
Children’s Hospital Environment Design Based on AHP/QFD and Other Theoretical Models




Abstract
1. Introduction
2. Materials and Methods
2.1. Analysis of the Current Situation of Environmental Space Design in Children’s Hospitals
2.2. Research Process for the Environmental Space Design of Children’s Hospitals
2.3. Analysis and Measurement of the Hierarchical Requirements of Children’s Hospital Space Design Users

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A1 | A11 | A12 | A13 | A14 | W |
|---|---|---|---|---|---|
| A11 | 1 | 4 | 4 | 1 | 0.4065 |
| A12 | 1/4 | 1 | 3 | 1/2 | 0.1591 |
| A13 | 1/4 | 1/3 | 1 | 1/5 | 0.0730 |
| A14 | 1 | 2 | 5 | 1 | 0.3614 |
| A2 | A21 | A22 | A23 | A24 | W |
|---|---|---|---|---|---|
| A21 | 1 | 1/4 | 3 | 1/3 | 0.1429 |
| A22 | 4 | 1 | 4 | 1 | 0.4042 |
| A23 | 1/3 | 1/4 | 1 | 1/4 | 0.0768 |
| A24 | 3 | 1 | 4 | 1 | 0.3761 |
| A3 | A31 | A32 | A33 | A34 | W |
|---|---|---|---|---|---|
| A31 | 1 | 1 | 1/3 | 3 | 0.2010 |
| A32 | 1 | 1 | 1/3 | 3 | 0.2010 |
| A33 | 3 | 3 | 1 | 5 | 0.5204 |
| A34 | 1/3 | 1/3 | 1/5 | 1 | 0.0776 |
| A4 | A41 | A42 | A43 | A44 | W |
|---|---|---|---|---|---|
| A41 | 1 | 1/5 | 1/3 | 1/5 | 0.0662 |
| A42 | 5 | 1 | 3 | 1 | 0.3836 |
| A43 | 3 | 1/3 | 1 | 1/4 | 0.1379 |
| A44 | 5 | 1 | 4 | 1 | 0.4123 |
3. Transformation of User Needs for Environmental Space Design in Children’s Hospitals
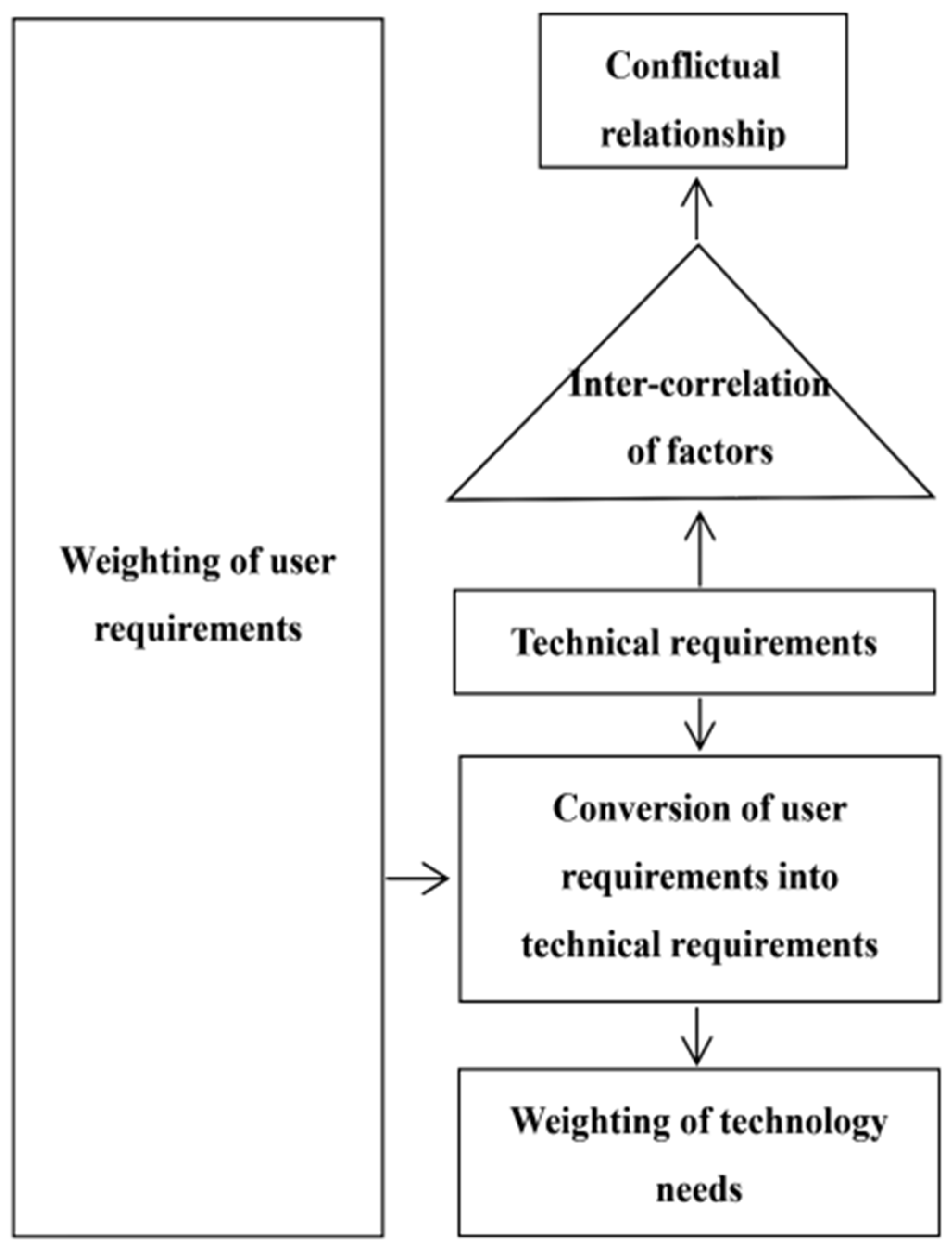
3.1. QFD-Based Design Feature Transformation
3.2. Children’s Hospital Spatial Environmental House of Quality
4. Discussion on Design Contradictions Based on TRIZ Theory
4.1. Analysis of Contradictions in the Spatial Design of Children’s Hospitals
4.2. Solutions to the Contradictions in the Spatial Design of Children’s Hospitals
5. Innovative Design Practice Based on Contradiction Analysis Results
5.1. Overall Internal Structure of Space Design for Children’s Hospitals
5.2. Interactive Guide Signage Design
5.3. Natural Materials and Representation
5.4. Humanized Design for Security
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McLaughlan, R.; Sadek, A.; Willis, J. Attractions to fuel the imagination: Reframing understandings of the role of distraction relative to well-being in the pediatric hospital. HERD Health Environ. Res. Des. J. 2019, 12, 130–146. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim Momtaz, R.; Shaban, R. The impact of healing gardens on improving psychological recovery of children-application on pediatric cancer hospital in egypt. J. Eng. Sci. 2018, 46, 333–345. [Google Scholar] [CrossRef]
- Sun, Q. Research on soft decoration design of children’s hospital wards under the concept of emotionalization. Shanxi Archit. 2023, 49, 182–185. [Google Scholar]
- Wang, S.; Fan, M. Research on the design of aging-appropriate shoe-changing seat based on Kano-AHP-QFD. Packag. Eng. 2024, 11, 1–13. [Google Scholar]
- Hu, C.; Shi, Y. Research on children’s toy design based on AHP/QFD/TRIZ model. J. Hubei Univ. Technol. 2023, 38, 100–107. [Google Scholar]
- Hu, K.; Cai, W. Research on the design of paper toys for 3–6 years old children integrating AHP-QFD-TRIZ theory. Ind. Eng. Des. 2023, 5, 78–85. [Google Scholar]
- Yu, M.; Cui, J. Research on the design of intelligent janitorial robot based on AHP/QFD/TRIZ. Packag. Eng. 2023, 44, 82–91. [Google Scholar]
- Doğan, N.Ö.; Akbal, H. Identification and evaluation of the ways of meeting patients’ expectations from a hospital: An ahp-weighted qfd case study in a pediatric hospital. Istanb. Bus. Res. 2020, 49, 224–247. [Google Scholar] [CrossRef]
- Yang, D. Research on the Design of Signage Guidance System of Children’s Hospital Based on Emotionalization. Mater’s Thesis, Jiangxi University of Finance and Economics, Nanchang, China, 11 July 2022. [Google Scholar]
- Song, H.-Y.; Shi, J. Research on the emotional design of children’s stethoscope. Design 2021, 34, 8–10. [Google Scholar]
- Li, P.-X. Diversity and Emotion: Optimizing the Design of Hospital Waiting Space Based on Children’s Waiting Behavior. Art Ocean 2021, 12, 86–88. [Google Scholar]
- Zhu, T.L.; Li, Y.J.; Wu, C.J.; Yue, H.; Zhao, Y.Q. Research on the design of surgical auxiliary equipment based on AHP, QFD, and PUGH decision matrix. Math. Probl. Eng. 2022, 2022, 4327390. [Google Scholar] [CrossRef]
- Fucheng, W.; Liu, Y.; Kuang, J. Research on Design of Intelligent Agricultural Harvester Based on QFD and AHP. Int. J. New Dev. Eng. Soc. 2022, 6, 11–19. [Google Scholar]
- Wang, N.; Shi, C.; Kang, X. Design of retractable dining table based on AHP/QFD/TRIZ theory. Packag. Eng. 2023, 44, 90–100. [Google Scholar]
- Zheng, Y.; Cheng, X.; Ding, Z. Research on the design of household disinfection closet based on AHP and QFD analysis. Furnit. Inter. Decor. 2023, 30, 60–65. [Google Scholar]
- Xiong, T.; Lin, Y.; An, X. Design of tracked mobile crusher based on AHP-QFD theory. Mech. Des. 2023, 40, 27–32. [Google Scholar] [CrossRef]
- Power, J.; Harris, J.; Leaper, D.J. Using QFD As a Method to Develop Functional Medical Products for Children with Cancer. In Proceedings of the 90th Textile Institute World Conference, Poznan, Poland, 25–28 April 2016. [Google Scholar]
- Mai, J.; Li, C.; Li, Y. Innovative design of children’s bed based on QFD and TRIZ theory. Ind. Des. 2022, 2, 29–31. [Google Scholar]
- Wang, G.; Yuan, Y. Practical Application of Environmental Design Psychology—Classroom Space Arrangement and Environmental Psychology. Sci. Technol. Inf. 2008, 28, 199–300. [Google Scholar]
- Nourmusavi Nasab, S.; Karimi Azeri, A.R.; Mirbazel, S. Ideal physical features of environmental design in children’s hospital: Using children ‘s perspectives. Facilities 2020, 38, 445–466. [Google Scholar] [CrossRef]
- Bonnes, M.; Bonaiuto, M.; Fornara, F.; Bilotta, E. Environmental psychology and architecture for health care design. In Proceedings of the 28th International Public Health Seminar, TESIS InterUniversity Research Center–Systems and Technologies in Healthcare Buildings, Florence, Italy, 23–27 April 2009. [Google Scholar]
- Gaminiesfahani, H.; Lozanovska, M.; Tucker, R.A. Scoping Review of the Impact on Children of the Built Environment Design Characteristics of Healing Spaces. HERD Health Environ. Res. Des. J. 2020, 13, 98–114. [Google Scholar] [CrossRef]
- Fu, L.; Dai, X.; Wu, Z.; Tan, C.; Gong, F.; Jiang, W. Introduction to the spatial design of children’s hospital based on color psychology. Eng. Constr. 2020, 52, 1–5. [Google Scholar]
- Biddiss, E.; McPherson, A.; Shea, G.; McKeever, P. The Design and Testing of Interactive Hospital Spaces to Meet the Needs of Waiting Children. HERD Health Environ. Res. Des. J. 2013, 6, 49–68. [Google Scholar] [CrossRef] [PubMed]
- Kasal, A.; Birgul, R.; Erdil, Y.Z. Determination of the strength performance of chair frames constructed of solid wood and wood composites. For. Prod. J. 2006, 56, 55. [Google Scholar]
- Bruckman, A.; Bandlow, A. Human-computer interaction for kids. In The Human-Computer Interaction Handbook; CRC Press: Boca Raton, FL, USA, 2003; Volume 1, pp. 428–440. [Google Scholar]
- Ponti, M. Screen time and preschool children: Promoting health and development in a digital world. Paediatr. Child Health 2023, 28, 184–192. [Google Scholar] [CrossRef] [PubMed]







| Indicator Scale | Description of the Extent |
|---|---|
| 1 | Indicates that a is as important as b in a two-by-two comparison |
| 3 | Indicates that a is slightly more important than b in a two-by-two comparison. |
| 5 | Indicates that a is significantly more important than b in a two-by-two comparison. |
| 7 | Indicates that a is more strongly important than b in a two-by-two comparison. |
| 9 | Indicates that a is more important than b in a two-by-two comparison. |
| 2, 4, 6, 8 | Between neighboring indicator scales |
| n | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
| RI | 0 | 0 | 0.52 | 0.89 | 1.12 | 1.26 | 1.36 | 1.41 | 1.46 |
| A | A1 | A2 | A3 | A4 | W |
|---|---|---|---|---|---|
| A1 | 1 | 1/5 | 1/5 | 1 | 0.0925 |
| A2 | 5 | 1 | 1 | 3 | 0.4073 |
| A3 | 5 | 1 | 1 | 2 | 0.3680 |
| A4 | 1 | 1/3 | 1/2 | 1 | 0.1322 |
| Weights at the Guideline Level | Indicator Layer | Weighting of Indicator Layers | Combined Weights |
|---|---|---|---|
Visual elements (A1) W = 0.0925 | Color(A11) | 0.4065 | 0.0376 |
| Use of shapes (A12) | 0.1591 | 0.0147 | |
| Sunlight (A13) | 0.0730 | 0.0068 | |
| Styles and themes (A14) | 0.3614 | 0.0334 | |
Human–computer interaction (A2) W = 0.4073 | Recreation facilities (A21) | 0.1429 | 0.0582 |
| Signage (A22) | 0.4042 | 0.1646 | |
| Medical equipment (A23) | 0.0768 | 0.0313 | |
| Game interaction (A24) | 0.3761 | 0.1532 | |
Safety (A3) W = 0.3680 | Use of materials (A31) | 0.2010 | 0.0740 |
| Corner design (A32) | 0.2010 | 0.0740 | |
| Social security (A33) | 0.5204 | 0.1915 | |
| Accessibility (A34) | 0.0776 | 0.0286 | |
Functional (A4) W = 0.1322 | Regional distribution (A41) | 0.0662 | 0.0088 |
| Healing function(A42) | 0.3836 | 0.0507 | |
| Educational function(A43) | 0.1379 | 0.0182 | |
| Personalized messages (A44) | 0.4123 | 0.0545 |
| Standardized Layer | Indicator Layer | Technological Needs |
|---|---|---|
Visual elements (A1) | Color (A11) | Interactive color decoration |
| Use of shapes (A12) | Safe and easy to clean | |
| Ergonomic | ||
| Sunlight (A13) | Safe and easy to clean | |
| Styles and themes (A14) | Low complexity | |
| Simple and aesthetically pleasing | ||
Human–computer interaction (A2) | Recreation facilities (A21) | Safe and easy to clean |
| Eco-friendly materials | ||
| Intelligent toys with a variety of ways to play | ||
| Signage (A22) | Total Automation System | |
| Eco-friendly materials | ||
| Interactive color decoration | ||
| Medical equipment (A23) | Safe and easy to clean | |
| Ergonomic | ||
| Interactive color decoration | ||
| Game interaction (A24) | Interactive devices | |
| Various ways to play | ||
Safety (A3) | Use of materials (A31) | Eco-friendly materials |
| Safe and easy to clean | ||
| Stable structure | ||
| Corner design (A32) | Safe and easy to clean | |
| Stable structure | ||
| Social security (A33) | Total Automation System | |
| Accessibility (A34) | Multifunctional flexibility of tables and chairs | |
| Child safety fixtures | ||
| Ergonomic | ||
Functional (A4) | Regional distribution (A41) | Interactive color decoration |
| Simple and aesthetically pleasing | ||
| Healing function(A42) | Interactive fixtures | |
| Educational function(A43) | Interactive devices | |
| Personalized messages(A44) | Total Automation System |
| Contradictory Conflicts | Recommended Inventive Principles | Solutions |
|---|---|---|
| Intelligent toys with diverse play methods—simplicity and beauty, low complexity | Principle 2: separation principle | Different parts of the toy can be interchangeable or recombined to create new ways to play |
| Interactive devices—low complexity | Principle 25: self-service principle | Tactile feedback and graphical indications |
| Comprehensive automation—structural stability | Principle 3: local quality principle | Each component maximizes its functionality to ensure overall structural stability |
| Multifunctional flexibility in tables and chairs—structural stability, safe and easy to clean, low complexity | Principle 2: separation principle (repeated) Principle 15: dynamization principle | Detachable and adjustable table and chair components, minimizing decorations to ensure smooth edges, and selecting sustainable materials |
| Interactive color decorations—sustainable, environmentally friendly materials | Principle 32: changing color principle | Dynamic interaction, choosing materials that can change color in response to different stimuli |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zheng, H.; Liu, L.; Zhang, Q.; Wang, Y.; Wei, Y. Children’s Hospital Environment Design Based on AHP/QFD and Other Theoretical Models. Buildings 2024, 14, 1499. https://doi.org/10.3390/buildings14061499
Zheng H, Liu L, Zhang Q, Wang Y, Wei Y. Children’s Hospital Environment Design Based on AHP/QFD and Other Theoretical Models. Buildings. 2024; 14(6):1499. https://doi.org/10.3390/buildings14061499
Chicago/Turabian StyleZheng, Haohua, Lingying Liu, Qi Zhang, Yihan Wang, and Yangyang Wei. 2024. "Children’s Hospital Environment Design Based on AHP/QFD and Other Theoretical Models" Buildings 14, no. 6: 1499. https://doi.org/10.3390/buildings14061499
APA StyleZheng, H., Liu, L., Zhang, Q., Wang, Y., & Wei, Y. (2024). Children’s Hospital Environment Design Based on AHP/QFD and Other Theoretical Models. Buildings, 14(6), 1499. https://doi.org/10.3390/buildings14061499