Heart Rate Variability, Neuromuscular and Perceptual Recovery Following Resistance Training



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.2.1. Experimental Design
2.2.2. Heart Rate Variability
2.2.3. Ten Repetition Maximum
2.2.4. Neuromuscular Performance
2.2.5. Perceptual Markers
2.2.6. Resistance Training Protocol
2.3. Statistical Analysis
3. Results
3.1. Model Effects
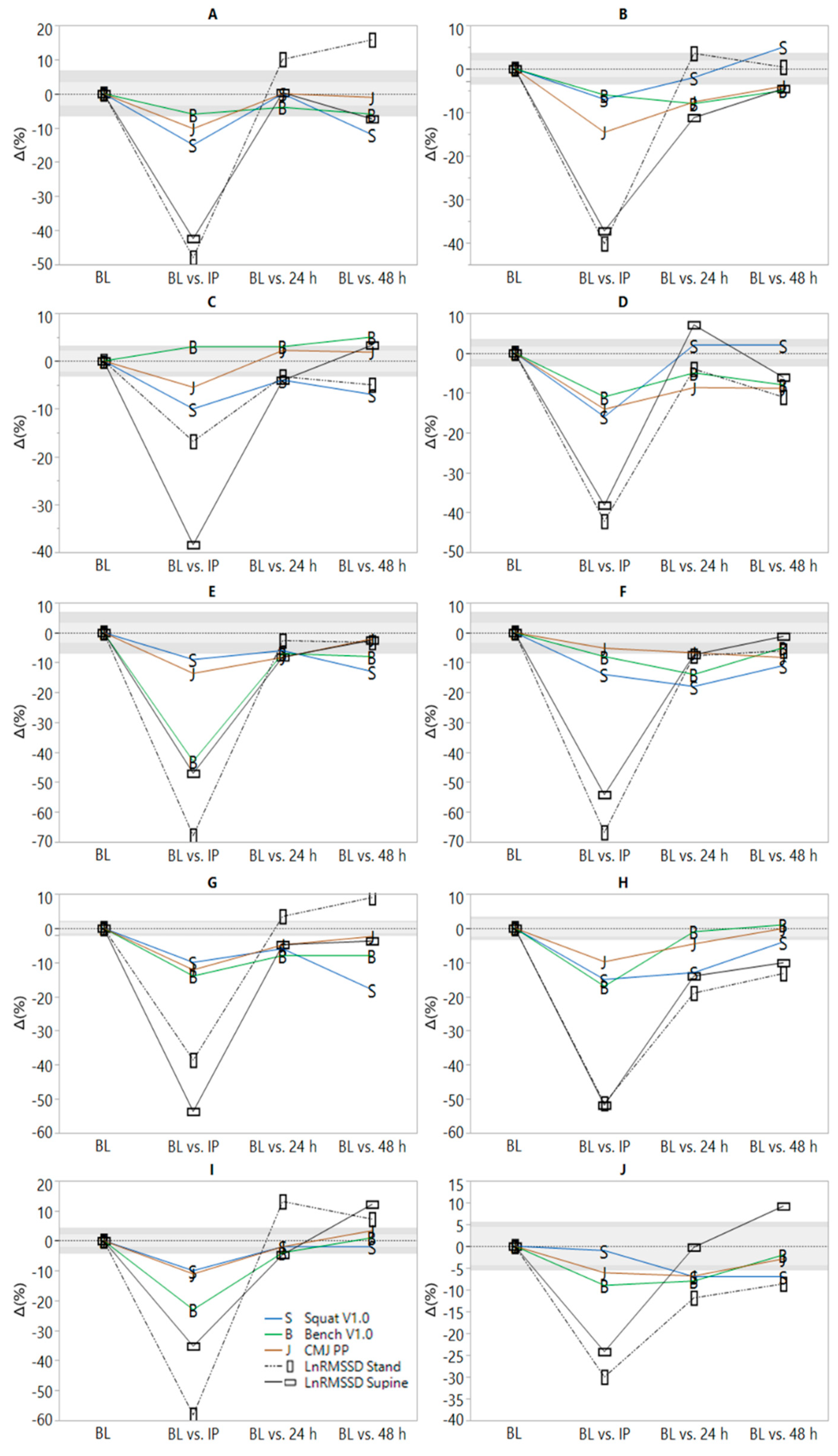
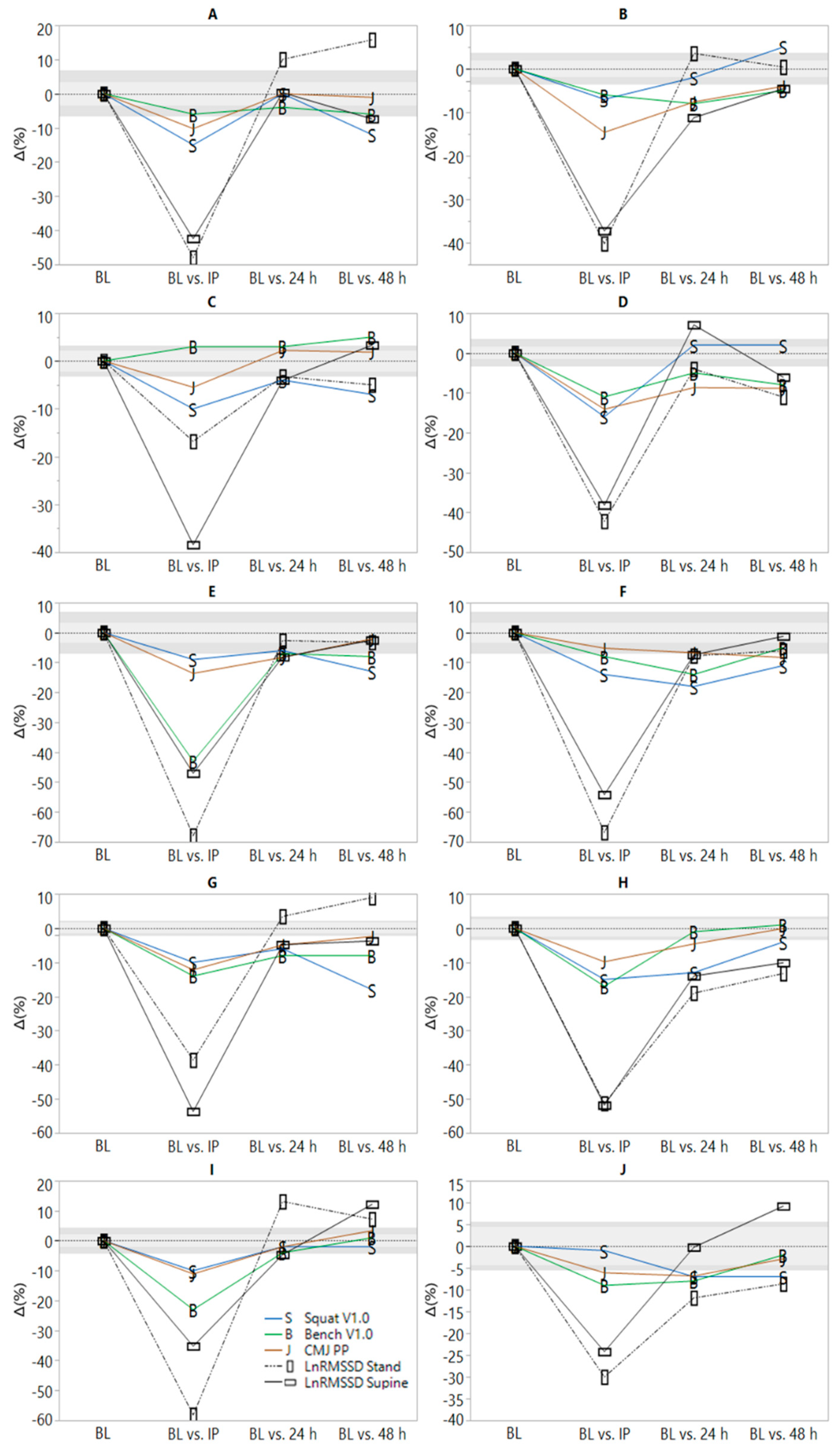
3.2. Associations
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- McMillan, J.L.; Stone, M.H.; Sartin, J.; Keith, R.; Marples, D.; Brown, C.; Lewis, R.D. 20-hour physiological responses to a single weight-training session. J. Strength Cond. Res. 1993, 7, 9–21. [Google Scholar]
- González-Badillo, J.; Rodríguez-Rosell, D.; Sánchez-Medina, L.; Ribas, J.; López-López, C.; Mora-Custodio, R.; Yañez-García, J.; Pareja-Blanco, F. Short-term recovery following resistance exercise leading or not to failure. Int. J. Sports Med. 2016, 37, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Ide, B.N.; Leme, T.C.; Lopes, C.R.; Moreira, A.; Dechechi, C.J.; Sarraipa, M.F.; Da Mota, G.R.; Brenzikofer, R.; Macedo, D.V. Time course of strength and power recovery after resistance training with different movement velocities. J. Strength Cond. Res. 2011, 25, 2025–2033. [Google Scholar] [CrossRef] [PubMed]
- Jones, E.J.; Bishop, P.A.; Richardson, M.T.; Smith, J.F. Stability of a practical measure of recovery from resistance training. J. Strength. Cond. Res. 2006, 20, 756. [Google Scholar]
- Mann, J.B.; Thyfault, J.P.; Ivey, P.A.; Sayers, S.P. The effect of autoregulatory progressive resistance exercise vs. Linear periodization on strength improvement in college athletes. J. Strength Cond. Res. 2010, 24, 1718–1723. [Google Scholar] [CrossRef]
- Chen, J.-l.; Yeh, D.-P.; Lee, J.-P.; Chen, C.-Y.; Huang, C.-Y.; Lee, S.-D.; Chen, C.-C.; Kuo, T.B.; Kao, C.-L.; Kuo, C.-H. Parasympathetic nervous activity mirrors recovery status in weightlifting performance after training. J. Strength Cond. Res. 2011, 25, 1546–1552. [Google Scholar] [CrossRef]
- Jovanović, M.; Flanagan, E.P. Researched applications of velocity based strength training. J. Aust. Strength Cond. 2014, 22, 58–69. [Google Scholar]
- Watkins, C.M.; Barillas, S.R.; Wong, M.A.; Archer, D.C.; Dobbs, I.J.; Lockie, R.G.; Coburn, J.W.; Tran, T.T.; Brown, L.E. Determination of vertical jump as a measure of neuromuscular readiness and fatigue. J. Strength Cond. Res. 2017, 31, 3305–3310. [Google Scholar] [CrossRef]
- Laurent, C.M.; Green, J.M.; Bishop, P.A.; Sjökvist, J.; Schumacker, R.E.; Richardson, M.T.; Curtner-Smith, M. A practical approach to monitoring recovery: Development of a perceived recovery status scale. J. Strength Cond. Res. 2011, 25, 620–628. [Google Scholar] [CrossRef]
- Sikorski, E.M.; Wilson, J.M.; Lowery, R.P.; Joy, J.M.; Laurent, C.M.; Wilson, S.M.; Hesson, D.; Naimo, M.A.; Averbuch, B.; Gilchrist, P. Changes in perceived recovery status scale following high-volume muscle damaging resistance exercise. J. Strength Cond. Res. 2013, 27, 2079–2085. [Google Scholar] [CrossRef]
- Stone, M.; Keith, R.; Kearney, J.; Fleck, S.; Wilson, G.; Triplett, N. Overtraining: A review of the signs, symptoms and possible causes. J. Strength Cond. Res. 1991, 5, 35–50. [Google Scholar] [CrossRef]
- De Souza, J.C.; Tibana, R.A.; Cavaglieri, C.R.; Vieira, D.C.L.; De Sousa, N.M.F.; Dos Santos, M.F.A.; Tajra, V.; Martins, W.R.; De Farias, D.L.; Balsamo, S. Resistance exercise leading to failure versus not to failure: Effects on cardiovascular control. BMC Cardiovasc. Disord. 2013, 13, 105. [Google Scholar] [CrossRef] [PubMed]
- Pareja-Blanco, F.; Rodríguez-Rosell, D.; Sánchez-Medina, L.; Ribas-Serna, J.; López-López, C.; Mora-Custodio, R.; Yáñez-García, J.M.; González-Badillo, J.J. Acute and delayed response to resistance exercise leading or not leading to muscle failure. Clin. Physiol. Funct. Imaging 2017, 37, 630–639. [Google Scholar] [CrossRef] [PubMed]
- Flatt, A.A.; Esco, M.R. Validity of the ithletetm smart phone application for determining ultra-short-term heart rate variability. J. Hum. Kinet. 2013, 39, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.; Booton, T.; Watson, M.; Rowland, D.; Altini, M. Heart rate variability is a moderating factor in the workload-injury relationship of competitive crossfit™ athletes. J. Sports Sci. Med. 2017, 16, 443. [Google Scholar]
- De Oliveira, R.M.; Ugrinowitsch, C.; Kingsley, J.D.; da Silva, D.G.; Bittencourt, D.; Caruso, F.R.; Borghi-Silva, A.; Libardi, C.A. Effect of individualized resistance training prescription with heart rate variability on individual muscle hypertrophy and strength responses. Eur. J. Sports Sci. 2019, 19, 1–9. [Google Scholar] [CrossRef]
- Schneider, C.; Wiewelhove, T.; Raeder, C.; Flatt, A.A.; Hoos, O.; Hottenrott, L.; Schumbera, O.; Kellmann, M.; Meyer, T.; Pfeiffer, M. Heart rate variability monitoring during strength and high-intensity interval training overload microcycles. Front. Physiol. 2019, 10, 582. [Google Scholar] [CrossRef]
- Flatt, A.A.; Howells, D. Effects of varying training load on heart rate variability and running performance among an olympic rugby sevens team. J. Sci. Med. Sport 2018, 22, 222–226. [Google Scholar] [CrossRef]
- Flatt, A.; Esco, M. Heart rate variability stabilization in athletes: Towards more convenient data acquisition. Clin. Physiol. Funct. Imaging 2016, 36, 331–336. [Google Scholar] [CrossRef]
- Nakamura, F.Y.; Flatt, A.A.; Pereira, L.A.; Ramirez-Campillo, R.; Loturco, I.; Esco, M.R. Ultra-short-term heart rate variability is sensitive to training effects in team sports players. J. Sports Sci. Med. 2015, 14, 602. [Google Scholar]
- Perrotta, A.S.; Jeklin, A.T.; Hives, B.A.; Meanwell, L.E.; Warburton, D.E. Validity of the elite hrv smartphone application for examining heart rate variability in a field-based setting. J. Strength Cond. Res. 2017, 31, 2296–2302. [Google Scholar] [CrossRef] [PubMed]
- Buchheit, M. Monitoring training status with hr measures: Do all roads lead to rome? Front. Physiol. 2014, 5, 73. [Google Scholar] [CrossRef] [PubMed]
- McElveen, M.T.; Riemann, B.L.; Davies, G.J. Bilateral comparison of propulsion mechanics during single-leg vertical jumping. J. Strength Cond. Res. 2010, 24, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Gathercole, R.; Sporer, B.; Stellingwerff, T.; Sleivert, G. Alternative countermovement-jump analysis to quantify acute neuromuscular fatigue. Int. J. Sports Physiol. Perf. 2015, 10, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Garnacho-Castaño, M.V.; López-Lastra, S.; Maté-Muñoz, J.L. Reliability and validity assessment of a linear position transducer. J. Sports Sci. Med. 2015, 14, 128–136. [Google Scholar] [PubMed]
- García-Ramos, A.; Haff, G.G.; Padial, P.; Feriche, B. Reliability of power and velocity variables collected during the traditional and ballistic bench press exercise. Sports Biomech. 2018, 17, 117–130. [Google Scholar] [CrossRef] [PubMed]
- Fritz, C.O.; Morris, P.E.; Richler, J.J. Effect size estimates: Current use, calculations, and interpretation. J. Exp. Psychol. Gen. 2012, 141, 2–18. [Google Scholar] [CrossRef]
- Hopkins, W.; Marshall, S.; Batterham, A.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef]
- Batterham, A.M.; Hopkins, W.G. Making meaningful inferences about magnitudes. Int. J. Sports Physiol. Perf. 2006, 1, 50–57. [Google Scholar] [CrossRef]
- Plews, D.J.; Laursen, P.B.; Kilding, A.E.; Buchheit, M. Heart rate variability in elite triathletes, is variation in variability the key to effective training? A case comparison. Eur. J. Appl. Physiol. 2012, 112, 3729–3741. [Google Scholar] [CrossRef]
- Flatt, A.A.; Esco, M.R.; Nakamura, F.Y. Association between subjective indicators of recovery status and heart rate variability among divison-1 sprint-swimmers. Sports 2018, 6, 93. [Google Scholar] [CrossRef] [PubMed]
- Stanley, J.; Peake, J.M.; Buchheit, M. Cardiac parasympathetic reactivation following exercise: Implications for training prescription. Sports Med. 2013, 43, 1259–1277. [Google Scholar] [CrossRef] [PubMed]
- Dousset, E.; Avela, J.; Ishikawa, M.; Kallio, J.; Kuitunen, S.; Kyrolainen, H.; Linnamo, V.; Komi, P.V. Bimodal recovery pattern in human skeletal muscle induced by exhaustive stretch-shortening cycle exercise. Med. Sci. Sports Exerc. 2007, 39, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Cheung, K.; Hume, P.A.; Maxwell, L. Delayed onset muscle soreness. Sports Med. 2003, 33, 145–164. [Google Scholar] [CrossRef] [PubMed]
- Mclester, J.R.; Bishop, P.A.; Smith, J.; Wyers, L.; Dale, B.; Kozusko, J.; Richardson, M.; Nevett, M.E.; Lomax, R. A series of studies—A practical protocol for testing muscular endurance recovery. J. Strength Cond. Res. 2003, 17, 259–273. [Google Scholar]

{kind=link}
| External Load | Load (kg) | Repetitions | Volume Load (kg) |
|---|---|---|---|
| Squat | 94.7 ± 12.7 | 62.7 ± 10.3 | 5952 ± 1310 |
| Bench Press | 81.1 ± 11.6 | 38.8 ± 4.5 | 3122 ± 480 |
| Pull-Down | 50.5 ± 6.6 | 42.2 ± 7.6 | 2098 ± 282 |
| Total Volume | - | - | 11,173 ± 1441 |
| Internal Load | Peak (b∙min−1) | Mean (b∙min−1) | - |
| HRex | 177.5 ± 14.7 | 136.4 ± 19.2 | - |
| Recovery Metric | Pre/BL | IP | 24 h P | 48 h P | Model Effect (p) |
|---|---|---|---|---|---|
| Supine LnRMSSD | 4.38 ± 0.74 | 2.32 ± 0.48 *V | 4.18 ± 0.81 S | 4.31 ± 0.59 | <0.0001 |
| Standing LnRMSSD | 3.45 ± 0.32 | 1.83 ± 0.56 *V | 3.38 ± 0.47 | 3.40 ± 0.48 | <0.0001 |
| CMJ Peak Power (W) | 4877 ± 432 | 4375 ± 404 *M | 4636 ± 321 *M | 4754 ± 427 S | <0.001 |
| Squat V1.0 (m·s−1) | 1.00 (0.00) | 0.90 (0.07) *V | 0.95 (0.07) *V | 0.93 (0.11) V | 0.002 |
| Bench Press V1.0 (m·s−1) | 1.00 (0.00) | 0.90 (0.13) *V | 0.94 (0.05) *V | 0.95 (0.09) L | 0.002 |
| Perceived Soreness (au) | 1.00 (1.25) | 5.50 (4.00) *V | 5.50 (3.25) *V | 6.50 (3.00) *V | <0.001 |
| Perceived Recovery (au) | 8.50 (2.00) | 4.00 (3.00) *V | 5.00 (1.50) *V | 6.50 (3.25) *V | 0.001 |
| Recovery Metric | ∆LnRMSSD Supine (%) | ∆LnRMSSD Standing (%) | ||
|---|---|---|---|---|
| 24 h P | 48 h P | 24 h P | 48 h P | |
| ∆Squat V1.0 (%) | r = 0.58 | r = 0.04 | r = 0.63 | r = −0.38 |
| ∆Bench Press V1.0 (%) | r = −0.06 | r = 0.45 | r = −0.08 | r = −0.23 |
| ∆CMJ Peak Power (%) | r = 0.04 | r = 0.39 | r = 0.35 | r = 0.36 |
| ∆Perceived Recovery (au) | r = −0.01 | r = −0.36 | r = 0.50 | r = 0.06 |
| ∆Perceived Soreness (au) | r = −0.01 | r = −0.37 | r = −0.58 | r = −0.47 |
| Total Volume Load (kg) | r = 0.16 | r = −0.10 | r = −0.41 | r = −0.47 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flatt, A.A.; Globensky, L.; Bass, E.; Sapp, B.L.; Riemann, B.L. Heart Rate Variability, Neuromuscular and Perceptual Recovery Following Resistance Training. Sports 2019, 7, 225. https://doi.org/10.3390/sports7100225
Flatt AA, Globensky L, Bass E, Sapp BL, Riemann BL. Heart Rate Variability, Neuromuscular and Perceptual Recovery Following Resistance Training. Sports. 2019; 7(10):225. https://doi.org/10.3390/sports7100225
Chicago/Turabian StyleFlatt, Andrew A., Liam Globensky, Evan Bass, Brooke L. Sapp, and Bryan L. Riemann. 2019. "Heart Rate Variability, Neuromuscular and Perceptual Recovery Following Resistance Training" Sports 7, no. 10: 225. https://doi.org/10.3390/sports7100225
APA StyleFlatt, A. A., Globensky, L., Bass, E., Sapp, B. L., & Riemann, B. L. (2019). Heart Rate Variability, Neuromuscular and Perceptual Recovery Following Resistance Training. Sports, 7(10), 225. https://doi.org/10.3390/sports7100225