
A Predictive Model of Regional Dementia Prevalence Using Geographic Weighted Regression Analysis


Abstract
:1. Introduction
- We identify the interregional spatial dependence of dementia prevalence in Korea.
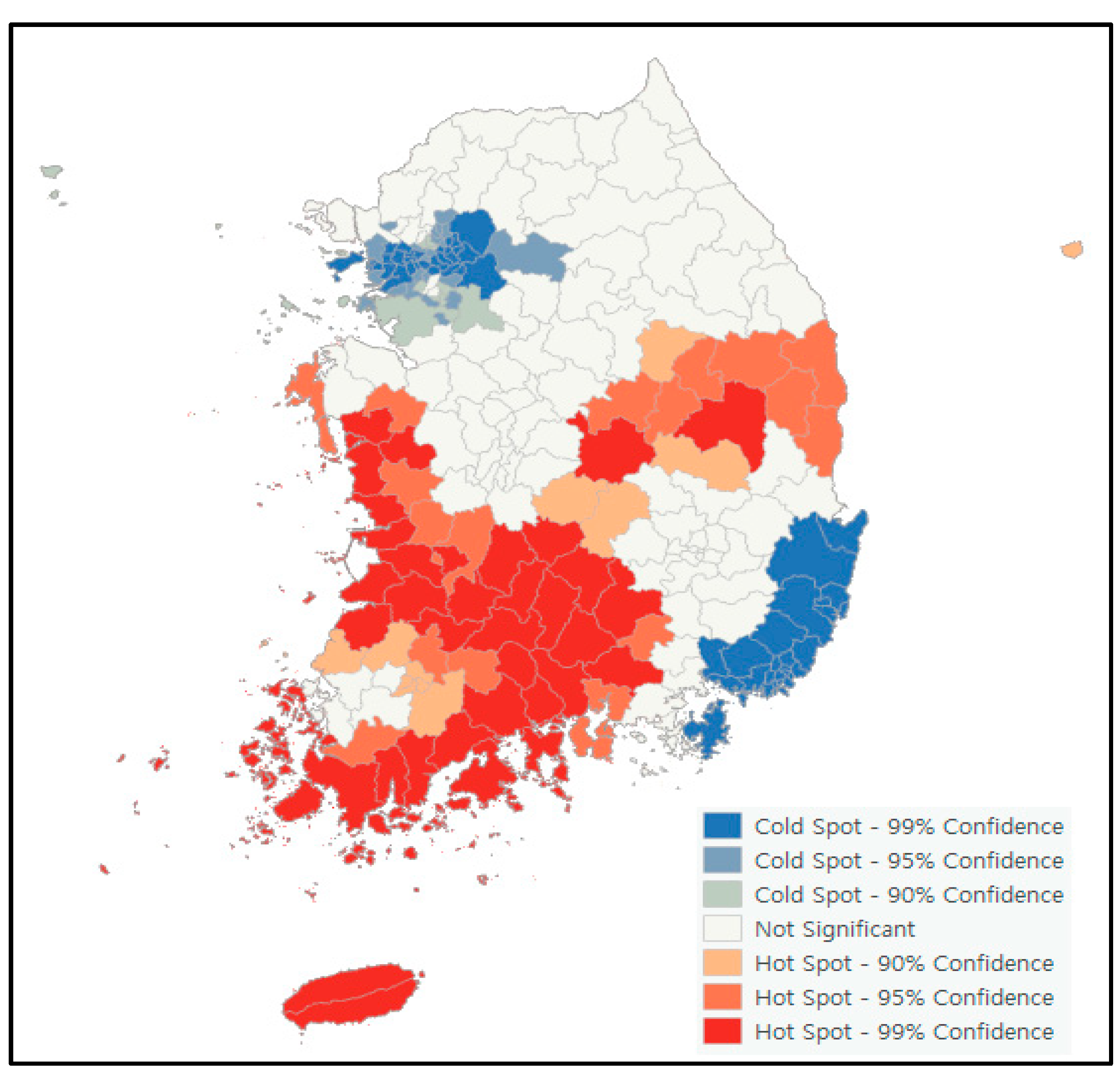
- We identify clusters in regions with high dementia prevalence through hot spot analysis.
- We identify risk factors for dementia prevalence in Korea through geographic weighted regression analysis.
2. Materials and Methods
2.1. Data Collection
2.2. Variables and Measures
2.3. Statistical Analysis
3. Results
3.1. General Characteristics of the Study Regions
3.2. Spatial Autocorrelation (Global Moran’s I) Analysis of Dementia Prevalence
3.3. Hot Spot Analysis of Dementia Prevalence
3.4. Geographically Weighted Regression Analysis in Risk Factors of Dementia Prevalence
3.5. Priorities of Dementia Prevalence Management
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Macintyre, S.; Ellaway, A.; Cummins, S. Place effects on health: How can we conceptualise, operationalise and measure them? Soc. Sci. Med. 2002, 55, 125–139. [Google Scholar] [CrossRef]
- Macintyre, S.; Ellaway, A. Ecological approaches: Rediscovering the role of the physical and social environment. Soc. Epidemiol. 2000, 9, 332–348. [Google Scholar]
- Jeong, B. Policy and regional health planning for reducing regional health inequalities. In Health Welfare Policy Forum; KIHASA: Yeongi-gun, Korea, 2018; pp. 50–61. [Google Scholar]
- Prince, M.J.; Wimo, A.; Guerchet, M.M.; Ali, G.C.; Wu, Y.-T.; Prina, M. World Alzheimer Report 2015-The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends; Alzheimer’s Disease International: London, UK, 2015. [Google Scholar]
- Gustafson, L. What is dementia? Acta Neurol. Scand. 1996, 94, 22–24. [Google Scholar] [CrossRef]
- Cleary, O.; McAvoy, H. Brain Health and Dementia Prevention in Ireland: A Discussion Paper; IPH: Dublin, Ireland, 2014. [Google Scholar]
- Norton, S.; Matthews, F.E.; Barnes, D.E.; Yaffe, K.; Brayne, C. Potential for primary prevention of Alzheimer’s disease: An analysis of population-based data. Lancet Neurol. 2014, 13, 788–794. [Google Scholar] [CrossRef]
- Kim, J.; Cheon, S.; Lim, J. IoT-Based Unobtrusive Physical Activity Monitoring System for Predicting Dementia. IEEE Access 2022, 10, 26078–26089. [Google Scholar] [CrossRef]
- Savva, G.M.; Stephan, B.C.; Alzheimer’s Society Vascular Dementia Systematic Review Group. Epidemiological studies of the effect of stroke on incident dementia: A systematic review. Stroke 2010, 41, e41–e46. [Google Scholar] [CrossRef] [PubMed]
- Kwak, H.-S.; Park, J.-H. A systematic review of the application nonpharmacological cognitive interventions in patients with dementia. Korean J. Occup. Ther. 2018, 26, 13–26. [Google Scholar] [CrossRef]
- Park, P. The Mediating Effect of Dementia Recognition on the Number of Chronic Diseases and Dementia Prevention Behaviors of Elders in Rural Communities. J. Korean Acad. Rural Health Nurs. 2020, 15, 41–48. [Google Scholar]
- Kim, K.-M.; Yang, Y.-O. The dementia knowledge, attitude and preventive behavior of the elderly lived in the urban-rural complex city. J. Korea Acad.-Ind. Coop. Soc. 2016, 17, 485–492. [Google Scholar]
- Park, K.-S.; Jeong, H.-Y.; So, S.-Y.; Park, Y.-H.; Yang, H.-J.; Jung, K.-R.; Moon, S.-J.; Kim, H.-K.; Cho, J.-H.; Yang, K.-H. The effects of the activity program for preventing dementia against depression, cognitive function, and quality of life for the elderly. J. Orient. Neuropsychiatry 2013, 24, 353–362. [Google Scholar] [CrossRef]
- Kim, H.; Lee, S. Changes in spatial dependence of crime and distribution of crime hot spots in Korea, 2001–2010. J. Resid. Environ. Inst. Korea 2013, 11, 27–41. [Google Scholar]
- Lim, H.; Park, Y. A study on the spatial pattern of regional safety in Korea. Korean J. Local Gov. Stud. 2017, 21, 385–407. [Google Scholar] [CrossRef]
- Lee, S. Understanding spatial dependence and using spatial regression analysis. Korean Policy Sci. Rev. 2014, 18, 39–79. [Google Scholar]
- Yang, B.-Y.; Hwang, C.-S. Spatial dependency and heterogeneity of adult diseases: In the cases of obesity, diabetes and high blood pressure in the USA. J. Korean Assoc. Reg. Geogr. 2010, 16, 610–622. [Google Scholar]
- Kim, Y.; Kang, S. A Study on the Geographic Variations in the Prevalence of Obesity using Geographically Weighted Regression. Geogr. J. Korea 2014, 48, 425–438. [Google Scholar]
- Park, I.-S.; Kim, E.-J.; Hong, S.-O.; Kang, S.-H. A study on factors related with regional occurrence of cardiac arrest using geographically weighted regression. Health Soc. Welf. Rev. 2013, 33, 237–257. [Google Scholar]
- Chen, J.-H.; Lin, K.-P.; Chen, Y.-C. Risk factors for dementia. J. Formos. Med. Assoc. 2009, 108, 754–764. [Google Scholar] [CrossRef]
- Kim, J. The relationships between perceived neighborhood characteristics and self-rated health or depression: The interaction effects with sociodemographic variables. Health Soc. Welf. Rev. 2018, 38, 290–315. [Google Scholar]
- Seeman, T.E.; Crimmins, E. Social environment effects on health and aging: Integrating epidemiologic and demographic approaches and perspectives. Ann. New York Acad. Sci. 2001, 954, 88–117. [Google Scholar] [CrossRef]
- Miller, H.J. Tobler’s first law and spatial analysis. Ann. Assoc. Am. Geogr. 2004, 94, 284–289. [Google Scholar] [CrossRef]
- Seok, H.; Kang, S. A study on the regional variation factor of hypertension prevalence. Health Soc. Welf. Rev. 2013, 33, 210–236. [Google Scholar]
- Kim, Y.; Cho, D.; Hong, S.; Kim, E.; Kang, S. Analysis on geographical variations of the prevalence of hypertension using multi-year data. J. Korean Geogr. Soc. 2014, 49, 935–948. [Google Scholar]
- Jo, E.-K.; Seo, E.-W.; Lee, K.-S. Spatial distribution of diabetes prevalence rates and its relationship with the regional characteristics. Health Policy Manag. 2016, 26, 30–38. [Google Scholar] [CrossRef]
- Suhn, M.O.; Kang, S.H.; Chun, J.-H. A Study on Variation and Application of Metabolic Syndrome Prevalence using Geographically Weighted Regression. J. Korea Acad.-Ind. Coop. Soc. 2018, 19, 561–574. [Google Scholar]
- Shin, Y.; Kim, D. A comparative study on the hotspot area in the Echelon analysis and spatial scan statistic using Korean cancer outbreak data. Korean Data Inf. Sci. Soc. 2018, 29, 975–985. [Google Scholar]
- Kim, S.H.; Han, S.-H. Prevalence of dementia among the South Korean population. J. Korean Diabetes 2012, 13, 124–128. [Google Scholar] [CrossRef]
- Kim, D.H. Epidemiology of dementia in Korea. J. Korean Med. Assoc. 2002, 45, 356–360. [Google Scholar] [CrossRef]
- Kim, K.W.; Park, J.H.; Kim, M.-H.; Kim, M.D.; Kim, B.-J.; Kim, S.-K.; Kim, J.L.; Moon, S.W.; Bae, J.N.; Woo, J.I. A nationwide survey on the prevalence of dementia and mild cognitive impairment in South Korea. J. Alzheimer’s Dis. 2011, 23, 281–291. [Google Scholar] [CrossRef]
- Ko, S.; Jung, Y.; Kim, D. The Social Burden and Care Management for People with Dementia. In Korean Institute for Health and Social Affairs Policy Report; KIHASA: Yeongi-gun, Korea, 2016. [Google Scholar]
- Barnes, D.E.; Yaffe, K. The projected effect of risk factor reduction on Alzheimer’s disease prevalence. Lancet Neurol. 2011, 10, 819–828. [Google Scholar] [CrossRef]
- Kim, D.-H.; Kang, J.; Yoo, S. A Literature Review on the Public Program of Walking Promotion for Active Living. J. Agric. Med. Community Health 2021, 46, 98–108. [Google Scholar]
- Yoon, T.H. Regional health inequalities in Korea: The status and policy tasks. J. Crit. Soc. Welf. 2010, 30, 49–77. [Google Scholar]
- Tesema, G.A.; Tessema, Z.T.; Angaw, D.A.; Tamirat, K.S.; Teshale, A.B. Geographic weighted regression analysis of hot spots of anemia and its associated factors among children aged 6–59 months in Ethiopia: A geographic weighted regression analysis and multilevel robust Poisson regression analysis. PLoS ONE 2021, 16, e0259147. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y. New approaches for calculating Moran’s index of spatial autocorrelation. PLoS ONE 2013, 8, e68336. [Google Scholar] [CrossRef] [PubMed]
- Tsai, P.-J.; Lin, M.-L.; Chu, C.-M.; Perng, C.-H. Spatial autocorrelation analysis of health care hotspots in Taiwan in 2006. BMC Public Health 2009, 9, 1–13. [Google Scholar] [CrossRef]
- Veldhuizen, E.M.; Osté, J.; Kunst, A.E. Environmental characteristics of hotspots of alcohol-related health incidents outside of the entertainment districts of Amsterdam. GeoJournal 2018, 83, 1053–1066. [Google Scholar] [CrossRef] [Green Version]
- Schneider, I.; William, H.; Stakleff, B.; Buser, L. Alcohol-Related Hot-Spot Analysis and Prediction; University of Minnesota, Center for Transportation Studies: Minneapolis, MN, USA, 2017. [Google Scholar]
- Hurzeler, T.; Buckley, N.A.; Noghrehchi, F.; Malouf, P.; Page, A.; Schumann, J.L.; Chitty, K.M. Alcohol-related suicide across Australia: A geospatial analysis. Aust. New Zealand J. Public Health 2021, 45, 394–399. [Google Scholar] [CrossRef]
- Idrovo, A.J. Three criteria for ecological fallacy. Environ. Health Perspect. 2011, 119, a332. [Google Scholar] [CrossRef]
- Lee, J. The regional health inequity, and individual and neighborhood level health determinants. Health Soc. Welf. 2016, 36, 345–384. [Google Scholar]


{kind=link}
{kind=link}
| Variables | Definition | Source (year) |
|---|---|---|
| Dementia prevalence | The proportion of the dementia population aged 65 and over among the population aged 65 and over (%) | Korea Central Dementia Center (2020) |
| Prevalence of mild cognitive impairment | The proportion of those with mild cognitive impairment aged 65 and over among the population aged 65 and over (%) | |
| Education level | The proportion of those with an education level below middle school education among the population aged 19 and over (%) | Community HealthSurvey (2020), KDCA 1 |
| Obesity prevalence | The proportion of the population with a body mass index of 25 and over (%) | |
| Hypertension prevalence | The proportion of the hypertension population aged 30 and over (diagnosed) (%) | |
| Diabetes prevalence | The proportion of the diabetes population aged 30 and over (diagnosed) (%) | |
| Depression prevalence | The proportion of the population with a total score of 10 or over on the Patient Health Questionnaire-9 (PHQ-9) (%) | |
| Current smoking | The proportion of the population who smoked more than five packs (100 cigarettes) in their lifetime, and who currently smoke (%) | |
| Moderate-to-high physical activity | The proportion of the population who engaged in high physical activity for at least 20 minutes a day, over 3 days in a recent week, or moderate physical activity, at least 30 minutes, over 5 days in a recent week (%) | |
| Stress recognition | The proportion of the population who feel ‘very stressful’ or ‘stressful’ in daily life (%) | |
| Walking practice | The proportion of the population who practiced walking at least 30 minutes a day, over 5 days in a recent week (%) | |
| High-risk drinking | The proportion of the population who drink alcohol more than twice a week; over seven glasses (or five cans of beer) for men, over five glasses (or three cans of beer) for women at once (%) | |
| Avoiding skipping breakfast | The proportion of the population who only had breakfast five or more times a week in the past year (%) | |
| Low-sodium diet preference | The proportion of the population who usually prefer a low-sodium diet (%) | Community Health Survey (2019) *, KDCA 1 |
| Variables | Min | Max | Average | SD 1 | EQ 2 | CV 3 |
|---|---|---|---|---|---|---|
| Dementia prevalence | 7.44 | 14.06 | 10.86 | 1.40 | 6.62 | 0.13 |
| Prevalence of mild cognitive impairment | 21.01 | 24.85 | 23.01 | 0.78 | 3.84 | 0.03 |
| Education level | 5.38 | 66.32 | 34.85 | 15.69 | 60.94 | 0.45 |
| Obesity prevalence | 20.10 | 43.50 | 31.34 | 3.45 | 23.40 | 0.11 |
| Hypertension prevalence | 14.10 | 26.80 | 19.33 | 2.31 | 12.70 | 0.12 |
| Diabetes prevalence | 4.30 | 13.30 | 8.33 | 1.41 | 9.00 | 0.17 |
| Depression prevalence | 0.00 | 6.40 | 2.66 | 1.34 | 6.40 | 0.51 |
| Current smoking | 10.10 | 29.30 | 19.66 | 3.13 | 19.20 | 0.16 |
| Moderate-to-high physical activity | 7.80 | 62.40 | 21.30 | 7.22 | 54.60 | 0.34 |
| Stress recognition | 6.20 | 36.10 | 25.72 | 4.86 | 29.90 | 0.19 |
| Walking practice | 14.20 | 82.00 | 37.91 | 10.92 | 67.80 | 0.29 |
| High-risk drinking | 6.50 | 29.20 | 15.75 | 3.97 | 22.70 | 0.25 |
| Avoiding skipping breakfast | 37.30 | 67.70 | 52.32 | 5.53 | 30.40 | 0.11 |
| Low-sodium diet preference | 23.50 | 62.40 | 41.41 | 6.04 | 38.90 | 0.15 |
| Variables | Regression Coefficient | |||
|---|---|---|---|---|
| Average | Median | Min | Max | |
| Education level (level below middle school education) | 0.069 | 0.068 | 0.057 | 0.086 |
| Hypertension prevalence | 0.023 | 0.024 | 0.003 | 0.041 |
| Walking practice | –0.018 | –0.017 | –0.022 | –0.002 |
| Low-sodium diet preference | –0.012 | –0.013 | –0.015 | 0.006 |
| Regional coefficient | 0.732 | 0.740 | 0.632 | 0.822 |
| R-square/Adj R-square | 0.743/0.727 | |||
| Variables | Hot Spot Region | Cold Spot Region | p | |||||
|---|---|---|---|---|---|---|---|---|
| N 1 | Average | SD 2 | N 1 | Average | SD 2 | |||
| Indicator value | Dementia prevalence | 69 | 12.264 | 1.117 | 88 | 9.623 | 0.739 | 0.000 |
| Education level | 69 | 49.955 | 12.011 | 88 | 22.177 | 7.999 | 0.000 | |
| Hypertension prevalence | 69 | 20.961 | 2.241 | 88 | 18.945 | 2.122 | 0.005 | |
| Walking practice | 69 | 31.981 | 9.711 | 88 | 44.780 | 8.583 | 0.000 | |
| Low-sodium diet preference | 69 | 39.106 | 7.294 | 88 | 42.258 | 4.321 | 0.002 | |
| Regression coefficient | Education level | 69 | 0.074 | 0.005 | 88 | 0.068 | 0.010 | 0.000 |
| Hypertension prevalence | 69 | 0.032 | 0.007 | 88 | 0.017 | 0.006 | 0.000 | |
| Walking practice | 69 | –0.019 | 0.001 | 88 | –0.016 | 0.002 | 0.000 | |
| Low-sodium diet preference | 69 | –0.014 | 0.001 | 88 | –0.008 | 0.005 | 0.000 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, J.; Park, J.-H. A Predictive Model of Regional Dementia Prevalence Using Geographic Weighted Regression Analysis. J. Pers. Med. 2022, 12, 1388. https://doi.org/10.3390/jpm12091388
Lim J, Park J-H. A Predictive Model of Regional Dementia Prevalence Using Geographic Weighted Regression Analysis. Journal of Personalized Medicine. 2022; 12(9):1388. https://doi.org/10.3390/jpm12091388
Chicago/Turabian StyleLim, Jihye, and Jong-Ho Park. 2022. "A Predictive Model of Regional Dementia Prevalence Using Geographic Weighted Regression Analysis" Journal of Personalized Medicine 12, no. 9: 1388. https://doi.org/10.3390/jpm12091388
APA StyleLim, J., & Park, J.-H. (2022). A Predictive Model of Regional Dementia Prevalence Using Geographic Weighted Regression Analysis. Journal of Personalized Medicine, 12(9), 1388. https://doi.org/10.3390/jpm12091388