
Aging Adaptation Transition of Health Care Buildings for Accessibility Optimization for the Elderly


Abstract
1. Introduction
1.1. Backgrounds
1.2. Literature Review
1.3. Objects and Focus
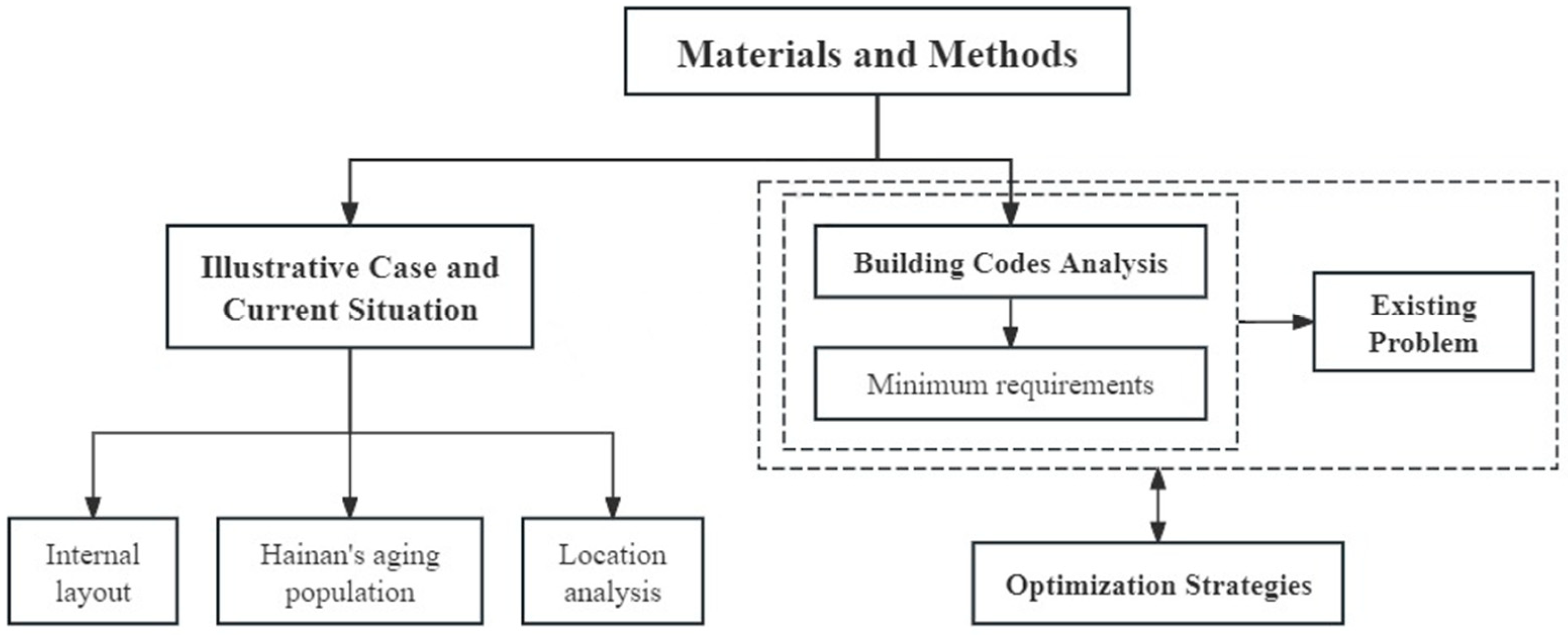
2. Materials and Methods
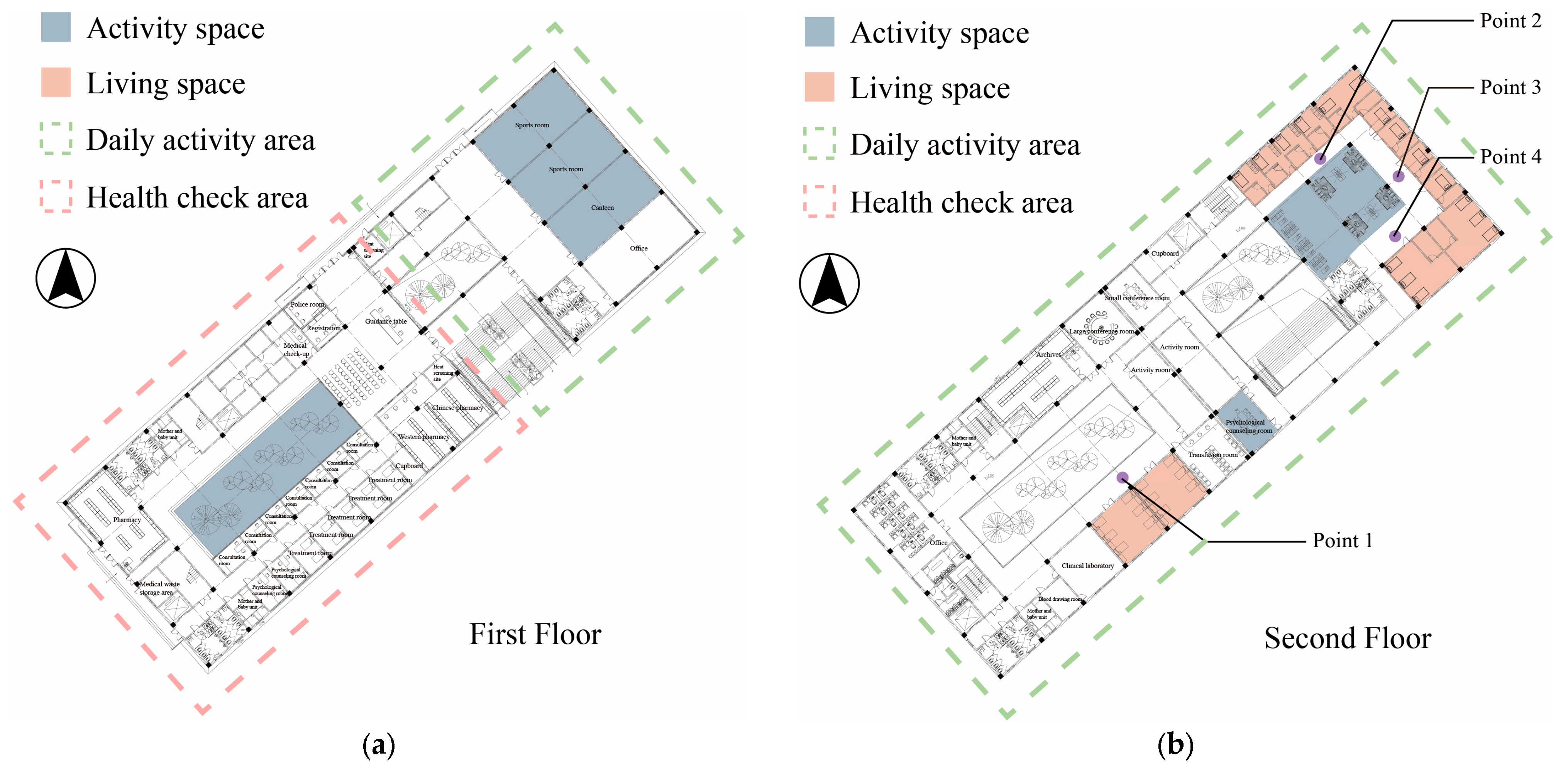
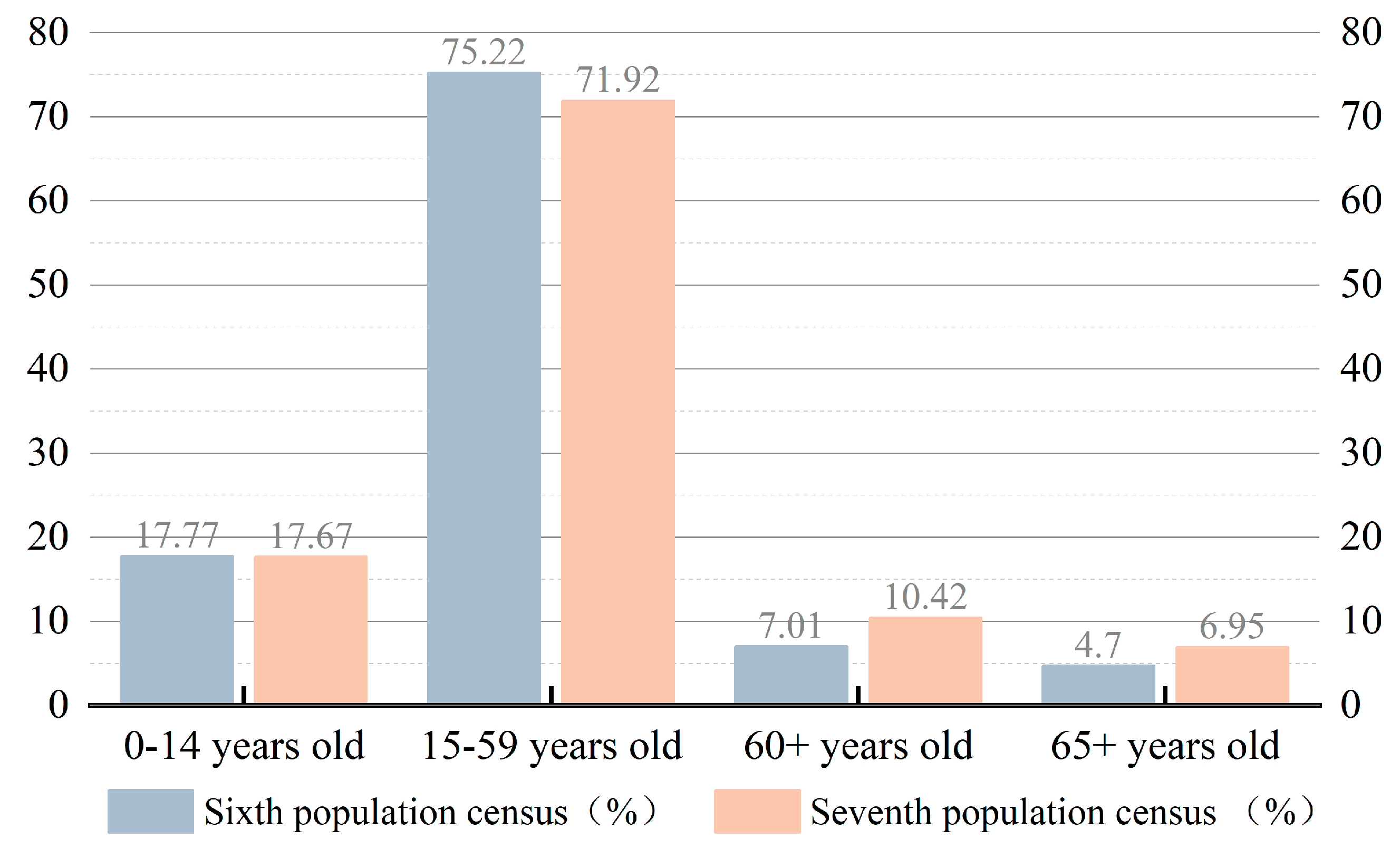
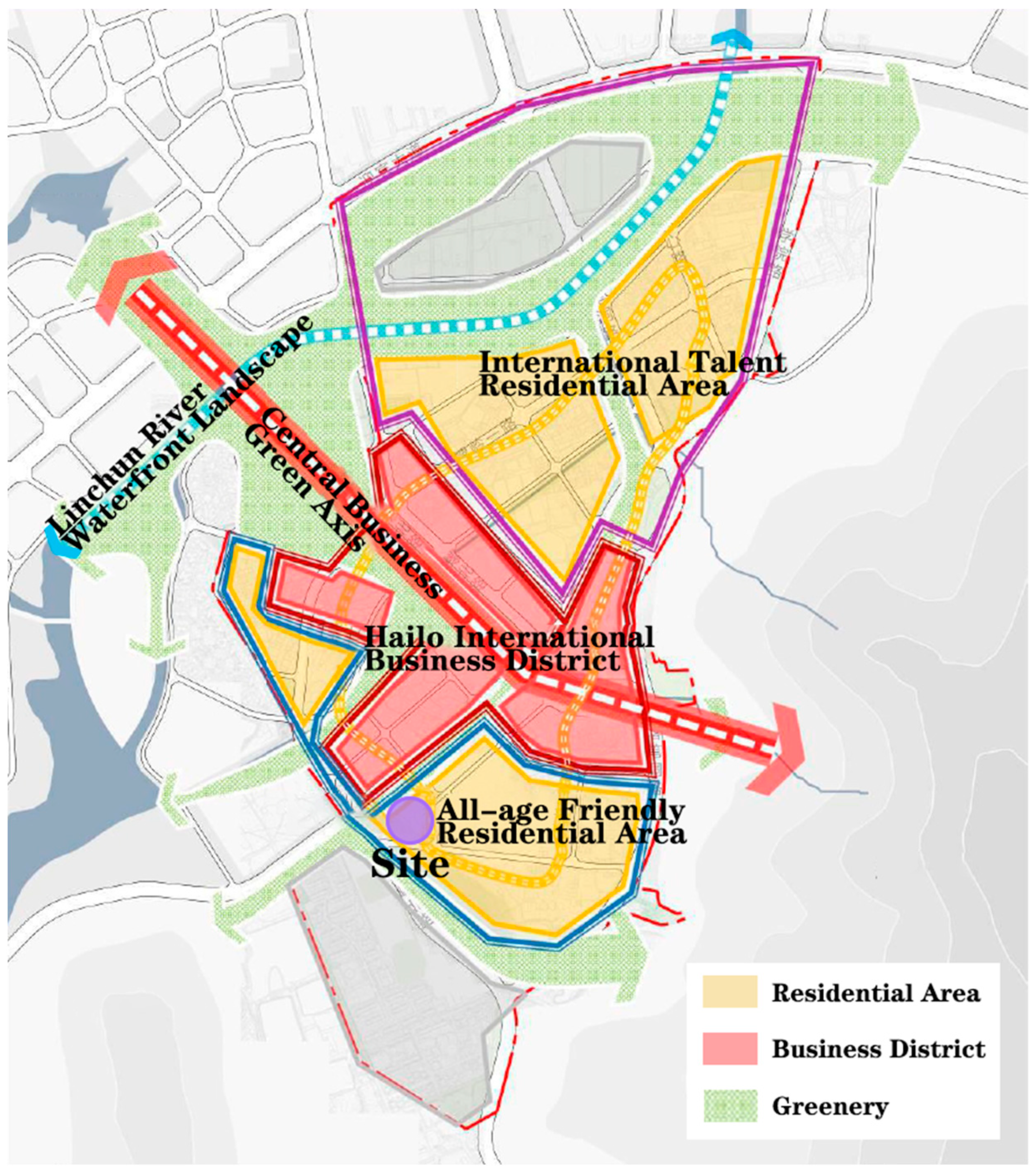
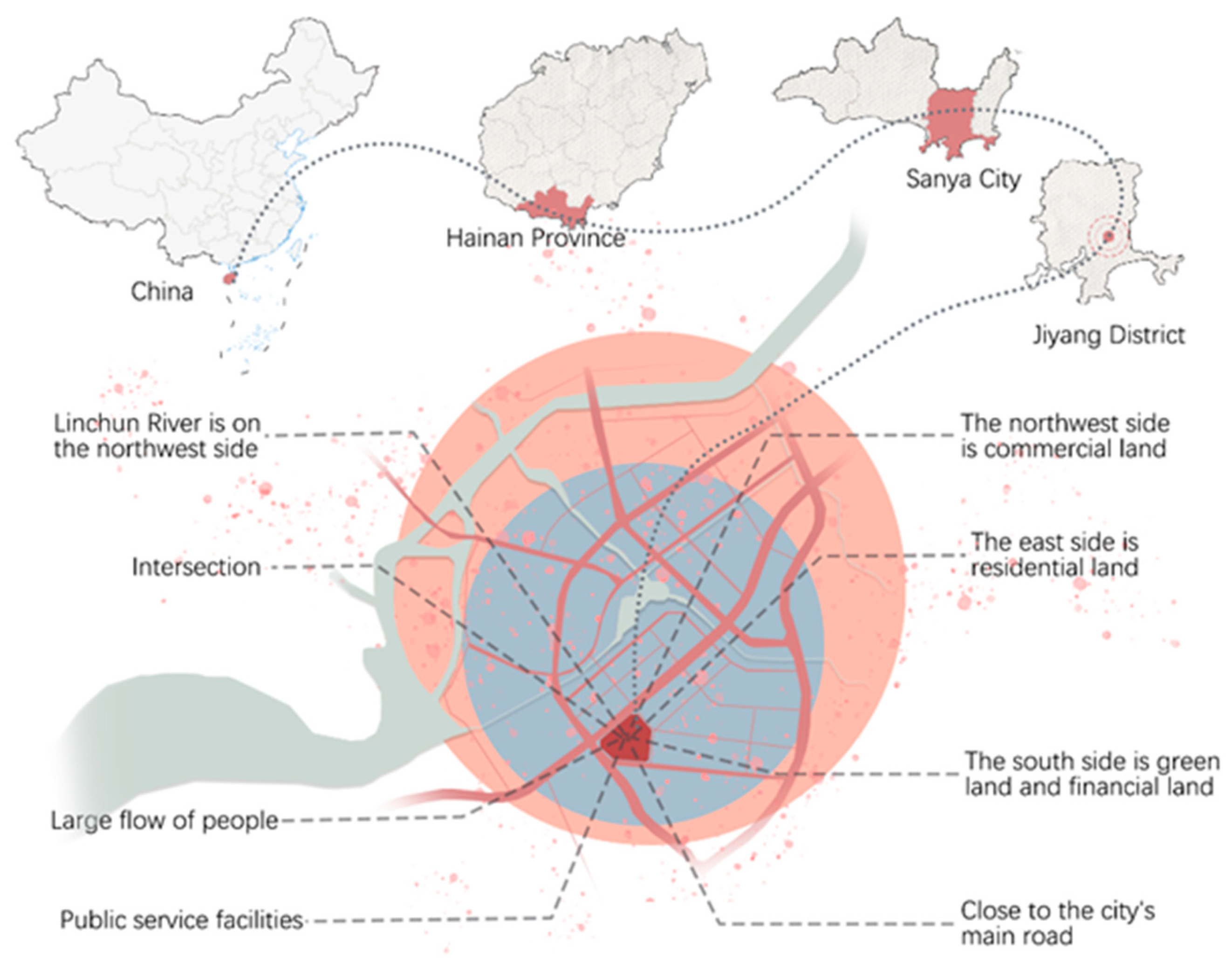
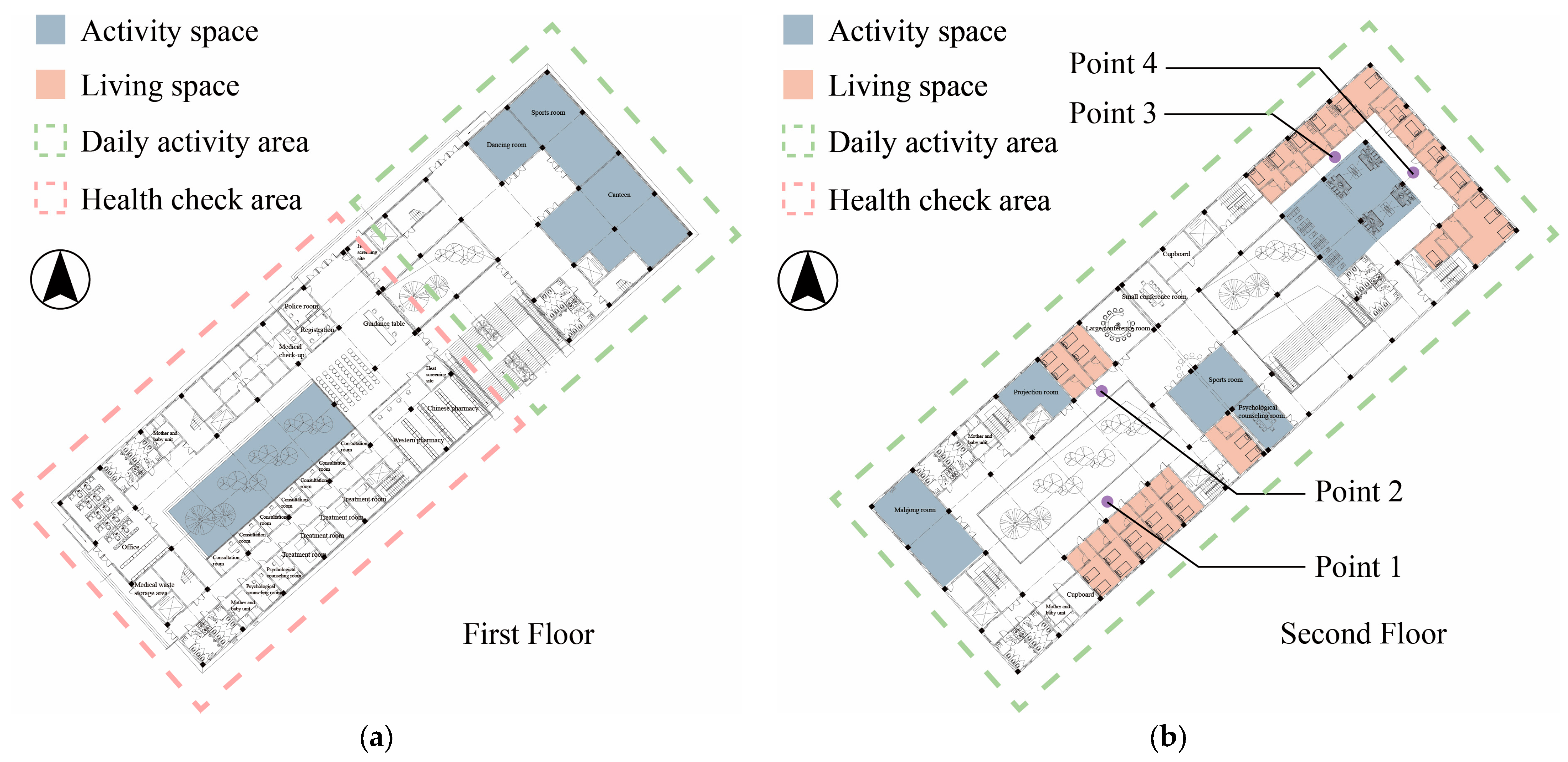
2.1. Illustrative Case and Current Situation
2.2. Building Codes Analysis
2.3. Existing Problem
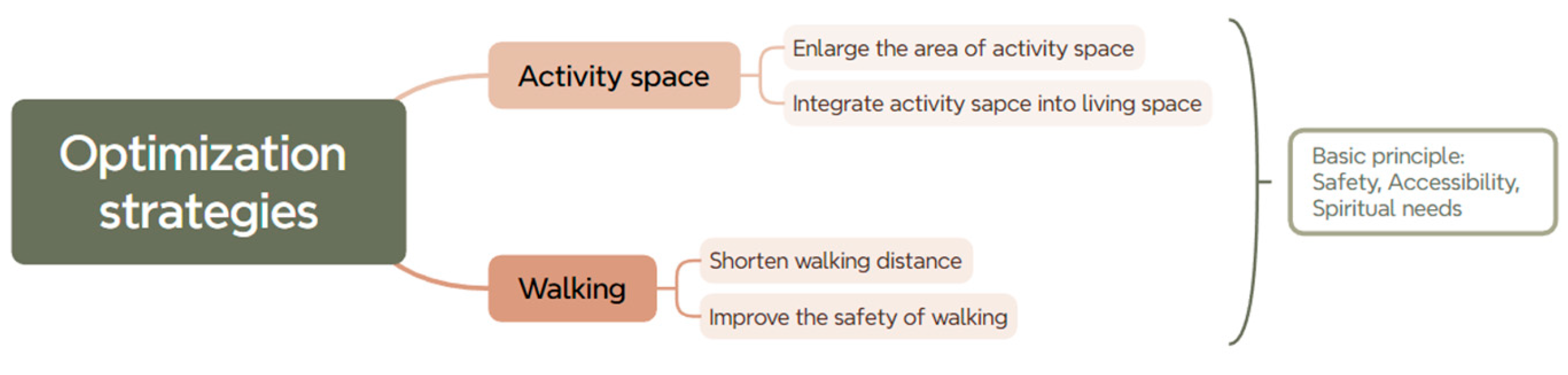
2.4. Optimization Strategies
3. Results and Discussions
3.1. Activity Space
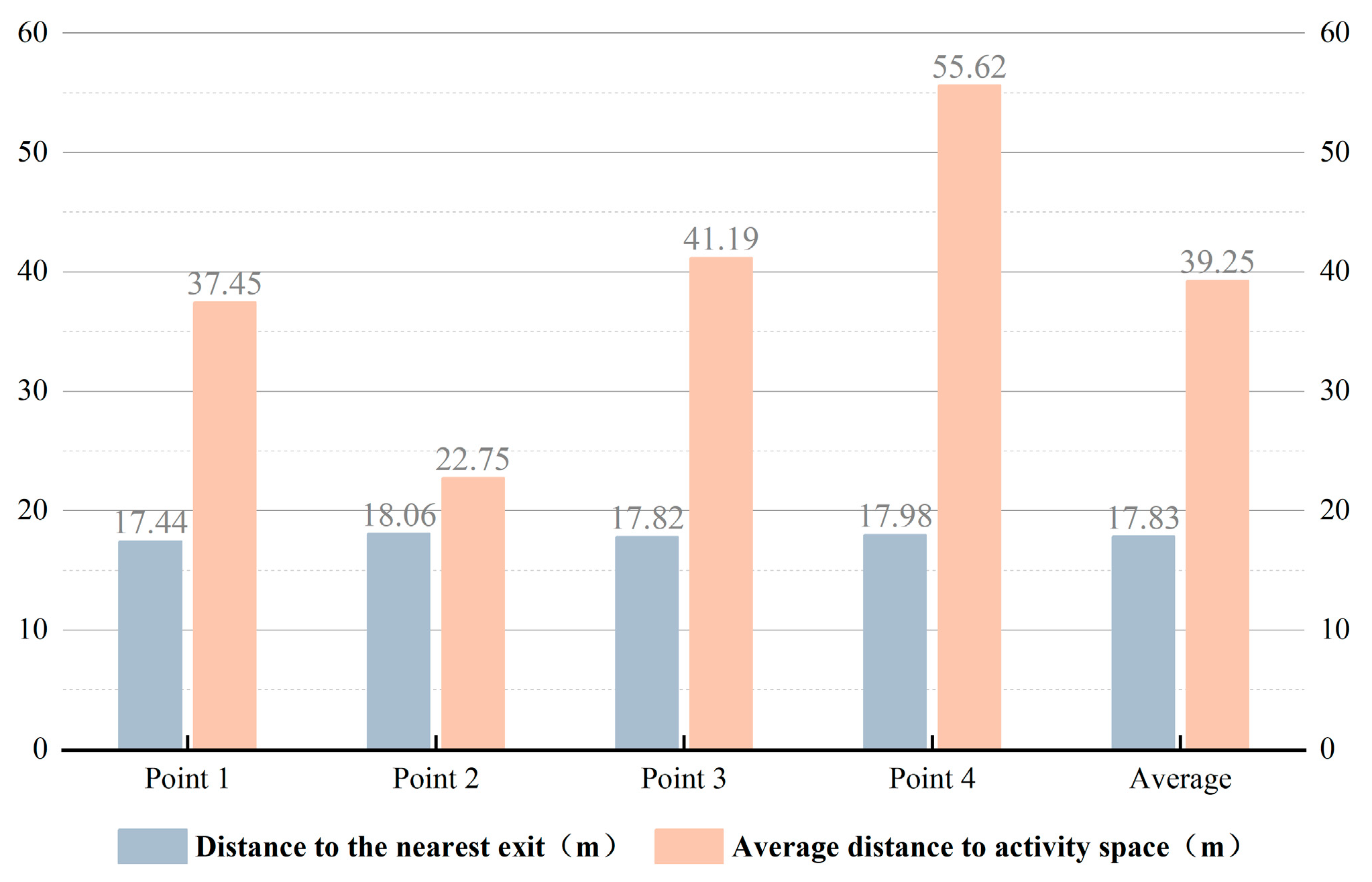
3.2. Accessibility of Walking
3.3. Safety of Walking
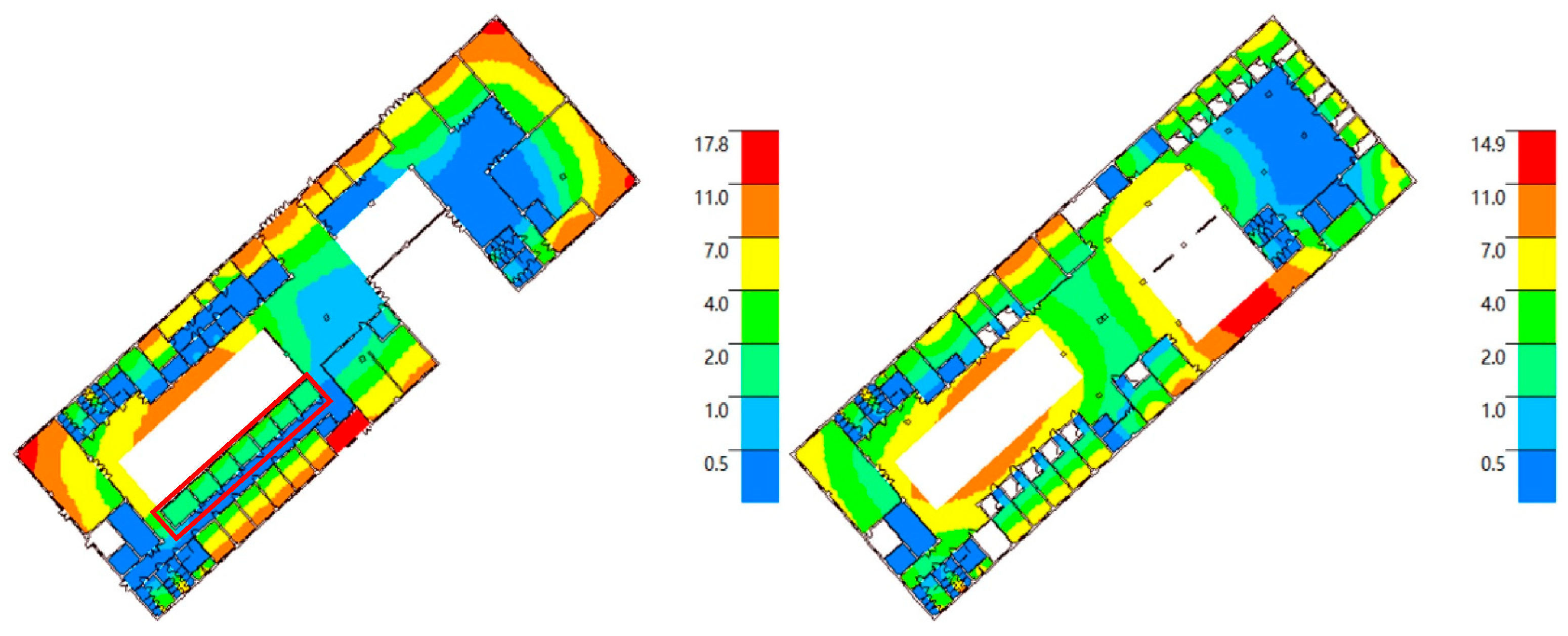
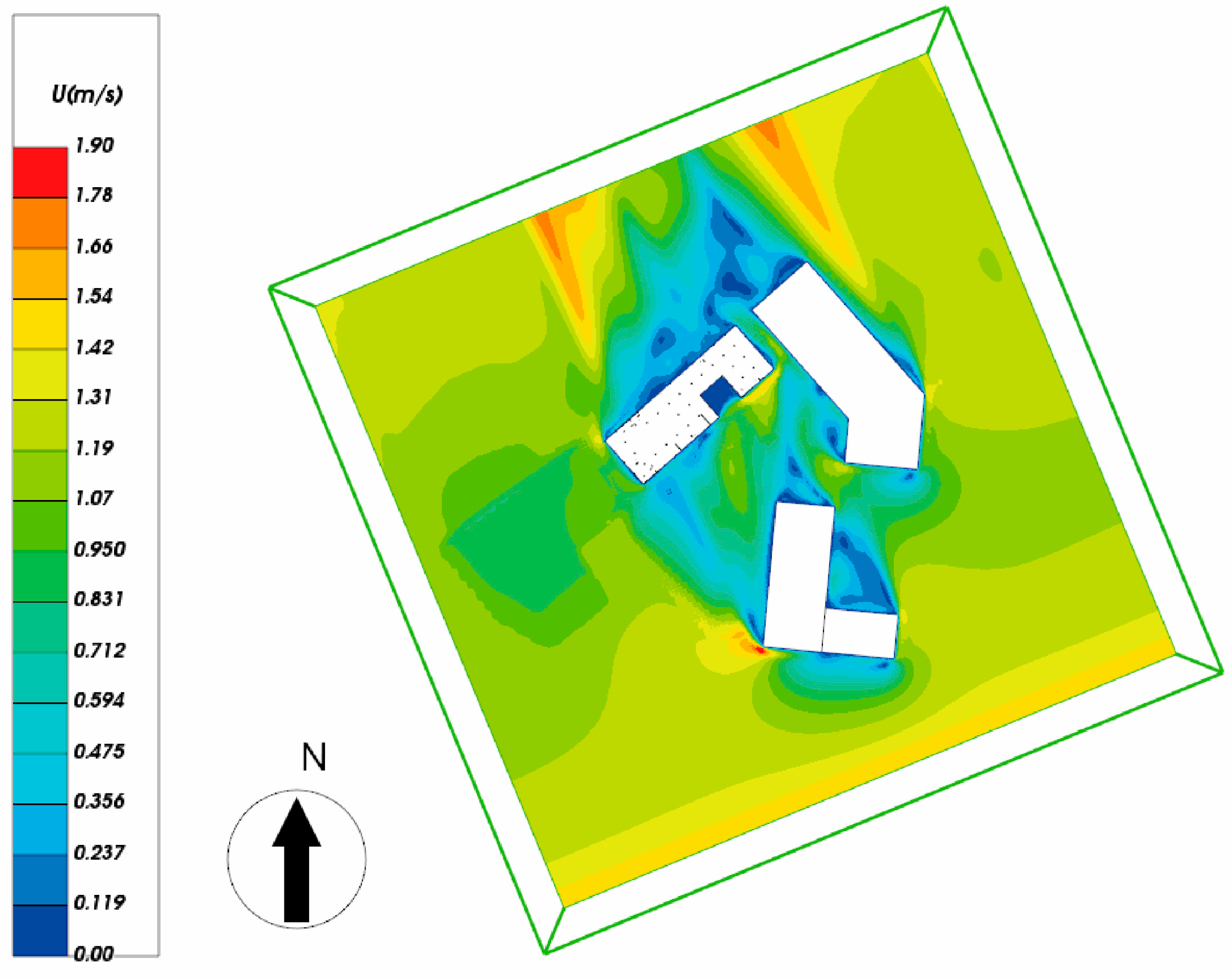
3.4. Daylight Factor and Ventilation
3.5. Discussions
4. Conclusions and Prospects
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Available online: https://www.who.int/china/health-topics/ageing (accessed on 23 January 2025).
- Langenbrunner, J.C.; Marquez, P.V.; Wang, S. Toward a Healthy and Harmonious Life in China: Stemming the Rising Tide of Non-Communicable Diseases; The World Bank: Washington, DC, USA, 2011. [Google Scholar]
- Wang, X.-Q.; Chen, P.-J. Population ageing challenges health care in China. Lancet 2014, 383, 870. [Google Scholar] [CrossRef] [PubMed]
- Harwood, R.H.; Sayer, A.A.; Hirschfeld, M. Current and future worldwide prevalence of dependency, its relationship to total population, and dependency ratios. Bull. World Health Organ. 2004, 82, 251–258. [Google Scholar] [PubMed]
- Wong, Y.C.; Leung, J. Long-term care in China: Issues and prospects. J. Gerontol. Soc. Work. 2012, 55, 570–586. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, A.J.; Mehta, A. Maslow’s hierarchy of needs-theory of human motivation. Int. J. Res. All Subj. Multi Lang. 2019, 7, 38–41. [Google Scholar]
- Nie, H.; Xu, Y.; Liu, B.; Zhang, Y.; Lei, T.; Hui, X.; Zhang, L.; Wu, Y. The prevalence of mild cognitive impairment about elderly population in China: A meta-analysis. Int. J. Geriatr. Psychiatry 2011, 26, 558–563. [Google Scholar] [CrossRef]
- Chen, Y.; Hicks, A.; While, A.E. Depression and related factors in older people in China: A systematic review. Rev. Clin. Gerontol. 2012, 22, 52–67. [Google Scholar] [CrossRef]
- Han, J.; Chan, E.H.; Yung, E.H.; Qian, Q.K.; Lam, P.T. A policy framework for producing age-friendly communities from the perspective of production of space. Int. J. Environ. Res. Public Health 2022, 19, 2031. [Google Scholar] [CrossRef]
- Xu, Y.; Liu, H.; Su, S.; Mao, P. Ageing suitability evaluation of residential districts based on Active Ageing Theory. Buildings 2023, 13, 1041. [Google Scholar] [CrossRef]
- Fallah, H.; Nazari, J.; Choobineh, A.; Morowatisharifabad, M.A.; Jafarabadi, M.A. Inclusive Design: An Approach to Adapt Homes for the Elderly. Pak. J. Med. Health Sci. 2021, 15, 1599–1603. [Google Scholar] [CrossRef]
- Liu, J.; Wei, Q. Discussion on the spatial design of elderly care buildings under the concept of ageing-friendly concept. In Proceedings of the SHS Web of Conferences, Harbin, China, 6–8 December 2024; p. 01015. [Google Scholar]
- Han, J.; Chan, E.H.W.; Qian, Q.K.; Yung, E.H.K. Achieving sustainable urban development with an ageing population: An “age-friendly city and community” approach. Sustainability 2021, 13, 8614. [Google Scholar] [CrossRef]
- Han, L.; Wang, B. Research on the Community Renewal of “Active Adaptation to the Elderly” in the Unit Compound. In Proceedings of the ECSF 2021: Engineering, Construction, and Infrastructure Solutions for Innovative Medicine Facilities, St. Petersburg, Russia, 19–21 May 2021; Springer: Cham, Switzerland, 2022; pp. 1–14. [Google Scholar]
- Tao, Y.; Zhang, W.; Gou, Z.; Jiang, B.; Qi, Y. Planning walkable neighborhoods for “aging in place”: Lessons from five aging-friendly districts in Singapore. Sustainability 2021, 13, 1742. [Google Scholar] [CrossRef]
- Tort Ayala, L.S. Principles and Recommendations to Design Aging-Friendly Homes. Doctoral Dissertation, Massachusetts Institute of Technology, Cambridge, MA, USA, 2019. [Google Scholar]
- Liu, J. Data Mining and Retrofit Design for Age-friendly Spaces. In Proceedings of the International Conference on Green Building, Civil Engineering and Smart City, Guiyang, China, 9–12 June 2023; pp. 835–843. [Google Scholar]
- Fang, M.L.; Sixsmith, J.; Hamilton-Pryde, A.; Rogowsky, R.; Scrutton, P.; Pengelly, R.; Woolrych, R.; Creaney, R. Co-creating inclusive spaces and places: Towards an intergenerational and age-friendly living ecosystem. Front. Public Health 2023, 10, 996520. [Google Scholar] [CrossRef] [PubMed]
- Luciano, A.; Pascale, F.; Polverino, F.; Pooley, A. Measuring age-friendly housing: A framework. Sustainability 2020, 12, 848. [Google Scholar] [CrossRef]
- Tao, Y.; Gou, Z.; Yu, Z.; Fu, J.; Chen, X. The challenge of creating age-friendly indoor environments in a high-density city: Case study of Hong Kong’s care and attention homes. J. Build. Eng. 2020, 30, 101280. [Google Scholar] [CrossRef]
- Jiao, Y.; Yu, Y.; Yu, H.; Wang, F. The impact of thermal environment of transition spaces in elderly-care buildings on thermal adaptation and thermal behavior of the elderly. Build. Environ. 2023, 228, 109871. [Google Scholar] [CrossRef]
- Hickerson, B.; Moore, A.; Oakleaf, L.; Edwards, M.; James, P.A.; Swanson, J.; Henderson, K.A. The Role of a Senior Center in Promoting Physical Activity for Older Adults. J. Park Recreat. Adm. 2008, 26, 22–39. [Google Scholar]
- The People’s Government of Sanya City. Available online: https://www.sanya.gov.cn/sanyasite/tjgb/202105/01681d7550e343c69c2b892709e504dd.shtml (accessed on 23 January 2025).
- The People’s Government of Sanya City. Available online: https://www.sanya.gov.cn/sanyasite/syyw/202311/1edf5e69fcf949a89fbda0fab5b52461.shtml (accessed on 23 January 2025).
- JGJ450-2018; Standards for Design of Care Facilities for the Aged. Architecture & Building Press: Beijing, China, 2018.
- GB 55037-2022; General Code for Fire Protection of Buildings and Constructions. China Planning Press: Beijing, China, 2022.
- GB 50763-2012; Codes for Accessibility Design. China Architecture & Building Press: Beijing, China, 2012.
- Shao, Q.; Wang, H.; Hu, T.; Gu, D. Effects of age and gender on biomechanical characteristics of human gait. Chin. J. Appl. Mech. 2022, 39, 1193–1202. [Google Scholar]
- Lee, S.; Dilani, A.; Morelli, A.; Byun, H. Health supportive design in elderly care homes: Swedish examples and their implication to Korean counterparts. Archit. Res. 2007, 9, 9–18. [Google Scholar]
- Tural, E.; Lu, D.; Cole, D.A. Factors predicting older Adults’ attitudes toward and intentions to use stair mobility assistive designs at home. Prev. Med. Rep. 2020, 18, 101082. [Google Scholar] [CrossRef]
- GB 50033-2013; Standard for daylighting design of buildings. China Architecture & Building Press: Beijing, China, 2013.
- GB 55016-2021; General code for building environment. China Architecture & Building Press: Beijing, China, 2021.
- Yang, H.; Guo, B.; Shi, Y.; Jia, C.; Li, X.; Liu, F. Interior daylight environment of an elderly nursing home in Beijing. Build. Environ. 2021, 200, 107915. [Google Scholar] [CrossRef]
- Cerqueira, F.; Nogueira, S.; Aelenei, D.; Viegas, J. Assessment of ventilation in elderly care centres. In Proceedings of the 40th IAHS World Congress on Housing Sustainable Housing Construction, Funchal, Portugal, 16–19 December 2014. [Google Scholar]
- Abbas, N.; Abrar ul Haq, M.; Ashiq, U.; Ubaid, S. Loneliness among elderly widows and its effect on social and mental well-being. Glob. Soc. Welf. 2020, 7, 215–229. [Google Scholar] [CrossRef]
- Lara, R.; Vázquez, M.L.; Ogallar, A.; Godoy-Izquierdo, D. Psychosocial resources for hedonic balance, life satisfaction and happiness in the elderly: A path analysis. Int. J. Environ. Res. Public Health 2020, 17, 5684. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Codes | Regulations | |||
|---|---|---|---|---|
| “Standards for design of care facilities for the aged” | There should be entertainment and fitness rooms in the senior building | Seats in dining room: nursing care: ≥40% of beds; 4 m2/seats non-nursing care: ≥70% of beds; ≥2.5 m2/seats | Area of entertainment and fitness rooms ≥ 2 m2/bed (person) | |
| “General code for fire protection of buildings and constructions” | “The evacuation distance from any point in a room to the room’s evacuation door should not exceed the maximum allowed evacuation distance from the evacuation door of rooms located on either side or end of a pocket corridor to the nearest safe exit”. | |||
| “Codes for accessibility design” | The size of cabin: 1500 mm (width) × 2700 mm (length) Handrails 850~900 mm high Mirrors: 900 mm high to the top | Single-layer handrails: 850~900 mm Double-layer handrails: upper 850~900 mm lower 650~700 mm | ||
| Point 1 | Point 2 | Point 3 | Point 4 | Average | |
|---|---|---|---|---|---|
| To the nearest exit | 28.82 m | 17.82 m | 33.75 m | 32.62 m | 28.25 m |
| To activity room on the first floor | 48.69 m | 37.69 m | 53.63 m | 52.49 m | 48.12 m |
| To outdoor activity room | 59.47 m | 48.47 m | 64.40 m | 63.27 m | 58.90 m |
| To communication space | 58.33 m | 6.12 m | 5.88 m | 7.81 m | 19.54 m |
| To psychological counseling room | 47.53 m | 47.18 m | 50.76 m | 33.74 m | 44.80 m |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yi, C.; Han, W.; Liu, Y.; Lin, Y.; Qi, Y. Aging Adaptation Transition of Health Care Buildings for Accessibility Optimization for the Elderly. Buildings 2025, 15, 379. https://doi.org/10.3390/buildings15030379
Yi C, Han W, Liu Y, Lin Y, Qi Y. Aging Adaptation Transition of Health Care Buildings for Accessibility Optimization for the Elderly. Buildings. 2025; 15(3):379. https://doi.org/10.3390/buildings15030379
Chicago/Turabian StyleYi, Chang, Wenyang Han, Yiheng Liu, Yijie Lin, and Yicong Qi. 2025. "Aging Adaptation Transition of Health Care Buildings for Accessibility Optimization for the Elderly" Buildings 15, no. 3: 379. https://doi.org/10.3390/buildings15030379
APA StyleYi, C., Han, W., Liu, Y., Lin, Y., & Qi, Y. (2025). Aging Adaptation Transition of Health Care Buildings for Accessibility Optimization for the Elderly. Buildings, 15(3), 379. https://doi.org/10.3390/buildings15030379