
Use of Porous Titanium Trabecular as a Bone Defect Regenerator: In Vivo Study



Abstract
:1. Introduction
- Make a mechanical study of this porous titanium implant
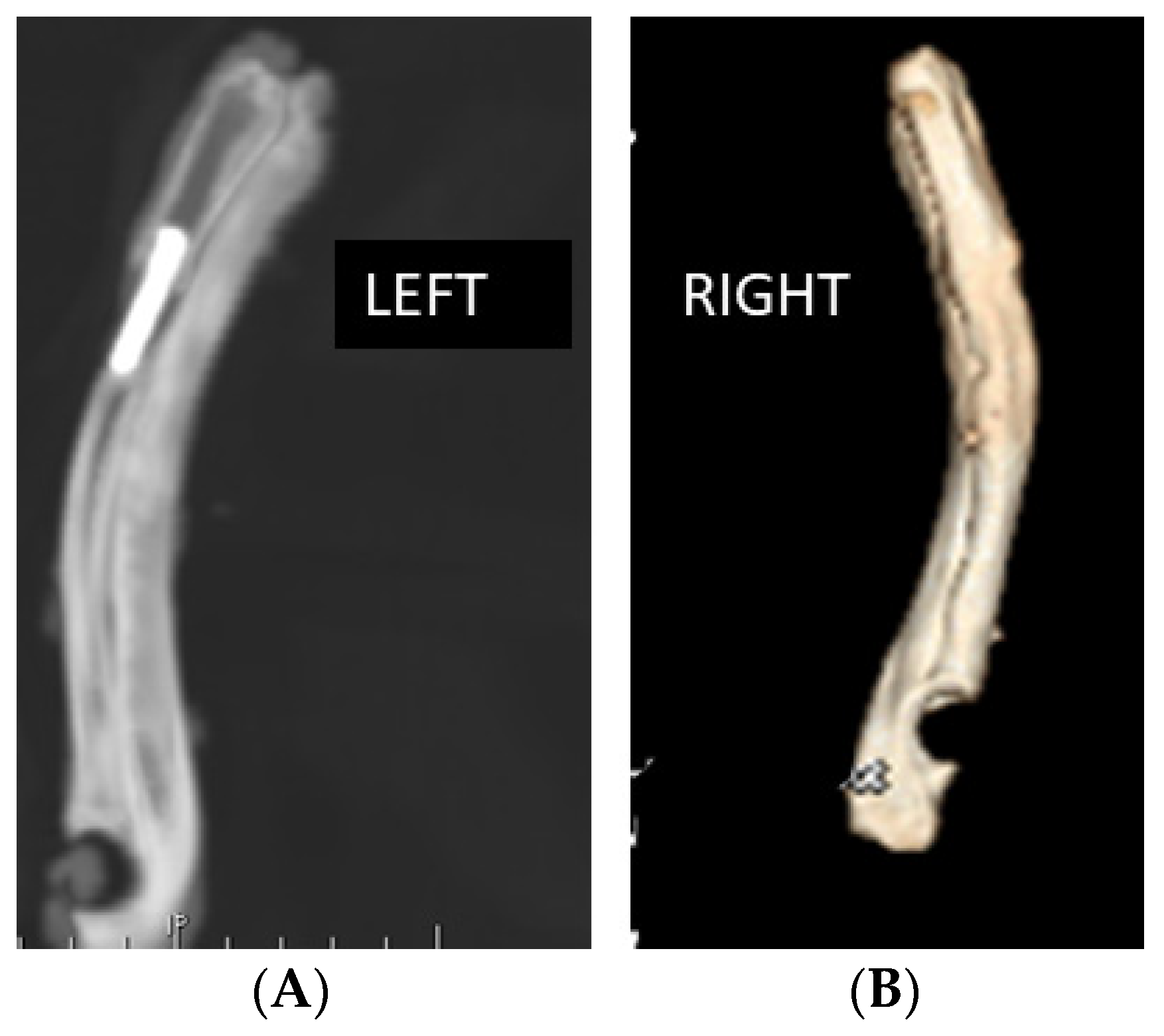
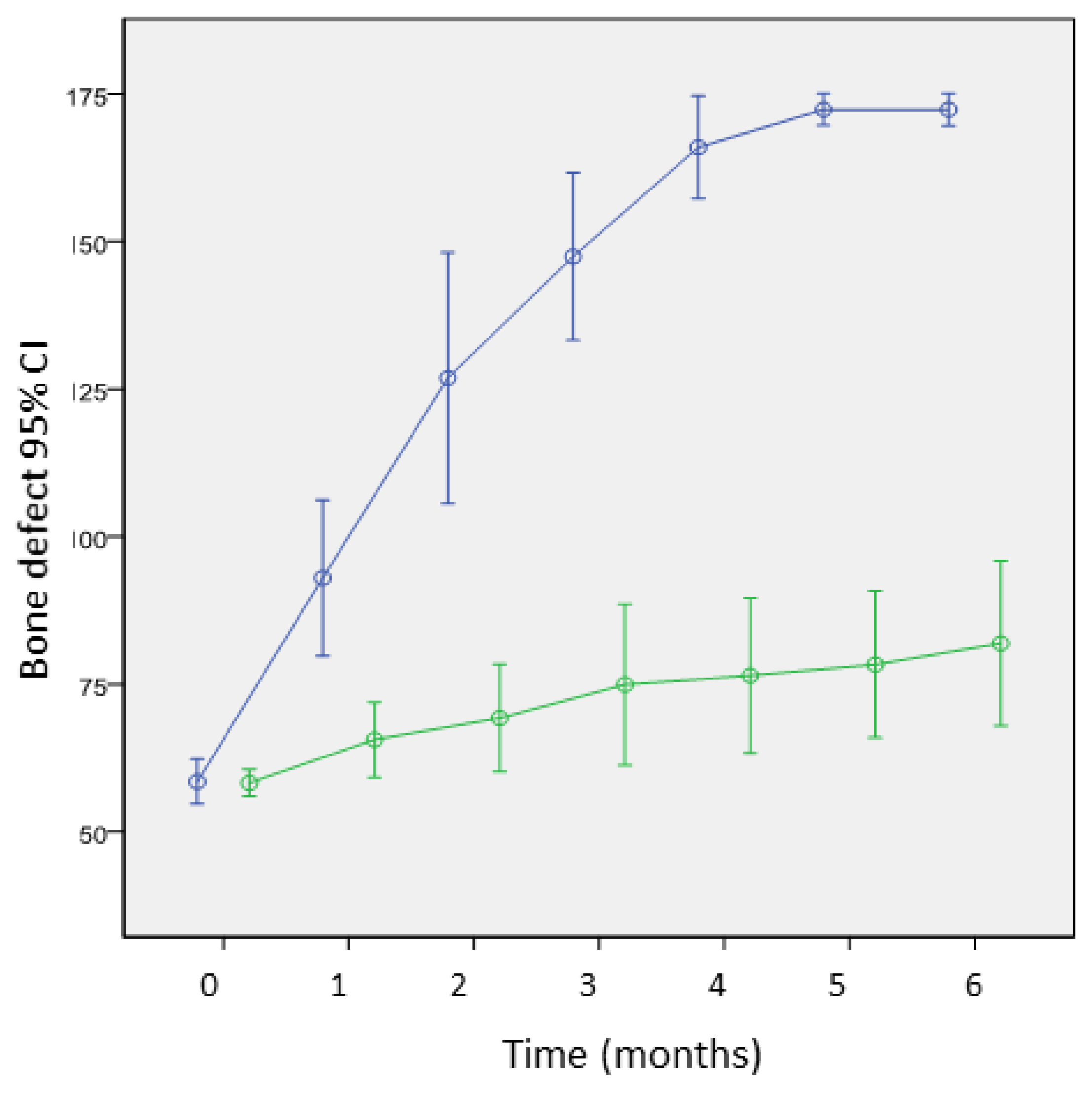
- Evaluate and compare bone regeneration in both groups (experimental and control) with image diagnosed techniques (simple x-ray, scanner) and morphodensitometric analysis
- Evaluate the bone regeneration in both groups with histologic techniques: optical microscopy, transmission and scanning electron microscopy and morphodensitometric analysis
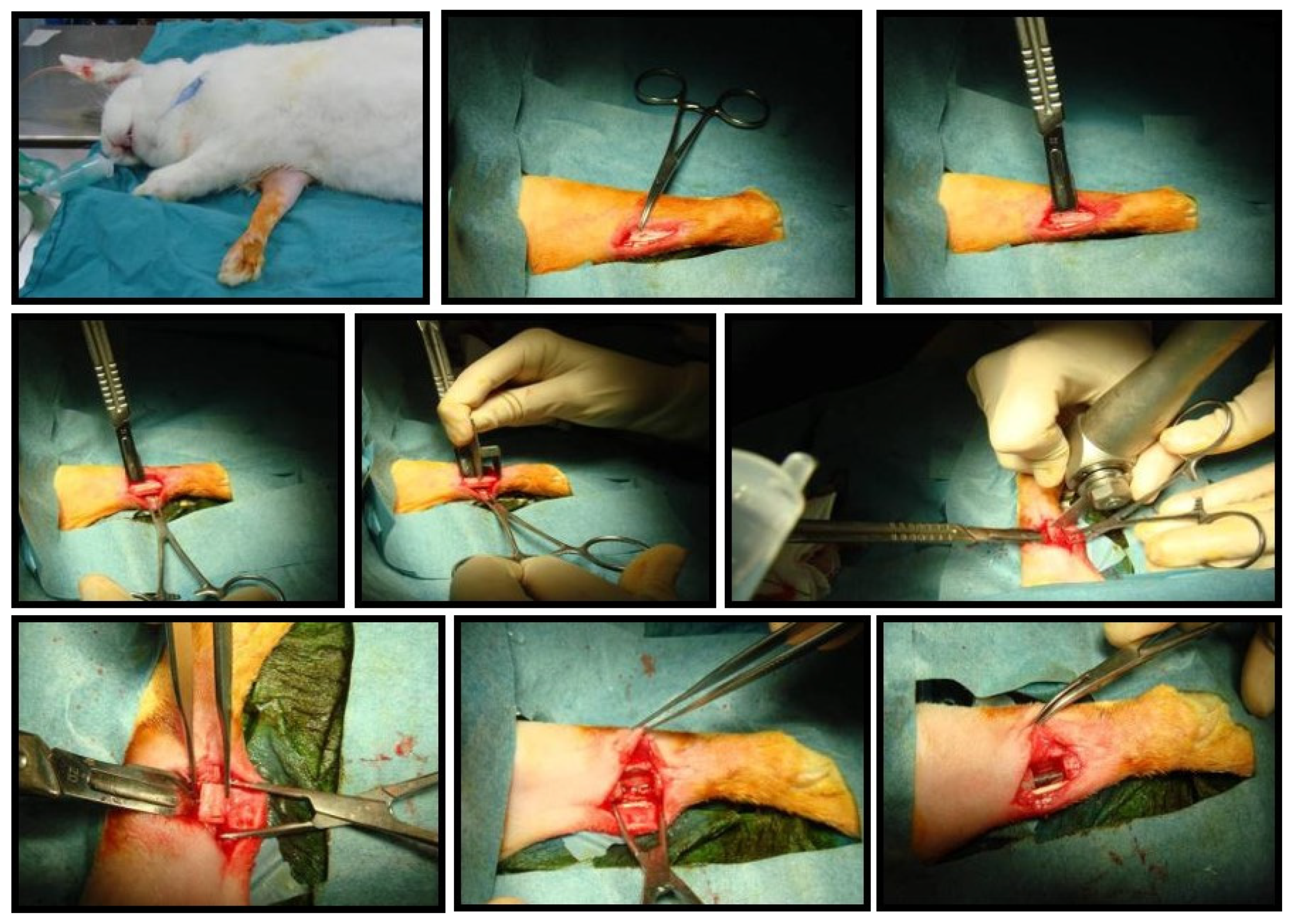
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fujibayashi, S.; Neo, M.; Kim, H.M.; Kokubo, T.; Nakamura, T. Osteoinduction of bioactive titanium metal. In Key Engineering Materials; Trans Tech Publications Ltd.: Freienbach, Switzerland, 2004; Volume 254, pp. 953–956. [Google Scholar]
- Cheng, X.Y.Y.; Li, S.J.J.; Murr, L.E.E. Compression deformation behavior of Ti-6Al-4V alloy with cellular structures fabricatedby electron beam melting. J. Mech. Behav. Biomed. Mater. 2012, 16, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Spoerke, E.D.; Murray, N.G.; Li, H.; Brinson, L.C.; Dunand, D.C.; Stupp, S.I. A bioactive titanium foam scaffold for bone repair. Acta Biomater. 2005, 1, 523–533. [Google Scholar] [CrossRef]
- Wang, X.; Xu, S.; Zhou, S.; Xu, W.; Leary, M.; Choong, P.; Qian, M.; Brandt, M.; Xie, Y.M. Topological design and additive manufacturing of porous metals for bone scaffolds and orthopaedic implants: A review. Biomaterials 2016, 83, 127–141. [Google Scholar]
- Abate, K.M.; Nazir, A.; Jeng, J.-Y. Design, optimization, and selective laser melting of vin tiles cellular structure-based hip implant. Int. J. Adv. Manuf. Technol. 2021, 112, 2037–2050. [Google Scholar] [CrossRef]
- Pałka, K.; Pokrowiecki, R. Porous Titanium Implants: A Review. Adv. Eng. Mater. 2018, 20, 1700648. [Google Scholar] [CrossRef]
- Dabrowski, B.; Swieszkowski, W.; Godlinski, D.; Kurzydlowski, K.J. Highly porous titanium scaffolds for orthopaedic applications. J. Biomed. Mater. Res. 2010, 95, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Bobyn, J.D.; Pilliar, R.M.; Cameron, H.U.; Weatherly, G.C. The optimum pore size for the fixation of porous surfaced metal im-plants by the ingrowth of bone. Clin. Orthop. Relat. Res. 1980, 150, 263–270. [Google Scholar] [CrossRef]
- Beaupré, G.S.; Orr, T.E.; Carter, D.R. An approach for time-dependent bone modeling and remodeling—Theoretical development. J. Orthop. Res. 1990, 8, 651–661. [Google Scholar] [CrossRef]
- Abate, K.M.; Nazir, A.; Chen, J.-E.; Jeng, J.-Y. Design, Optimization, and Evaluation of Additively Manufactured Vintiles Cellular Structure for Acetabular Cup Implant. Processes 2020, 8, 25. [Google Scholar] [CrossRef] [Green Version]
- Caparros, C.; Guillem-Martí, J.; Punset, M.; Molmeneu, M.; Calero, J.; Gil, F.J. Mechanical properties and in vitro biological response to porous titanium alloys for intervertebrae implants. J. Mech. Behav. Biomed. Mater. 2014, 39, 79–86. [Google Scholar] [CrossRef]
- Caparrós, C.; Ortiz-Hernandez, M.; Molmeneu, M.; Punset, M.; Calero, J.A.; Aparicio, C.; Fernández-Fairén, M.; Pérez, R.A.; Gil, F.J. Bioactive macroporous titanium implants highly interconnected. J. Mater. Sci. Mater. Med. 2016, 27, 151. [Google Scholar] [CrossRef]
- Ortiz-Hernandez, M.; Rappe, K.S.; Molmeneu, M.; Mas-Moruno, C.; Guillem-Marti, J.; Punset, M.; Caparros, C.; Calero, J.; Franch, J.; Fernandez-Fairen, M.; et al. Two Different Strategies to Enhance Osseointegration in Porous Titanium: Inorganic Thermo-Chemical Treatment Versus Organic Coating by Peptide Adsorption. Int. J. Mol. Sci. 2018, 19, 2574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez-Contreras, A.; Punset, M.; Calero, J.A.; Gil, F.J.; Ruperez, E.; Manero, J.M. Powder metallurgy with space holder for porous titanium implants: A review. J. Mater. Sci. Technol. 2021, 76, 129–149. [Google Scholar] [CrossRef]
- Jafari, M.S.; Bender, B.; Coyle, C.; Parvizi, J.; Sharkey, P.F.; Hozack, W.J. Do Tantalum and Titanium Cups Show Similar Results in Revision Hip Arthroplasty? Clin. Orthop. Relat. Res. 2010, 468, 459–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reikeras, O.; Gunderson, R.B. Failure of HA coating on a grit-blasted acetabular cup: 155 patients followed for 7–10 years. Acta Orthop. Scand. 2002, 73, 104–108. [Google Scholar] [CrossRef]
- Rodriguez, J.A. Acetabular fixation options: Notes from the otherside. J. Arthroplast. 2006, 21, 93–96. [Google Scholar] [CrossRef] [PubMed]
- Siegmeth, A.; Duncan, C.P.; Masri, B.A.; Kim, W.Y.; Garbuz, D.S. Modular tantalum augments for acetabular defects in revision hiparthroplasty. Clin. Orthop. Relat. Res. 2009, 467, 199–205. [Google Scholar] [CrossRef] [Green Version]
- Rupérez, E.; Manero, J.M.; Ricciardi, K.; Li, Y.; Aparicio, C.; Gil, F.J. Development of tantalum scaffold for orthopaedic applications produced by space-holder method. Mater. Des. 2015, 83, 112–119. [Google Scholar] [CrossRef] [Green Version]
- Nazir, A.; Abate, K.M.; Kumar, A.; Jeng, J.-Y. A state-of-the-art review on types, design, optimization, and additive manufacturing of cellular structures. Int. J. Adv. Manuf. Technol. 2019, 104, 3489–3510. [Google Scholar] [CrossRef]
- IUPAC. Manual os Symbols and Terminology, Appendix 2, Pt. 1, Colloid and Surface Chemistry. Pure Appl. Chem. 1972, 31, 578. [Google Scholar]
- St Pierre, J.P.; Gauthier, M.; Lefebvre, L.P.; Tabrizian, M. Three-dimensional growth of differentiating MC3T3-El pre-osteoblast on porous titanium scaffolds. Biomaterials 2005, 26, 7319–7328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, C.E.; Yamada, Y.; Shimojima, K.; Chino, Y.; Asahina, T.; Mabuchi, M. Processing and mechanical properties of autogenous titanium implant materials. J. Mater. Sci. Mater. Med. 2002, 13, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Habibovic, L.J.P.; Van den Doel, P.; Wilson, M.F.; De Wijn, C.E.; Van Blitterswijk, C.A. Bone ingrowth in porous titanium implants produced by 3D fiber deposition. Biomaterials 2007, 28, 2810–2820. [Google Scholar]
- Li, J.P.; de Wijn, J.R.; Van Blitterswijk, C.A.; De Groot, K. Porous Ti6Al4Vscaffolds directly fabricated by 3D fibre deposition technique: Effect of nozzle diameter. J. Mater. Sci. Mater. Med. 2005, 16, 1159–1163. [Google Scholar] [CrossRef]
- Pamula, E.; Bacakova, L.; Filova, E.; Buczynska, J.; Dobrzynski, P.; Noskova, L.; Grausova, L. The influence of pore size on colonization of poly (l-lactide glycolide) scaffolds with human osteoblast like MG 63 cells in vitro. J. Mater. Sci. Mater. Med. 2008, 19, 425–435. [Google Scholar] [CrossRef] [PubMed]
- Sicchieri, L.G.; Crippa, G.E.; de Oliveira, P.T.; Beloti, M.M.; Rosa, A.L. Pore size regulates cell and tissue interactions with PLGA-CaP scaffolds used for bone engineering. J. Tissue Eng. Regen. Med. 2012, 6, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Rappe, K.S.; Ortiz-Hernandez, M.; Punset, M.; Molmeneu, M.; Barba, A.; Mas-Moruno, C.; Guillem-Marti, J.; Caparrós, C.; Rupérez, E.; Calero, J.; et al. On-Growth and In-Growth Osseointegration Enhancement in PM Porous Ti-Scaffolds by Two Different Bioactivation Strategies: Alkali Thermochemical Treatment and RGD Peptide Coating. Int. J. Mol. Sci. 2022, 23, 1750. [Google Scholar] [CrossRef]
- Teixeira, L.N.; Crippa, G.E.; Lefebvre, L.P.; De Oliveira, P.T.; Rosa, A.L.; Beloti, M.M. The influence of pore size on osteoblast phenotype expression in cultures grown on porous titanium. Int. J. Oral Maxillofac. Surg. 2012, 41, 1097–1101. [Google Scholar] [CrossRef] [Green Version]
- Fujibayashi, S.; Neo, M.; Kim, H.M.; Kokubo, T.; Nakamura, T. Osteoinduction of porous bioactive titanium metal. Biomaterials 2004, 25, 443–450. [Google Scholar] [CrossRef]
- Tamai, N.; Myoui, A.; Tomita, T.; Nakase, T.; Tanaka, J.; Ochi, T.; Yoshikawa, H. Novel hydroxyapatite ceramics with an interconnective porous structure exhibit superior osteoconduction in vivo. J. Biomed. Mater. Res. 2002, 59, 110–117. [Google Scholar] [CrossRef]
- Flatley, T.J.; Lynch, K.L.; Benson, M. Tissue response to implants of calcium phosphate ceramic in the rabbit spine. Clin. Orthop. 1983, 179, 246–252. [Google Scholar] [CrossRef]
- Hulbert, S.F.; Morrison, S.J.; Klawitter, J.J. Tissue reaction to three ceramics of porous and non-porous structures. J. Biomed. Mater. Res. 1972, 6, 347–374. [Google Scholar] [CrossRef]
- Brånemark, R.; Öhrnell, L.O.; Nilsson, P.; Thomsen, P. Biomechanical characterization of osseointegration during healing an experimental in vivo study in the rato. Biomaterials 1997, 18, 969–978. [Google Scholar] [CrossRef]
- Dhert, W.J.A.; Thomsen, P.; Blomgren, A.K.; Esposito, M.; Ericson, L.E.; Verbout, A.J. Integration os press-fit implants in cortical bone: A study on interface kinetics. J. Biomed. Mater. Res. 1998, 41, 574–583. [Google Scholar] [CrossRef]
- Hanawa, T.; Kamiura, Y.; Yamamoto, S. Early bone formation around calcium-ion implanted titanium inserted into rat tibia. J. Biomed. Mater. Res. 1997, 36, 131–136. [Google Scholar] [CrossRef]
- Cole, B.J.; Bostrom, M.P.; Pritchard, T.L.; Sumner, D.R.; Tomin, E.; Lane, J.M.; Weiland, A.J. Use of bone morphogenetic protein 2 on ectopic porous coated implants in the rat. Clin. Orthop. 1997, 345, 219–228. [Google Scholar] [CrossRef]
- Vehof, J.W.M.; Spauwen, P.H.M.; Jansen, J.A. Bone formation in calcium-phosphate-coated titanium mesh. Biomaterials 2000, 21, 2003–2009. [Google Scholar] [CrossRef]
- Ferretti, C.; Ripamonti, U. Human segmental mandibular defects treated with naturally derived bone morphogenetic proteins. J. Craniofac. Surg. 2002, 13, 434–444. [Google Scholar] [CrossRef]
- Hoyos-Nogues, M.; Velasco, E.; Ginebra, M.P.; Manero, J.M.; Gil, J.; Mas-Moruno, C. Regenerating bone via multifunctional coatings: The blending of cell integration and bacterial inhibition properties on the surface of biomaterials. ACS Appl. Mater. Interfaces 2017, 9, 21618–21630. [Google Scholar] [CrossRef] [PubMed]
- Yuan, H.; de Bruijn, J.D.; Li, Y.; Feng, J.; Yang, Z.; de Groot, K.; Zhang, X. Bone formation induced by calcium phosphate ceramics in soft tissue of dogs: A comparative study between porous a-TCP and B-TCP. J. Mater. Sci. Mater. Med. 2001, 12, 7–13. [Google Scholar] [CrossRef]
- Zhang, X. The osteoinductivity of Ca-P biomaterials and the potential in clinic. In Proceedings of the Asian BioCeramics, Gyeongju, Korea, 24–26 October 2002; pp. 21–24. [Google Scholar]
- Meinig, R.P. Polylactide membranes in the treatment of segmental diaphyseal defects: Animal model experiments in the rabbit radius, sheep tibia, Yucatan minipig radius, and goat tibia. Injury 2002, 33 (Suppl. 2), B58–B65. [Google Scholar] [CrossRef]
- Mosheiff, R.; Friedman, A.; Friedman, M.; Liebergall, M. Quantification of guided regeneration of weight-bearing bones. Orthopedics 2003, 26, 789–794. [Google Scholar] [CrossRef] [PubMed]
- Giardino, R.; Fini, M.; Aldini, N.N.; Giavaresi, G.; Rocca, M.; Martini, L.; Zaffe, D.; Canè, V. A reabsorbable tubular chamber for the treatment of large diaphyseal bone defects. Experimental study in rabbits. Int. J. Artif. Organs 1998, 21, 473–482. [Google Scholar]
- Nyman, R.; Magnusson, M.; Sennerby, L.; Nyman, S.; Lundgren, D. Membrane-guided bone regeneration. Segmental radius defects studied in the rabbit. Acta Orthop. Scand. 1995, 66, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Roberts, W.; Smith, R.K.; Zilberman, Y.; Mozsary, P.G.; Smith, R.S. Osseous adaptation to continuous loading of rigid endosseous implants. Am. J. Orthod. 1984, 86, 95–111. [Google Scholar] [CrossRef]
- Bobyn, J.D.; Pilliar, R.M.; Cameron, H.U.; Weatherly, G.C. Osteogenic phenomena across endosteal bone-implant spaces with porous-surfaced intramedullary implants. Acta Orthop. Scand. 1981, 52, 145–153. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mechanical Tests | Elastic Modulus (GPa) | Yield Strength (MPa) | Maximal Strength (MPa) |
|---|---|---|---|
| Compression | K = 9.0 ± 0.9 | 67.7 ± 3.5 | 249 ± 15 |
| Flexion | E = 7.6 ± 0.5 | 61.5 ± 3.9 | 105 ± 20 |
| Tension | E = 13.6 ± 1.7 | 63.1 ± 2.5 | 70 ± 11 |
| Torsion | G = 7.7 ± 0.4 | 33.1 ± 3.5 | 62 ± 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torres Pérez, A.I.; Fernández Fairén, M.; Torres Pérez, Á.A.; Gil Mur, J. Use of Porous Titanium Trabecular as a Bone Defect Regenerator: In Vivo Study. Metals 2022, 12, 327. https://doi.org/10.3390/met12020327
Torres Pérez AI, Fernández Fairén M, Torres Pérez ÁA, Gil Mur J. Use of Porous Titanium Trabecular as a Bone Defect Regenerator: In Vivo Study. Metals. 2022; 12(2):327. https://doi.org/10.3390/met12020327
Chicago/Turabian StyleTorres Pérez, Ana Isabel, Mariano Fernández Fairén, Ángel Antonio Torres Pérez, and Javier Gil Mur. 2022. "Use of Porous Titanium Trabecular as a Bone Defect Regenerator: In Vivo Study" Metals 12, no. 2: 327. https://doi.org/10.3390/met12020327
APA StyleTorres Pérez, A. I., Fernández Fairén, M., Torres Pérez, Á. A., & Gil Mur, J. (2022). Use of Porous Titanium Trabecular as a Bone Defect Regenerator: In Vivo Study. Metals, 12(2), 327. https://doi.org/10.3390/met12020327