Abstract
Healthy City policies are often enforced based on expert assessments, which calls for research on the presence and occurrence of mismatches between experts’ and public opinions. Additionally, the unique challenges in small and midsized cities (SMCs) are often ignored. In this study, we compared the values of experts and the public on achieving a healthy SMC. A survey with both experts and public participants was conducted. An explorative factor analysis (EFA) and fuzzy synthetic evaluation (FSE) were adopted to identify the key factors and their importance hierarchy. Both the experts and the public highlight the importance of Environmental Quality and Governance/Service (EQ). More attention could be given to public participation and urban form to reflect the public’s perceptions better, as they prioritized these factors more than the experts did. Both similarities and mismatches between experts and the public were revealed in this study, indicating that more studies are necessary to understand heterogeneous values and achieve mutual understanding. Thus, public participation and involvement are recommended to construct a Healthy City for more comprehensive benefits. Our results also offer valuable insights from the public to plan Healthy Cities in the future, avoiding reactive decision making.
1. Introduction
A growing body of evidence shows that health equity has become a significant goal in Healthy Cities, which aims to reduce the health-related gap between geographical and social groups [1,2,3]. Previous research has also revealed that more attention could be given to underprivileged and easily ignored geographic areas in urban planning and public health [4,5,6]. Overwhelmingly more attention is being paid to big cities compared to small and midsized cities (SMCs) in Healthy City-related research [7,8], leaving potential health inequalities among cities of different scales. Though SMCs face unique challenges, calling for a better understanding of the key factors of urban design and governance [9,10,11], their requirements are easily ignored. To better achieve health equality, we must consider varied city scales and urban–rural differences [12,13]. This factor underlines the need for further explorative research on how urban design and governance could better contribute to healthy SMCs.
Healthy Cities improve every citizen’s well-being [14,15]. However, many previous research studies have shown different values between experts and the public [16,17], no matter the built environment [18,19] or health-related field [20,21,22]. Public opinion has a very small influence on policy, particularly when the knowledge of public opinions is based on personal perception rather than empirical evidence [23]. Management decisions that do not adequately reflect public values may lead to controversy and conflict, especially when the actions are unacceptable to stakeholders [21,24]. Most systematic Healthy City studies and related indicators are based on expert assessments, reflecting a possible lack of opinions from the public. We must analyze the difference between experts and public opinions on urban and built environmental issues [19]. Thus, this study aims to enhance the role of the public in Healthy City construction by comparing and revealing expert–public perception similarities (or differences).
To analyze the mismatch between criteria valuable to the expert and the public, a questionnaire survey was conducted, including 54 experts and 229 members of the public. The survey data were then analyzed using exploring factor analysis (EFA) and fuzzy synthetic evaluation (FSE) techniques to demonstrate the valued importance hierarchy. Then, the similarities and differences between them were further compared. Clear differences between the expert and public values were identified. The results indicate that Environmental Quality and Governance/Service (EQ) are considered the most important factors in this study by both the experts and the public. The importance of participation and urban form was not adequately appreciated by the experts compared with the public. The heterogeneous values between the experts and the public found in this research may point to further public participation in future Healthy City development. By focusing on SMCs and emphasizing public perception, this study may contribute to enhancing health equality and guide future Healthy City construction for more social groups. Based on examining the extent to which the experts’ judgment on Healthy Cities reflects public perception, this study also provides a reference for standard setters to include the public’s view in decision making.
We started with a comprehensive review to develop a health–space indicator system as the basis for evaluations of the experts and the public, and then, the key factors were identified and compared. The data collection and analysis methods were then employed. The following text reflects the discussions of the findings, from the similarities to the differences; the main conclusions and future studies are also discussed.
2. Theoretical Framework
SMCs are different from big cities; they can be defined by population size [25,26] and recognized by self-identification [27]. The special challenges and essential factors of SMC development have been noted in previous studies, which call for more understanding of the unique issues that SMCs face [9]. For example, entertainment opportunities and diversity have a much smaller influence on the development of SMCs compared with that of big cities [25]. The less-complex governance system in SMCs might lead to more immediate intervention results [26]. To obtain an understanding of the determinants of achieving a Healthy City, five factors with 39 variables were summarized from a comprehensive review, namely, Health-Friendly Services, Urban Forms and Facilities, Green and Open Spaces, Environmental Quality and Energy, and Community and Governance. The majority of the previous experiences are derived from big cities or expert assessments [8,28,29]; therefore, there is much less evidence from SMCs [30,31], so their role in this context require further understanding.
2.1. Health-Friendly Services
Varied types of health facilities, including hospitals, health centers, and medical institutions, provide fundamental security for urban health [32,33,34]. Small towns in South Africa, such as Prince Albert, cannot always access basic services [34]. Based on an empirical examination from Shanghai, a metropolitan city in East China, the accessibility of healthcare facilities varies in different socio-economic districts, while high-income households have better access [35]. By comparing the values of experts and the public on healthcare in the Netherlands, mixed values have been documented [22]. Neighborhood emergency services are crucial in delivering effective treatment, especially because there is a lack of primary care physicians and knowledge of the healthcare system [36].
The role of health facilities is becoming more influential for vulnerable groups, such as elderly and disabled people. Special caring and considerations include disability inclusion in public programs and a larger human workforce [37]. Achieving aging-friendly cities is important for overall construction. The basic living environment, open spaces, and community amenities can profoundly impact the health of aging individuals [28,38,39]. Providing more barrier-free entries for wheelchair users, specialized handrails, guide dogs, and modified ground colors is helpful for accommodating individuals with disabilities [37].
2.2. Urban Forms and Facilities
The configuration of urban spaces and transportation facilities significantly shapes residents’ lifestyles, either promoting or hindering activities like walking and cycling, thus further impacting citizens’ health [40,41,42], with the added benefits of reducing harmful emissions [43]. The urban transportation system, encompassing road networks, sidewalks, formal and informal pathways, and, particularly, public transport services play a crucial role in influencing residents’ mobility [44,45,46].
The details of residential spaces, such as estate density, affordable housing provision, and an appropriate layout and density of community and social services [39,47,48] should be thoughtfully considered. Restorative residential environments are possible [49]. Age-friendly community planning should guarantee residents’ access to facilities and the equitable distribution of facilities [50]. Facilities, including commercial, cultural, municipal, and leisure, can encourage physical activity, which further lead to better healthy conditions [47,51,52]. Recreational and entertainment facilities, especially those accessible to the public, are essential for social and cultural engagement.
2.3. Green and Open Spaces
The majority of previous studies paid attention to the role of GOSs for urban health, especially in the context of big cities. GOSs support physical activity, which in turn, contribute to both physical and mental health [53,54,55], which is especially helpful in decreasing the respiratory mortality rate [56]. In the right places, GOSs can benefit Air Quality, thus further contributing to physical health [57]. Streetscapes, as one type of GOS, are associated with less crime and more safety, which is also beneficial for mental health [58,59,60]. This evidence is supported by both lab experiments and big city empirical data. Lab experiments using photos to compare the health impacts of vegetation and brightness indicate that vegetation is helpful in recovering from mental fatigue [61]. Big city empirical research has included cities like Abu Dhabi in the Middle East [62], Houston in North America [54], and Chengdu from China [59], but SMCs have not been considered yet.
The real usage of GOSs is deeply impacted by their accessibility, with specific indicators, such as GOS density, park proximity, and the time to reach the nearest GOS [63]. GOS distribution is related to socio-economic factors like equity and contributes to health conditions especially for people living in more deprived areas [64]. Green spaces of varied quality have different impacts on health conditions [55,65]. The quality of an open space is associated with walking and mental health and affects healthy urban design and planning [48,66].
GOSs provide opportunities for people to connect with nature, fostering nature relatedness and a sense of connectedness [67]. The variables include nature connectivity, the park number, size, and density [68]. Urban design plays a part in promoting people’s engagement with nature every day, emphasizing the importance of a ‘wildlife-inclusive’ approach for public health [69]. The importance of biodiversity for urban health, linking human beings to wildlife such as birds [70], has also been documented.
2.4. Environmental Quality and Energy
Environmental Quality plays a pivotal role in urban health by impacting basic hygiene and sanitation conditions, especially physical health. Analyzing the spatial patterns of pollutants like ozone and PM10 is crucial for understanding and mitigating air pollution [71]. Based on experiences from an SMC, Santa Ana, in the US, PM2.5 is more concentrated in disadvantaged communities [31]. Disadvantaged groups, such as elderly people and small children, suffer more from pollution-related respiratory issues [72]. Providing clean water and improving toilet facilities typically improve urban hygiene and sanitation [11,47]. Stormwater facilities not only serve as urban amenities but also work as water sanitation facilities that can contribute to health [73,74]. Green building elements, such as roof gardens, are a practical approach for improving Environmental Quality [75].
Considering the internal relationship within the five factors, UFFs and GOSs impact EQE and further affect urban health indirectly. For example, Thermal Comfort is positively correlated with green spaces [76,77]. Sound is another crucial environmental factor correlated with living comfort. Serious urban noise nuisances negatively impact human health but can be reduced by carefully designing soundscapes [78]. Thermal Comfort and humidity are impacted by urban forms and housing settings and further play a vital role in human health [79].
2.5. Community and Governance
Urban design is a public policy that has a close relationship with urban governance in addition to the environmental vision. Public participation can enhance people’s well-being by involving varied stakeholders [80,81,82], but it is difficult to achieve real co-governance due to the unbalanced power relationships in SMCs [83]. Social interactions and fostering a sense of community at the neighborhood level are crucial for local health [84]. Spaces that encourage informal social interaction opportunities are positively related to mental health, mitigating loneness and isolation [85]. Safety is a vital perceptional factor. A lower physical activity level has been documented in disadvantaged neighborhoods, which negatively affects residents’ health [15,33]. From a socio-cultural perspective, heritage and local culture are also vital for urban health and well-being. The summarized indicator system will be examined in the context of SMCs, with an emphasis on the public.
3. Methodology
The research process was conducted in three main stages (Figure 1). A comprehensive literature review was conducted to extract the preliminary factor series for the next step. The Web of Science dataset was searched, with the publishing period ranging from 2010 to 2023 (years included). Four study fields, urban studies, regional urban planning, geography, and architecture were considered. Only academic journals that had published at least three papers were considered.
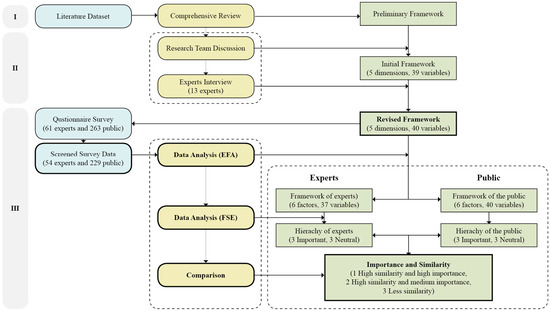
Figure 1.
Methodological flow chart (source: drawn by authors).
The preliminary framework was summarized in the literature review. The research team conducted three rounds of discussion, and five dimensions with 39 variables were prepared. Then, we conducted an expert interview using 13 professionals that are knowledgeable in the areas of architecture, urban planning and design, public health, and social workers. The experts were invited to give comments on the criteria derived from the previous step. One variable about public participation was added in this step. Finally, a questionnaire based on the revised variables was developed. Forty statements were categorized into five groups, namely, Health-Friendly Services, Urban Forms and Facilities, Green and Open Spaces, Environmental Quality and Energy, and Community and Governance. The importance of each variable was measured on a seven-point Likert scale, with seven indicating the highest importance. The questionnaire was also used to collect the respondents’ information, including socio-economic and career-related data. This information was used to distinguish between the experts and the public.
The same questionnaire was used to study the experts and the public. Compared with collecting expert and public views in different ways, using the same questionnaire can reveal different opinions from the same initial framework and context [21,22]. This method helped us to compare the priorities in a more fine-grained way. For the experts, in the beginning, the questionnaire survey was deliberately given to scholars who had published on a related topic. For the public, a small group of laypeople who are interested in urban issues were contacted first. Then, a snowball sampling method was adopted, in which the respondents were asked to disseminate the survey link to acquaintances to enlarge the sample size [86].
In total, 324 responses were collected in China. While the previous studies on SMCs were derived from the US [31], the EU [22], and South Africa [34], this study will provide more experiences from non-Western SMCs. The experts in this study are professionals working in architecture and urban planning institutions who often propose, decide on, and implement urban planning and development proposals. According to the working field data, 61 experts and 263 members of the public remained. Then, the respondents who self-selected “not familiar with the Healthy City concept (at all)” were excluded from data analysis (41). After data screening, a final total of 283 questionnaires, 54 from the experts and 229 from the public, were used in the data analysis (Table 1). In total, 69.61% of the respondents thought the framework was effective or highly effective. There were more female than male respondents (55.55% vs. 44.45%). As expected, more experts thought they were more familiar or very familiar with the SMC situation than the public (53.71% vs. 44.1%). In the expert group, the majority had at least six years of professional experience (59.26%), which means they are senior and more influential in their fields.

Table 1.
Respondent profiles.
4. Data Analysis and Findings
After obtaining the questionnaire data, we used EFA and FSE techniques to derive the framework and hierarchy from the experts and the public for further comparison. The primary purposes of the EFA are to identify the principal directions and remove sub-dimensions in the dataset with a minimal loss of information [87]. SPSS 26 was used for the EFA. After constructing the variables, we used an FSE to grasp each factor’s importance and ranked them [88].
In the EFA, Cronbach’s alpha values of 0.965 (experts) and 0.972 (public) show good reliability, indicating proper consistency among the responses. The Kaiser–Meyer–Olkin (KMO) test (experts 0.765 and public 0.955) shows adequate sampling for this study. As we adopted a seven-point Likert scale, we examined the mean scores of each variable and ranked each of them according to their mean value. No variable had a mean value below 4.0, which represents less importance in our case, so all the variables were further analyzed [89]. For the expert group, after component rotation, the variables of integrated development, ordinary life spaces, and biodiversity were deleted (coefficient value below 0.5). Six factors with 37 variables were validated using the EFA (Supplemental Table S1). For the public group, six factors with 40 variables were validated after component rotation using the EFA (Supplemental Table S2).
To further reveal the factors’ importance hierarchy, this study adopted the FSE technique. FSEs have been widely used for generating criteria ranking indexes [88]. Following similar studies, an FSE was conducted with six key steps [88,90,91]. The FSE results of the indices and importance levels for all the factors are shown in Table 2 and Table 3 and Supplemental Tables S3 and S4. The validated factors and variables were ranked and compared according to the importance index of each factor from the FSE and the factor loading of each variable from EFA (Figure 2).
Table 2.
Indices and importance levels for all factors of experts.
Table 3.
Indices and importance levels for all factors of public.
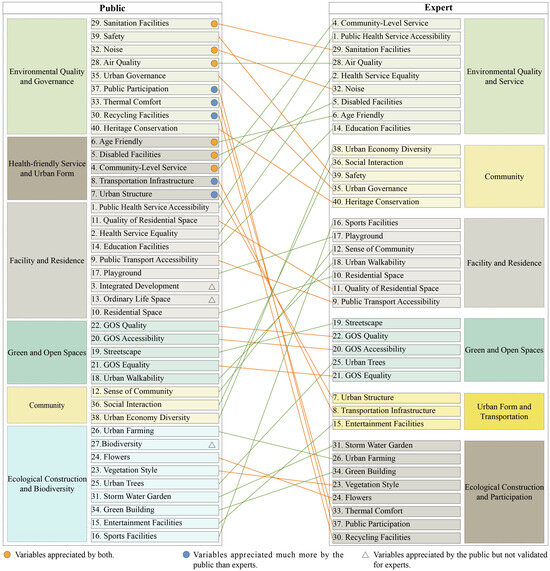
Figure 2.
Comparison of frameworks of experts and public (source: drawn by authors).
5. Discussion and Observations
Facing potential health inequity and expert bias in Healthy City construction, this study compares the values of experts and the public to achieve healthy SMCs. The compared results demonstrate both similarities and a mismatch of opinions between the experts and the public, allowing us to better understanding the values among these groups. Environmental Quality and Governance/Service (EQ) are appreciated as the most important factors by both the experts and the public. Facilities and Residences (FRs) and Green and Open Spaces (GOSs) are also appreciated by both the groups but with medium importance. The most obvious mismatch was for participation and urban form, which the public appreciated, but the experts did not. The identified factors and variables were discussed according to the similarities and importance ranked from high to low as follows (Figure 3):
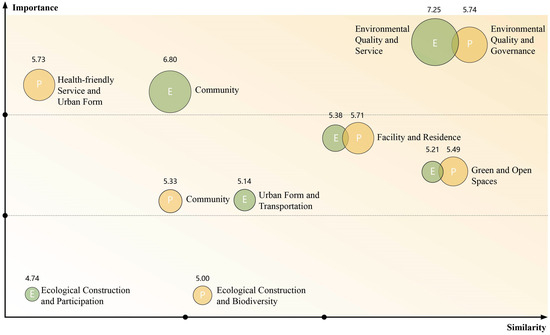
Figure 3.
Comparison of factors’ importance and similarities between experts and public (source: drawn by authors).
5.1. High Degrees of Similarity and Importance
Environmental Quality and Governance/Service (EQ) are both valued as the most important factors by the experts and the public (Figure 3) because EQ has the highest importance index among the experts (7.25, Table 2) and the public (5.74, Table 3). These factors emphasize both tangible aspects, such as Sanitation Facilities, and intangible ones, such as Noise and Air Quality, which have factor loadings of 0.726, 0.603, and 0.694 among the experts (Supplemental Table S1) and 0.732, 0.687, and 0.674 among the public (Supplemental Table S2). This finding reflects the public’s consensus and acceptance of those viables’ importance, acknowledging their help in stopping the spread of infectious diseases [11]. The importance of Sanitation Facilities probably reflects the inadequate provision of fundamental sanitation and hygiene services in SMCs. Sanitation facility construction and long-term maintenance are not usually affordable for individual regions, so they are heavily sponsored by the government, and, therefore, they need to be carefully placed and provided [34]. The importance of Air Quality deeply echoes the experiences of other SMCs [31], reflecting air pollutions’ strong impact on disadvantaged districts and groups [72]. To improve Environmental Quality, urban noise nuisances can be removed though legal regulations, zoning plans for the rationalization of spaces, and architectural structures, such as noise protection walls [78].
Within the EQ factor, it is also worth noting that the important variables include public participation, Thermal Comfort, and Recycling Facilities. They present obvious differences between the experts (factor loadings of 0.483, 0.608, and 0.542; Supplemental Table S1) and the public (factor loadings of 0.571, 0.562, and 0.533; Supplemental Table S2), indicating the public’s higher appreciation compared to that of the experts (Figure 2). The results possibly reveal a recessive gap between the importance that the experts attached to participation [82]. Though the role of social interaction in maintaining a healthy lifestyle has been well documented, practical public participation in decision-making processes remains lacking [83,85]. The importance of Thermal Comfort and Recycling Facilities emphasized by the public are in line with the previous studies about ameliorating the microclimate and improving the hygienic environment [79]. Efforts, including carefully selecting and planning trees in streets and in parks, should be made since windspeed and UV protection for pedestrians via tree shade could influence urban health [76].
5.2. High Similarity of Medium Importance
The experts and the public both highlighted the importance of Facilities and Residences (FRs), ranking third, with indexes of 5.38 (the experts, Table 2) and 5.71 (the public, Table 3). Public Health Service Accessibility (0.699, Supplemental Table S2) has the highest factor loading in the FR scores of the public. Similar to the previous empirical studies from big cities, it seems that accessing fundamental healthcare services is vital for urban health conditions, no matter the city scale [35]. Quality Residential Spaces have factor loadings of 0.506 among the experts and 0.602 among the public. As it is closely related to the daily life of residents, it is more important to the public. In the FR factor, it is worth to mention that two variables, Integrated Development (0.504) and Ordinary Life Spaces (0.476), are appreciated by the public, but not even validated in the framework of the experts. They emphasize that health facilities should be considered and integrated together with the surrounding neighborhood environment, rather than being isolated. Daily life facilities, including grocery stores, farmers’ markets, and traditional shops, are also essential for residents’ health.
We also found that the experts, as well as the public, generally appreciate Green and Open Spaces (GOSs), with indexes of 5.21 (experts) and 5.49 (the public). This result corresponds to several studies that have shown that Green and Open Spaces are an essential element associated with urban health [53,56,67]. In the GOS factor, the variable GOS Quality has factor loadings of 0.785 (experts) and 0.596 (public). GOS Accessibility has factor loadings of 0.771 (experts) and 0.595 (public), reflecting a similar consensus between the experts and the public. GOS Equality has factor loadings of 0.680 (experts) and 0.572 (public). The results show the extent to which these three variables perceived by the experts match up with their scores. It is worth noting that the public appreciates Streetscapes and Urban Walkability less than the experts do, indicating the possible overemphasis of these variables in elite planning. One aspect that can explain this result is that the majority of the existing Healthy City studies are based on big cities, while SMCs tend to be smaller in scale and more pedestrian-friendly as well.
5.3. Less Similarity
The results show the biggest discrepancy between Urban Form and Transportation (UFT) by the experts and the Health-Friendly Services and Urban Form (HFSs) of the public. Whereas HFSs rank second among the public (5.73, Table 3), UFT ranks second to last among the experts (5.14, Table 2). Two variables, Transportation Infrastructure and Urban Structure, received more attention from the public than that from the experts. Transportation Infrastructure is a much more important variable to the public than it is to the experts, concerning road density, network connectivity, and traffic jams. Consistent with the previous studies, the results of this study highlight the strong correlation between transportation planning and urban health [46], also enhancing the evidence from other SMCs [40]. The public also appreciates Urban Structure more than the experts do, emphasizing layout, density, land-use mix, polycentric forms, and job–housing distance, which further affects the residents’ lifestyle and health. It seems that the public are aware of the importance of urban structure planning, which can encourage the population to exercise more and reduce their exposure to noise, pollution, and accidents simultaneously [71,78]. The identified mismatch may also point to the necessity to improve Transportation Infrastructure and the Urban Structure through urban renewal and regeneration programs in SMCs.
There are also differences in how the experts and the public value Community (COM), as the experts (6.80, second) appreciate it much more than the public (5.33, fifth). It is possible that, in SMCs, people tend to have closer interactions and a stronger sense of community compared with that in big cities.
In summary, the identified mismatches (and similarities) in this study support the necessity of comparing expert and public perceptions [17,19,92], presenting a more complicated landscape beyond mere expert bias [21,22]. This study provides a fine-grained understanding of heterogeneous groups’ understanding of the same topic, with the inclusion of the public’s voice. In this sense, public stakeholder surveys might be necessary before urban initiatives are proposed to better reflect the people’s needs [19]. Regarding the essential factors of SMCs, the importance of Environmental Quality and Governance/Service (EQ) emphasized by both the experts and the public in this study further enhances the previous experiences [31,72]. This effect is possibly because EQ’s impact on health is direct and strong; both Urban Forms and GOSs affect health through EQ. The priority of EQ and FRs pointed out by the laypeople possibly reflects that the basic conditions in SMCs require more investment and attention.
Overall, the framework of the experts and the public validated in this study can be used to reinforce the development of healthy SMCs and fill the gap between elite expert assessments and the general public’s perception. These findings also highlight the importance of recognizing and acknowledging the inherent and unavoidable perceptions of people, even of those acting as experts [16]. This study provides a better understanding of the wider public’s opinions on achieving good urban health in SMCs in comparison with those of experts. More attention on improving urban governance to encourage and allow active public participation and engagement is recommended according to this study. While Healthy City studies are often focused on big cities, this study extends the topic by addressing SMCs with different ecological, economic, and social contexts. We also call for more Healthy City studies with varied development backgrounds. The methodology presented in this study offers one approach to increasing public input in planning processes that can be applied to other contexts and issues. From a practical aspect, the importance hierarchy indicates the scope for more communication and the exchanging of experiences among experts and the public. For the managers of Healthy City projects, creating opportunities for sharing opinions and values between varied groups is important. The highlighted factors in this study offer valuable insights and can be used as a reference for urban designers in future planning.
When interpreting the results and conducting future studies, some aspects should be borne in mind. First, this survey did not fully cover respondents of all ages and was not large due to time limits. Future studies could be conducted on a wider geographical scale to obtain a larger number of participants. While aging is a global phenomenon and achieving an aging-friendly city is becoming more important, more attention could be given to collecting data from elderly people. Second, though this study focuses on and defines the SMC context, the respondents of this survey were not limited to people who live in SMCs. Consequently, future studies could pay attention to residents in SMCs as they may have more lived experiences and perceptions of the issues in Healthy City construction.
6. Conclusions
As this study focuses on SMCs, with an emphasis on the public’s values, it has the potential to enhance health equality and further contribute to sustainable urban development for all. This contribution enhances the effects and importance of achieving Healthy Cities by answering the question “Healthy City for whom?”. While evidence of Healthy Cities has mainly emerged from big cities, this study has focused on SMCs, enriching the theoretical research by considering marginal city types. In this sense, this study also provides an approach to overcoming health inequality by hearing from easily ignored social groups, either the public or SMC citizens.
Key factors and important views of experts and the public were identified and compared in this study. The views of the experts and the public were aligned in appreciation of Environmental Quality and Governance/Service (EQ). This finding indicates that more action and attention from related sectors to protect the Environmental Quality of SMCs are necessary. However, while participation and Urban Forms are prioritized by the public, the experts were not strongly influenced by this particular set of beliefs. To better reflect the views of the public, involving them more via engagement events and activities is recommended in future Healthy City construction. Major deficiencies were identified between the experts’ and general public’s assessments in achieving healthy SMCs, providing an in-depth understanding of varied groups and indicating the necessity for more non-expert voices. This study highlighted the public’s input; better communication needs to be established between experts and the public so the experts can explain why certain values are considered important from a technical aspect and so they can understand and incorporate the views of the public. It is vital to achieve mutual understanding among heterogeneous stakeholders. With more exchanges, experts’ and non-experts’ opinions can be understood and combined in the shared vision of healthier cities.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/buildings14123769/s1, Table S1: Mean values, factor loading, percentage of variance explained, and cumulative percentage of the variance of all variables-experts; Table S2: Mean values, factor loading, percentage of variance explained, and cumulative percentage of the variance of all variables- the public; Table S3: Weightings and membership functions of all variables and factors-experts; Table S4: Weightings and membership functions of all variables and factors-the public.
Author Contributions
J.L.: Conceptualization, methodology, formal analysis, writing—review and editing. M.M.: Data curation, writing—original draft, visualization, validation. M.H.: Writing—review and editing, supervision. E.H.W.C.: Resources, conceptualization, writing—review and editing, funding acquisition. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the National Natural Science Foundation of China (No. 52078447). This research was funded by the National Social Science Fund of China (No. 24CSH073).
Data Availability Statement
The original contributions presented in the study are included in the article and supplementary material, further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Kleinert, S.; Horton, R. Urban design: An important future force for health and wellbeing. Lancet 2016, 388, 2848–2850. [Google Scholar] [CrossRef] [PubMed]
- Mehdipanah, R.; Novoa, A.M.; León-Gómez, B.B.; López, M.J.; Palència, L.; Vasquez, H.; Díez, È.; Borrell, C.; Pérez, K. Effects of Superblocks on health and health inequities: A proposed evaluation framework. J. Epidemiol. Community Health 2019, 73, 585–588. [Google Scholar] [CrossRef] [PubMed]
- Sho, K.; Fukuda, R.; Lim, H.; Kim, S.M.; Kidokoro, T. Self-consciousness inequality under spatial polarization: Evidence from growing and declining neighborhoods of Osaka City, Japan. Cities 2024, 148, 104846. [Google Scholar] [CrossRef]
- Yang, J.; Siri, J.G.; Remais, J.V.; Cheng, Q.; Zhang, H.; Chan, K.K.Y.; Sun, Z.; Zhao, Y.; Cong, N.; Li, X.; et al. The Tsinghua–Lancet Commission on Healthy Cities in China: Unlocking the power of cities for a healthy China. Lancet 2018, 391, 2140–2184. [Google Scholar] [CrossRef]
- Wen, Y.; Liu, B.; Li, Y.; Zhao, L. A Review of Research Progress on the Impact of Urban Street Environments on Physical Activity: A Comparison between China and Developed Countries. Buildings 2024, 14, 1779. [Google Scholar] [CrossRef]
- Gu, L.; Yang, L.; Wang, L.; Yu, J.; Wei, B. An exploratory study of neighbourhood heterogeneity in health: Evidence from China. Local Environ. 2020, 25, 787–809. [Google Scholar] [CrossRef]
- Mazhar, N.; Brown, R.D.; Kenny, N.; Lenzholzer, S. Thermal comfort of outdoor spaces in Lahore, Pakistan: Lessons for bioclimatic urban design in the context of global climate change. Landsc. Urban Plan. 2015, 138, 110–117. [Google Scholar] [CrossRef]
- Orga, F.; Mitchell, A.; Freixes, M.; Aletta, F.; Alsina-Pagès, R.M.; Foraster, M. Multilevel Annoyance Modelling of Short Environmental Sound Recordings. Sustainability 2021, 13, 5779. [Google Scholar] [CrossRef]
- Balsas, C.J.L. Exciting walk-only precincts in Asia, Europe and North-America. Cities 2021, 112, 103129. [Google Scholar] [CrossRef]
- Liu, D.; Zhao, L.-Y.; Yu, D.-M.; Ju, L.-H.; Zhang, J.; Wang, J.-Z.; Zhao, W.-H. Dietary patterns and association with obesity of children aged 6–17 years in medium and small cities in China: Findings from the CNHS 2010–2012. Nutrients 2019, 11, 3. [Google Scholar] [CrossRef]
- Vedachalam, S.; Riha, S.J. Who’s the cleanest of them all? Sanitation scores in Indian cities. Environ. Urban. 2015, 27, 117–136. [Google Scholar] [CrossRef]
- Bucko, A.G.; Porter, D.E.; Saunders, R.; Shirley, L.; Dowda, M.; Pate, R.R. Walkability indices and children’s walking behavior in rural vs. urban areas. Health Place 2021, 72, 102707. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Llamas, A.; García-Mayor, J.; De la Cruz-Sánchez, E. Urban-rural differences in trajectories of physical activity in Europe from 2002 to 2017. Health Place 2021, 69, 102570. [Google Scholar] [CrossRef] [PubMed]
- Webster, P.; Sanderson, D. Healthy Cities Indicators-A Suitable Instrument to Measure Health? J. Urban Health-Bull. N. Y. Acad. Med. 2013, 90, S52–S61. [Google Scholar] [CrossRef]
- Rivera-Navarro, J.; Bonilla, L.; Gullón, P.; González-Salgado, I.; Franco, M. Can we improve our neighbourhoods to be more physically active? Residents’ perceptions from a qualitative urban health inequalities study. Health Place 2021, 77, 102658. [Google Scholar] [CrossRef] [PubMed]
- Mizrahi, M. Arguments from expert opinion and persistent bias. Argumentation 2018, 32, 175–195. [Google Scholar] [CrossRef]
- Drijfhout, M.; Kendal, D.; Green, P. Mind the gap: Comparing expert and public opinions on managing overabundant koalas. J. Environ. Manag. 2022, 308, 114621. [Google Scholar] [CrossRef]
- Junge, X.; Hunziker, M.; Bauer, N.; Arnberger, A.; Olschewski, R. Invasive Alien Species in Switzerland: Awareness and Preferences of Experts and the Public. Environ. Manag. 2019, 63, 80–93. [Google Scholar] [CrossRef]
- Conrad, E.; Fazey, I.; Christie, M.; Galdies, C. Choosing landscapes for protection: Comparing expert and public views in Gozo, Malta. Landsc. Urban Plan. 2019, 191, 103621. [Google Scholar] [CrossRef]
- Galli, I.; Fasanelli, R. Public understanding of science and common sense: Social representations of the human microbiome among the expert and non-expert public. Health Psychol. Open 2020, 7, 2055102920913239. [Google Scholar] [CrossRef]
- Grover, S.; McClelland, A.; Furnham, A. Preferences for scarce medical resource allocation: Differences between experts and the general public and implications for the COVID-19 pandemic. Br. J. Health Psychol. 2020, 25, 889–901. [Google Scholar] [CrossRef] [PubMed]
- Dieteren, C.M.; Reckers-Droog, V.T.; Schrama, S.; de Boer, D.; van Exel, J. Viewpoints among experts and the public in the Netherlands on including a lifestyle criterion in the healthcare priority setting. Health Expect. Int. J. Public Particip. Health Care Health Policy 2022, 25, 333–344. [Google Scholar] [CrossRef] [PubMed]
- Kato-Nitta, N.; Maeda, T.; Inagaki, Y.; Tachikawa, M. Expert and public perceptions of gene-edited crops: Attitude changes in relation to scientific knowledge. Palgrave Commun. 2019, 5, 137. [Google Scholar] [CrossRef]
- Kendal, D.; Ford, R.M. The role of social license in conservation. Conserv. Biol. 2018, 32, 493–495. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.; Ruther, M.; Ehresman, S.; Nickerson, B. Placemaking as an Economic Development Strategy for Small and Midsized Cities. Urban Aff. Rev. 2017, 53, 435–462. [Google Scholar] [CrossRef]
- Dova, E.; Sivitanidou, A.; Anastasi, N.R.; Tzortzi, J.G.-N. A mega-event in a small city: Community participation, heritage and scale in the case of Pafos 2017 European Capital of Culture. Eur. Plan. Stud. 2022, 30, 457–477. [Google Scholar] [CrossRef]
- Michael, A.B. Downtown Revitalization in Small and Midsized Cities. In Planning Advisory Service Report; American Planning Association: Washington, DC, USA, 2018; 11p. [Google Scholar]
- Lau, K.K.-L.; Yung, C.C.-Y.; Tan, Z. Usage and perception of urban green space of older adults in the high-density city of Hong Kong. Urban For. Urban Green. 2021, 64, 127251. [Google Scholar] [CrossRef]
- Zhu, R.; Dong, X.; Wong, M.S. Estimation of the Urban Heat Island Effect in a Reformed Urban District: A Scenario-Based Study in Hong Kong. Sustainability 2022, 14, 4409. [Google Scholar] [CrossRef]
- Shao, J.; Yang, M.; Liu, G.; Li, Y.; Luo, D.; Tan, Y.; Zhang, Y.; Song, Q. Urban Sub-Center Design Framework Based on theWalkability Evaluation Method: Taking Coomera Town Sub-Center as an Example. Sustainability 2021, 13, 6259. [Google Scholar] [CrossRef]
- Masri, S.; Cox, K.; Flores, L.; Rea, J.; Wu, J. Community-Engaged Use of Low-Cost Sensors to Assess the Spatial Distribution of PM2.5 Concentrations across Disadvantaged Communities: Results from a Pilot Study in Santa Ana, CA. Atmosphere 2022, 13, 304. [Google Scholar] [CrossRef]
- McKee, G.A. The Hospital City in an Ethnic Enclave: Tufts-New England Medical Center, Boston’s Chinatown, and the Urban Political Economy of Health Care. J. Urban Hist. 2016, 42, 259–283. [Google Scholar] [CrossRef]
- Li, T.; Fang, Y.; Zeng, D.; Shi, Z.; Sharma, M.; Zeng, H.; Zhao, Y. Developing an indicator system for a healthy City: Taking an urban area as a pilot. Risk Manag. Healthc. Policy 2020, 13, 83. [Google Scholar] [CrossRef] [PubMed]
- Abrams, A.L.; Carden, K.; Teta, C.; Wågsæther, K. Water, sanitation, and hygiene vulnerability among rural areas and small towns in south Africa: Exploring the role of climate change, marginalization, and inequality. Water 2021, 13, 2810. [Google Scholar] [CrossRef]
- Jin, T.H.; Cheng, L.; Wang, K.; Cao, J.; Huang, H.; Witlox, F. Examining equity in accessibility to multi-tier healthcare services across different income households using estimated travel time. Transp. Policy 2022, 121, 1–13. [Google Scholar] [CrossRef]
- Reeder, T.; Locascio, E.; Tucker, J.; Czaplijski, T.; Benson, N.; Meggs, W. ED utilization: The effect of changing demographics from 1992 to 2000. Am. J. Emerg. Med. 2002, 20, 583–587. [Google Scholar] [CrossRef]
- Engïnöz, E.B.; Şavli, H. Examination of accessibility for disabled people at metro stations. Iconarp Int. J. Archit. Plan. 2016, 4, 34–48. [Google Scholar]
- Yung, E.H.K.; Conejos, S.; Chan, E.H.W. Social needs of the elderly and active aging in public open spaces in urban renewal. Cities 2016, 52, 114–122. [Google Scholar] [CrossRef]
- Chen, Y.; Bouferguene, A.; Shirgaokar, M.; Al-Hussein, M. Spatial Analysis Framework for Age-Restricted Communities Integrating Spatial Distribution and Accessibility Evaluation. J. Urban Plan. Dev. 2020, 146, 04019021. [Google Scholar] [CrossRef]
- Hynes, M.; Seoighthe, E. Heading in the Right Direction? Investigating Walkability in Galway City, Ireland. Urban Sci. 2018, 2, 31. [Google Scholar] [CrossRef]
- Zhang, F.; Song, T.; Cheng, X.; Li, T.; Yang, Z. Transportation infrastructure, population mobility, and public health. Int. J. Environ. Res. Public Health 2022, 20, 751. [Google Scholar] [CrossRef]
- Hu, Y.; Lin, Z.; Jiao, S.; Zhang, R. High-Density Communities and Infectious Disease Vulnerability: A Built Environment Perspective for Sustainable Health Development. Buildings 2024, 14, 103. [Google Scholar] [CrossRef]
- Sarkar, C.; Webster, C. Healthy Cities of Tomorrow: The Case for Large Scale Built Environment- Health Studies. J. Urban Health-Bull. N. Y. Acad. Med. 2017, 94, 4–19. [Google Scholar] [CrossRef]
- Lai, Y.; Kontokosta, C.E. Quantifying place: Analyzing the drivers of pedestrian activity in dense urban environments. Landsc. Urban Plan. 2018, 180, 166–178. [Google Scholar] [CrossRef]
- McCormack, G.R.; Koohsari, M.J.; Turley, L.; Nakaya, T.; Shibata, A.; Ishii, K.; Yasunaga, A.; Oka, K. Evidence for urban design and public health policy and practice: Space syntax metrics and neighborhood walking. Health Place 2021, 67, 102277. [Google Scholar] [CrossRef] [PubMed]
- Park, K.; Ewing, R.; Sabouri, S.; Choi, D.-A.; Hamidi, S.; Tian, G. Guidelines for a Polycentric Region to Reduce Vehicle Use and Increase Walking and Transit Use. J. Am. Plan. Assoc. 2020, 86, 236–249. [Google Scholar] [CrossRef]
- Bibri, S.E.; Krogstie, J. Smart Eco-City Strategies and Solutions for Sustainability: The Cases of Royal Seaport, Stockholm, andWestern Harbor, Malmo, Sweden. Urban Sci. 2020, 4, 11. [Google Scholar] [CrossRef]
- Wang, A.; Zheng, W.; Tan, Z.; Han, M.; Chan, E.H. Synergies and trade-offs in achieving sustainable targets of urban renewal: A decision-making support framework. Environ. Plan. B-Urban Anal. City Sci. 2024. [Google Scholar] [CrossRef]
- Peters, T.; Halleran, A. How our homes impact our health: Using a COVID-19 informed approach to examine urban apartment housing. Archnet-IJAR Int. J. Archit. Res. 2021, 15, 10–27. [Google Scholar] [CrossRef]
- Wang, S.; Esther, H.K.Y.; Yu, Y.; Tsou, J.Y. Right to the city and community facility planning for elderly: The case of urban renewal district in Hong Kong. Land Use Policy 2022, 114, 105978. [Google Scholar] [CrossRef]
- Karuppannan, S.; Sivam, A. Comparative analysis of utilisation of open space at neighbourhood level in three Asian cities: Singapore, Delhi and Kuala Lumpur. Urban Des. Int. 2013, 18, 145–164. [Google Scholar] [CrossRef]
- Marquet, O.; Hipp, J.A.; Alberico, C.; Huang, J.-H.; Fry, D.; Mazak, E.; Lovasi, G.S.; Floyd, M.F. Park use preferences and physical activity among ethnic minority children in low-income neighborhoods in New York City. Urban For. Urban Green. 2019, 38, 346–353. [Google Scholar] [CrossRef]
- Abass, K.; Serbeh, R. Public perceptions of the health benefits of green spaces in urban Ghana. Local Environ. 2023, 28, 967–978. [Google Scholar] [CrossRef]
- Simon-Friedt, B.R.; Pan, A.P.; Nisar, T.; Al-Kindi, S.; Nunley, A.; Graiff, L.; Kash, B.A.; Maddock, J.E.; Nasir, K. Effects of trail and greenspace exposure on hospitalisations in a highly populated urban area: Retrospective cohort study of the Houston Bayou Greenways program. Local Environ. 2023, 28, 365–378. [Google Scholar] [CrossRef]
- Wang, A.; Ho, D.C.W.; Lai, L.W.C.; Chau, K.W. Public preferences for government supply of public open space: A neo-institutional economic and lifecycle governance perspective. Cities 2023, 141, 104463. [Google Scholar] [CrossRef]
- Zhou, X.; Sho, K.; Qiu, H.; Chang, S.; Cen, Q. Longitudinal association between urban blue-green space exposure and mortality: A systematic review and meta-analysis of exposure types and buffers. Sustain. Cities Soc. 2024, 116, 105901. [Google Scholar] [CrossRef]
- Kumar, P.; Druckman, A.; Gallagher, J.; Gatersleben, B.; Allison, S.; Eisenman, T.S.; Hoang, U.; Hama, S.; Tiwari, A.; Sharma, A.; et al. The nexus between air pollution, green infrastructure and human health. Environ. Int. 2019, 133, 14. [Google Scholar] [CrossRef]
- Lee, S. Does tree canopy moderate the association between neighborhood walkability and street crime? Urban For. Urban Green. 2021, 65, 127336. [Google Scholar] [CrossRef]
- Zhao, W.; Tan, L.; Niu, S.; Qing, L. Assessing the Impact of Street Visual Environment on the Emotional Well-Being of Young Adults through Physiological Feedback and Deep Learning Technologies. Buildings 2024, 14, 1730. [Google Scholar] [CrossRef]
- Zhang, Y.; Tang, H.; Huo, K.; Tang, J. Research on Urban Community Street Environment Evaluation and Optimization Strategy under the Concept of a Healthy City: A Case Study of the Dingwangtai Area of Changsha City. Buildings 2024, 14, 2449. [Google Scholar] [CrossRef]
- Hidalgo, A.K. Mental health in winter cities: The effect of vegetation on streets. Urban For. Urban Green. 2021, 63, 127226. [Google Scholar] [CrossRef]
- Alawadi, K.; Striedinger, V.H.; Maghelal, P.; Khanal, A. Assessing walkability in hot arid regions: The case of downtown Abu Dhabi. Urban Des. Int. 2020, 27, 211–231. [Google Scholar] [CrossRef]
- Li, Y.; Tang, H. Health-Oriented Evaluation and Optimization of Urban Square Space Elderly Suitability: A Case Study of Yiyang City Center. Buildings 2024, 14, 2482. [Google Scholar] [CrossRef]
- Mears, M.; Brindley, P.; Maheswaran, R.; Jorgensen, A. Understanding the socioeconomic equity of publicly accessible greenspace distribution: The example of Sheffield, UK. Geoforum 2019, 103, 126–137. [Google Scholar] [CrossRef]
- Mak, B.K.; Jim, C. Examining fear-evoking factors in urban parks in Hong Kong. Landsc. Urban Plan. 2018, 171, 42–56. [Google Scholar] [CrossRef]
- Koohsari, M.J.; Badland, H.; Mavoa, S.; Villanueva, K.; Francis, J.; Hooper, P.; Owen, N.; Giles-Corti, B. Are public open space attributes associated with walking and depression? Cities 2018, 74, 119–125. [Google Scholar] [CrossRef]
- Palardy, N.P.; Boley, B.B.; Gaither, C.J. Resident support for urban greenways across diverse neighborhoods: Comparing two Atlanta BeltLine segments. Landsc. Urban Plan. 2018, 180, 223–233. [Google Scholar] [CrossRef]
- Zhang, X.; Melbourne, S.; Sarkar, C.; Chiaradia, A.; Webster, C. Effects of green space on walking: Does size, shape and density matter? Urban Stud. 2020, 57, 3402–3420. [Google Scholar] [CrossRef]
- Apfelbeck, B.; Snep, R.P.; Hauck, T.E.; Ferguson, J.; Holy, M.; Jakoby, C.; MacIvor, J.S.; Schär, L.; Taylor, M.; Weisser, W.W. Designing wildlife-inclusive cities that support human-animal co-existence. Landsc. Urban Plan. 2020, 200, 103817. [Google Scholar] [CrossRef]
- Cameron, R.W.F.; Brindley, P.; Mears, M.; McEwan, K.; Ferguson, F.; Sheffield, D.; Jorgensen, A.; Riley, J.; Goodrick, J.; Ballard, L.; et al. Where the wild things are! Do urban green spaces with greater avian biodiversity promote more positive emotions in humans? Urban Ecosyst. 2020, 23, 301–317. [Google Scholar] [CrossRef]
- Ramirez, E. Triangular blocks and wind tunnels: Augustin Rey’s logic of air resistance. J. Archit. 2014, 19, 272–291. [Google Scholar] [CrossRef]
- Grigorieva, E.; Lukyanets, A. Combined Effect of Hot Weather and Outdoor Air Pollution on Respiratory Health: Literature Review. Atmosphere 2021, 12, 790. [Google Scholar] [CrossRef]
- Porse, E. Open data and stormwater systems in Los Angeles: Applications for equitable green infrastructure. Local Environ. 2018, 23, 505–517. [Google Scholar] [CrossRef]
- Tsegaye, S.; Singleton, T.L.; Koeser, A.K.; Lamb, D.S.; Landry, S.M.; Lu, S.; Barber, J.B.; Hilbert, D.R.; Hamilton, K.O.; Northrop, R.J.; et al. Transitioning from gray to green (G2G)-A green infrastructure planning tool for the urban forest. Urban For. Urban Green. 2019, 40, 204–214. [Google Scholar] [CrossRef]
- Ozer, E. Mutualistic relationships versus hyper-efficiencies in the sustainable building and city. Urban Ecosyst. 2014, 17, 195–204. [Google Scholar] [CrossRef]
- Brown, R.D.; Vanos, J.; Kenny, N.; Lenzholzer, S. Designing urban parks that ameliorate the effects of climate change. Landsc. Urban Plan. 2015, 138, 118–131. [Google Scholar] [CrossRef]
- Zhou, H.; Tao, G.; Yan, X.; Sun, J. Influences of greening and structures on urban thermal environments: A case study in Xuzhou City, China. Urban For. Urban Green. 2021, 66, 127386. [Google Scholar] [CrossRef]
- Jasper, S. Sonic refugia: Nature, noise abatement and landscape design in West Berlin. J. Archit. 2018, 23, 936–960. [Google Scholar] [CrossRef]
- Middel, A.; Häb, K.; Brazel, A.J.; Martin, C.A.; Guhathakurta, S. Impact of urban form and design on mid-afternoon microclimate in Phoenix Local Climate Zones. Landsc. Urban Plan. 2014, 122, 16–28. [Google Scholar] [CrossRef]
- Hanssen, G.S. The Social Sustainable City: How to Involve Children in Designing and Planning for Urban Childhoods? Urban Plan. 2019, 4, 53–66. [Google Scholar] [CrossRef]
- Pearson, M.; Lebow-Skelley, E.; Whitaker, L.; Young, L.; Warren, C.B.; Williamson, D.; Kegler, M.C. Implementation of a community grant program to address community-driven environmental health concerns. Local Environ. 2020, 25, 830–848. [Google Scholar] [CrossRef]
- Wang, A.Q.; Chan, E.H.W. The impact of power-geometry in participatory planning on urban greening. Urban For. Urban Green. 2020, 48, 126571. [Google Scholar] [CrossRef]
- Delgado-Baena, A.; Sianes, A. Power Dynamics in Collaborative Governance Processes: A Case Study of a Disadvantaged Neighbourhood in Southern Spain. Buildings 2024, 14, 1002. [Google Scholar] [CrossRef]
- Elsorady, D.A. Revitalisation of Downtown Khedive Cairo: A contested sovereignty. Cities 2018, 73, 51–62. [Google Scholar] [CrossRef]
- Hillier, A.; Han, B.; Eisenman, T.S.; Evenson, K.R.; McKenzie, T.L.; Cohen, D.A. Using Systematic Observations to Understand Conditions that Promote Interracial Experiences in Neighbourhood Parks. Urban Plan. 2016, 1, 51–64. [Google Scholar] [CrossRef]
- Hamilton-MacLaren, F.; Loveday, D.L.; Mourshed, M. Public opinions on alternative lower carbon wall construction techniques for UK housing. Habitat Int. 2013, 37, 163–169. [Google Scholar] [CrossRef]
- Yung, E.H.K.; Zhang, Q.; Chan, E.H.W. Underlying social factors for evaluating heritage conservation in urban renewal districts. Habitat Int. 2017, 66, 135–148. [Google Scholar] [CrossRef]
- Haider, H.; Hewage, K.; Umer, A.; Ruparathna, R.; Chhipi-Shrestha, G.; Culver, K.; Holland, M.; Kay, J.; Sadiq, R. Sustainability assessment framework for small-sized urban neighbourhoods: An application of fuzzy synthetic evaluation. Sustain. Cities Soc. 2018, 36, 21–32. [Google Scholar] [CrossRef]
- Chan, E.H.W.; Hou, J. Developing a framework to appraise the critical success factors of transfer development rights (TDRs) for built heritage conservation. Habitat Int. 2015, 46, 35–43. [Google Scholar] [CrossRef]
- Liu, J.; Li, Q.; Wang, Y. Risk analysis in ultra deep scientific drilling project—A fuzzy synthetic evaluation approach. Int. J. Proj. Manag. 2013, 31, 449–458. [Google Scholar] [CrossRef]
- Osei-Kyei, R.; Chan, A.P.C.; Ameyaw, E.E. A fuzzy synthetic evaluation analysis of operational management critical success factors for public-private partnership infrastructure projects. Benchmarking Int. J. 2017, 24, 2092–2112. [Google Scholar] [CrossRef]
- Gjerde, M. Visual evaluation of urban streetscapes: How do public preferences reconcile with those held by experts? Urban Des. Int. 2011, 16, 153–161. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).