyps. Laryngoscope 2004, 114, 1200–1203. [Google Scholar] [CrossRef]
- Cheng, Y.K.; Tsai, M.H.; Lin, C.D.; Hwang, G.Y.; Hang, L.W.; Tseng, G.C.; Shen, P.S.; Chang, W.C. Oxidative stress in nonallergic nasal polyps associated with bronchial hyperresponsiveness. Allergy 2006, 61, 1290–1298. [Google Scholar] [CrossRef]
- Tai, J.; Shin, J.M.; Park, J.; Han, M.; Kim, T.H. Oxidative Stress and Antioxidants in Chronic Rhinosinusitis with Nasal Polyps. Antioxidants 2023, 12, 195. [Google Scholar] [CrossRef]
- Karlidag, T.; Ilhan, N.; Kaygusuz, I.; Keles, E.; Yalcin, S.; Yildiz, M. Roles of free radicals, nitric oxide, and scavenging enzymes in nasal polyp development. Ann. Otol. Rhinol. Laryngol. 2005, 114, 122–126. [Google Scholar] [CrossRef]
- Kountouras, J.; Chatzopoulos, D.; Zavos, C. Reactive oxygen metabolites and upper gastrointestinal diseases. Hepatogastroenterology 2001, 48, 743–751. [Google Scholar]
- Papaefthymiou, A.; Doulberis, M.; Katsinelos, P.; Liatsos, C.; Polyzos, S.A.; Kotronis, G.; Papanikolaou, K.; Kountouras, J. Impact of nitric oxide’s bidirectional role on glaucoma: Focus on Helicobacter pylori-related nitrosative stress. Ann. N. Y. Acad. Sci. 2020, 1465, 10–28. [Google Scholar] [CrossRef]
- Ragab, A.E.; Al-Madboly, L.A.; Al-Ashmawy, G.M.; Saber-Ayad, M.; Abo-Saif, M.A. Unravelling the In Vitro and In Vivo Anti-Helicobacter pylori Effect of Delphinidin-3-O-Glucoside Rich Extract from Pomegranate Exocarp: Enhancing Autophagy and Downregulating TNF-alpha and COX2. Antioxidants 2022, 11, 1752. [Google Scholar] [CrossRef]
- Hong, Z.; Guo, Z.; Zhang, R.; Xu, J.; Dong, W.; Zhuang, G.; Deng, C. Airborne Fine Particulate Matter Induces Oxidative Stress and Inflammation in Human Nasal Epithelial Cells. Tohoku J. Exp. Med. 2016, 239, 117–125. [Google Scholar] [CrossRef]
- Laidlaw, T.M.; Buchheit, K.M. Biologics in chronic rhinosinusitis with nasal polyposis. Ann. Allergy Asthma Immunol. 2020, 124, 326–332. [Google Scholar] [CrossRef]
- Aria, H.; Kalani, M.; Hodjati, H.; Doroudchi, M. Different cytokine patterns induced by Helicobacter pylori and Lactobacillus acidophilus extracts in PBMCs of patients with abdominal aortic aneurysm. Comp. Immunol. Microbiol. Infect. Dis. 2020, 70, 101449. [Google Scholar] [CrossRef]
- Liutu, M.; Kalimo, K.; Kalimo, H.; Uksila, J.; Leino, R. Mast cells and IgE-containing cells in gastric mucosa of Helicobacter pylori infected and non-infected patients with chronic urticaria. J. Eur. Acad. Dermatol. Venereol. 2004, 18, 69–72. [Google Scholar] [CrossRef]
- Greaves, M. Chronic urticaria. J. Allergy Clin. Immunol. 2000, 105, 664–672. [Google Scholar] [CrossRef]
- Nettis, E.; Brussino, L.; Patella, V.; Bonzano, L.; Detoraki, A.; Di Leo, E.; Sirufo, M.M.; Caruso, C.; Lodi Rizzini, F.; Conte, M.; et al. Effectiveness and safety of dupilumab in patients with chronic rhinosinusitis with nasal polyps and associated comorbidities: A multicentric prospective study in real life. Clin. Mol. Allergy 2022, 20, 6. [Google Scholar] [CrossRef]
- Pawlowicz, R.; Wytrychowski, K.; Panaszek, B. Eradication of Helicobacter pylori, as add-on therapy, has a significant, but temporary influence on recovery in chronic idiopathic urticaria: A placebo-controlled, double blind trial in the Polish population. Postep. Dermatol. Alergol. 2018, 35, 151–155. [Google Scholar] [CrossRef]
- Kim, H.J.; Kim, Y.J.; Lee, H.J.; Hong, J.Y.; Park, A.Y.; Chung, E.H.; Lee, S.Y.; Lee, J.S.; Park, Y.L.; Lee, S.H.; et al. Systematic review and meta-analysis: Effect of Helicobacter pylori eradication on chronic spontaneous urticaria. Helicobacter 2019, 24, e12661. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Li, H.M.; Zhu, W.Q.; Li, Z. Role of Helicobacter pylori Eradication in Chronic Spontaneous Urticaria: A Propensity Score Matching Analysis. Clin. Cosmet. Investig. Dermatol. 2021, 14, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Elhendawy, M.; Hagras, M.M.; Soliman, S.S.; Shaker, E.S.E. Positive Effect of Helicobacter pylori Treatment on Outcome of Patients with Chronic Spontaneous Urticaria. Am. J. Clin. Pathol. 2021, 155, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Del Toro, E.; Portela, J. Nasal Polyps; National Library of Medicine: Bethesda, MD, USA, 2022. [Google Scholar]
- Doulberis, M.; Kountouras, J.; Rogler, G. Reconsidering the “protective” hypothesis of Helicobacter pylori infection in eosinophilic esophagitis. Ann. N. Y. Acad. Sci. 2020, 1481, 59–71. [Google Scholar] [CrossRef] [PubMed]
- Kapetanakis, N.; Kountouras, J.; Zavos, C.; Polyzos, S.A.; Venizelos, I.; Nikolaidou, C. Association of Helicobacter pylori infection with colorectal cancer. Immunogastroenterology 2013, 2, 47–56. [Google Scholar] [CrossRef]
- Kapetanakis, N.; Kountouras, J.; Zavos, C.; Polyzos, S.A.; Kouklakis, G.; Venizelos, I.; Nikolaidou, C.; Vardaka, E.; Paikos, D.; Katsinelos, P.; et al. Helicobacter pylori infection and colorectal carcinoma: Pathologic aspects. J. Gastrointest. Oncol. 2012, 3, 377–379. [Google Scholar] [CrossRef]
- Lu, D.; Wang, M.; Ke, X.; Wang, Q.; Wang, J.; Li, D.; Wang, M.; Wang, Q. Association between H. pylori Infection and Colorectal Polyps: A Meta-Analysis of Observational Studies. Front. Med. 2021, 8, 706036. [Google Scholar] [CrossRef]
- Yakoob, J.; Khan, M.R.; Abbas, Z.; Jafri, W.; Azmi, R.; Ahmad, Z.; Naeem, S.; Lubbad, L. Helicobacter pylori: Association with gall bladder disorders in Pakistan. Br. J. Biomed. Sci. 2011, 68, 59–64. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | Year | Country | Study Type | Study Period | Gender (Male, %) | Age of Cases (Mean ± SD/Median, Range) | Age of Controls (Mean ± SD/Median, Range) | Test for Gastric H. pylori Infection |
|---|---|---|---|---|---|---|---|---|
| [35] | 2012 | Εgypt | prospective case-control | 2010–2012 | 173 (59.2%) | 29.5 ± 15.4 | PCR | |
| [16] | 2016 | India | prospective case-control | 2011–2012 | 52 (74.3%) | 32 ± 11.0 | 28.2 ± 8.0 | IHC |
| [33] | 2008 | Serbia | prospective case-control | IHC | ||||
| [31] | 2004 | Turkey | prospective case-control | 2001–2003 | 17 (56.7%) | 41.5 (13–62) | 39.5 (25–58) | IHC |
| [28] | 2009 | Turkey | prospective case-control | 26 (66.6%) | 37.56 (19–69) | 31 (17–49) | CLO/IHC | |
| [27] | 2009 | Τurkey | prospective case-control | 2007–2008 | 28 (93.2%) | 34.48 (17–77) | 22.3 (19–28) | PCR |
| [26] | 2015 | Iran | prospective case-control | 2007–2008 | 55 (63.2%) | 37.5 ± 13.7 | 31 ± 11.5 | PCR |
| [22] | 2018 | Lithuania | prospective case-control | 2011–2012 | 29 (70.6%) | 51.8 ± 14.9 | 41.6 ± 17.6 | IHC |
| [25] | 2012 | Croatia | prospective case-control | 25 (71.4%) | 54 (27–78) | 42.5 (19–75) | PCR | |
| [34] | 2012 | Iran | prospective case-control | 2006–2008 | 52 (69.3%) | 41.27 (16–76) | 24.4 (17–59) | PCR/CLO |
| [49] | 2011 | Poland | prospective case-control | 19 (63.3%) | 48. 7 (23–71) | 43.3 (19–62) | PCR | |
| [29] | 2011 | Iran | prospective case-control | 2010 | 32.12 ± 14.08 | 24.36 ± 5.91 | PCR/CLO | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doulberis, M.; Kountouras, J.; Stadler, T.; Meerwein, C.; Polyzos, S.A.; Kulaksiz, H.; Chapman, M.H.; Rogler, G.; Riva, D.; Linas, I.; et al. Association between Helicobacter pylori Infection and Nasal Polyps: A Systematic Review and Meta-Analysis. Microorganisms 2023, 11, 1581. https://doi.org/10.3390/microorganisms11061581
Doulberis M, Kountouras J, Stadler T, Meerwein C, Polyzos SA, Kulaksiz H, Chapman MH, Rogler G, Riva D, Linas I, et al. Association between Helicobacter pylori Infection and Nasal Polyps: A Systematic Review and Meta-Analysis. Microorganisms. 2023; 11(6):1581. https://doi.org/10.3390/microorganisms11061581
Chicago/Turabian StyleDoulberis, Michael, Jannis Kountouras, Thomas Stadler, Christian Meerwein, Stergios A. Polyzos, Hasan Kulaksiz, Michael H. Chapman, Gerhard Rogler, Daniele Riva, Ioannis Linas, and et al. 2023. "Association between Helicobacter pylori Infection and Nasal Polyps: A Systematic Review and Meta-Analysis" Microorganisms 11, no. 6: 1581. https://doi.org/10.3390/microorganisms11061581
APA StyleDoulberis, M., Kountouras, J., Stadler, T., Meerwein, C., Polyzos, S. A., Kulaksiz, H., Chapman, M. H., Rogler, G., Riva, D., Linas, I., Kavaliotis, J., Kazakos, E., Mouratidou, M., Liatsos, C., & Papaefthymiou, A. (2023). Association between Helicobacter pylori Infection and Nasal Polyps: A Systematic Review and Meta-Analysis. Microorganisms, 11(6), 1581. https://doi.org/10.3390/microorganisms11061581