
High Incidence of Acute Liver Failure among Patients in Egypt Coinfected with Hepatitis A and Hepatitis E Viruses

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. HEV Diagnosis and Molecular Assessment of HAV and HEV Viruses
2.3. Sequencing of HAV and HEV in Patient Samples
2.4. Statistics
3. Results
3.1. Characteristics of HAV-Infected Patients Enrolled in the Study
3.2. The Prevalence of HEV Infection among HAV-Infected Patients and Characteristics of HAV–HEV Co-Infected Patients
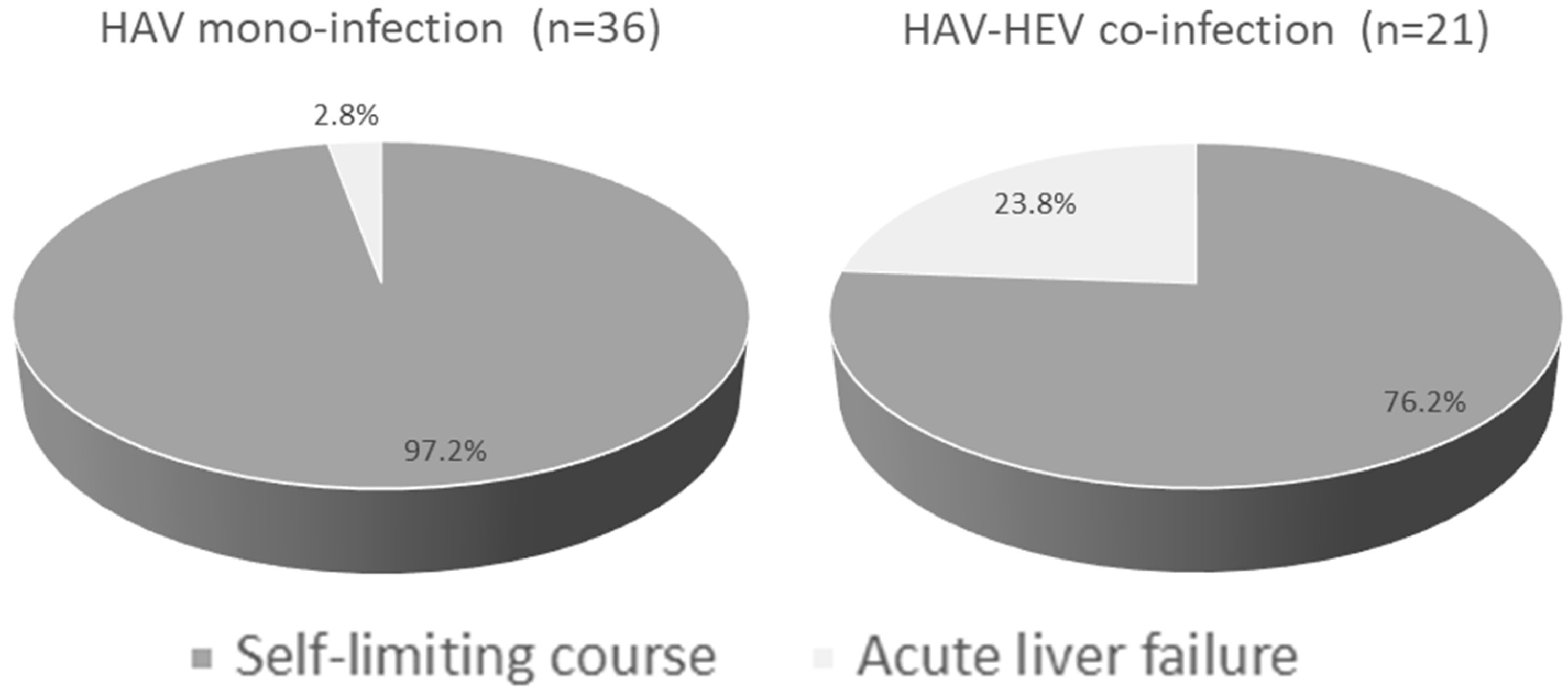
3.3. Outcomes of HAV Mono-Infection and HAV–HEV Co-Infections and Characteristics of ALF Cases in Both Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Elbahrawy, A.; Ibrahim, M.K.; Eliwa, A.; Alboraie, M.; Madian, A.; Aly, H.H. Current situation of viral hepatitis in Egypt. Microbiol. Immunol. 2021, 65, 352–372. [Google Scholar] [CrossRef] [PubMed]
- Talaat, M.; Afifi, S.; Reaves, E.J.; Abu Elsood, H.; El-Gohary, A.; Refaey, S.; Hammad, R.; Abdel Fadeel, M.; Kandeel, A. Evidence of sustained reductions in the relative risk of acute hepatitis B and C virus infections, and the increasing burden of hepatitis a virus infection in Egypt: Comparison of sentinel acute viral hepatitis surveillance results, 2001–2017. BMC Infect. Dis. 2019, 19, 159. [Google Scholar] [CrossRef] [PubMed]
- Sayed, I.M.; Abdelwahab, S.F. Is Hepatitis E Virus a Neglected or Emerging Pathogen in Egypt? Pathogens 2022, 11, 1337. [Google Scholar] [CrossRef] [PubMed]
- Das, A.; Hirai-Yuki, A.; González-López, O.; Rhein, B.; Moller-Tank, S.; Brouillette, R.; Hensley, L.; Misumi, I.; Lovell, W.; Cullen, J.M.; et al. TIM1 (HAVCR1) Is Not Essential for Cellular Entry of Either Quasi-enveloped or Naked Hepatitis A Virions. mBio 2017, 8, e00969-17. [Google Scholar] [CrossRef]
- Montpellier, C.; Wychowski, C.; Sayed, I.M.; Meunier, J.C.; Saliou, J.M.; Ankavay, M.; Bull, A.; Pillez, A.; Abravanel, F.; Helle, F.; et al. Hepatitis E Virus Lifecycle and Identification of 3 Forms of the ORF2 Capsid Protein. Gastroenterology 2018, 154, 211–223.e218. [Google Scholar] [CrossRef] [PubMed]
- Foster, M.A.; Hofmeister, M.G.; Kupronis, B.A.; Lin, Y.; Xia, G.L.; Yin, S.; Teshale, E. Increase in Hepatitis A Virus Infections–United States, 2013–2018. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 413–415. [Google Scholar] [CrossRef] [PubMed]
- Kaur, M.; Sidhu, S.K.; Singh, K.; Devi, P.; Kaur, M.; Singh, N.J. Hepatitis E virus: A leading cause of waterborne viral hepatitis in Northwest Districts of Punjab, India. J. Lab. Physicians 2017, 9, 121–124. [Google Scholar] [CrossRef]
- Sayed, I.M. Dual Infection of Hepatitis A Virus and Hepatitis E Virus-What Is Known? Viruses 2023, 15, 298. [Google Scholar] [CrossRef]
- De Serres, G.; Cromeans, T.L.; Levesque, B.; Brassard, N.; Barthe, C.; Dionne, M.; Prud’homme, H.; Paradis, D.; Shapiro, C.N.; Nainan, O.V.; et al. Molecular confirmation of hepatitis A virus from well water: Epidemiology and public health implications. J. Infect. Dis. 1999, 179, 37–43. [Google Scholar] [CrossRef]
- Di Cola, G.; Fantilli, A.C.; Pisano, M.B.; Ré, V.E. Foodborne transmission of hepatitis A and hepatitis E viruses: A literature review. Int. J. Food Microbiol. 2021, 338, 108986. [Google Scholar] [CrossRef]
- Bergeisen, G.H.; Hinds, M.W.; Skaggs, J.W. A waterborne outbreak of hepatitis A in Meade County, Kentucky. Am. J. Public Health 1985, 75, 161–164. [Google Scholar] [CrossRef] [PubMed]
- McKnight, K.L.; Lemon, S.M. Hepatitis A Virus Genome Organization and Replication Strategy. Cold Spring Harb. Perspect. Med. 2018, 8, a033480. [Google Scholar] [CrossRef] [PubMed]
- Tam, A.W.; Smith, M.M.; Guerra, M.E.; Huang, C.C.; Bradley, D.W.; Fry, K.E.; Reyes, G.R. Hepatitis E virus (HEV): Molecular cloning and sequencing of the full-length viral genome. Virology 1991, 185, 120–131. [Google Scholar] [CrossRef]
- Sayed, I.M.; Vercouter, A.S.; Abdelwahab, S.F.; Vercauteren, K.; Meuleman, P. Is hepatitis E virus an emerging problem in industrialized countries? Hepatology 2015, 62, 1883–1892. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.; Lemon, S.M. The molecular biology of hepatitis A virus. In Hepatitis Viruses; Springer: Berlin/Heidelberg, Germany, 2002; pp. 23–50. [Google Scholar]
- Cancela, F.; Noceti, O.; Arbiza, J.; Mirazo, S. Structural aspects of hepatitis E virus. Arch. Virol. 2022, 167, 2457–2481. [Google Scholar] [CrossRef]
- Arora, N.K.; Nanda, S.K.; Gulati, S.; Ansari, I.H.; Chawla, M.K.; Gupta, S.D.; Panda, S.K. Acute viral hepatitis types E, A, and B singly and in combination in acute liver failure in children in north India. J. Med. Virol. 1996, 48, 215–221. [Google Scholar] [CrossRef]
- Copado-Villagrana, E.D.; Anaya-Covarrubias, J.Y.; Viera-Segura, O.; Trujillo-Ochoa, J.L.; Panduro, A.; José-Abrego, A.; Roman, S.; Fierro, N.A. Spatial and Temporal Distribution of Hepatitis A Virus and Hepatitis E Virus among Children with Acute Hepatitis in Mexico. Viral Immunol. 2021, 34, 653–657. [Google Scholar] [CrossRef] [PubMed]
- Hyams, K.C.; McCarthy, M.C.; Kaur, M.; Purdy, M.A.; Bradley, D.W.; Mansour, M.M.; Gray, S.; Watts, D.M.; Carl, M. Acute sporadic hepatitis E in children living in Cairo, Egypt. J. Med. Virol. 1992, 37, 274–277. [Google Scholar] [CrossRef]
- García, C.G.; Sánchez, D.; Villalba, M.C.; Pujol, F.H.; de Los Ángeles Rodríguez Lay, L.; Pinto, B.; Chacón, E.P.; Guzmán, M.G. Molecular characterization of hepatitis E virus in patients with acute hepatitis in Venezuela. J. Med. Virol. 2012, 84, 1025–1029. [Google Scholar] [CrossRef]
- Spada, E.; Costantino, A.; Pezzotti, P.; Bruni, R.; Pisani, G.; Madonna, E.; Chionne, P.; Simeoni, M.; Villano, U.; Marcantonio, C.; et al. Hepatitis E virus infection prevalence among men who have sex with men involved in a hepatitis A virus outbreak in Italy. Blood Transfus. 2019, 17, 428–432. [Google Scholar] [CrossRef]
- Rodríguez-Tajes, S.; Perpiñán, E.; Leonel, T.; Lens, S.; Mariño, Z.; Pérez-Del-Pulgar, S.; García-López, M.; Pocurull, A.; Koutsoudakis, G.; Forns, X. Low seroprevalence and zero incidence rate of hepatitis E in men who have sex with men during a hepatitis A outbreak. J. Med. Virol. 2020, 92, 1359–1362. [Google Scholar] [CrossRef] [PubMed]
- Hofmeister, M.G.; Gupta, N. Preventable Deaths During Widespread Community Hepatitis A Outbreaks—United States, 2016–2022. MMWR Morb. Mortal. Wkly. Rep. 2023, 72, 1128–1133. [Google Scholar] [CrossRef] [PubMed]
- Kunanitthaworn, N.; Mueangmo, O.; Saheng, J.; Wongjak, W.; Lertsiriladakul, T.; Chaito, T.; Nantarat, P.; Sudjaritruk, T. Seroprevalence of hepatitis A virus antibodies among children and adolescents living in Northern Thailand: An implication for hepatitis A immunization. Sci. Rep. 2023, 13, 17432. [Google Scholar] [CrossRef] [PubMed]
- Fontana, S.; Ripellino, P.; Niederhauser, C.; Widmer, N.; Gowland, P.; Petrini, O.; Aprile, M.; Merlani, G.; Bihl, F. Epidemiology of HEV Infection in Blood Donors in Southern Switzerland. Microorganisms 2023, 11, 2375. [Google Scholar] [CrossRef] [PubMed]
- Politou, M.; Boti, S.; Androutsakos, T.; Valsami, S.; Pittaras, T.; Kapsimali, V. Seroprevalence of hepatitis E in HIV infected patients in Greece. J. Med. Virol. 2015, 87, 1517–1520. [Google Scholar] [CrossRef]
- Hasan, G.; Assiri, A.; Marzuuk, N.; Daef, E.; Abdelwahab, S.; Ahmed, A.; Mohamad, I.; Al-Eyadhy, A.; Alhaboob, A.; Temsah, M.H. Incidence and characteristics of hepatitis E virus infection in children in Assiut, Upper Egypt. J. Int. Med. Res. 2016, 44, 1115–1122. [Google Scholar] [CrossRef] [PubMed]
- Fouad, H.M.; Reyad, E.M.; El-Din, A.G. Acute hepatitis A is the chief etiology of acute hepatitis in Egyptian children: A single-center study. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 1941–1947. [Google Scholar] [CrossRef] [PubMed]
- Ramadan, H.K.; Sayed, I.M.; Elkhawaga, A.A.; Meghezel, E.M.; Askar, A.A.; Moussa, A.M.; Osman, A.; Elfadl, A.A.; Khalifa, W.A.; Ashmawy, A.M.; et al. Characteristics and outcomes of acute hepatitis of unknown etiology in Egypt: First report of adult adenovirus-associated hepatitis. Infection 2022, 51, 887–895. [Google Scholar] [CrossRef]
- EASL Clinical Practice Guidelines on hepatitis E virus infection. J. Hepatol. 2018, 68, 1256–1271. [CrossRef]
- Wendon, J.; Cordoba, J.; Dhawan, A.; Larsen, F.S.; Manns, M.; Samuel, D.; Simpson, K.J.; Yaron, I.; Bernardi, M. EASL Clinical Practical Guidelines on the management of acute (fulminant) liver failure. J. Hepatol. 2017, 66, 1047–1081. [Google Scholar] [CrossRef]
- Jothikumar, N.; Cromeans, T.L.; Sobsey, M.D.; Robertson, B.H. Development and evaluation of a broadly reactive TaqMan assay for rapid detection of hepatitis A virus. Appl. Environ. Microbiol. 2005, 71, 3359–3363. [Google Scholar] [CrossRef] [PubMed]
- Jothikumar, N.; Cromeans, T.L.; Robertson, B.H.; Meng, X.J.; Hill, V.R. A broadly reactive one-step real-time RT-PCR assay for rapid and sensitive detection of hepatitis E virus. J. Virol. Methods 2006, 131, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Probert, W.S.; Gonzalez, C.; Espinosa, A.; Hacker, J.K. Molecular Genotyping of Hepatitis A Virus, California, USA, 2017–2018. Emerg. Infect. Dis. 2019, 25, 1594–1596. [Google Scholar] [CrossRef]
- Hutin, Y.J.F.; Pool, V.; Cramer, E.H.; Nainan, O.V.; Weth, J.; Williams, I.T.; Goldstein, S.T.; Gensheimer, K.F.; Bell, B.P.; Shapiro, C.N.; et al. A Multistate, Foodborne Outbreak of Hepatitis A. N. Engl. J. Med. 1999, 340, 595–602. [Google Scholar] [CrossRef] [PubMed]
- Huang, F.F.; Haqshenas, G.; Guenette, D.K.; Halbur, P.G.; Schommer, S.K.; Pierson, F.W.; Toth, T.E.; Meng, X.J. Detection by reverse transcription-PCR and genetic characterization of field isolates of swine hepatitis E virus from pigs in different geographic regions of the United States. J. Clin. Microbiol. 2002, 40, 1326–1332. [Google Scholar] [CrossRef] [PubMed]
- El-Mokhtar, M.A.; Elkhawaga, A.A.; Sayed, I.M. Assessment of hepatitis E virus (HEV) in the edible goat products pointed out a risk for human infection in Upper Egypt. Int. J. Food Microbiol. 2020, 330, 108784. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.B.; Izopet, J.; Nicot, F.; Simmonds, P.; Jameel, S.; Meng, X.J.; Norder, H.; Okamoto, H.; van der Poel, W.H.M.; Reuter, G.; et al. Update: Proposed reference sequences for subtypes of hepatitis E virus (species Orthohepevirus A). J. Gen. Virol. 2020, 101, 692–698. [Google Scholar] [CrossRef]
- Smith, D.B.; Simmonds, P.; Izopet, J.; Oliveira-Filho, E.F.; Ulrich, R.G.; Johne, R.; Koenig, M.; Jameel, S.; Harrison, T.J.; Meng, X.J.; et al. Proposed reference sequences for hepatitis E virus subtypes. J. Gen. Virol. 2016, 97, 537–542. [Google Scholar] [CrossRef]
- Purdy, M.A.; Drexler, J.F.; Meng, X.J.; Norder, H.; Okamoto, H.; Van der Poel, W.H.M.; Reuter, G.; de Souza, W.M.; Ulrich, R.G.; Smith, D.B. ICTV Virus Taxonomy Profile: Hepeviridae 2022. J. Gen. Virol. 2022, 103, 001778. [Google Scholar] [CrossRef]
- Smith, D.B.; Simmonds, P.; Jameel, S.; Emerson, S.U.; Harrison, T.J.; Meng, X.J.; Okamoto, H.; Van der Poel, W.H.; Purdy, M.A. Consensus proposals for classification of the family Hepeviridae. J. Gen. Virol. 2015, 96, 1191–1192. [Google Scholar] [CrossRef]
- Barnaud, E.; Rogée, S.; Garry, P.; Rose, N.; Pavio, N. Thermal inactivation of infectious hepatitis E virus in experimentally contaminated food. Appl. Environ. Microbiol. 2012, 78, 5153–5159. [Google Scholar] [CrossRef] [PubMed]
- Doceul, V.; Bagdassarian, E.; Demange, A.; Pavio, N. Zoonotic Hepatitis E Virus: Classi fi cation, Animal Reservoirs and Transmission Routes. Viruses 2016, 8, 270. [Google Scholar] [CrossRef] [PubMed]
- Feagins, A.R.; Opriessnig, T.; Guenette, D.K.; Halbur, P.G.; Meng, X.J. Inactivation of infectious hepatitis E virus present in commercial pig livers sold in local grocery stores in the United States. Int. J. Food Microbiol. 2008, 123, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Battistini, R.; Rossini, I.; Listorti, V.; Ercolini, C.; Maurella, C.; Serracca, L. HAV detection from milk-based products containing soft fruits: Comparison between four different extraction methods. Int. J. Food Microbiol. 2020, 328, 108661. [Google Scholar] [CrossRef]
- Frank, C.; Walter, J.; Muehlen, M.; Jansen, A.; van Treeck, U.; Hauri, A.M.; Zoellner, I.; Rakha, M.; Hoehne, M.; Hamouda, O.; et al. Major outbreak of hepatitis A associated with orange juice among tourists, Egypt, 2004. Emerg. Infect. Dis. 2007, 13, 156–158. [Google Scholar] [CrossRef]
- Maunula, L.; Kaupke, A.; Vasickova, P.; Söderberg, K.; Kozyra, I.; Lazic, S.; van der Poel, W.H.; Bouwknegt, M.; Rutjes, S.; Willems, K.A.; et al. Tracing enteric viruses in the European berry fruit supply chain. Int. J. Food Microbiol. 2013, 167, 177–185. [Google Scholar] [CrossRef]
- Aboubakr, H.; Goyal, S. Involvement of Egyptian Foods in Foodborne Viral Illnesses: The Burden on Public Health and Related Environmental Risk Factors: An Overview. Food Environ. Virol. 2019, 11, 315–339. [Google Scholar] [CrossRef]
- Frank, C.; Walter, J.; Muehlen, M.; Jansen, A.; van Treeck, U.; Hauri, A.M.; Zoellner, I.; Schreier, E.; Hamouda, O.; Stark, K. Large outbreak of hepatitis A in tourists staying at a hotel in Hurghada, Egypt, 2004—Orange juice implicated. Eurosurveill 2005, 10, E050609.2. [Google Scholar] [CrossRef]
- Shata, M.T.; Daef, E.A.; Zaki, M.E.; Abdelwahab, S.F.; Marzuuk, N.M.; Sobhy, M.; Rafaat, M.; Abdelbaki, L.; Nafeh, M.A.; Hashem, M.; et al. Protective role of humoral immune responses during an outbreak of hepatitis E in Egypt. Trans. R. Soc. Trop. Med. Hyg. 2012, 106, 613–618. [Google Scholar] [CrossRef]
- Talaat, M.; El-Sayed, N.; Kandeel, A.; Azab, M.A.; Afifi, S.; Youssef, F.G.; Ismael, T.; Hajjeh, R.; Mahoney, F.J. Sentinel surveillance for patients with acute hepatitis in Egypt, 2001–2004. East. Mediterr. Health J. 2010, 16, 134–140. [Google Scholar] [CrossRef]
- Divizia, M.; Gabrieli, R.; Stefanoni, M.L.; Renganathan, E.; El Ghazzawi, E.; Kader, O.A.; Gamil, F.; El Sawaf, G.; El Sherbini, E.; Saleh, E.; et al. HAV and HEV infection in hospitalised hepatitis patients in Alexandria, Egypt. Eur. J. Epidemiol. 1999, 15, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Zaki, M.E.S.; Alsayed, M.A.L.; Abbas, H.R.R.; Ahmed, D.M.; Ashry, A.Y.E. Prevalence of hepatitis E virus in children with acute hepatitis: One Egyptian center study. Germs 2020, 10, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Zhang, H.; Wang, L.; Li, Z.; Wang, J.; Xu, B.; Hao, R.; Liu, C.; Fu, H.; Rao, H.; et al. The investigation of hepatitis A virus and hepatitis E virus co-infection in humans and animals in China. Acta Virol. 2020, 64, 20–27. [Google Scholar] [CrossRef]
- Malathi, S.; Mohanavalli, B.; Menon, T.; Srilatha, P.; Sankaranarayanan, V.S.; Raju, B.B.; Ramathilagam, B.; Thyagarajan, S.P. Clinical and viral marker pattern of acute sporadic hepatitis in children in Madras, South India. J. Trop. Pediatr. 1998, 44, 275–278. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Muchiri, I.; Okoth, F.A.; Ngaira, J.; Tuei, S. Seroprevalence of hav, hbv, hcv, and hev among acute hepatitis patients at kenyatta national hospital in Nairobi, Kenya. East Afr. Med. J. 2012, 89, 199–205. [Google Scholar] [PubMed]
- Mazhar, M.K.A.; Finger, F.; Evers, E.S.; Kuehne, A.; Ivey, M.; Yesurajan, F.; Shirin, T.; Ajim, N.; Kabir, A.; Musto, J.; et al. An outbreak of acute jaundice syndrome (AJS) among the Rohingya refugees in Cox’s Bazar, Bangladesh: Findings from enhanced epidemiological surveillance. PLoS ONE 2021, 16, e0250505. [Google Scholar] [CrossRef] [PubMed]
- Sayed, I.M.; El-Mokhtar, M.A.; Mahmoud, M.A.R.; Elkhawaga, A.A.; Gaber, S.; Seddek, N.H.; Abdel-Wahid, L.; Ashmawy, A.M.; Alkareemy, E.A.R. Clinical Outcomes and Prevalence of Hepatitis E Virus (HEV) Among Non-A-C Hepatitis Patients in Egypt. Infect. Drug Resist. 2021, 14, 59–69. [Google Scholar] [CrossRef]
- Tsarev, S.A.; Binn, L.N.; Gomatos, P.J.; Arthur, R.R.; Monier, M.K.; van Cuyck-Gandre, H.; Longer, C.F.; Innis, B.L. Phylogenetic analysis of hepatitis E virus isolates from Egypt. J. Med. Virol. 1999, 57, 68–74. [Google Scholar] [CrossRef]
- Hamza, H.; Abd-Elshafy, D.N.; Fayed, S.A.; Bahgat, M.M.; El-Esnawy, N.A.; Abdel-Mobdy, E. Detection and characterization of hepatitis A virus circulating in Egypt. Arch. Virol. 2017, 162, 1921–1931. [Google Scholar] [CrossRef]
- Pintó, R.M.; Alegre, D.; Domínguez, A.; El-Senousy, W.M.; Sánchez, G.; Villena, C.; Costafreda, M.I.; Aragonès, L.; Bosch, A. Hepatitis A virus in urban sewage from two Mediterranean countries. Epidemiol. Infect. 2007, 135, 270–273. [Google Scholar] [CrossRef]
- Kaur, R.; Gur, R.; Berry, N.; Kar, P. Etiology of endemic viral hepatitis in urban North India. Southeast Asian J. Trop. Med. Public Health 2002, 33, 845–848. [Google Scholar] [PubMed]
- Kumar, A.; Yachha, S.K.; Poddar, U.; Singh, U.; Aggarwal, R. Does co-infection with multiple viruses adversely influence the course and outcome of sporadic acute viral hepatitis in children? J. Gastroenterol. Hepatol. 2006, 21, 1533–1537. [Google Scholar] [CrossRef] [PubMed]
- Samaddar, A.; Taklikar, S.; Kale, P.; Kumar, C.A.; Baveja, S. Infectious hepatitis: A 3-year retrospective study at a tertiary care hospital in India. Indian J. Med. Microbiol. 2019, 37, 230–234. [Google Scholar] [CrossRef] [PubMed]
- Palewar, M.S.; Joshi, S.; Choudhary, G.; Das, R.; Sadafale, A.; Karyakarte, R. Prevalence of Hepatitis A virus (HAV) and Hepatitis E virus (HEV) in patients presenting with acute viral hepatitis: A 3-year retrospective study at a tertiary care Hospital in Western India. J. Fam. Med. Prim. Care 2022, 11, 2437–2441. [Google Scholar] [CrossRef]
- Manka, P.; Verheyen, J.; Gerken, G.; Canbay, A. Liver Failure due to Acute Viral Hepatitis (A–E). Visc. Med. 2016, 32, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Manka, P.; Bechmann, L.P.; Coombes, J.D.; Thodou, V.; Schlattjan, M.; Kahraman, A.; Syn, W.K.; Saner, F.; Gerken, G.; Baba, H.; et al. Hepatitis E Virus Infection as a Possible Cause of Acute Liver Failure in Europe. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2015, 13, 1836–1842. [Google Scholar] [CrossRef]
- Malik, H.; Malik, H.; Uderani, M.; Berhanu, M.; Soto, C.J.; Saleem, F. Fulminant Hepatitis A and E Co-infection Leading to Acute Liver Failure: A Case Report. Cureus 2023, 15, e38101. [Google Scholar] [CrossRef]
- Sayed, I.M.; Elkhawaga, A.A.; El-Mokhtar, M.A. Circulation of hepatitis E virus (HEV) and/or HEV-like agent in non-mixed dairy farms could represent a potential source of infection for Egyptian people. Int. J. Food Microbiol. 2020, 317, 108479. [Google Scholar] [CrossRef]
- El-Mokhtar, M.A.; Karam-Allah Ramadan, H.; Abdel Hameed, M.R.; Kamel, A.M.; Mandour, S.A.; Ali, M.; Abdel-Malek, M.A.; Abd El-Kareem, D.M.; Adel, S.; HSalama, E.; et al. Evaluation of hepatitis E antigen kinetics and its diagnostic utility for prediction of the outcomes of hepatitis E virus genotype 1 infection. Virulence 2021, 12, 1334–1344. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Items | HAV Patients (n = 57) |
|---|---|
| Age (years) | 15 (3–62) |
| (Median, minimum–maximum) | |
| <10 years | 15/57 (26.3%) |
| 10–20 years | 21/57 (36.84%) |
| 20–30 years | 15/57 (26.3%) |
| >30 years | 6/57 (10.52%) |
| Gender | |
| Male | 33/ 57 (57.9%) |
| Female * | 24/57 (42.1%) |
| Residence | |
| Rural | 49/57 (86%) |
| Urban | 8/57 (14%) |
| Clinical presentation | |
| Jaundice | 47/57 (82.46%) |
| Nausea/Vomiting | 32/57 (56.14%) |
| Fever | 22/57 (38.6%) |
| Abdominal pain | 20/57 (35.08%) |
| Liver function tests | |
| (Median, IQR) | |
| AST (IU/L) | 850 (424–1635) |
| ALT (IU/L) | 1521 (803–1918) |
| ALP (IU/L) | 187 (162–212) |
| Total bilirubin (mg/dL) | 4.95 (3.5–8.4) |
| Direct bilirubin (mg/dL) | 3.9 (2.9–6.5) |
| Serum albumin g/dL | 3.9 (3.31–4.1) |
| Items | HAV-Mono-Infection (n = 36) | HAV-HEV Co-Infection (n = 21) | p Value |
|---|---|---|---|
| Age (years) | 15 (8.5–27) | 15 (7–21) | ns |
| (Median, IQR) | |||
| <10 years | 9/36 (25%) | 6/21 (28.6%) | |
| 10–20 years | 12/36 (33.3%) | 9/21 (42.9%) | |
| 20–30 years | 10/36 (27.8%) | 5/21 (23.8%) | |
| >30 years | 5/36 (13.9%) | 1/21 (4.8%) | |
| Gender | ns | ||
| Male | 21/36 (58.3%) | 12/ 21 (57.9%) | |
| Female | 15/36 (41.7%) | 9/21 (42.1%) | |
| Residence | ns | ||
| Rural | 29/36 (80.6%) | 20/21 (95.2%) | |
| Urban | 7/36 (19.4%) | 1/21 (4.8%) | |
| Clinical presentation | |||
| Jaundice | 32/36 (88.9%) | 15/21 (71.4%) | ns |
| Nausea/Vomiting | 19/36 (52.78%) | 13/21 (61.9%) | ns |
| Fever | 14/36 (39%) | 8/21 (38%) | ns |
| Abdominal pain | 11/36 (30.6%) | 9/21 (42.9%) | ns |
| Hepatitis markers | |||
| Anti-HAV IgM | 36/36 (100%) | 21/21 (100%) | |
| HAV RNA | 36/36 (100%) | 21/21 (100%) | |
| Anti-HEV IgM | 0/36 (0%) | 21/21 (100%) | |
| HEV-RNA | 0/36 (0%) | 21/21 (100%) | |
| Outcome | 0.02 (*) | ||
| Self-limiting course | 35/36 (97.2%) | 16/21 (76.2%) | |
| Acute liver failure | 1/36 (2.8%) | 5/21 (23.8%) | |
| Encephlaopathy | 0/36 (0%) | 5/21 (23.8%) | 0.0049 (**) |
| Items | HAV Mono-Infection | HAV–HEV Co-Infection | ||||
|---|---|---|---|---|---|---|
| Patient #1 | Patient #2 | Patient #3 | Patient #4 | Patient #5 | ||
| Age (years) | 26 | 15 | 15 | 15 | 62 | 21 |
| Gender | male | male | male | female | female | female |
| Residence | Urban | Rural | Rural | Rural | Rural | Rural |
| Clinical symptoms | Jaundice, fever, and dark urine | Jaundice, fever, vomiting, dark urine, abdominal pain, and encephalopathy | Jaundice, vomiting, abdominal pain, and encephalopathy | Jaundice, fever, vomiting, and encephalopathy | Jaundice, dark urine, and encephalopathy | Jaundice, vomiting, and encephalopathy |
| Liver function tests | ||||||
| AST (IU/L) | 713 | 2134 | 707 | 959 | 1000 | 1141 |
| ALT (IU/L) | 1071 | 2140 | 1053 | 1159 | 1800 | 379 |
| ALP (IU/L) | 245 | 159 | 294 | 169 | 158 | 131 |
| Total bilirubin (mg/dL) | 8.2 | 3.3 | 2.6 | 13.7 | 13.8 | 8.8 |
| Direct bilirubin (mg/dL) | 6.4 | 2.6 | 2.0 | 12.6 | 11.7 | 7.0 |
| Serum albumin g/dL | 3.1 | 4.4 | 4.0 | 2.7 | 2.6 | 2.8 |
| International normalized ratio (INR) | 2.0 | 2.6 | 2.0 | 1.9 | 1.8 | 2.5 |
| Recovary (Days) | 17 | 14 | 16 | 17 | 27 | 18 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El-Mokhtar, M.A.; Elkhawaga, A.A.; Ahmed, M.S.H.; El-Sabaa, E.M.W.; Mosa, A.A.; Abdelmohsen, A.S.; Moussa, A.M.; Salama, E.H.; Aboulfotuh, S.; Ashmawy, A.M.; et al. High Incidence of Acute Liver Failure among Patients in Egypt Coinfected with Hepatitis A and Hepatitis E Viruses. Microorganisms 2023, 11, 2898. https://doi.org/10.3390/microorganisms11122898
El-Mokhtar MA, Elkhawaga AA, Ahmed MSH, El-Sabaa EMW, Mosa AA, Abdelmohsen AS, Moussa AM, Salama EH, Aboulfotuh S, Ashmawy AM, et al. High Incidence of Acute Liver Failure among Patients in Egypt Coinfected with Hepatitis A and Hepatitis E Viruses. Microorganisms. 2023; 11(12):2898. https://doi.org/10.3390/microorganisms11122898
Chicago/Turabian StyleEl-Mokhtar, Mohamed A., Amal A. Elkhawaga, Mona Sedky Hussein Ahmed, Ehsan M. W. El-Sabaa, Aliaa A. Mosa, Ahmed Shawkat Abdelmohsen, Abdelmajeed M. Moussa, Eman H. Salama, Sahar Aboulfotuh, Ahmed M. Ashmawy, and et al. 2023. "High Incidence of Acute Liver Failure among Patients in Egypt Coinfected with Hepatitis A and Hepatitis E Viruses" Microorganisms 11, no. 12: 2898. https://doi.org/10.3390/microorganisms11122898
APA StyleEl-Mokhtar, M. A., Elkhawaga, A. A., Ahmed, M. S. H., El-Sabaa, E. M. W., Mosa, A. A., Abdelmohsen, A. S., Moussa, A. M., Salama, E. H., Aboulfotuh, S., Ashmawy, A. M., Seddik, A. I., Sayed, I. M., & Ramadan, H. K.-A. (2023). High Incidence of Acute Liver Failure among Patients in Egypt Coinfected with Hepatitis A and Hepatitis E Viruses. Microorganisms, 11(12), 2898. https://doi.org/10.3390/microorganisms11122898