
Evaluation of the Chagas Western Blot IgG Assay for the Diagnosis of Chagas Disease

 and
and
Abstract
1. Introduction
2. Results
2.1. Patients’ Characteristics
2.2. Performance of the Chagas Western Blot IgG Assay® in Comparaison with Two Other Commercial Assays
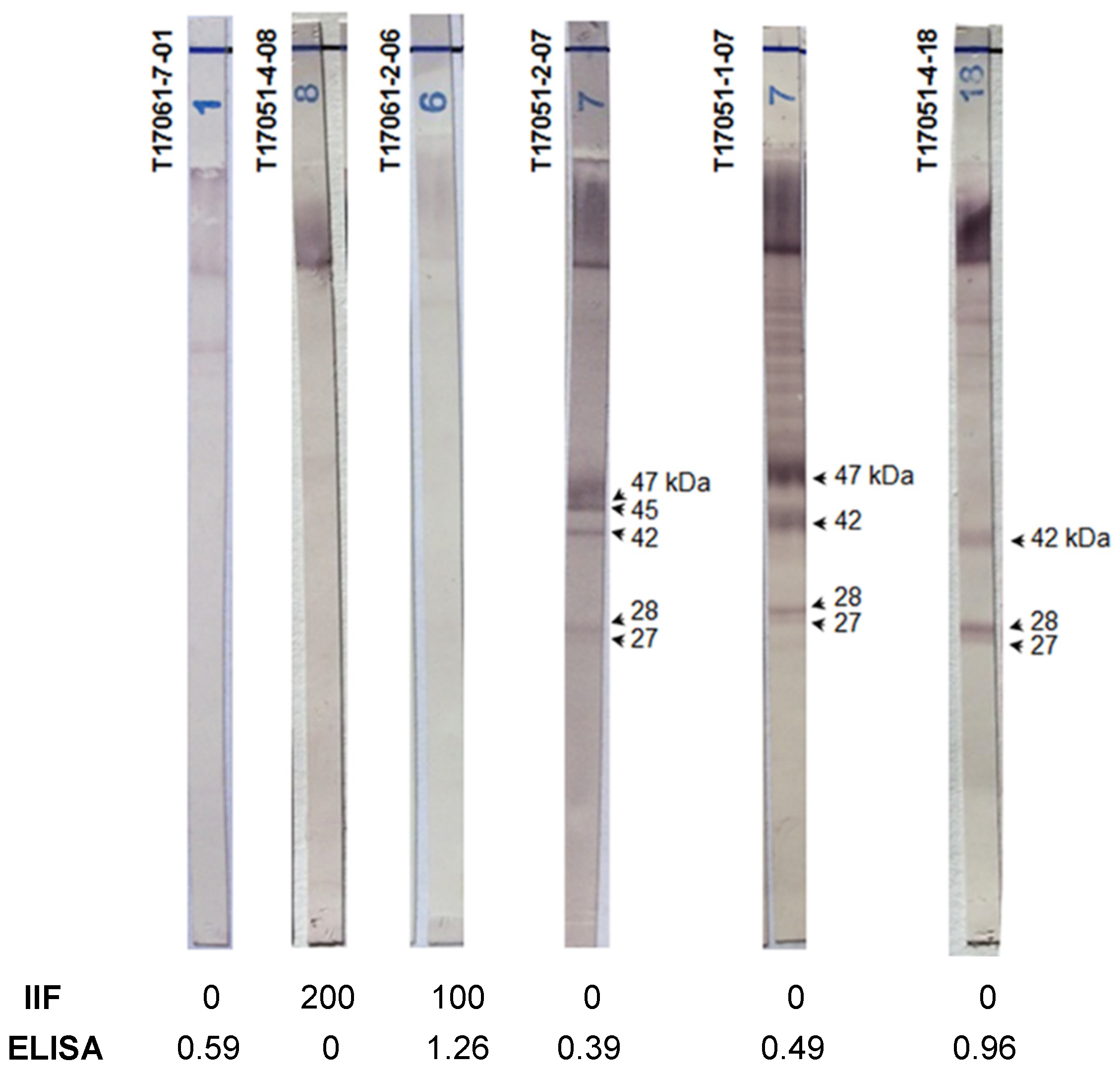
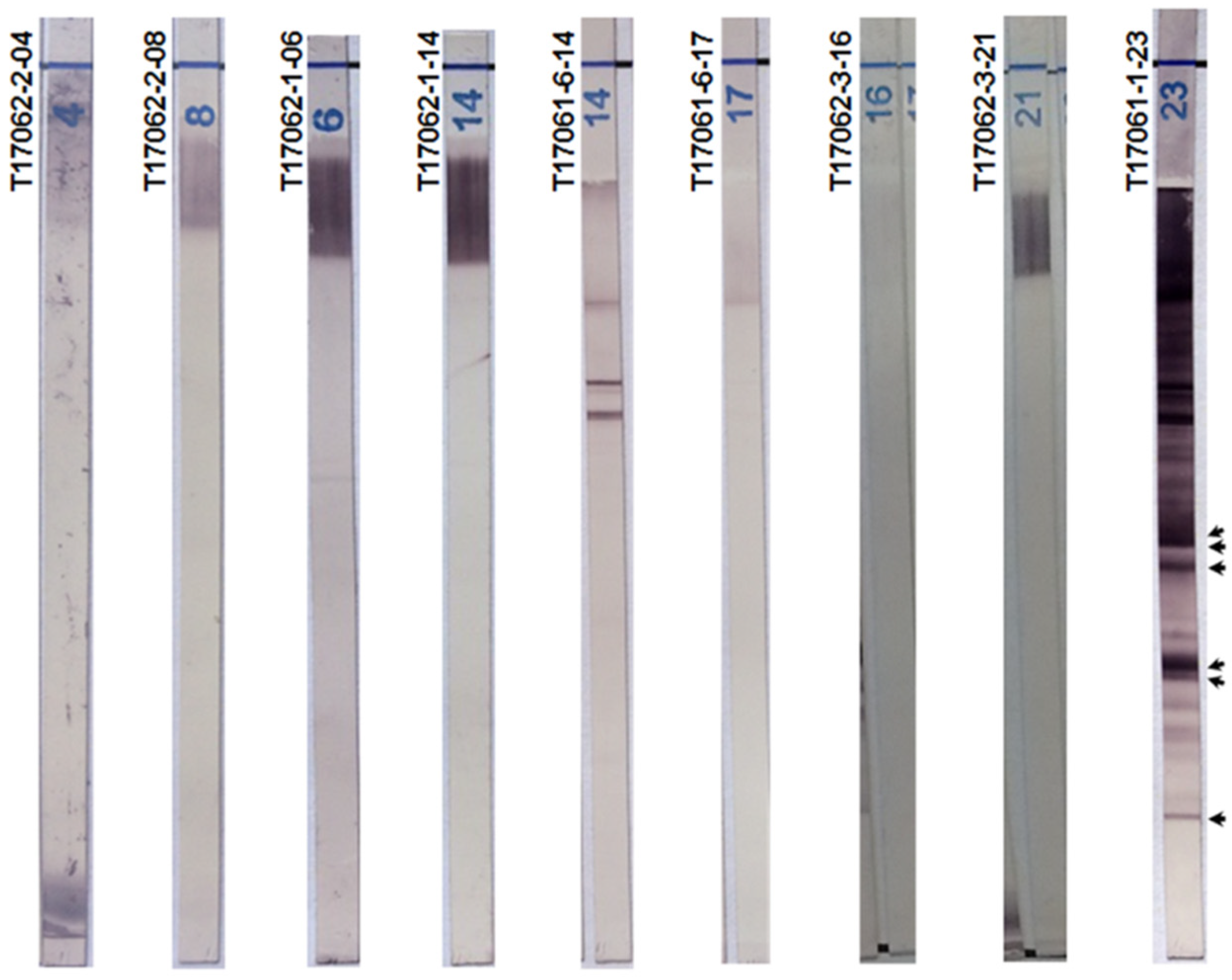
2.3. The Chagas Blot on Serum with Discordant Serological Results
2.4. Chagas Blot Performed on Sera from Newborns
2.5. Chagas Blot Performed on Sera with Other Parasitic Diseases
3. Discussion
4. Materials and Methods
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| IHA | Hemagglutination |
| IIF | Indirect Immunofluorescence |
| EIA | Enzyme Immunoassay |
| ELISA | Enzyme-Linked Immunosorbent Assay |
| WHO | World Health Organization, |
| NBT-BCIP | Nitrotetrazolium blue chloride. 5-bromo-4-chloro-3-indolyl-phosphate-p-toluidine salt |
| DTU | Discrete Typing Unit |
Appendix A
- Criteria for sample positivity
- Sensitivity and specificity
References
- Medone, P.; Ceccarelli, S.; Parham, P.E.; Figuera, A.; Rabinovich, J.E. The impact of climate change on the geographical distribution of two vectors of Chagas disease: Implications for the force of infection. Philos. Trans. R. Soc. B Biol. Sci. 2015, 370, 20130560. [Google Scholar] [CrossRef]
- Garza, M.; Arroyo, T.P.F.; Casillas, E.A.; Sanchez-Cordero, V.; Rivaldi, C.-L.; Sarkar, S. Projected future distributions of vectors of Trypanosoma cruzi in North America under climate change scenarios. PLoS Negl. Trop. Dis. 2014, 8, e2818. [Google Scholar] [CrossRef] [PubMed]
- WHO Expert Committee on the Control of Chagas Disease. Control of Chagas Disease: Second Report of the WHO Expert Committee; World Health Organization: Geneva, Switzerland, 2002; p. 109. Available online: https://apps.who.int/iris/handle/10665/42443 (accessed on 28 April 2018).
- Daltro, R.T.; Leony, L.M.; Freitas, N.; Silva, A.O.; Santos, E.F.; Del-Rei, R.P.; Brito, M.E.F.; Filho, S.B.; Gomes, Y.M.; Silva, M.S.; et al. Cross-Reactivity Using Chimeric Trypanosoma cruzi Antigens: Diagnostic Performance in Settings Where Chagas Disease and American Cutaneous or Visceral Leishmaniasis Are Coendemic. J. Clin. Microbiol. 2019, 57, e00762-19. [Google Scholar] [CrossRef]
- Pérez-Molina, J.A.; Molina, I. Chagas disease cardiomyopathy treatment remains a challenge—Authors’ reply. Lancet 2018, 391, 2209–2210. [Google Scholar] [CrossRef]
- Kirchhoff, L.V.; Paredes, P.; Lomelí-Guerrero, A.; Paredes-Espinoza, M.; Ron-Guerrero, C.S.; Delgado-Mejía, M.; Peña-Muñoz, J.G. Transfusion-associated Chagas disease (American trypanosomiasis) in Mexico: Implications for transfusion medicine in the United States. Transfusion 2006, 46, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Bryan, C.F.; Tegtmeier, G.E.; Rafik, N.; Markham, L.E.; Murillo, D.; Nelson, P.W.; Shield, C.F., III; Warady, B.A.; Aeder, M.I. The risk for Chagas’ disease in the Midwestern United States organ donor population is low. Clin. Transpl. 2004, 18, 12–15. [Google Scholar] [CrossRef] [PubMed]
- de Pereira, G.A.; Louzada-Neto, F.; de Barbosa, V.F.; Ferreira-Silva, M.M.; de Moraes-Souza, H. Performance of six diagnostic tests to screen for Chagas disease in blood banks andprevalence of Trypanosoma cruzi infection among donors with inconclusive serologyscreening based on the analysis of epidemiological variables. Rev. Bras. Hematol. Hemoter. 2012, 34, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Camargo, C.L.; Albajar-Viñas, P.; Wilkins, P.P.; Nieto, J.; Leiby, D.A.; Paris, L.; Scollo, K.; Flórez, C.; Guzmán-Bracho, C.; Luquetti, A.O.; et al. Comparative evaluation of 11 commercialized rapid diagnostic tests for detecting Trypanosoma cruzi antibodies in serum banks in areas of endemicity and nonendemicity. J. Clin. Microbiol. 2014, 52, 2506–2512. [Google Scholar] [CrossRef]
- Afonso, A.M.; Ebell, M.H.; Tarleton, R. A systematic review of high quality diagnostic tests for Chagas disease. PLoS Negl. Trop. Dis. 2012, 6, e1881. [Google Scholar] [CrossRef]
- Brasil, P.E.A.A.D.; Castro, R.; de Castro, L. Commercial enzyme-linked immunosorbent assay versuspolymerase chain reaction for the diagnosis of chronic Chagas disease: A systematic review and meta-analysis. Memórias do Instituto Oswaldo Cruz 2016, 111, 1–19. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Anti-Trypanosoma Cruzi Assays: Operational Characteristics, Report 1; World Health Organization: Geneva, Switzerland, 2010; Available online: https://apps.who.int/iris/handle/10665/75844 (accessed on 28 April 2018).
- Assal, A.; Corbi, C. Chagas disease and blood transfusion: An emerging issue in non-endemic countries. Transfus. Clin. Biol. J. Soc. Fr. Transfus. Sang. 2011, 18, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Moya-Salazar, J.; Ubidia-Incio, R.; Incio-Grande, M.; Blejer, J.L.; Gonzalez, C.A. Seroprevalence, cost per donation and reduction in blood supply due to positive and indeterminate results for infectious markers in a blood bank in Lima, Peru. Rev. Bras. Hematol. Hemoter. 2017, 39, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Gil-Gallardo, L.; Simón, M.; Iborra, M.; Carrilero, B.; Segovia, M. Chemiluminescent Microparticle Immunoassay for the Diagnosis of Congenital Chagas Disease: A Prospective Study in Spain. Am. J. Trop. Med. Hyg. 2021. [Google Scholar] [CrossRef] [PubMed]
- Abras, A.; Ballart, C.; Fernández-Arévalo, A.; Llovet, T.; Gállego, M.; Muñoz, C. ARCHITECT Chagas® as a single test candidate for Chagas disease diagnosis: Evaluation of two algorithms implemented in a non-endemic setting (Barcelona, Spain). Clin. Microbiol. Infect. 2020, 27, 782.e1–782.e6. [Google Scholar] [CrossRef] [PubMed]
- Flores-Chavez, M.D.; Sambri, V.; Schottstedt, V.; Higuera-Escalante, F.A.; Roessler, D.; Chaves, M.; Laengin, T.; Martinez, A.; Fleischer, B. Evaluation of the Elecsys Chagas Assay for Detection of Trypanosoma cruzi-Specific Antibodies in a Multicenter Study in Europe and Latin America. J. Clin. Microbiol. 2018, 56, e01446-17. [Google Scholar] [CrossRef]
- Pérez-Ayala, A.; Fradejas, I.; Rebollo, L.; Lora-Pablos, D.; Lizasoain, M.; Herrero-Martínez, J.M. Usefulness of the ARCHITECT Chagas(®) assay as a single test for the diagnosis of chronic Chagas disease. Trop. Med. Int. Health 2018, 23, 634–640. [Google Scholar] [CrossRef]
- Duarte, L.F.; Flórez, O.; Rincón, G.; González, C.I. Comparison of seven diagnostic tests to detect Trypanosoma cruzi infection in patients in chronic phase of Chagas disease. Colomb. Médica 2014, 45, 61–66. [Google Scholar] [CrossRef]
- Araújo, A.B.; Berne, M.E.A. Conventional serological performance in diagnosis of Chagas’ disease in southern Brazil. Braz. J. Infect. Dis. 2013, 17, 174–178. [Google Scholar] [CrossRef]
- Mendes, R.P.; Hoshino-Shimizu, S.; da Moura Silva, A.M.; Mota, I.; Heredia, R.A.; Luquetti, A.O.; Leser, P.G. Serological diagnosis of Chagas’ disease: A potential confirmatory assay using preserved protein antigens of Trypanosoma cruzi. J. Clin. Microbiol. 1997, 35, 1829–1834. [Google Scholar] [CrossRef]
- Berrizbeitia, M.; Ndao, M.; Bubis, J.; Gottschalk, M.; Aché, A.; Lacouture, S.; Medina, M.; Ward, B.J. Purified excreted-secreted antigens from Trypanosoma cruzi trypomastigotes as tools for diagnosis of Chagas’ disease. J. Clin. Microbiol. 2006, 44, 291–296. [Google Scholar] [CrossRef]
- Umezawa, E.S.; Nascimento, M.S.; Kesper, N., Jr.; Coura, J.R.; Borges-Pereira, J.; Junqueira, A.C.; Camargo, M.E. Immunoblot assay using excreted-secreted antigens of Trypanosoma cruzi in serodiagnosis of congenital, acute, and chronic Chagas’ disease. J. Clin. Microbiol. 1996, 34, 2143–2147. [Google Scholar] [CrossRef] [PubMed]
- Silveira-Lacerda, E.P.; Silva, A.G.; Junior, S.F.; Souza, M.A.; Kesper, N.; Botelho-Filho, A.; Umezawa, E.S. Chagas’ disease: Application of TESA-blot in inconclusive sera from a Brazilian blood bank. Vox Sang. 2004, 87, 204–207. [Google Scholar] [CrossRef]
- Neto, V.A.; De Marchi, C.R.; Ferreira, C.S.; Ferreira, A.W. Observations on the use of TESA blot for the serological diagnosis of Chagas’ disease. Rev. Soc. Bras. Med. Trop. 2005, 38, 534–535. [Google Scholar] [CrossRef]
- Umezawa, E.S.; Bastos, S.F.; Coura, J.R.; Levin, M.J.; Gonzalez, A.; Rangel-Aldao, R.; Zingales, B.; Luquetti, A.O.; Da Silveira, J.F. An improved serodiagnostic test for Chagas’ disease employing a mixture of Trypanosoma cruzi recombinant antigens. Transfusion 2003, 43, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Zarate-Blades, C.R.; Bladés, N.; Nascimento, M.S.; da Silveira, J.F.; Umezawa, E.S. Diagnostic performance of tests based on Trypanosoma cruzi excreted-secreted antigens in an endemic area for Chagas’ disease in Bolivia. Diagn. Microbiol. Infect. Dis. 2007, 57, 229–232. [Google Scholar] [CrossRef] [PubMed]
- Furuchó, C.R.; Umezawa, E.S.; Almeida, I.; Freitas, V.L.; Bezerra, R.; Nunes, E.V.; Sanches, M.C.; Guastini, C.M.; Teixeira, A.R.; Shikanai-Yasuda, M.A. Inconclusive results in conventional serological screening for Chagas’ disease in blood banks: Evaluation of cellular and humoral response. Trop. Med. Int. Health 2008, 13, 1527–1533. [Google Scholar] [CrossRef]
- Moure, Z.; Angheben, A.; Molina, I.; Gobbi, F.; Espasa, M.; Anselmi, M.; Salvador, F.; Tais, S.; Sánchez-Montalvá, A.; Pumarola, T.; et al. Serodiscordance in chronic Chagas disease diagnosis: A real problem in non-endemic countries. Clin. Microbiol. Infect. 2016, 22, 788–792. [Google Scholar] [CrossRef] [PubMed]
- Cheng, K.Y.; Chang, C.-D.; Salbilla, V.A.; Kirchhoff, L.V.; Leiby, D.A.; Schochetman, G.; Shah, D.O. Immunoblot assay using recombinant antigens as a supplemental test to confirm the presence of antibodies to Trypanosoma cruzi. Clin. Vaccine Immunol. 2007, 14, 355–361. [Google Scholar] [CrossRef]
- Praast, G.; Herzogenrath, J.; Bernhardt, S.; Christ, H.; Sickinger, E. Evaluation of the Abbott ARCHITECT Chagas prototype assay. Diagn. Microbiol. Infect. Dis. 2011, 69, 74–81. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Anti-Trypanosoma cruzi Antibodies Detected | Anti-Trypanosoma cruzi Antibodies Not Detected | ||
|---|---|---|---|
| Group | Group 1 | Group 2 | |
| Sample | Serum (N) | 100 | 178 |
| Gender | Male (%) | 24 (24%) | 78 (44%) |
| Female (%) | 73 (73%) | 55 (31%) | |
| Not Available | 3 (03%) | 45 (25%) | |
| Age | Median | 34 years | 37 years |
| Average | 32 years | 38 years | |
| Limits | (1 day–78 years) | (10 months–77 years) | |
| Origin | Endemic areas | Non endemic areas |
| Test | Group 1 (n = 100) | Group 2 (n = 178) | ||
|---|---|---|---|---|
| True Positive | False Negative | True Negative | False Positive | |
| Chagas Western Blot IgG assay | 100 | 0 | 178 | 0 |
| Immunofluor CHAGAS | 95 | 5 | 148 | 30 |
| Chagatest ELISA Recombinante v.4,0 | 99 | 1 | 160 | 18 |
| Test | Sensitivity | Specificity |
|---|---|---|
| n = 100 | n = 178 | |
| (95% CI) | (95% CI) | |
| Chagas Western Blot IgG assay | 100 | 100 |
| (95.3–100) | (97.4–100.0) | |
| Immunofluor CHAGAS | 95.0 | 83.1 |
| (88.2–98.1) | (76.6–88.2) | |
| Chagatest ELISA Recombinante v.4.0 | 99.0 | 91.3 |
| (93.8–100.0) | (85.9–91.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brossas, J.-Y.; Griselda, B.; Bisio, M.; Guihenneuc, J.; Gulin, J.E.N.; Jauréguiberry, S.; Lescure, F.-X.; Fekkar, A.; Mazier, D.; Altcheh, J.; et al. Evaluation of the Chagas Western Blot IgG Assay for the Diagnosis of Chagas Disease. Pathogens 2021, 10, 1455. https://doi.org/10.3390/pathogens10111455
Brossas J-Y, Griselda B, Bisio M, Guihenneuc J, Gulin JEN, Jauréguiberry S, Lescure F-X, Fekkar A, Mazier D, Altcheh J, et al. Evaluation of the Chagas Western Blot IgG Assay for the Diagnosis of Chagas Disease. Pathogens. 2021; 10(11):1455. https://doi.org/10.3390/pathogens10111455
Chicago/Turabian StyleBrossas, Jean-Yves, Ballering Griselda, Margarita Bisio, Jeremy Guihenneuc, Julián Ernesto Nicolás Gulin, Stéphane Jauréguiberry, François-Xavier Lescure, Arnaud Fekkar, Dominique Mazier, Jaime Altcheh, and et al. 2021. "Evaluation of the Chagas Western Blot IgG Assay for the Diagnosis of Chagas Disease" Pathogens 10, no. 11: 1455. https://doi.org/10.3390/pathogens10111455
APA StyleBrossas, J.-Y., Griselda, B., Bisio, M., Guihenneuc, J., Gulin, J. E. N., Jauréguiberry, S., Lescure, F.-X., Fekkar, A., Mazier, D., Altcheh, J., & Paris, L. (2021). Evaluation of the Chagas Western Blot IgG Assay for the Diagnosis of Chagas Disease. Pathogens, 10(11), 1455. https://doi.org/10.3390/pathogens10111455