
The Association between Mycoplasma pneumoniae Genotype and Cutaneous Disease


Abstract
1. Introduction
2. Materials and Methods
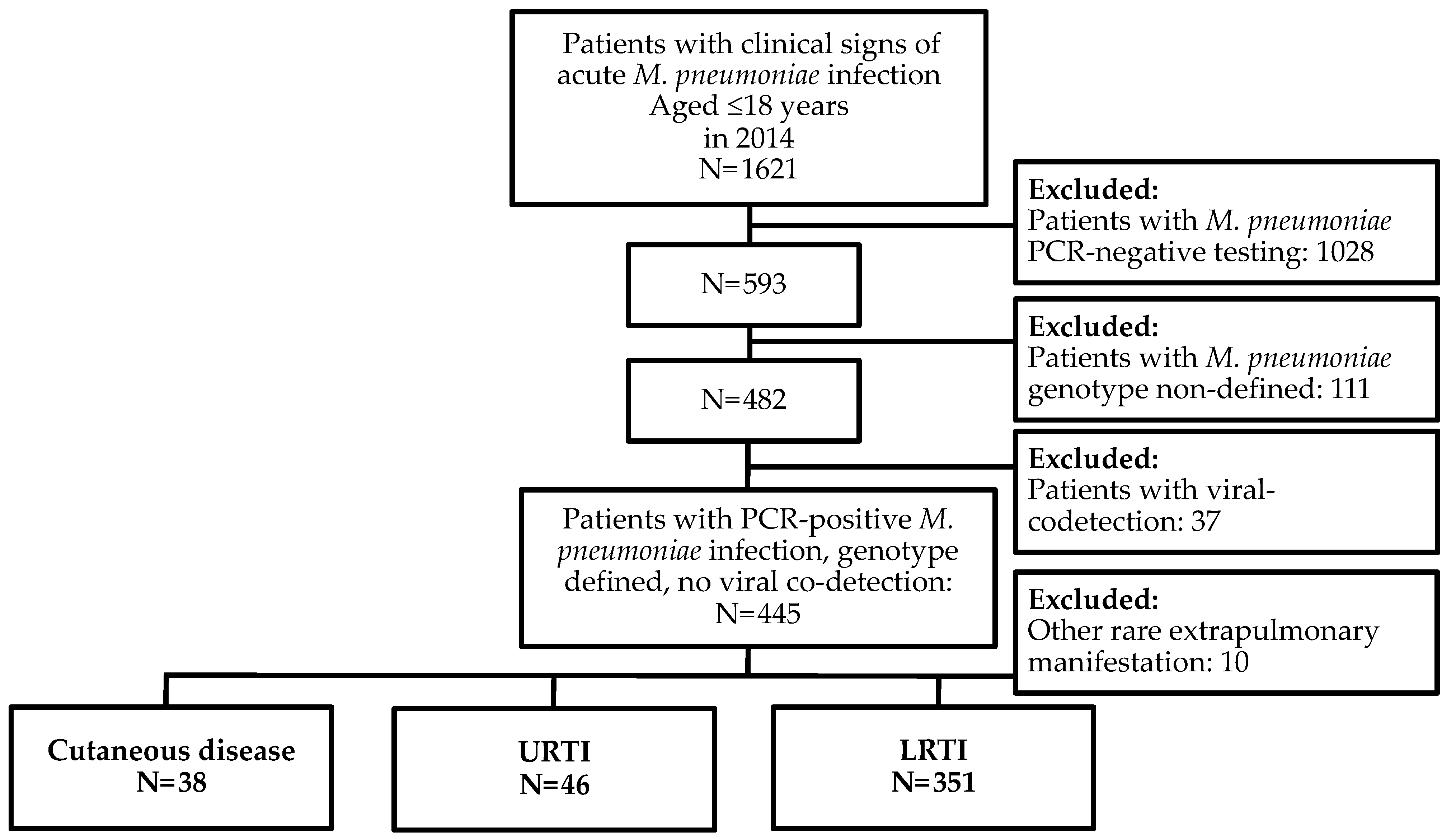
2.1. Study Subjects
2.2. Study Design
2.3. Methods
2.4. Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Atkinson, T.P.; Waites, K.B. Mycoplasma pneumoniae infections in childhood. Pediatr. Infect. Dis. J. 2014, 33, 92–94. [Google Scholar] [CrossRef]
- Kutty, P.K.; Jain, S.; Taylor, T.H.; Bramley, A.M.; Diaz, M.H.; Ampofo, K.; Arnold, S.; Williams, D.; Edwards, K.; McCullers, J.; et al. Mycoplasma pneumoniae among children hospitalized with community-acquired pneumonia. Clin. Infect. Dis. 2019, 68, 5–12. [Google Scholar] [CrossRef]
- Blasi, F. Atypical pathogens and respiratory tract infections. Eur. Respir. J. 2004, 24, 171–181. [Google Scholar] [CrossRef]
- Hu, J.; Ye, Y.; Chen, X.; Xiong, L.; Xie, W.; Liu, P. Insight into the Pathogenic Mechanism of Mycoplasma pneumoniae. Curr. Microbiol. 2022, 80, 14. [Google Scholar] [CrossRef]
- Schalock, P.C.; Dinulos, J.G. Mycoplasma pneumoniae-induced cutaneous disease. Int. J. Dermatol. 2009, 48, 673–680. [Google Scholar] [CrossRef] [PubMed]
- Terraneo, L.; Lava, S.A.; Camozzi, P.; Zgraggen, L.; Simonetti, G.D.; Bianchetti, M.G.; Milani, G.P. Unusual eruptions associated with Mycoplasma pneumoniae respiratory infections: Review of the literature. Dermatology 2015, 231, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Canavan, T.N.; Mathes, E.F.; Frieden, I. Mycoplasma pneumoniae-induced rash and mucositis as a syndrome distinct from Stevens-Johnson syndrome and erythema multiforme: A systematic review. J. Am. Acad. Dermatol. 2015, 72, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Liakos, W.; Xu, A.; Finelt, N. Clinical features of recurrent Mycoplasma pneumoniae-induced rash and mucositis. Pediatr. Dermatol. 2021, 38, 154–158. [Google Scholar] [CrossRef]
- Chen, N.; Li, M. Case Report and Literature Review: Clinical Characteristics of 10 Children With Mycoplasma pneumoniae-Induced Rash and Mucositis. Front. Pediatr. 2022, 10, 823376. [Google Scholar] [CrossRef]
- Fan, X.; Luo, Y.; Lu, J.; Xu, J.; Chen, Q.; Guo, H.; Jin, P. Erythema Multiforme Major Associated With Community-Acquired Pneumonia: Lessons From a Case Report. Front. Pediatr. 2021, 9, 698261. [Google Scholar] [CrossRef]
- Dégrange, S.; Cazanave, C.; Charron, A.; Renaudin, H.; Bébéar, C.; Bébéar, C.M. Development of multiple-locus variable-number tandem-repeat analysis for molecular typing of Mycoplasma pneumoniae. J. Clin. Microbiol. 2009, 47, 914–923. [Google Scholar] [CrossRef]
- Dumke, R.; Rodriguez, N. Use of different approaches for the culture-independent typing of Mycoplasma pneumoniae from two geographically distinct regions. J. Microbiol. Methods 2021, 186, 106239. [Google Scholar] [CrossRef]
- Xiao, J.; Liu, Y.; Wang, M.; Jiang, C.; You, X.; Zhu, C. Detection of Mycoplasma pneumoniae P1 subtype variations by denaturing gradient gel electrophoresis. Diagn Microbiol. Infect. Dis. 2014, 78, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Zhao, F.; Cao, B.; Li, J.; Song, S.; Tao, X.; Yin, Y.; He, L.; Zhang, J. Sequence analysis of the p1 adhesin gene of Mycoplasma pneumoniae in clinical isolates collected in Beijing in 2008 to 2009. J. Clin. Microbiol. 2011, 49, 3000–3003. [Google Scholar] [CrossRef]
- Dorigo-Zetsma, J.W.; Dankert, J.; Zaat, S.A. Genotyping of Mycoplasma pneumoniae clinical isolates reveals eight P1 subtypes within two genomic groups. J. Clin. Microbiol. 2000, 38, 965–970. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Xue, G.; Yan, C.; Li, S.; Cao, L.; Yuan, Y.; Zhao, H.; Feng, Y.; Wang, L.; Fan, Z. Multiple-locus variable-number tandem-repeat analysis of Mycoplasma pneumoniae clinical specimens and proposal for amendment of MLVA nomenclature. PLoS ONE 2013, 8, e64607. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.J.; Holden, M.T.; Spiller, O.B.; Chalker, V.J. Development of a Multilocus Sequence Typing Scheme for Molecular Typing of Mycoplasma pneumoniae. J. Clin. Microbiol. 2015, 53, 3195–3203. [Google Scholar] [CrossRef]
- Rodman Berlot, J.; Krivec, U.; Mrvič, T.; Kogoj, R.; Keše, D. Mycoplasma pneumoniae P1 genotype indicates severity of lower respiratory tract infections in children. J. Clin. Microbiol. 2021, 59, e0022021. [Google Scholar] [CrossRef]
- Rodman Berlot, J.; Mrvič, T.; Keše, D. Mycoplasma pneumoniae multilocus variable-number tandem-repeat analysis genotypes are associated with inflammatory biomarker levels in children with lower respiratory tract infections. Eur. J. Clin. Microbiol. Infect. Dis. 2022, 41, 1099–1105. [Google Scholar] [CrossRef]
- Kogoj, R.; Praprotnik, M.; Mrvič, T.; Korva, M.; Keše, D. Genetic diversity and macrolide resistance of Mycoplasma pneumoniae isolates from two consecutive epidemics in Slovenia. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 99–107. [Google Scholar] [CrossRef]
- Lee, S.W. Methods for testing statistical differences between groups in medical research: Statistical standard and guideline of Life Cycle Committee. Life Cycle 2022, 2, e1. [Google Scholar] [CrossRef]
- Lee, S.W. Regression analysis for continuous independent variables in medical research: Statistical standard and guideline of Life Cycle Committee. Life Cycle 2022, 2, e3. [Google Scholar] [CrossRef]
- Meyer Sauteur, P.M.; Theiler, M.; Buettcher, M. Frequency and clinical presentation of mucocutaneous disease due to Mycoplasma pneumoniae infection in children with community-acquired pneumonia. JAMA Dermatol. 2020, 156, 144–150. [Google Scholar] [CrossRef]
- Narita, M. Classification of extrapulmonary manifestations due to Mycoplasma pneumoniae infection on the basis of possible pathogenesis. Front. Microbiol. 2016, 7, 23. [Google Scholar] [CrossRef]
- Sánchez-Vargas, F.M.; Gómez-Duarte, O.G. Mycoplasma pneumoniae-an emerging extra-pulmonary pathogen. Clin. Microbiol. Infect. 2008, 14, 105–117. [Google Scholar] [CrossRef] [PubMed]
- Simmons, W.L.; Daubenspeck, J.M.; Osborne, J.D.; Balish, M.F.; Waites, K.B.; Dybvig, K. Type 1 and type 2 strains of Mycoplasma pneumoniae form different biofilms. Microbiology 2013, 159, 737–747. [Google Scholar] [CrossRef]
- Lluch-Senar, M.; Cozzuto, L.; Cano, J.; Delgado, J.; Llórens-Rico, V.; Pereyre, S.; Bebear, C.; Serrano, L. Comparative “-omics” in Mycoplasma pneumoniae clinical isolates reveals key virulence factors . PLoS ONE 2015, 10, e0137354. [Google Scholar] [CrossRef] [PubMed]
- Techasaensiri, C.; Tagliabue, C.; Cagle, M.; Iranpour, P.; Katz, K.; Kannan, T.R.; Coalson, J.J.; Baseman, J.B.; Hardy, R.D. Variation in colonization, ADP-ribosylating and vacuolating cytotoxin, and pulmonary disease severity among Mycoplasma pneumoniae strains. Am. J. Respir. Crit. Care Med. 2010, 182, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Qu, J.; Yu, X.; Liu, Y.; Yin, Y.; Gu, L.; Cao, B.; Wang, C. Specific multilocus variable-number tandem-repeat analysis genotypes of Mycoplasma pneumoniae are associated with diseases severity and macrolide susceptibility. PLoS ONE 2013, 8, e82174. [Google Scholar] [CrossRef] [PubMed]
- Yan, C.; Xue, G.; Zhao, H.; Feng, Y.; Li, S.; Cui, J.; Ni, S.; Sun, H. Molecular and clinical characteristics of severe Mycoplasma pneumoniae pneumonia in children. Pediatr. Pulmonol. 2019, 54, 1012–1021. [Google Scholar] [CrossRef] [PubMed]
- Meyer Sauteur, P.M.; Pánisová, E.; Seiler, M.; Theiler, M.; Berger, C.; Dumke, R. Mycoplasma pneumoniae genotypes and clinical outcome in children. J. Clin. Microbiol. 2021, 18, e0074821. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Zhang, Y.; Sheng, Y.; Zhang, L.; Shen, Z.; Chen, Z. More complications occur in macrolide-resistant than in macrolide-sensitive Mycoplasma pneumoniae pneumonia. Antimicrob. Agents Chemother. 2014, 58, 1034–1038. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Cutaneous Disease | URTI | LRTI | Test Statistic, p | |
|---|---|---|---|---|
| Subjects N | 38 | 46 | 351 | |
| Boys/girls (%) | 50%/50% | 63%/37% | 51%/49% | χ2(2) = 2.54, 0.281 |
| Age (years) | 6.6 (IQR 4.6–9.8) | 5.9 (IQR 4.1–9.4) | 7.0 (IQR 4.9–9.9) | H(2) = 1.34, 0.511 |
| <5 years 5–18 years | 32% (12/38) 68% (26/38) | 33% (15/46) 67% (31/46) | 26% (93/351) 74% (258/351) | χ2(2) = 1.09, 0.579 |
| Mp Genotype P1-1/P1-2 (%) MLVA type | 82%/18% | 70%/30% | 74%/26% | χ2(2) = 1.63, 0.442 |
| MLVA-3,6,6,2 MLVA-4,5,7,2 MLVA-4,5,7,3 | 10% (3/29) 86% (25/29) 4% (1/29) | 18% (7/38) 66% (25/38) 3% (1/38) | 12% (31/255) 72% (183/255) 4% (9/255) | χ2(2) = 1.33, 0.514 χ2(2) = 3.65, 0.162 χ2(2) = 0.08, 0.960 |
| Dermatological Presentation | Frequency |
|---|---|
| Urticarial eruptions | 55.3% (21/38) |
| Maculopapular eruptions | 36.8% (14/38) |
| Erythema multiforme | 2.6% (1/38) |
| Henoch–Schönlein purpura | 2.6% (1/38) |
| Pityriasis rosea | 2.6% (1/38) |
| Maculopapular Eruptions | Urticarial Eruptions | Test Statistic, p | |
|---|---|---|---|
| Subjects N | 14 | 21 | |
| Boys/girls (%) | 43%/57% | 48%/52% | χ2(1) = 0.08, 0.782 |
| Age (years) | 6.5 (IQR 4.6–10.0) | 6.5 (IQR 4.4–8.1) | U(1) = 129.0, 0.544 |
| <5 years 5–18 years | 29% (4/14) 71% (10/14) | 38% (8/21) 62% (13/21) | χ2(1) = 0.34, 0.561 |
| CRP (mg/L) | 14.0 (IQR 4.0–32.3) | 19.5 (IQR 4.5–47.0) | U(1) = 92.5, 0.413 |
| WBC (×109/L) | 9.1 (IQR 6.4–12.3) | 10.0 (IQR 7.5–14.2) | U(1) = 96.5, 0.519 |
| Hospitalization because of rash | 0% (0/14) | 24% (5/21) | χ2(1) = 3.89, 0.049 |
| Treatment Macrolide antibiotic Antihistamines Systemic steroids | 93% (13/14) 0% (0/14) 0% (0/14) | 100% (21/21) 24% (5/21) 10% (2/21) | χ2(1) = 1.54, 0.214 χ2(1) = 3.89, 0.049 χ2(1) = 1.41, 0.234 |
| Mp Genotype | |||
| P1-1/P1-2 (%) MLVA type | 93%/7% | 76%/24% | χ2(1) = 1.64, 0.200 |
| MLVA-3,6,6,2 MLVA-4,5,7,2 MLVA-4,5,7,3 | 0% (0/12) 100% (12/12) 0% (0/12) | 14% (2/14) 79% (11/14) 7% (1/14) | χ2(1) = 1.86, 0.173 χ2(1) = 2.91, 0.088 χ2(1) = 0.89, 0.345 |
| Age (yrs.)/ Gender | Dermatological Presentation | P1 Type | MLVA Type | Symptoms | Treatment | Outcome |
|---|---|---|---|---|---|---|
| 11/M | Erythema multiforme | 1 | 4,5,7,2 | Target lesions on limbs, dehydration | azithromycin parenteral hydration | Complete recovery |
| 6/M | Henoch–Schönlein purpura with GIT involvement | 1 | 4,5,7,2 | Abdominal pain, petechiae on lower limbs | azithromycin methylprednisolone | Complete recovery |
| 12/M | Pityriasis rosea | 2 | 3,6,6,2 | Rash | azithromycin | Complete recovery |
| Inpatients | Outpatients | Test Statistic, p | |
|---|---|---|---|
| Subjects N | 6 | 32 | |
| Boys/girls (%) | 50%/50% | 50%/50% | χ2(1) = 0.00, 1.000 |
| Age (years) | 4.9 (IQR 3.8–7.9) | 6.9 (IQR 5.0–10.0) | U(1) = 64.0, 0.200 |
| <5 years 5–18 years | 67% (4/6) 33% (2/6) | 25% (8/32) 75% (24/32) | χ2(1) = 4.06, 0.044 |
| CRP (mg/L) | 12.5 (IQR 4.0–29.0) | 12.0 (IQR 4.0–39.0) | U(1) = 71.5, 0.654 |
| WBC (× 109/L) | 9.8 (IQR 6.3–11.5) | 9.7 (IQR 7.4–12.4) | U(1) = 72.0, 0.674 |
| Treatment Macrolide antibiotic Antihistamines Systemic steroids | 100% (6/6) 67% (4/6) 50% (3/6) | 97% (31/32) 3% (1/32) 0% (0/32) | χ2(1) = 0.19, 0.661 χ2(1) = 17.85, <0.001 χ2(1) = 17.37, <0.001 |
| Mp Genotype | |||
| P1-1/P1-2 (%) MLVA type | 67%/33% | 84%/16% | χ2(1) = 1.05, 0.305 |
| MLVA-3,6,6,2 MLVA-4,5,7,2 MLVA-4,5,7,3 | 40% (2/5) 60% (3/5) 0% (0/5) | 4% (1/24) 92% (22/24) 4% (1/24) | χ2(1) = 5.73, 0.017 χ2(1) = 3.49, 0.062 χ2(1) = 0.22, 0.642 |
| Crude OR (95%-CI) | Adjusted a OR (95%-CI) | p Values (Crude/Adjusted) | |
|---|---|---|---|
| P1 type 1 P1 type 2 | 0.37 (0.05–2.60) 2.70 (0.39–18.93) | 0.33 (0.04–2.48) 3.02 (0.40–22.60) | 0.317/0.281 0.317/0.281 |
| MLVA-3,6,6,2 MLVA-4,5,7,2 | 15.33 (1.05–224.78) 0.14 (0.01–1.36) | 232.43 (1.18–45,972.69) 0.10 (0.01–1.32) | 0.046/0.043 0.090/0.081 |
| MLVA-4,5,7,3 | 0.00 (0.00) | 0.00 (0.00) | 1.000/1.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodman Berlot, J.; Mrvič, T.; Košnik, M.; Keše, D. The Association between Mycoplasma pneumoniae Genotype and Cutaneous Disease. Microorganisms 2023, 11, 205. https://doi.org/10.3390/microorganisms11010205
Rodman Berlot J, Mrvič T, Košnik M, Keše D. The Association between Mycoplasma pneumoniae Genotype and Cutaneous Disease. Microorganisms. 2023; 11(1):205. https://doi.org/10.3390/microorganisms11010205
Chicago/Turabian StyleRodman Berlot, Jasna, Tatjana Mrvič, Mitja Košnik, and Darja Keše. 2023. "The Association between Mycoplasma pneumoniae Genotype and Cutaneous Disease" Microorganisms 11, no. 1: 205. https://doi.org/10.3390/microorganisms11010205
APA StyleRodman Berlot, J., Mrvič, T., Košnik, M., & Keše, D. (2023). The Association between Mycoplasma pneumoniae Genotype and Cutaneous Disease. Microorganisms, 11(1), 205. https://doi.org/10.3390/microorganisms11010205