
Exposure to SARS-CoV-2 in Hospital Environment: Working in a COVID-19 Ward Is a Risk Factor for Infection

 , , , and
, , , and
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pallett, S.J.C.; Rayment, M.; Patel, A.; Fitzgerald-Smith, S.A.M.; Denny, S.J.; Charani, E.; Mai, A.L.; Gilmour, K.C.; Hatcher, J.; Scott, C.; et al. Point-of-care serological assays for delayed SARS-CoV-2 case identification among health-care workers in the UK: A prospective multicentre cohort study. Lancet Respir. Med. 2020, 8, 885–894. [Google Scholar] [CrossRef]
- Kohmer, N.; Westhaus, S.; Rühl, C.; Ciesek, S.; Rabenau, H.F. Brief clinical evaluation of six high-throughput SARS-CoV-2 IgG antibody assays. J. Clin. Virol. 2020, 129, 104480. [Google Scholar] [CrossRef]
- Martin, C.; Montesinos, I.; Dauby, N.; Gilles, C.; Dahma, H.; Van Den Wijngaert, S.; De Wit, S.; Delforge, M.; Clumeck, N.; Vandenberg, O. Dynamics of SARS-CoV-2 RT-PCR positivity and seroprevalence among high-risk healthcare workers and hospital staff. J. Hosp. Infect. 2020, 106, 102–106. [Google Scholar] [CrossRef]
- Blairon, L.; Mokrane, S.; Wilmet, A.; Dessilly, G.; Kabamba-Mukadi, B.; Beukinga, I.; Tre-Hardy, M. Large-scale, molecular and serological SARS-CoV-2 screening of healthcare workers in a 4-site public hospital in Belgium after COVID-19 outbreak. J. Infect. 2020, 82, 159–198. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7392848/ (accessed on 15 November 2020). [CrossRef]
- Paderno, A.; Fior, M.; Berretti, G.; Schreiber, A.; Grammatica, A.; Mattavelli, D.; Deganello, A. SARS-CoV-2 infection in health care workers: Cross-sectional analysis of an Otolaryngology unit. Otolaryngol. Head Neck Surg. 2020, 163, 671–672. [Google Scholar] [CrossRef]
- Korth, J.; Wilde, B.; Dolff, S.; Anastasiou, O.E.; Krawczyk, A.; Jahn, M.; Cordes, S.; Rosse, B.; Esser, S.; Lindemann, M.; et al. SARS-CoV-2-specific antibody detection in healthcare workers in Germany with direct contact to COVID-19 patients. J. Clin. Virol. 2020, 128, 104437. [Google Scholar] [CrossRef]
- Mansour, M.; Leven, E.; Muellers, K.; Stone, K.; Mendu, D.R.; Wajnberg, A. Prevalence of SARS-CoV-2 antibodies among healthcare workers at a tertiary academic hospital in New York City. J. Gen. Intern. Med. 2020, 35, 2485–2486. [Google Scholar] [CrossRef] [PubMed]
- Sotgiu, G.; Barassi, A.; Miozzo, M.; Saderi, L.; Piana, A.; Orfeo, N.; Colosio, C.; Felisati, G.; Davi, M.; Gerli, A.G.; et al. SARS-CoV-2 specific serological pattern in healthcare workers of an Italian COVID-19 forefront hospital. BMC Pulm. Med. 2020, 20, 203. [Google Scholar] [CrossRef] [PubMed]
- Lahner, E.; Dilaghi, E.; Prestigiacomo, C.; Alessio, G.; Marcellini, L.; Simmaco, M.; Santino, I.; Orsi, G.B.; Anibaldi, P.; Marcolongo, A.; et al. Prevalence of Sars-Cov-2 infection in health workers (HWs) and diagnostic test performance: The experience of a teaching hospital in central Italy. Int. J. Environ. Res. Public Health 2020, 17, 4417. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7345358/ (accessed on 24 November 2020). [CrossRef] [PubMed]
- Lackermair, K.; William, F.; Grzanna, N.; Lehmann, E.; Fichtner, S.; Kucher, H.B.; Wilhelm, K.; Estner, H. Infection with SARS-CoV-2 in primary care health care workers assessed by antibody testing. Fam. Pract. 2020, 38, 76–79. Available online: https://europepmc.org/article/med/32766704 (accessed on 24 November 2020). [CrossRef]
- Iversen, K.; Bundgaard, H.; Hasselbalch, R.B.; Kristensen, J.H.; Nielsen, P.B.; Pries-Heje, M.; Knudsen, A.D.; Christensen, C.E.; Fogh, K.; Norsk, J.B.; et al. Risk of COVID-19 in health-care workers in Denmark: An observational cohort study. Lancet Infect. Dis. 2020, 20, 1401–1408. Available online: https://read.qxmd.com/read/32758438/risk-of-covid-19-in-health-care-workers-in-denmark-an-observational-cohort-study (accessed on 24 November 2020). [CrossRef]
- Sikkema, R.S.; Pas, S.D.; Nieuwenhuijse, D.F.; O’Toole, Á.; Verweij, J.; van der Linden, A.; Chestakova, I.; Schapendonk, C.; Pronk, M.; Lexmond, P.; et al. COVID-19 in health-care workers in three hospitals in the south of the Netherlands: A cross-sectional study. Lancet Infect. Dis. 2020, 20, 1273–1280. [Google Scholar] [CrossRef]
- Garcia-Basteiro, A.L.; Moncunill, G.; Tortajada, M.; Vidal, M.; Guinovart, C.; Jiménez, A.; Santano, R.; Sanz, S.; Mendez, S.; Llupia, A.; et al. Seroprevalence of antibodies against SARS-CoV-2 among health care workers in a large Spanish reference hospital. Nat. Commun. 2020, 11, 3500. [Google Scholar] [CrossRef] [PubMed]
- Jeremias, A.; Nguyen, J.; Levine, J.; Pollack, S.; Engellenner, W.; Thakore, A.; Lucore, C. Prevalence of SARS-CoV-2 infection among health care workers in a tertiary community hospital. JAMA Intern. Med. 2020, 180, 1707–1709. Available online: https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2769442 (accessed on 24 November 2020). [CrossRef] [PubMed]
- Barrett, E.S.; Horton, D.B.; Roy, J.; Gennaro, M.L.; Brooks, A.; Tischfield, J.; Greenberg, P.; Andrews, T.; Jagpal, S.; Reilly, N.; et al. Prevalence of SARS-CoV-2 infection in previously undiagnosed health care workers at the onset of the U.S. COVID-19 epidemic. medRxiv 2020. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7276027/ (accessed on 24 November 2020).
- Vahidy, F.S.; Bernard, D.W.; Boom, M.L.; Drews, A.L.; Christensen, P.; Finkelstein, J.; Schwartz, R. Prevalence of SARS-CoV-2 infection among asymptomatic health care workers in the greater Houston, Texas, Area. JAMA Netw. Open. 2020, 3, e2016451. [Google Scholar] [CrossRef]
- Chen, Y.; Tong, X.; Wang, J.; Huang, W.; Yin, S.; Huang, R.; Yang, H.; Chen, Y.; Huang, A.; Liu, Y.; et al. High SARS-CoV-2 antibody prevalence among healthcare workers exposed to COVID-19 patients. J. Infect. 2020, 81, 420–426. [Google Scholar] [CrossRef]
- Unoki, T.; Sakuramoto, H.; Sato, R.; Ouchi, A.; Kuribara, T.; Furumaya, T.; Tatsuno, J.; Wakabayashi, Y.; Tado, A.; Hashimoto, N.; et al. Adverse effects of personal protective equipment among intensive care unit healthcare professionals during the COVID-19 pandemic: A scoping review. SAGE Open Nurs. 2021, 6, 1–14. [Google Scholar] [CrossRef]
- Debisarun, P.A.; Struycken, P.; Domínguez-Andrés, J.; Moorlag, S.J.C.F.M.; Taks, E.; Gössling, K.L.; Ostermann, P.N.; Muller, L.; Schaal, H.; Oever, J.; et al. The effect of influenza vaccination on trained immunity: Impact on COVID-19. medRxiv 2020. [Google Scholar] [CrossRef]
- Amato, M.; Werba, J.P.; Frigerio, B.; Coggi, D.; Sansaro, D.; Ravani, A.; Ferrante, P.; Veglia, F.; Tremoli, E.; Baldassarre, D. Relationship between Influenza vaccination coverage rate and COVID-19 outbreak: An italian ecological study. Vaccines 2020, 8, 535. [Google Scholar] [CrossRef]
- Zanettini, C.; Omar, M.; Dinalankara, W.; Imada, E.L.; Colantuoni, E.; Parmigiani, G.; Marchionni, L. Influenza vaccination and COVID19 mortality in the USA. medRxiv 2020. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7325191/ (accessed on 15 November 2020).
- Petrillo, F.; Pignataro, D.; Lavano, M.A.; Santella, B.; Folliero, V.; Zannella, C.; Astarita, C.; Gagliano, C.; Franci, G.; Avitabile, T.; et al. Current evidence on the ocular surface microbiota and related diseases. Microorganisms 2020, 8, 1033. [Google Scholar] [CrossRef] [PubMed]
- Tré-Hardy, M.; Wilmet, A.; Beukinga, I.; Dogné, J.-M.; Douxfils, J.; Blairon, L. Validation of a chemiluminescent assay for specific SARS-CoV-2 antibody. Clin. Chem. Lab. Med. 2020, 58, 1357–1364. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Overall, N = 235 | PCR or Immunoassay | p-Value 2 | ||
|---|---|---|---|---|
| Negative, N = 145 1 | Positive, N = 90 1 | |||
| Function | 0.3 | |||
| Nurse | 166 (71%) | 98 (68%) | 68 (76%) | |
| Paramedical | 26 (11%) | 17 (12%) | 9 (10%) | |
| Physician | 19 (8.1%) | 11 (7.6%) | 8 (8.9%) | |
| Technician | 24 (10%) | 19 (13%) | 5 (5.6%) | |
| Age class | 0.3 | |||
| <29 years | 64 (27%) | 40 (28%) | 24 (27%) | |
| >60 years | 6 (2.6%) | 5 (3.4%) | 1 (1.1%) | |
| 30–39 years | 72 (31%) | 43 (30%) | 29 (32%) | |
| 40–49 years | 53 (23%) | 37 (26%) | 16 (18%) | |
| 50–59 years | 40 (17%) | 20 (14%) | 20 (22%) | |
| BMI | 24.3 (21.5, 27.8) | 24.2 (21.6, 27.8) | 24.7 (21.5, 28.0) | 0.6 |
| Sex | 0.012 | |||
| Female | 182 (77%) | 104 (72%) | 78 (87%) | |
| Male | 53 (23%) | 41 (28%) | 12 (13%) | |
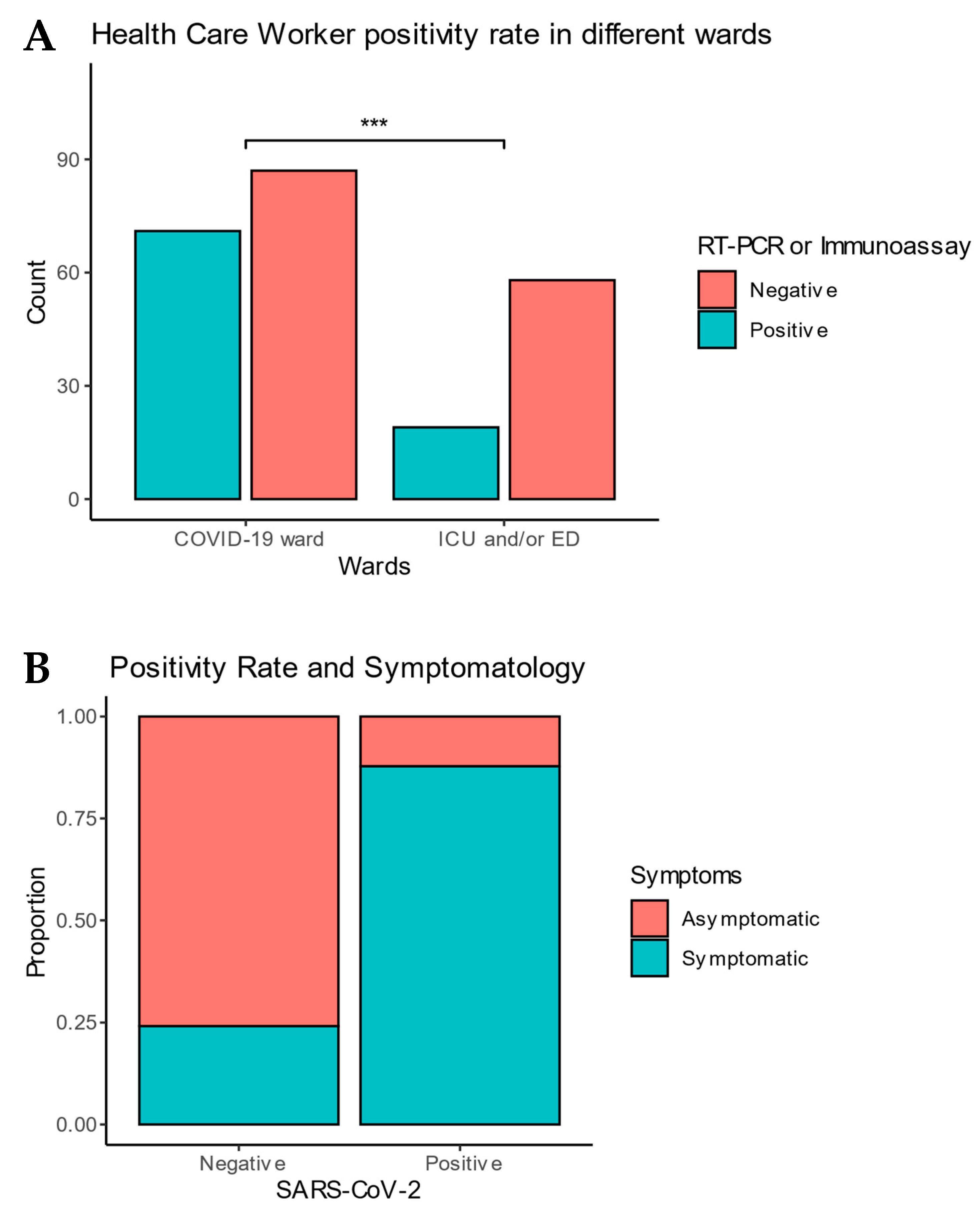
| Ward | 0.004 | |||
| COVID-19 ward | 158 (67%) | 87 (60%) | 71 (79%) | |
| ICU and/or ED | 77 (33%) | 58 (40%) | 19 (21%) | |
| Contact risk | 0.038 | |||
| High Risk | 195 (88%) | 112 (84%) | 83 (94%) | |
| Low Risk | 26 (12%) | 21 (16%) | 5 (5.7%) | |
| Respect of social distancing at work | 0.6 | |||
| Not respected | 11 (4.7%) | 7 (4.8%) | 4 (4.5%) | |
| Partly respected | 80 (34%) | 46 (32%) | 34 (39%) | |
| Well respected | 142 (61%) | 92 (63%) | 50 (57%) | |
| Respect of social distancing outside work | 0.5 | |||
| Not respected | 2 (0.9%) | 2 (1.4%) | 0 (0%) | |
| Partly respected | 14 (6.0%) | 10 (7.0%) | 4 (4.4%) | |
| Well respected | 217 (93%) | 131 (92%) | 86 (96%) | |
| Symptoms | 114 (49%) | 35 (24%) | 79 (88%) | <0.001 |
| Fever | 51 (22%) | 13 (9.0%) | 38 (42%) | <0.001 |
| Dyspnea | 38 (16%) | 10 (6.9%) | 28 (31%) | <0.001 |
| Flu-like symptoms | 93 (40%) | 27 (19%) | 66 (73%) | <0.001 |
| Respiratory symptoms | 62 (26%) | 16 (11%) | 46 (51%) | <0.001 |
| ENT 3 symptoms | 72 (31%) | 10 (6.9%) | 62 (69%) | <0.001 |
| Abdominal discomfort | 43 (18%) | 11 (7.6%) | 32 (36%) | <0.001 |
| Skin lesions | 10 (4.3%) | 3 (2.1%) | 7 (7.8%) | 0.047 |
| Influenza vaccination 2019 | 52 (22%) | 30 (21%) | 22 (24%) | 0.6 |
| Thorax Tomodensitometry | 20 (8.5%) | 7 (4.8%) | 13 (14%) | 0.020 |
| Pulmonary lesions on TDM | 10 (50%) | 0 (0%) | 10 (77%) | 0.003 |
| qRT-PCR testing | 76 (32%) | 29 (20%) | 47 (52%) | NA |
| Immunoassay testing | 226 (96%) | 139 (96%) | 87 (97%) | NA |
| Hospitalization | 5 (4.5%) | 0 (0%) | 5 (6.2%) | 0.3 |
| Work absenteeism | 74 (37%) | 17 (15%) | 57 (66%) | <0.001 |
| OR 1 | 95% CI 1 | p-Value | |
|---|---|---|---|
| Symptoms | |||
| Asymptomatic | — | — | |
| Symptomatic | 23.3 | 11.1, 53.1 | <0.001 |
| Risk | |||
| Low Risk (reference level) | — | — | |
| High Risk | 3.08 | 0.89, 11.9 | 0.085 |
| Ward | |||
| ICU and/or ED (reference level) | — | — | |
| COVID-19 ward | 3.25 | 1.50, 7.28 | 0.003 |
| Author Hospital Country | Hospital and Country | Studied Population | Detection Method | Reported Positivity Rate | Additional Findings |
|---|---|---|---|---|---|
| Martin et al. [3] | Saint Pierre Hospital Belgium | N = 326 HCWs from COVID-19, ED, ICU wards | RT-PCR and Immunoassay | 12.6% | Screening of all groups of HCWs in highly exposed COVID-19 units is recommended. |
| Blairon et al. [4] | Reseau IRIS Belgium | N = 3145 hospital staff from COVID-19 and COVID-19 free wards | RT-PCR and Immunoassay | 14.6% | |
| Paderno et al. [5] | Italy (Northern Italy) | N = 58 from a otolaryngology unit | RT-PCR if symptoms and Immunoassay if absence of symptoms | 9% | The prevalent risk of infection was related to extrahospital contacts |
| Sotgiu et al. [8] | Italy (Milan) | N = 202 HCWs from COVID-19 wards | Immunoassay (IgM, IgG) | IgM: 14.4% IgG: 7.41% | IgM are higher in the age group 20–29 and 60–69 |
| Lahner et al. [9] | Italy (Rome) | N = 2057 HCWs from a COVID-19 regional hub during the pandemic | RT-PCR and Immunoassay (IgM, IgG) | RT-PCR: 2.7% IgM: 0% IgG: 0.7% | Seroprevalence is higher in HCW than general population; IgM seems not to be useful test for active Sars-Cov-2infection |
| Korth et al. [6] | Germany | N = 316: HCWs with direct contact with COVID-19 confirmed patients | Immunoassay | 1.6% | Good local hygiene standard |
| Lackermair et al. [10] | Germany | N = 151 HCWs | Immunoassay | 2.6% | |
| Kasper Iversen et al. [11] | Denmark (Capital region) | N = 29117 HCWs including students | Immunoassay (IgM, IgG) | 4.04% | Comparison with a blood donor group with positivity rate was inferior |
| Sikkema et al. [12] | Netherlands (from 9 hospitals) | N = 1796 symptomatic HCWs | RT-PCR | 5% | |
| Garcia-Basteiro et al. [13] | Spain | N = 578 HCWs from COVID-19 wards and COVID-19-free wards | Immunoassay (IgM, IgG, IgA) | 9.3% | IgA demonstrating the highest sensitivity in the initial days after symptoms onset |
| Mansour et al. [7] | USA (NYC) | N = 285 HCWs with high risk with contacts and aerosols | Immunoassay | 36% | |
| Jeremias et al. [14] | USA (NYC) | N = 3046 HCWs | RT-PCR if symptoms and Immunoassay without symptoms | 9.8% | PPE confers protection and lower infection rates of COVID-19 among HCWs |
| Barret et al. [15] | USA | N = 546 HCWs and N = 283 non HCWs | RT-PCR | HCWs: 7.3% Non HCWs: 0.4% | Comparison HCWs with non-HCWs |
| Vahidy et al. [16] | USA (Texas) | N = 2787 HCWs and non-clinical workers from COVID-19 wards and COVID-19-free wards | RT-PCR | Total: 3.9% COVID-19 wards: 5.4%; COVID-19-free wards: 0.6% | |
| Chen et al. [17] | China | N = 105 HCWs exposed to confirmed COVID-19 patients | Immunoassays | 17.1% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kapuczinski, A.; de Terwangne, C.; De Keukeleire, S.; Goffard, J.-C.; Sorgente, A.; Place, S.; De Cubber, M. Exposure to SARS-CoV-2 in Hospital Environment: Working in a COVID-19 Ward Is a Risk Factor for Infection. Pathogens 2021, 10, 1175. https://doi.org/10.3390/pathogens10091175
Kapuczinski A, de Terwangne C, De Keukeleire S, Goffard J-C, Sorgente A, Place S, De Cubber M. Exposure to SARS-CoV-2 in Hospital Environment: Working in a COVID-19 Ward Is a Risk Factor for Infection. Pathogens. 2021; 10(9):1175. https://doi.org/10.3390/pathogens10091175
Chicago/Turabian StyleKapuczinski, Abeline, Christophe de Terwangne, Steven De Keukeleire, Jean-Christophe Goffard, Antonio Sorgente, Sammy Place, and Michael De Cubber. 2021. "Exposure to SARS-CoV-2 in Hospital Environment: Working in a COVID-19 Ward Is a Risk Factor for Infection" Pathogens 10, no. 9: 1175. https://doi.org/10.3390/pathogens10091175
APA StyleKapuczinski, A., de Terwangne, C., De Keukeleire, S., Goffard, J.-C., Sorgente, A., Place, S., & De Cubber, M. (2021). Exposure to SARS-CoV-2 in Hospital Environment: Working in a COVID-19 Ward Is a Risk Factor for Infection. Pathogens, 10(9), 1175. https://doi.org/10.3390/pathogens10091175