



Design and Analysis of a Spatial 2R1T Remote Center of Motion Mechanism for a Subretinal Surgical Robot

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Preliminary Design of the 2R1T RCM Mechanism
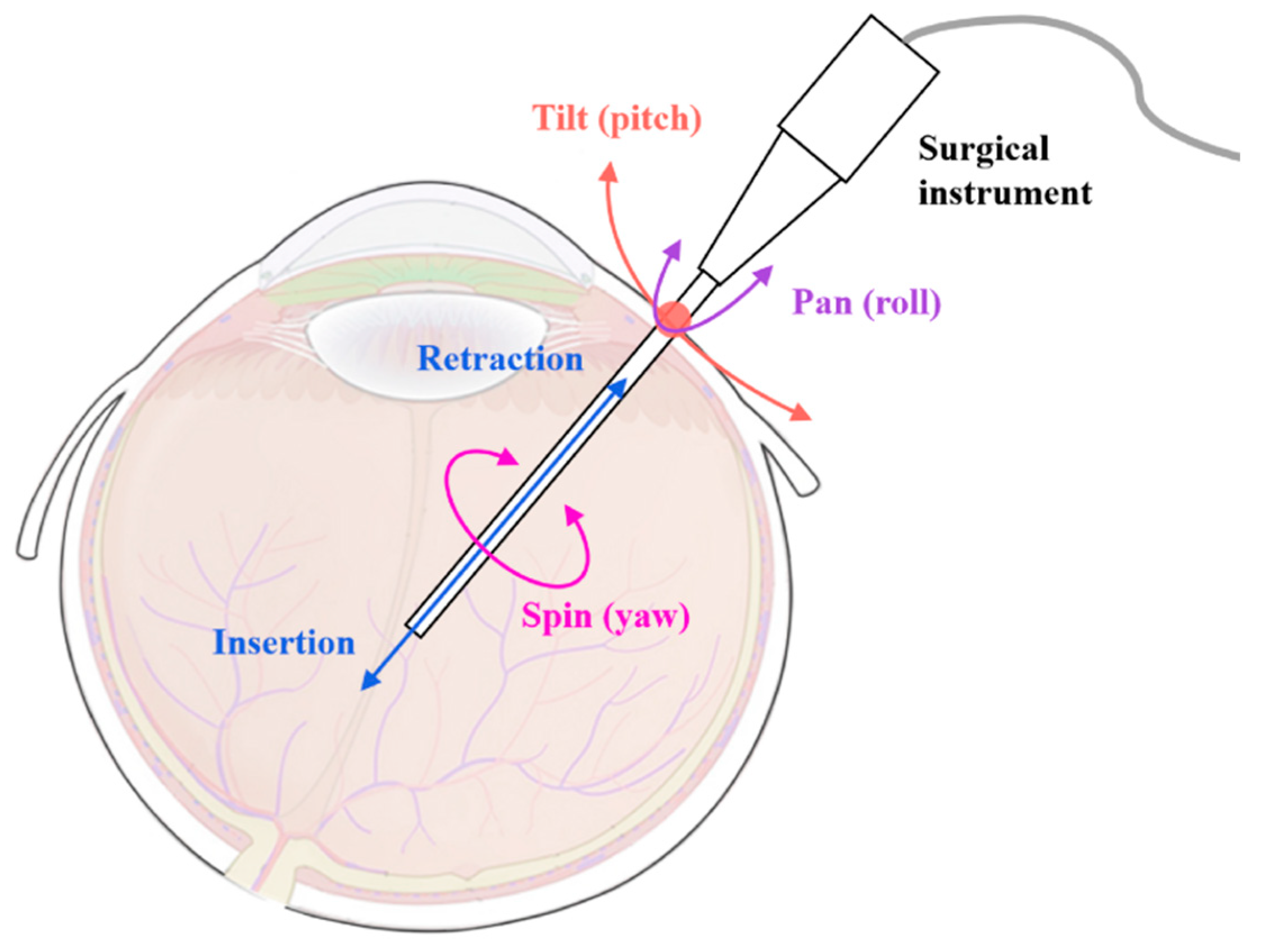
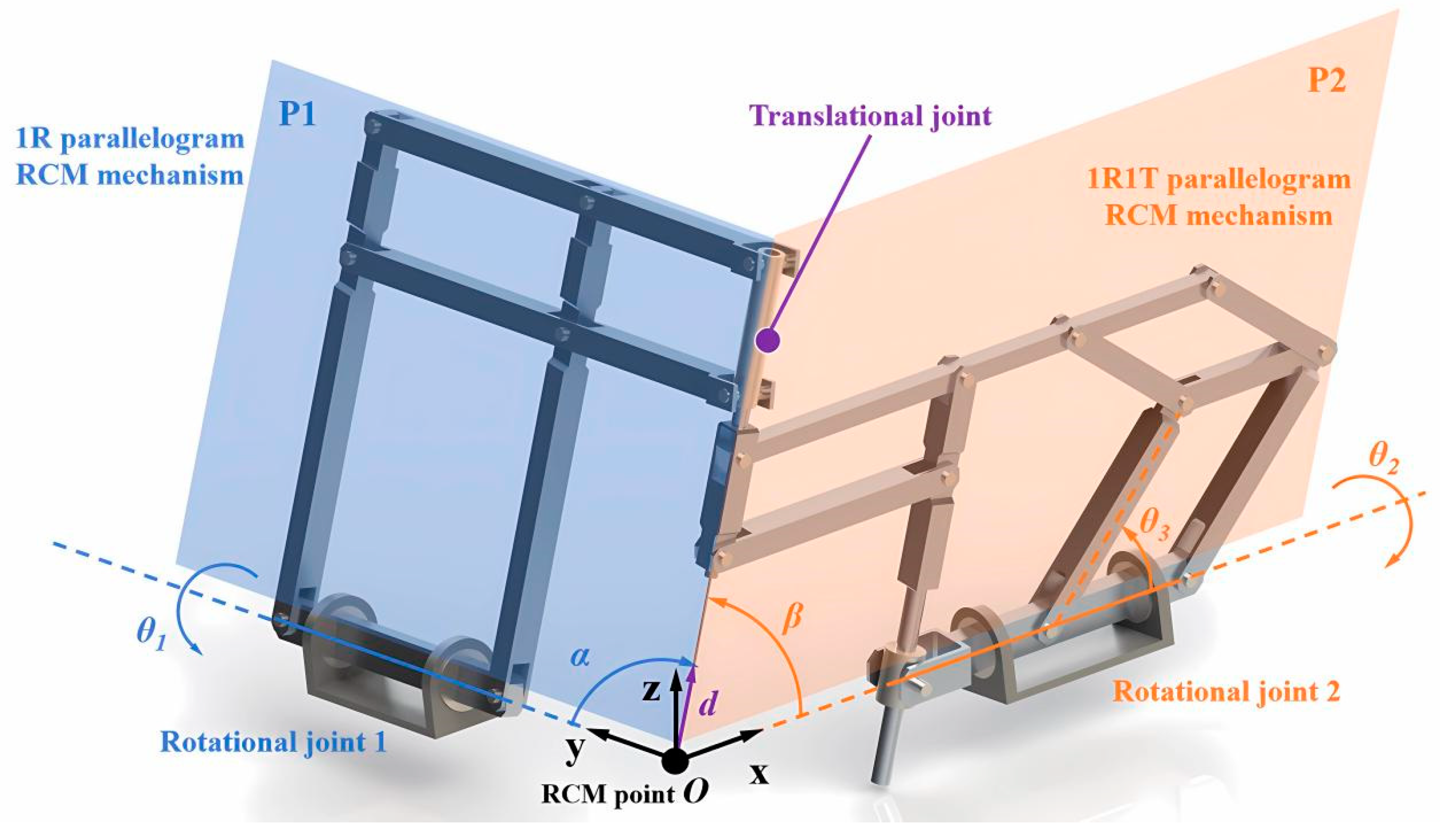
2.1. Concept of the Spatial 2R1T RCM Mechanism
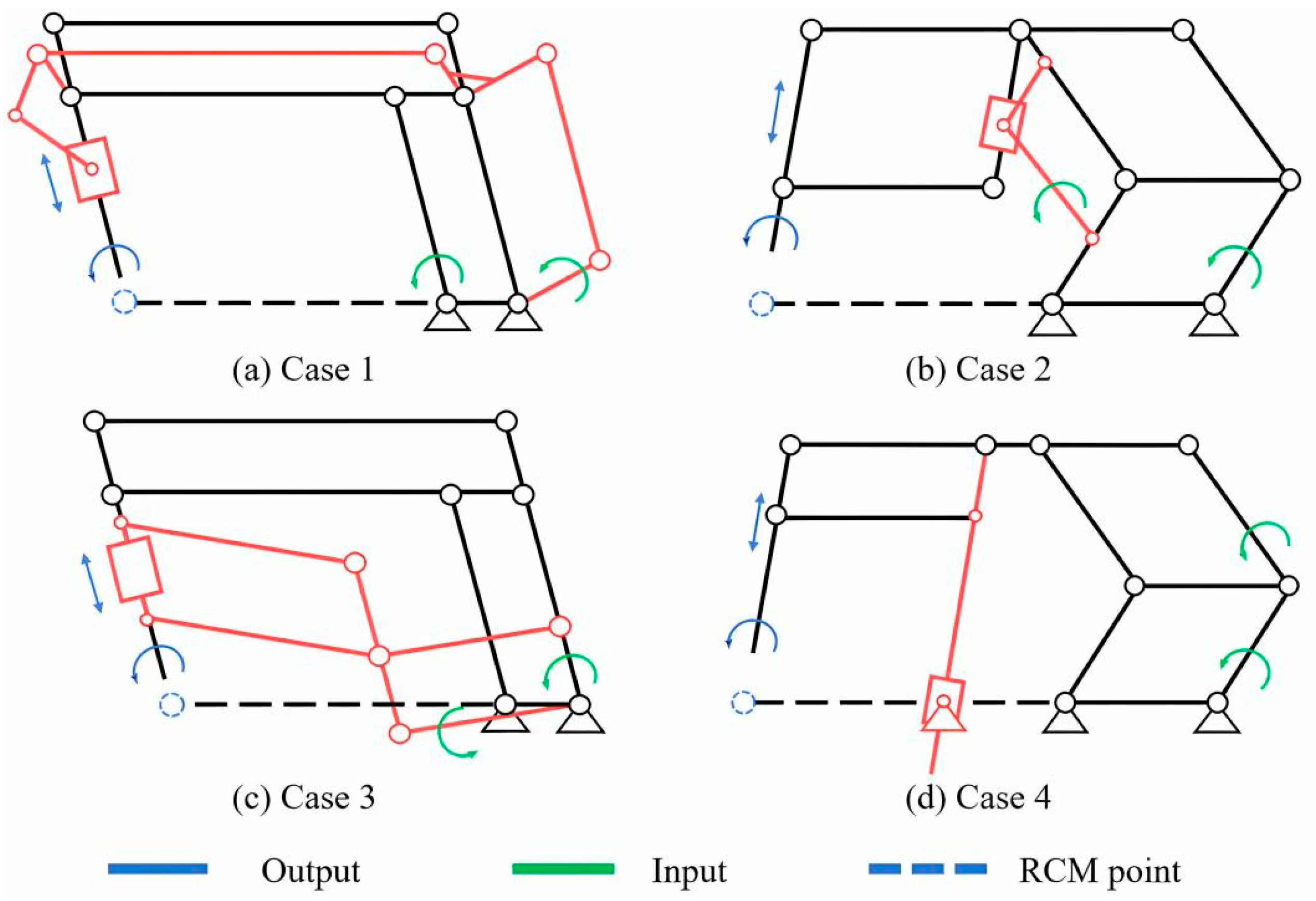
2.2. Type Synthesis of the Spatial 2R1T RCM Mechanism
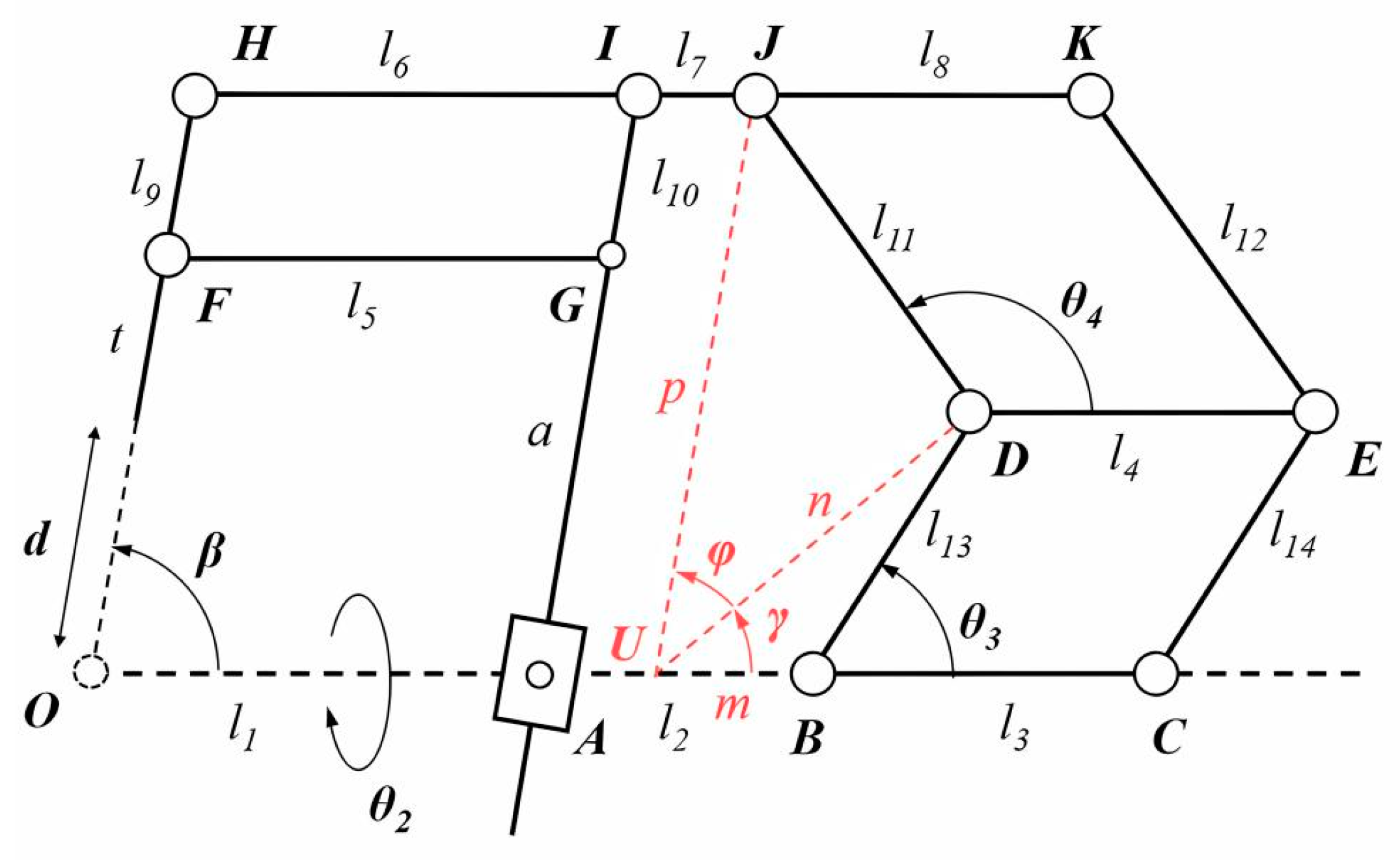
2.3. Kinematic Modeling and Analysis
2.4. Inverse Kinematics
2.5. Forward Kinematics
2.6. Differential Kinematics
2.7. Singularity
3. Workspace Analysis and Parameter Determination
3.1. Planar Workspace
3.2. Parameter Analysis and Selection for the 1R1T Mechanism
3.2.1. Parameter Analysis and Kinematic Constraints
3.2.2. Analysis and Evaluation Methods
- (1)
- For each configuration, calculate its workspace.
- (2)
- Eliminate the configurations that do not cover the targeted workspace.
- (3)
- Eliminate the configurations that do not satisfy the kinematic constraints.
- (4)
- For the qualified configurations, calculate their coverage of the non-targeted space within the vitreoretinal area.
- (5)
- Rank the coverage of the non-targeted area and output the configuration with the highest coverage.
3.2.3. Results
3.3. Three-Dimensional Workspace
4. Prototype
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A. Detailed Expressions for the Jacobian Matrix
References
- Nuzzi, R.; Brusasco, L. State of the art of robotic surgery related to vision: Brain and eye applications of newly available devices. Eye Brain 2018, 10, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, L.; Oliveira, J.; Kuroiwa, D.; Kolko, M.; Fernandes, R.; Junior, O.; Moraes, N.; Vasconcelos, H.; Oliveira, T.; Maia, M. Advances in vitreoretinal surgery. J. Clin. Med. 2022, 11, 6428. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.; Dai, J.S.; Dasgupta, P. Kinematic design considerations for minimally invasive surgical robots: An overview. Int. J. Med. Robot. Comput. Assist. Surg. 2012, 8, 127–145. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.; Stoianovici, D. Medical robotics in computer-integrated surgery. IEEE Trans. Robot. Autom. 2003, 19, 765–781. [Google Scholar] [CrossRef]
- Rahimy, E.; Wilson, J.; Tsao, T.-C.; Schwartz, S.; Hubschman, J.-P. Robot-assisted intraocular surgery: Development of the IRISS and feasibility studies in an animal model. Eye 2013, 27, 972–978. [Google Scholar] [CrossRef] [PubMed]
- Molaei, A.; Abedloo, E.; Taghirad, H.D.; Marvi, Z. Kinematic and workspace analysis of diamond: An innovative eye surgery robot. In Proceedings of the Iranian Conference on Electrical Engineering, Tehran, Iran, 10–14 May 2015; pp. 882–887. [Google Scholar]
- Tsukimoto, Y.; Kawai, T.; Nishikawa, A.; Nishizawa, Y.; Nakamura, T. Surgical assistant manipulator with rack gear and gear train mechanism for laparoscopic surgery. In Proceedings of the IEEE/SICE International Symposium on System Integration, Narvik, Norway, 9–12 January 2022; pp. 60–64. [Google Scholar] [CrossRef]
- Zong, G.; Pei, X.; Yu, J.; Bi, S. Classification and type synthesis of 1-DOF remote center of motion mechanisms. Mech. Mach. Theory 2008, 43, 1585–1595. [Google Scholar] [CrossRef]
- Taylor, R.H.; Funda, J.; Grossman, D.D.; Karidis, J.P.; LaRose, D.A. Remote Center-of-Motion Robot for Surgery. U.S. Patent 5,397,323, 14 March 1995. [Google Scholar]
- Taylor, R.; Funda, J.; Eldridge, B.; Gomory, S.; Gruben, K.; LaRose, D.; Talamini, M.; Kavoussi, L.; Anderson, J. A telerobotic assistant for laparoscopic surgery. IEEE Eng. Med. Biol. Mag. 1995, 14, 279–288. [Google Scholar] [CrossRef]
- He, C.-Y.; Huang, L.; Yang, Y.; Liang, Q.-F.; Li, Y.-K. Research and realization of a master-slave robotic system for retinal vascular bypass surgery. Chin. J. Mech. Eng. 2019, 31, 78. [Google Scholar] [CrossRef]
- Wang, N.; Zhang, X.; Li, M.; Zhang, H.; Stoyanov, D.; Stilli, A. A 5-DOFs robot for posterior segment eye microsurgery. IEEE Robot. Autom. Lett. 2022, 7, 10128–10135. [Google Scholar] [CrossRef]
- Channa, R.; Iordachita, I.; Handa, J.T. Robotic vitreoretinal surgery. Retin. J. Retin. Vitr. Dis. 2017, 37, 1220–1228. [Google Scholar] [CrossRef]
- Zong, G. Design of double parallelogram remote-center-of-motion mechanisms. Chin. J. Mech. Eng. 2007, 43, 103–108. [Google Scholar] [CrossRef]
- Huang, L.; Yang, Y.; Xiao, J.J.; Su, P. Type synthesis of 1r1t remote center of motion mechanisms based on pantograph mechanisms. J. Mech. Des. 2016, 138, 014501. [Google Scholar] [CrossRef]
- Smits, J.; Reynaerts, D.; Poorten, E.V. Synthesis and methodology for optimal design of a parallel remote center of motion mechanism: Application to robotic eye surgery. Mech. Mach. Theory 2020, 151, 103896. [Google Scholar] [CrossRef]
- Lin, R.; Guo, W.; Cheng, S.S. Type synthesis of 2R1T remote center of motion parallel mechanisms with a passive limb for minimally invasive surgical robot. Mech. Mach. Theory 2022, 172, 104766. [Google Scholar] [CrossRef]
- Zhang, F.; Zhang, X.; Hang, L.; Lu, C.; Furukawa, T. Type Synthesis of N-Parallelogram-Based Surgical Arm with Remote Actuated Configuration; Lecture Notes in Electrical Engineering; Springer: Singapore, 2017; Volume 408, pp. 183–194. [Google Scholar] [CrossRef]
- Gijbels, A.; Wouters, N.; Stalmans, P.; Van Brussel, H.; Reynaerts, D.; Poorten, E.V. Design and realization of a novel robotic manipulator for retinal surgery. In Proceedings of the IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS), Tokyo, Japan, 3–7 November 2013; pp. 3598–3603. [Google Scholar]
- Ourak, M.; Smits, J.; Esteveny, L.; Borghesan, G.; Gijbels, A.; Schoevaerdts, L.; Douven, Y.; Scholtes, J.; Lankenau, E.; Eixmann, T.; et al. Combined OCT distance and FBG force sensing cannulation needle for retinal vein cannulation: In vivo animal validation. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Gijbels, A.; Smits, J.; Schoevaerdts, L.; Willekens, K.; Poorten, E.B.V.; Stalmans, P.; Reynaerts, D. In-human robot-assisted retinal vein cannulation, a world first. Ann. Biomed. Eng. 2018, 46, 1676–1685. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Wang, J.; Wang, H. A new type of planar two degree-of-freedom remote center-of-motion mechanism inspired by the Peaucellier-Lipkin straight-line linkage. J. Mech. Des. 2018, 141, 015001. [Google Scholar] [CrossRef]
- Ye, W.; Zhang, B.; Li, Q.C. Design of a 1R1T planar mechanism with remote center of motion. Mech. Mach. Theory 2020, 149, 103845. [Google Scholar] [CrossRef]
- Liu, S.T.; Harewood, L.; Chen, B.; Chen, C. A skeletal prototype of surgical arm based on dual-triangular mechanism. J. Mech. Robot.-Trans. ASME 2016, 8, 041015. [Google Scholar] [CrossRef]
- Jingjing, X.; Long, H.; Lijun, S.; Yang, Y. Design and research of a robotic aided system for retinal vascular bypass surgery. J. Med Devices-Trans. ASME 2014, 8, 044501. [Google Scholar] [CrossRef]
- Yan, C.; Liu, M.; Shi, G.; Fan, J.; Li, Y.; Wu, S.; Hu, J. Design of a subretinal injection robot based on the rcm mechanism. Micromachines 2023, 14, 1998. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Zhang, P.; Jin, H.; Hu, Y.; Zhang, J. Type synthesis for remote center of motion mechanisms based on coupled motion of two degrees-of-freedom. J. Mech. Des. 2017, 138, 122301. [Google Scholar] [CrossRef]
- Liu, S.; Chen, B.; Caro, S.; Briot, S.; Harewood, L.; Chen, C. A cable linkage with remote centre of motion. Mech. Mach. Theory 2016, 105, 583–605. [Google Scholar] [CrossRef]
- Huang, L.; Yin, L.; Liu, B.; Yang, Y. Design and error evaluation of planar 2dof remote center of motion mechanisms with cable transmissions. J. Mech. Des. 2020, 143, 013301. [Google Scholar] [CrossRef]
- Wang, Z.; Zhang, W.; Ding, X. Design and analysis of a novel mechanism with a two-DOF remote centre of motion. Mech. Mach. Theory 2021, 153, 103990. [Google Scholar] [CrossRef]
- Chen, G.; Wang, J.; Wang, H.; Chen, C.; Parenti-Castelli, V.; Angeles, J. Design and validation of a spatial two-limb 3R1T parallel manipulator with remote center-of-motion. Mech. Mach. Theory 2020, 149, 103807. [Google Scholar] [CrossRef]
- Sarks, J.P.; Sarks, S.H.; Killingsworth, M.C. Evolution of geographic atrophy of the retinal-pigment epithelium. Eye 1988, 2, 552–577. [Google Scholar] [CrossRef] [PubMed]
- Artal, P. Optics of the eye and its impact in vision: A tutorial. Adv. Opt. Photonics 2014, 6, 340–367. [Google Scholar] [CrossRef]
- Hashemi, H.; KhabazKhoob, M.; Yazdani, K.; Mehravaran, S.; Jafarzadehpur, E.; Fotouhi, A. Distribution of angle Kappa measurements with orbscan II in a population-based survey. J. Refract. Surg. 2010, 26, 966–971. [Google Scholar] [CrossRef]
- Malhotra, A.; Minja, F.J.; Crum, A.; Burrowes, D. Ocular anatomy and cross-sectional imaging of the eye. Semin. Ultrasound CT MRI 2011, 32, 2–13. [Google Scholar] [CrossRef]
- Lemley, C.A.; Han, D.P. An age-based method for planning sclerotomy placement during pediatric vitrectomy: A 12-year experience. Retin. J. Retin. Vitr. Dis. 2007, 27, 974–977. [Google Scholar] [CrossRef] [PubMed]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.; Wu, S.; Fan, J.; Jiang, T.; Shi, G. Design and Analysis of a Spatial 2R1T Remote Center of Motion Mechanism for a Subretinal Surgical Robot. Actuators 2024, 13, 124. https://doi.org/10.3390/act13040124
Li Y, Wu S, Fan J, Jiang T, Shi G. Design and Analysis of a Spatial 2R1T Remote Center of Motion Mechanism for a Subretinal Surgical Robot. Actuators. 2024; 13(4):124. https://doi.org/10.3390/act13040124
Chicago/Turabian StyleLi, Yunyao, Sujian Wu, Jinyu Fan, Tianliang Jiang, and Guohua Shi. 2024. "Design and Analysis of a Spatial 2R1T Remote Center of Motion Mechanism for a Subretinal Surgical Robot" Actuators 13, no. 4: 124. https://doi.org/10.3390/act13040124
APA StyleLi, Y., Wu, S., Fan, J., Jiang, T., & Shi, G. (2024). Design and Analysis of a Spatial 2R1T Remote Center of Motion Mechanism for a Subretinal Surgical Robot. Actuators, 13(4), 124. https://doi.org/10.3390/act13040124