
Non-Pharmacological Nursing Interventions to Prevent Delirium in ICU Patients—An Umbrella Review with Implications for Evidence-Based Practice

 ,
,  ,
,  ,
, 
Abstract
:1. Background
1.1. Aim
1.2. What Is Already Known about the Topic?
- Delirium is a common complication of hospitalization among ICU patients.
- It has an impact on treatment outcomes, increases mortality, and prolongs hospitalization and cognitive impairment.
- Delirium still remains undiagnosed among ICU patients.
- Patient assessment for delirium is still not common practice in all countries.
1.3. What This Paper Adds?
- Non-pharmacological nursing interventions can be effective in preventing and reducing the duration of delirium in ICU patients.
- Multi-component interventions have the highest efficacy.
- The family is an important part of the prevention of delirium.
- Light therapy can improve the patient’s circadian rhythm.
- Improving sleep quality may reduce the incidence of delirium.
- Medical staff should be aware of and implement the practice of delirium assessment in patients in intensive care units.
2. Methods
2.1. Review Questions
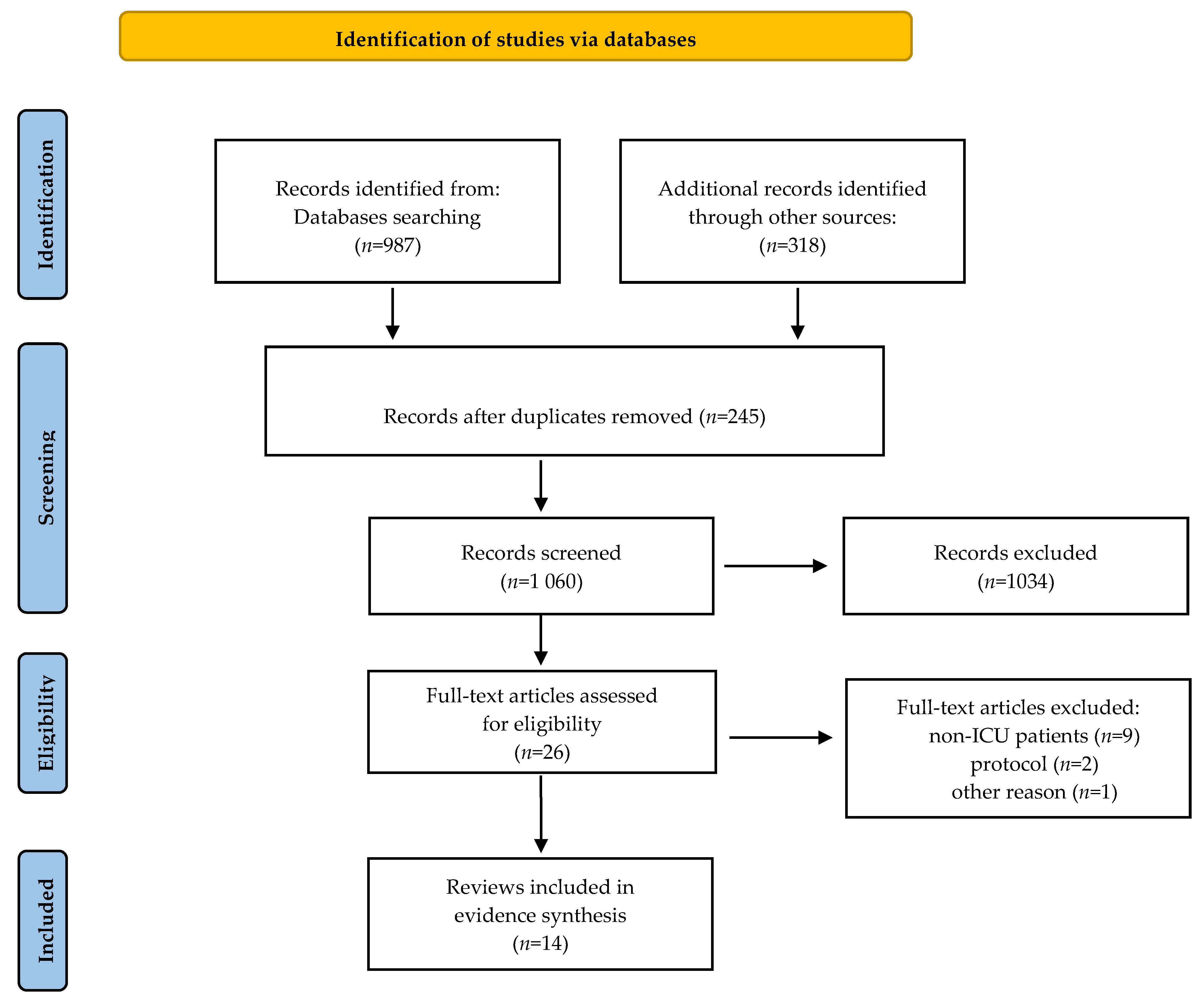
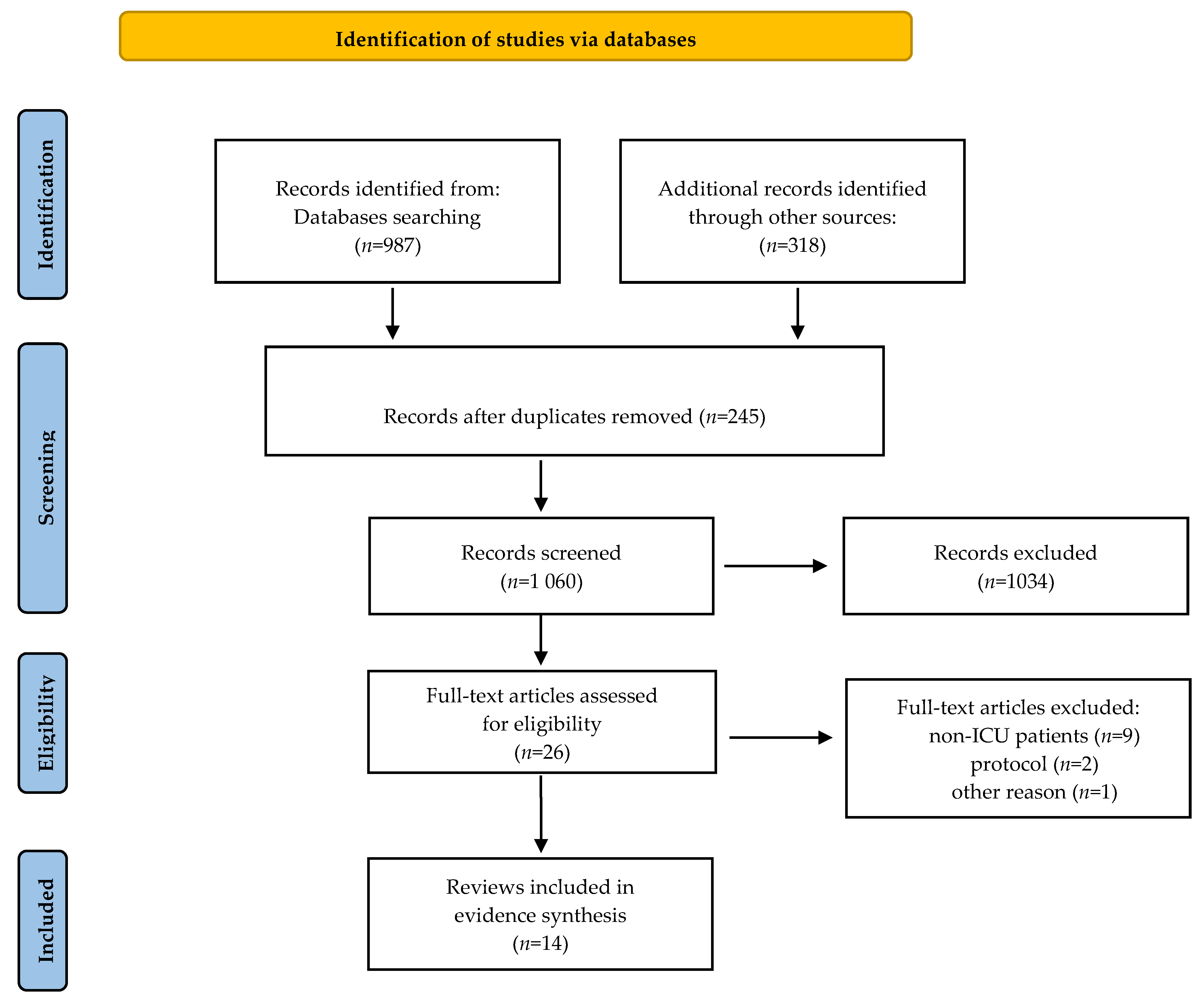
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
2.4. Data Collection
2.5. Quality Assessment
3. Results
3.1. Main Findings and Conclusions of the Reviews
3.2. Effects of Non-Pharmacological Nursing Interventions
3.3. Multi-Component Non-Pharmacological Interventions
3.4. Early Mobilization
3.5. Family Participation
3.6. Environmental Interventions
4. Discussion
5. Conclusions
6. Implications for Practice
7. Implications for Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hshieh, T.T.; Inouye, S.K.; Oh, E.S. Delirium in the Elderly. Psychiatr. Clin. N. Am. 2018, 41, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Volland, J.; Fisher, A.; Drexler, D. Preventing and identifying hospital-acquired delirium. Nursing 2020, 50, 32–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, J.E.; Mart, M.F.; Cunningham, C.; Shehabi, Y.; Girard, T.D.; MacLullich, A.M.J.; Slooter, A.J.C.; Ely, E.W. Delirium. Nat. Rev. Dis. Prim. 2020, 6, 90. [Google Scholar] [CrossRef] [PubMed]
- Kotfis, K.; Marra, A.; Ely, E.W. ICU delirium—A diagnostic and therapeutic challenge in the intensive care unit. Anaesthesiol. Intensiv. Ther. 2018, 50, 128–140. [Google Scholar] [CrossRef] [Green Version]
- Ely, E.W.; Shintani, A.; Truman, B.; Speroff, T.; Gordon, S.M.; Harrell, F.E.; Inouye, S.K.; Bernard, G.R.; Dittus, R.S. Delirium as a Predictor of Mortality in Mechanically Ventilated Patients in the Intensive Care Unit. J. Am. Med. Assoc. 2004, 291, 1753–1762. [Google Scholar] [CrossRef] [Green Version]
- Hayhurst, C.J.; Pandharipande, P.P.; Hughes, C.G. Intensive Care Unit Delirium: A Review of Diagnosis, Prevention, and Treatment. Anesthesiology 2016, 125, 1229–1241. [Google Scholar] [CrossRef] [Green Version]
- Inouye, S.K.; Bogardus, S.T.; Baker, D.I.; Leo-Summers, L.; Cooney, L.M. The hospital elder life program: A model of care to prevent cognitive and functional decline in older hospitalized patients. J. Am. Geriatr. Soc. 2000, 48, 1697–1706. [Google Scholar] [CrossRef]
- Tran, N.N.; Hoang, T.P.N.; Ho, T.K.T. Diagnosis and risk factors for delirium in elderly patients in the emergency rooms and intensive care unit of the national geriatric hospital emergency department: A cross-sectional observational study. Int. J. Gen. Med. 2021, 14, 6505–6515. [Google Scholar] [CrossRef]
- Ozga, D.; Krupa, S.; Witt, P.; Mędrzycka-Dabrowska, W. Nursing interventions to prevent delirium in critically ill patients in the intensive care unit during the covid19 pandemic—narrative overview. Healthcare 2020, 8, 578. [Google Scholar] [CrossRef]
- McKenzie, J.; Joy, A. Family intervention improves outcomes for patients with delirium: Systematic review and meta-analysis. Australas. J. Ageing 2020, 39, 21–30. [Google Scholar] [CrossRef]
- Hipp, D.M.; Ely, E.W. Pharmacological and Nonpharmacological Management of Delirium in Critically Ill Patients. Neurotherapeutics 2012, 9, 158–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pun, B.T.; Ely, E.W. The importance of diagnosing and managing ICU delirium. Chest 2007, 132, 624–636. [Google Scholar] [CrossRef] [PubMed]
- Krupa, S.; Ozga, D. Review of the Literature on the Occurrence of Delirium after Veno-Venous and Veno-Arterial Extracorporeal Membrane Oxygenation: A Systematic Review. Dement. Geriatr. Cogn. Dis. Extra 2019, 9, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Cascella, M.; Fiore, M.; Leone, S.; Carbone, D.; Di Napoli, R. Current controversies and future perspectives on treatment of intensive care unit delirium in adults. World J. Crit. Care Med. 2019, 8, 18–27. [Google Scholar] [CrossRef]
- Devlin, J.W.; Skrobik, Y.; Gélinas, C.; Needham, D.M.; Slooter, A.J.C.; Pandharipande, P.P.; Watson, P.L.; Weinhouse, G.L.; Nunnally, M.E.; Rochwerg, B.; et al. Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU. Crit. Care Med. 2018, 46, e825–e873. [Google Scholar] [CrossRef] [Green Version]
- Blodgett, T.J.; Blodgett, N.P. Melatonin and melatonin-receptor agonists to prevent delirium in hospitalized older adults: An umbrella review. Geriatr. Nurs. 2021, 42, 1562–1568. [Google Scholar] [CrossRef]
- Khaing, K.; Nair, B.R. Melatonin for delirium prevention in hospitalized patients: A systematic review and meta-analysis. J. Psychiatr. Res. 2021, 133, 181–190. [Google Scholar] [CrossRef]
- Ng, K.T.; Teoh, W.Y.; Khor, A.J. The effect of melatonin on delirium in hospitalised patients: A systematic review and meta-analyses with trial sequential analysis. J. Clin. Anesth. 2020, 59, 74–81. [Google Scholar] [CrossRef]
- Osiezagha, K.; Ali, S.; Freeman, C.; Barker, N.C.; Jabeen, S.; Maitra, S.; Olagbemiro, Y.; Richie, W.; Bailey, T.K. Thiamine deficiency and delirium. Innov. Clin. Neurosci. 2013, 10, 26–32. [Google Scholar]
- McKenzie, C.A.; Page, V.J.; Strain, W.D.; Blackwood, B.; Ostermann, M.; Taylor, D.; Peter, E.; Spronk, P.E.; McAuley, D.F. Parenteral thiamine for prevention and treatment of delirium in critically ill adults: A systematic review protocol. Syst. Rev. 2020, 9, 131. [Google Scholar] [CrossRef]
- Sedhai, Y.R.; Shrestha, D.B.; Budhathoki, P.; Jha, V.; Mandal, S.K.; Karki, S.; Baniya, R.; Cable, C.A.; Kashiouris, M.G. Effect of thiamine supplementation in critically ill patients: A systematic review and meta-analysis. J. Crit. Care 2021, 65, 104–115. [Google Scholar] [CrossRef] [PubMed]
- Lange, S.; Mędrzycka-Dąbrowska, W.; Friganovic, A.; Oomen, B.; Krupa, S. Delirium in critical illness patients and the potential role of thiamine therapy in prevention and treatment: Findings from a scoping review with implications for evidence-based practice. Int. J. Environ. Res. Public Health 2021, 18, 8809. [Google Scholar] [CrossRef] [PubMed]
- Martinez, F.; Tobar, C.; Hill, N. Preventing delirium: Should non-pharmacological, multicomponent interventions be used? A systematic review and meta-analysis of the literature. Age Ageing 2015, 44, 196–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burton, J.K.; E Craig, L.; Yong, S.Q.; Siddiqi, N.; A Teale, E.; Woodhouse, R.; Barugh, A.J.; Shepherd, A.M.; Brunton, A.; Freeman, S.C.; et al. Non-pharmacological interventions for preventing delirium in hospitalised non-ICU patients. Cochrane Database Syst. Rev. 2021, 2021, CD013307. [Google Scholar] [CrossRef] [Green Version]
- Rivosecchi, R.M.; Smithburger, P.L.; Svec, S.; Campbell, S.; Kane-Gill, S.L. Nonpharmacological interventions to prevent delirium: An evidence-based systematic review. Crit. Care Nurse 2015, 35, 39–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papatheodorou, S.I.; Evangelou, E. Umbrella Reviews: What They Are and Why We Need Them. Methods Mol. Biol. 2022, 2345, 135–146. [Google Scholar] [CrossRef]
- Papatheodorou, S.I. Umbrella reviews: What they are and why we need them. Eur. J. Epidemiol. 2019, 34, 543–546. [Google Scholar] [CrossRef]
- Aromataris, E.; Fernandez, R.; Godfrey, C.; Holly, C.; Khalil, H.; Tungpunkom, P. The Joanna Briggs Institute Reviewers’ Manual 2014 Methodology for JBI Umbrella Reviews; The Joanna Briggs Institute: Adelaide, Australia, 2014. [Google Scholar]
- Zhang, H.; Lu, Y.; Liu, M.; Zou, Z.; Wang, L.; Xu, F.-Y.; Shi, X.-Y. Strategies for prevention of postoperative delirium: A systematic review and meta-analysis of randomized trials. Crit. Care 2013, 17, R47. [Google Scholar] [CrossRef] [Green Version]
- Litton, E.; Carnegie, V.; Elliott, R.; Webb, S.A.R. The Efficacy of Earplugs as a Sleep Hygiene Strategy for Reducing Delirium in the ICU: A Systematic Review and Meta-Analysis. Crit. Care Med. 2016, 44, 992–999. [Google Scholar] [CrossRef]
- Bannon, L.; McGaughey, J.; Verghis, R.; Clarke, M.; McAuley, D.F.; Blackwood, B. The effectiveness of non-pharmacological interventions in reducing the incidence and duration of delirium in critically ill patients: A systematic review and meta-analysis. Intensiv. Care Med. 2019, 45, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luther, R.; McLeod, A. The effect of chronotherapy on delirium in critical care—A systematic review. Nurs. Crit. Care 2018, 23, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Locihová, H.; Axmann, K.; Padyšáková, H.; Fejfar, J. Effect of the use of earplugs and eye mask on the quality of sleep in intensive care patients: A systematic review. J. Sleep Res. 2018, 27, e12607. [Google Scholar] [CrossRef] [PubMed]
- Nassar, A.P.; Besen, B.A.M.P.; Robinson, C.C.; Falavigna, M.; Teixeira, C.; Rosa, R.G. Flexible versus restrictive visiting policies in ICUs: A systematic review and meta-analysis. Crit. Care Med. 2018, 46, 1175–1180. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.; Lee, M.; Ko, H.; Kim, S.; Yun, S.; Jeong, Y.; Ch, Y. Effect of nonpharmacological interventions for the prevention of delirium in the intensive care unit: A systematic review and meta-analysis. J. Crit. Care 2018, 48, 372–384. [Google Scholar] [CrossRef] [PubMed]
- Herling, S.F.; Greve, I.E.; Vasilevskis, E.E.; Egerod, I.; Mortensen, C.B.; Møller, A.M.; Svenningsen, H.; Thomsen, T. Interventions for preventing intensive care unit delirium in adults. Cochrane Database Syst. Rev. 2018, 11, CD009783. [Google Scholar] [CrossRef]
- Janssen, T.L.; Alberts, A.R.; Hooft, L.; Mattace-Raso, F.U.S.; Mosk, C.A.; Van Der Laan, L. Prevention of postoperative delirium in elderly patients planned for elective surgery: Systematic review and meta-analysis. Clin. Interv. Aging 2019, 14, 1095–1117. [Google Scholar] [CrossRef] [Green Version]
- Deng, L.-X.; Cao, L.; Zhang, L.-N.; Peng, X.-B.; Zhang, L. Non-pharmacological interventions to reduce the incidence and duration of delirium in critically ill patients: A systematic review and network meta-analysis. J. Crit. Care 2020, 60, 241–248. [Google Scholar] [CrossRef]
- León-Salas, B.; Trujillo-Martín, M.M.; Del Castillo, L.P.M.; García-García, J.; Pérez-Ros, P.; Rivas-Ruiz, F.; Serrano-Aguilar, P. Multicomponent Interventions for the Prevention of Delirium in Hospitalized Older People: A Meta-Analysis. J. Am. Geriatr. Soc. 2020, 68, 2947–2954. [Google Scholar] [CrossRef]
- Ludolph, P.; Msc, J.S.; Kunzler, A.M.; Rösch, R.; Geschke, K.; Vahl, C.F.; Lieb, K. Non-Pharmacologic Multicomponent Interventions Preventing Delirium in Hospitalized People. J. Am. Geriatr. Soc. 2020, 68, 1864–1871. [Google Scholar] [CrossRef]
- Liang, S.; Chau, J.P.C.; Lo, S.H.S.; Zhao, J.; Choi, K.C. Effects of nonpharmacological delirium-prevention interventions on critically ill patients’ clinical, psychological, and family outcomes: A systematic review and meta-analysis. Aust. Crit. Care 2021, 34, 378–387. [Google Scholar] [CrossRef]
- Ekeozor, C.U.; Jeyaruban, D.; Lasserson, D. Where should patients with or at risk of delirium be treated in an acute care system? Comparing the rates of delirium in patients receiving usual care vs alternative care: A systematic review and meta-analysis. Int. J. Clin. Pract. 2021, 75, e13859. [Google Scholar] [CrossRef]
- de Foubert, M.; Cummins, H.; McCullagh, R.; Brueton, V.; Naughton, C. Systematic review of interventions targeting fundamental care to reduce hospital-associated decline in older patients. J. Adv. Nurs. 2021, 77, 4661–4678. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Lee, J.; Kim, J.; Jung, Y. Non-pharmacological nursing interventions for prevention and treatment of delirium in hospitalized adult patients: Systematic review of randomized controlled trials. Int. J. Environ. Res. Public Health 2021, 18, 8853. [Google Scholar] [CrossRef] [PubMed]
- Burry, L.D.; Cheng, W.; Williamson, D.R.; Adhikari, N.K.; Egerod, I.; Kanji, S.; Martin, C.M.; Hutton, B.; Rose, L. Pharmacological and non-pharmacological interventions to prevent delirium in critically ill patients: A systematic review and network meta-analysis. Intensiv. Care Med. 2021, 47, 943–9460. [Google Scholar] [CrossRef]
- Saritas, S.; Tarlaci, S. A Systematic Review of Non-Pharmacological Interventions to Prevent Delirium at Intensive Care Units. Psychiatry Behav. Sci. 2021, 11, 141–147. [Google Scholar] [CrossRef]
- Qin, M.; Gao, Y.; Guo, S.; Lu, X.; Zhu, H.; Li, Y. Family intervention for delirium for patients in the intensive care unit: A systematic meta-analysis. J. Clin. Neurosci. 2022, 96, 114–119. [Google Scholar] [CrossRef]
- Chen, T.J.; Traynor, V.; Wang, A.Y.; Shih, C.Y.; Tu, M.C.; Chuang, C.H.; Chiu, H.-Y.; Chang, H.-C. Comparative Effectiveness of Non-Pharmacological Interventions for Preventing Delirium in Critically Ill Adults: A Systematic Review and Network Meta-Analysis. Int. J. Nurs. Stud. 2022, 131, 104239. [Google Scholar] [CrossRef]
- Liu, J.; Wang, J. Efficacy of EWINDOW for prevention of delirium at intensive care units: A protocol for systematic review and meta-analysis. Medicine 2022, 101, e28598. [Google Scholar] [CrossRef]
- Bohart, S.; Møller, A.M.; Andreasen, A.S.; Waldau, T.; Lamprecht, C.; Thomsen., T. Effect of Patient and Family Centred Care interventions for adult intensive care unit patients and their families: A systematic review and meta-analysis. Intensiv. Crit. Care Nurs. 2022, 69, 103156. [Google Scholar] [CrossRef]
- Xu, C.; Chen, Z.; Zhang, L.; Guo, H. Systematic review and meta-analysis on the incidence of delirium in intensive care unit inpatients after cognitive exercise intervention. Ann. Palliat. Med. 2022, 11, 663–672. [Google Scholar] [CrossRef]
- Aromataris, E.; Munn, Z. JBI Manual for Evidence Synthesis; The Joanna Briggs Institute: Adelaide, Australia, 2020. [Google Scholar] [CrossRef]
- Pezzullo, L.; Streatfeild, J.; Hickson, J.; Teodorczuk, A.; Agar, M.R.; Caplan, G.A. Economic impact of delirium in Australia: A cost of illness study. BMJ Open 2019, 9, e027514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavallazzi, R.; Saad, M.; Marik, P.E. Delirium in the ICU: An overview. Ann. Intensiv. Care 2012, 2, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckstein, C.; Burkhardt, H. Multicomponent, nonpharmacological delirium interventions for older inpatients: A scoping review. Z. Gerontol. Geriatr. 2019, 52, 229–242. [Google Scholar] [CrossRef] [Green Version]
- Sahawneh, F.; Boss, L. Non-pharmacologic interventions for the prevention of delirium in the intensive care unit: An integrative review. Nurs. Crit. Care 2021, 26, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Wright, S.E.; Thomas, K.; Watson, G.; Baker, C.; Bryant, A.; Chadwick, T.J.; Jing Shen, J.; Wood, R.; Wilkinson, J.; Mansfield, L.; et al. Intensive versus standard physical rehabilitation therapy in the critically ill (EPICC): A multicentre, parallel-group, randomised controlled trial. Thorax 2018, 73, 213–221. [Google Scholar] [CrossRef] [Green Version]
- Doiron, K.; Hoffmann, T.; Beller, E. Early intervention (mobilization or active exercise) for critically ill adults in the intensive care unit (Review). Cochrane Database Syst. Rev. 2018. [Google Scholar] [CrossRef] [Green Version]
- Schweickert, W.D.; Pohlman, M.C.; Pohlman, A.S.; Nigos, C.; Pawlik, A.J.; Esbrook, C.L.; Spears, L.; Miller, M.; Franczyk, M.; Deprizio, D.; et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: A randomised controlled trial. Lancet 2009, 373, 1874–1882. [Google Scholar] [CrossRef]
- Morris, P.E.; Berry, M.J.; Files, D.C.; Thompson, J.C.; Hauser, J.; Flores, L.; Dhar, S.; Chmelo, E.; Lovato, J.; Case, L.D. Standardized rehabilitation and hospital length of stay among patients with acute respiratory failure a randomized clinical trial. JAMA—J. Am. Med. Assoc. 2016, 315, 2694–2702. [Google Scholar] [CrossRef]
- Engwall, M.; Fridh, I.; Johansson, L.; Bergbom, I.; Lindahl, B. Lighting, sleep and circadian rhythm: An intervention study in the intensive care unit. Intensiv. Crit. Care Nurs. 2015, 31, 325–335. [Google Scholar] [CrossRef] [Green Version]
- Guo, Y.; Sun, L.; Li, L.; Jia, P.; Zhang, J.; Jiang, H.; Jiang, W. Impact of multicomponent, nonpharmacologic interventions on perioperative cortisol and melatonin levels and postoperative delirium in elderly oral cancer patients. Arch. Gerontol. Geriatr. 2016, 62, 112–117. [Google Scholar] [CrossRef]
- Ono, H.; Taguchi, T.; Kido, Y.; Fujino, Y.; Doki, Y. The usefulness of bright light therapy for patients after oesophagectomy. Intensiv. Crit. Care Nurs. 2011, 27, 158–166. [Google Scholar] [CrossRef] [PubMed]
- Kleinpell, R.; Zimmerman, J.; Vermoch, K.L.; Harmon, L.A.; Vondracek, H.; Hamilton, R.; Hanson, B.; Hwang, D.Y. Promoting Family Engagement in the ICU: Experience from a National Collaborative of 63 ICUs. Crit. Care Med. 2019, 47, 1692–1698. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Pabón-Martínez, B.A.; Rodríguez-Pulido, L.I.; Henao-Castaño, A.M. The family in preventing delirium in the intensive care unit: Scoping review. Enferm. Intensiva 2022, 33, 33–43. [Google Scholar] [CrossRef]
- Ely, E.W. The ABCDEF bundle: Science and philosophy of how ICU liberation serves patients and families. Crit. Care Med. 2017, 45, 321–330. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| PICO | Inclusion Criteria | Exclusion Criteria | Keywords | Search Strategies |
|---|---|---|---|---|
| Patients | Adults (>18 years), ICU patients | Adults patients of other units, children, ICU children | ICU, critical care, critical illnesses | ICU OR critical care OR critical illnesses |
| Interventions | Non-pharmacological interventions | Pharmacological interventions, mixed interventions, interventions only focusing on screening delirium | Non-pharmacological interventions, multicomponent interventions, earplugs, noise reduction, eye masks, lighting control, education, orientation, cognitive therapy, bright light therapy, music therapy, physical therapy, early mobilization, exercise | Non-pharmacological interventions OR multicomponent interventions OR earplugs OR noise reduction OR eye masks OR lighting control OR education OR orientation OR cognitive therapy OR bright light therapy OR music therapy OR physical therapy OR early mobilization OR exercise |
| Comparison | Usual care, any comparator or including no comparator | n/a | Delirium, delirium prevention | Delirium OR delirium prevention |
| Outcomes | Delirium-related data (e.g., reducing the incidence of delirium, shortening the duration of delirium) | n/a | n/a | n/a |
| Study design | Systematic review | Other types of reviews | Systematic review | Systematic review |
| Author (First) | Type of Review | Methodology/Search Strategy | Number of Studies Included | In-Or Excluded (Comment) |
|---|---|---|---|---|
| Zhang, H. [29] | A systematic review and meta-analysis | Literature searches: MEDLINE, EMBASE, CINAHL, Cochrane Library, reference lists, “Google Scholar”. Type of studies: RCTs. Time: before August 2012 | 38 | Excluded—No ICU patients |
| Rivosecch, R.M. [25] | An evidence-based systematic review | Literature searches: MEDLINE and EMBASE. Type of studies: RCTs, prospective RCTs, CCTs. Time: from 1946 to 15 October 2013 | 17 | Excluded—Not only ICU patients |
| Litton, E. [30] | A systematic review and meta-analysis | Literature searches: MEDLINE, EMBASE, the Cochrane Central Register of controlled trials. Type of studies: Interventional studies. Time: period between 1966 and May 2015 | 9 | Included |
| Bannon, L. [31] | A systematic review of quantitative and qualitative research | Literature searches: MEDLINE, EMBASE, CINAHL, Web of Science, AMED, PsycINFO, Cochrane Library. Type of studies: RCTs, CCTs. Time: n/d | n/d | Excluded—Protocol |
| Martinez, F. [23] | A systematic review and meta-analysis | Literature searches: PubMed/MEDLINE, EMBASE, PsycINFO, CINAHL, Cochrane Library, CENTRAL, LILACS, SciELO, grey literature Type of studies: Randomized trials. Time: from inception to 31 December 2012. | 7 | Excluded—No ICU patients |
| Luther, R. [32] | A systematic review of quantitative studies | Literature searches: Academic Search Complete, CINAHL Plus with Full Text, E-Journals, MEDLINE Complete, PsycARTICLES, PsycINFO. Type of studies: RCTs, and a cohort-based design. Time: 2006–2016 | 6 | Included—Without melatonin study |
| Locihová, H. [33] | A systematic review | Literature searches: CINAHL, PubMed, SCOPUS. Type of studies: RCTs, CCTs. Time: 1990–2015 | 19 | Included |
| Nassar Junior, A.P. [34] | A systematic review and meta-analysis | Literature searches: Medline, Scopus, Web of Science. Type of studies: Observational and randomized studies. Time: | 16 | Included |
| Kang, J. [35] | A systematic review and meta-analysis | Literature searches: MEDLINE, Cochrane Library, CINAHL, PsycINFO, EMBASE. Type of studies: cohort studies, RCTs, CBA, and CCT Time: between 2007 and 2016. | 35 | Included |
| Herling, S.F. [36] | Review | Literature searches: ENTRAL, MEDLINE, Embase, BIOSIS, International Web of Science, Latin American Caribbean Health Sciences Literature, CINAHL. Type of studies: RCTs. Time: from 1980 to 11 April 2018 | 12 (4 non-pharmacological interventions) | Included—Only non-pharmacological interventions analyzed |
| Bannon, L. [31] | A systematic review and meta-analysis | Literature searches: MEDLINE, EMBASE, CINAHL, Web of Science, PsycINFO, AMED, Cochrane Library. Type of studies: RCTs. Time: up to March 2018 | 15 | Included |
| Janssen, T.L. [37] | A systematic review and meta-analysis | Literature searches: PubMed (Medline OvidSP), Embase, Cochrane Centre, Web of Science. Type of studies: RCTs, CBA. Time: in March 2018 | 35 | Excluded—No ICU patients |
| Deng, L. [38] | A systematic review and network meta-analysis | Literature searches: PubMed, Embase, CINAHL, Cochrane Library. Type of studies: RCTs and cohort studies. Time: the end of June 2019 | 26 | Included |
| León-Salas, B. [39] | A systematic review with meta-analysis | Literature searches: MEDLINE, EMBASE, Web of Science, Cochrane Central Register of Controlled Trials. Type of studies: RCTs. Time: 2015 to March 2019. | 49 | Excluded—Not only ICU patients |
| Ludolph, P. [40] | A systematic review | Literature searches: PubMed and CENTRAL. Type of studies: RCTs and cluster RCTs. Time: without any time constraints | 8 | Excluded—Not only ICU patients |
| Liang, S. [41] | A systematic review and meta-analysis | Literature searches: MEDLINE, CINAHL, EMBASE, Cochrane CENTRAL, Web of Science, PsycINFO, Chinese electronic databases. Type of studies: RCTs, CCTs, CBA. Time: until September 2020 | 34 | Included |
| Ekeozor, C.U. [42] | A systematic review and meta-analysis | Literature searches: MEDLINE, EMBASE, PsycINFO, OpenGrey, Web of Science, reference lists of journals. Type of studies: RCTs, observational studies, and non-randomized CTs. Time: from inception to 12 February 2020 | 59 | Excluded—No ICU patients |
| de Foubert, M. [43] | A systematic review | Literature searches: CINAHL, MEDLINE, EMBASE, Cochrane Library, Google Scholar, BMJ quality reports. Type of studies: randomized and quasi-experimental designs. Time: from January 2009 to February 2020. | 18 | Excluded—No ICU patients |
| Lee, Y. [44] | A systematic review of randomized controlled trials | Literature searches: PubMed, CINAHL, Embase, Cochrane Central Register of Randomized Controlled Trials. Type of studies: prospective RCTs. Time: up to 27 January 2021 | 9 | Excluded—Not only ICU patients |
| Burry, L.D. [45] | A systematic review and network meta-analysis | Literature searches: MEDLINE, Embase, PsycINFO, CINAHL, Web of Science, Cochrane Library, Prospero, WHO international clinical trial. Type of studies: RCTs. Time: from inception to 8 April 2021 | 80 (25 studies of non-pharmacological interventions) | Included—Only non-pharmacological interventions analyzed |
| Saritas, S. [46] | A systematic review | Literature searches: Cochrane, CINAHL, PsycINFO, PubMed, EMBA Type of studies: Quasi-experimental, experimental, RCTs. Time: October 2013 and March 2020 | 13 | Included—Without melatonin study |
| Qin, M. [47] | A systematic review and meta-analysis | Literature searches: PubMed, Embase, MEDLINE, Cochrane Library. Type of studies: RCTs, CBA, and cohort trials. Time: up to September 2021 | 6 | Included |
| Chen, T-J. [48] | A systematic review and network meta-analysis. | Literature searches: PubMed, EMBASE, CINAHL, Cochrane CENTRAL, ProQuest Dissertations and Theses A&I. Type of studies: RCTs. Time: from the inception to December 2021 | 29 | Included |
| Liu, J. [49] | A systematic review and meta-analysis | Literature searches: China National Knowledge Infrastructure Database, Excerpta Medica database, PubMed, Cochrane Central Register of Controlled Trials, Wan Fang, Cumulative Index of Nursing and Allied Health Literature. Type of studies: RCTs. Time: from January 2012 to December 2021. | n/d | Excluded—Protocol |
| Bohart, S. [50] | A systematic review and meta-analysis | Literature searches: MEDLINE, EMBASE, Cochrane Central Register of Controlled Trials, CINAHL, PsycINFO, and Web of Science, hand searched the reference lists of relevant reviews and original trials and searched for unpublished and ongoing studies, and grey literature in Opengrey.eu, and ClinicalTrial.gov. Type of studies: RCTs. Time: n/d | 9 | Excluded—None of the included studies assessed the number of coma- and delirium-free days in ICU. |
| Xu, H. [51] | Systematic review and meta-analysis | Literature searches: PubMed, MEDLINE, Cochrane Library, Chinese National Knowledge Infrastructure (CNKI), China Biology Medicine Disc (CBMD), Wanfang Database, and Western Biomedical Journal Database. Type of studies: RCTs. Time: from the establishment to 28 June 2021 | 7 | Included |
| Study | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Litton, E. [29] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | n/a |
| Bannon, L. [31] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Luther, R. [32] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Locihová, H. [33] | Y | Y | Y | Y | U | U | U | Y | Y | Y | Y |
| Nassar, A.P. [34] | U | Y | Y | Y | Y | Y | Y | Y | Y | Y | n/a |
| Kang, J. [35] | Y | Y | Y | Y | Y | Y | Y | Y | Y | n/a | n/a |
| Herling, S.F. [36] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Deng, L.XX [38] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Liang, S. [41] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Burry, L.D. [45] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | n/a |
| Saritas, S. [46] | Y | Y | Y | Y | Y | U | Y | n/a | N | n/a | n/a |
| Qin, M. [47] | Y | Y | Y | Y | Y | Y | Y | Y | Y | n/a | n/a |
| Chen, T.J. [48] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | n/a |
| Xu, C. [51] | U | Y | Y | Y | Y | Y | Y | Y | Y | n/a | Y |
| Author (First) | Aim | Participants | Interventions | Results | Findings |
|---|---|---|---|---|---|
| Litton, E. [30] | To assess the efficacy of earplugs as an ICU strategy for reducing delirium | Adult patients admitted to a critical care environment. | Earplugs—as an isolated intervention (3 studies). Earplugs—as a part of a bundle with eye shades alone (2 studies) or earplugs, eye shades, and additional sleep noise abatement strategies (4 studies). | Earplug placement = RR of 0.59 (95% CI, 0.44–0.78). Hospital mortality: earplug placement was associated with an RR of 0.77 (95% CI, 0.54–1.11). | Earplugs in patients admitted to the ICU, either isolation or as part of a bundle of sleep hygiene improvement, is associated with a significant reduction in risk of delirium. |
| Luther, R. [32] | To understand whether implementation of chronotherapy within the critical care setting can reduce the prevalence of delirium | Adult patients (18+ years). Critical care settings. | DLA—Controlled dynamic light application; BLT—Bright light therapy; MINI 1—Multi-component non-pharmacological interventions: reduction of lighting and noise; MINI 2—frequent patient orientation, use of music, ear plugs/eye shades, reduction in noise, and use of natural light/dimmed lighting in evening. | DLA: Delirium occurred in 137 of 361 (38%) vs. 123 of 373 (33%) control. BLT: Reductions in delirium occurrence in the groups receiving BLT (collectively 2/16 BLT versus 10/17 control). MINI: Delirium occurred 55 of 167 (33%) pre-intervention (MINI 1) vs. 24 of 171 (14%) post-intervention (p < 0.001). Duration of delirium reduced from 3–4 days pre vs. 1–2 days post (p = 0.021). Mean sleep efficiency index and increased sleep quality increased. Patients with high sleep efficiency index scores demonstrated significantly reduced risk of delirium. MINI2: Delirium occurred in 10 of 81 (12%) vs. 25 of 79 (31.25%) control (p < 0.006). Duration of delirium was also significantly reduced. | Chronotherapy can reduce the incidence of delirium within critical care. |
| Locihová, H. [33] | To comment on the effectiveness of selected non-pharmacological interventions and to provide a basis for discussion of whether these measures may have an impact upon the improvement of the short-term (reduction of delirium, shortening of hospitalization time) and long-term outcomes. | Patients in ICUs. | Plugs; Eye mask; Plugs and eye mask; Plugs, mask, and music | Earplugs: Cox regression analysis revealed a reduction in the risk of early development of delirium and confusion by 53%. Earplugs + eye mask + relaxing music: confirmed a statistically significant reduction in the delirium incidence of the investigated interventions: pre-phase: (22%), cf. post-phase (49%; OR: 0.46, 95% CI: 0.23–0.89, p = 0.02) and confirmed a statistically significant difference in the occurrence of the daily delirium-free status in patients in the pre-phase (43%) cf. post-phase (48%; OR: 1.64, 95% CI: 1.04–2.58, p = 0.03). Earplugs + eye mask: confirmed a statistically significant reduction in the incidence of postoperative disorientation in the intervention group (control group 14%, cf. intervention group 0%, p = 0.01). | The examined interventions reduce the incidence of delirium significantly. |
| Nassar Junior, A.P. [34] | To synthesize data on outcomes related to patients, family members, and ICU professionals by comparing flexible vs. restrictive visiting policies in ICUs. | ICU-patients, family members, ICU-professionals. | Flexible visiting policies. | Two studies evaluated the frequency of delirium (354 patients). The flexible visiting policy was associated with a reduced frequency of delirium (OR, 0.39; 95% CI, 0.22–0.69; I2 = 0%). | Flexible ICU visiting hours have the potential to reduce delirium. |
| Kang, J. [35] | To examine the effect of nonpharmacological interventions that are used in the prevention of ICU delirium. | Adult patients (>18 years) admitted to an ICU of various types (ICU, MICU, SICU in five studies (14.3%), MICU and SICU in cardiac ICU, traumatic, and cardiac care unit). | MLT—multicomponent interventions; PEI—physical environment interventions; DIS—daily interruption of sedation, exercise; PE—patient education; AWS—automatic warning system; CHI—cerebral hemodynamics improvement; FP—family participation; SR—sedation reduction. | The effect sizes of non-pharmacological interventions for onset of delirium and duration of delirium were statistically significant. The effect sizes for length of ICU stay and ICU mortality were not statistically significant. The effect size in relation to the occurrence of delirium was statistically significant only for MLT. | MLTs significantly reduced the occurrence of delirium but did not significantly shorten the duration of delirium. |
| Herling, S.F. [36] | To assess existing evidence for the effect of preventive interventions on ICU delirium, in-hospital mortality, the number of delirium-, coma-, and ventilator-free days, length of stay in the ICU and cognitive impairment. | Adult medical or surgical ICU patients | Physical or cognitive therapy interventions or both, environmental interventions with changes in light or sound/hearing (earplugs), and nursing care intervention. | Physical and cognitive therapy versus standard care: no effect of the intervention; Early mobilization and occupational therapy: positive effects of the intervention time on return to independent function and ventilator-free days and duration of delirium within the first 28 days of hospital stay. Environmental intervention versus standard care: no significant difference between groups. Preventive nursing care interventions: no effect on the event rate of ICU delirium, in-hospital mortality, and on length of ICU stay. | Physical, cognitive, and occupational therapy interventions may have a potential for preventing or reducing the duration of delirium. |
| Bannon, L. [31] | To evaluate the effect of non-pharmacological interventions versus standard care on incidence and duration of delirium in critically ill patients. | ICU patient populations including medical surgical and mixed medical and surgical. | Physical and physical with occupational therapy; bright light therapy; range of motion exercises; earplugs; multicomponent orientation and cognitive stimulation protocol; multicomponent occupational therapy including positioning, cognitive training, and relative involvement; a mirrors intervention; multicomponent targeting risk factors for delirium; protocolized weaning and daily sedation interruption; reorientation using family voice; and paired awakening and breathing. | Incidence of delirium: BLT and individual interventions showed no significant effect between groups. Duration of delirium: MLT physical therapy and various individual interventions showed no significance. Family voice reorientation showed a beneficial effect. | Only family voice reorientation showed a beneficial effect on delirium duration. |
| Deng, L. [38] | To compare non-pharmacological interventions in their ability to prevent delirium in critically ill patients. | Adult patients (>18 years) admitted to ICU of any type. | CHI—cerebral hemodynamic improving; PEI—physical environment intervention; SR—sedation reduction; FP—family participation; EP—exercise program; MLT—multicomponent interventions; UC—usual care. | The most effective intervention in reducing the incidence of delirium was: FP (94%), EP (74%), MLT (68%), CHI (58%), PEI (26%), and SR (18%). In terms of reduction in in-hospital mortality, EP ranked highest (97.2%), followed by: MLT (73.2%), CHI (35.8%), PEI (34.8%), and SR (31.8%). Although not statistically significant, MLT ranked first in both reducing the number of days of delirium (78.6%) and reducing the length of stay in the intensive care unit (71.2%). | MLT are promising; FP has also shown promise as an intervention in reducing the incidence of delirium (still needs further study). |
| Liang, S. [41] | To determine the effects of non-pharmacological interventions on preventing delirium and improving critically ill patients’ clinical, psychological, and family outcomes. | Adult patients (>18 years) admitted to an ICU of various types (surgical, medical, trauma, or cardiac ICUs or a high-dependency unit). Studies involving ICU patients with a history of neurological disorders were excluded. | EM—early mobilization; FP—family participation; PE—patient education; M—music; SP—sleep promotion; PEI—physical environment intervention; MLT—multicomponent interventions; UC—usual care. | MLT had a higher OR than single component interventions. EM in the combined analyses showed a statistically significant effect on reducing the incidence of delirium and duration. FP-analysis pooled showed a statistically significant effect on reducing the incidence of delirium. Additionally, pooled analysis of three of these studies showed a positive effect on LOS in the intensive care unit. There was a statistically significant effect of music on reducing the incidence of delirium (M). Pooled analysis showed that PE caused a statistically significant reduction in the incidence of delirium. The use of earplugs reduced the risk of delirium or disorientation by 53% (SP). | MLT should be a priority for the prevention of delirium in the ICU in clinical practice; FP and EM can be effective non-pharmacological methods for the prevention of delirium in ICU patients. |
| Burry, LD. [45] | To compare the effects of prevention interventions on delirium occurrence in critically ill adults. | Critically ill adults (≥16 years of age in an ICU of any type or high-acuity unit). | Occupational therapy, Early physical therapy daily, Early physical therapy + cognitive exercises, Music, Eye mask + ear plugs + routine night care, Family intervention, Multi-component strategies, Mirrors, Noise reduction, refurbished rooms with suspended ceiling and low frequency sound absorption, Family intervention, orientation training/supervision (memory guidance), therapeutic engagement (cognitive stimulation) and sensory control (e.g., glasses and hearing aids), Delirium prevention protocol including screening for delirium risk factors, subsequent cognitive assessment and orientation, environmental management and therapeutic intervention, Interprofessional early mobilization protocol, Bright light therapy, Standard post-stroke care, therapeutic activities twice daily based on the Hospital Elder Life Program and assessment of anticholinergic burden and medication risk, ABCDE bundle daily. | Pairwise comparisons for single or multicomponent non-pharmacological interventions found no differences compared to standard care for ICU or hospital length of stay, except for mobilization with occupational or physical therapists compared to standard care. | Single and multicomponent non-pharmacological interventions did not connect to any evidence networks to allow for ranking and comparisons as planned; pairwise comparisons did not detect differences compared to standard care. |
| Saritas, S. [46] | To prepare a systematic review with articles that tested the effectiveness of non-pharmacological interventions towards preventing delirium at adult intensive care units. | Patients hospitalized at secondary or tertiary institutions’ adult ICUs. | MLT—multicomponent, PE—patient education, HI—hormone intervention, PEI—physical environment intervention, TI—therapeutic intervention, APS—automated preventive system, QDS—quitting daily sedation and exercise. | All interventions were effective. The multicomponent intervention was statistically significantly effective in terms of reducing/preventing delirium. | The interventions had important effects regarding delirium management, but only the MLT application was significant |
| Qin, M. [47] | To evaluate the effects of family intervention on the incidence and duration of delirium, length of ICU stay, and duration of ventilation in ICU patients. | Adult ICU patients. | Orientation—memory clues delivered by family members, family members’ voices, flexible visitation, or standard family visitation. | Family intervention was associated with a 24% lower risk of delirium. Family intervention reduced the number of delirium days. | Family intervention was associated with a lower risk of delirium and fewer delirium days, but it did not affect the length of ICU stay, the duration of ventilation, or patient mortality. |
| Xu, H. [51] | Impact of cognitive exercise on the incidence of delirium in ICU inpatients. | Adult patients with delirium in the ICU. | Cognitive exercise | The duration of delirium in the treatment group and routine group was significantly different (Z = 3.24, MD = −1.99, 95% CI: −3.20, −0.79, p = 0.001). That cognitive exercise significantly shortened the length of hospital stay in ICU patients with delirium (Z = 10.84, MD = −2.10, 95% CI: −2.48, −1.72, p < 0.00001). | Cognitive exercises can reduce the incidence and duration of delirium in ICU inpatients and shorten the length of hospitalization. |
| Chen, T-J. [48] | To compare the effects of non-pharmacological interventions by combining direct and indirect evidence of the incidence and duration of delirium in intensive care units. | Adults (age ≥ 18 years) in ICU. | EC—environment control; CA—clinical adjustment; PA—physical activity; HE—health education; Multi_A, B, C, D—multicomponent A, B, C, D; LT = light therapy; FM = fluid management; EM—early mobilization, FV—family visit, EE—eye mask and earplugs, EEM—eye mask, earplugs, and melatonin, PHE—preoperative health education. | Multi_A significantly reduced delirium incidence risk compared to routine care (OR = 0.12, 95% CI = 0.02 to 0.83) and was ranked best based on the findings of SUCRA (87.4%). | Multicomponent non-pharmacological interventions are the most effective intervention for ICU delirium prevention but not ICU delirium duration. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lange, S.; Mędrzycka-Dąbrowska, W.; Friganovic, A.; Oomen, B.; Krupa, S. Non-Pharmacological Nursing Interventions to Prevent Delirium in ICU Patients—An Umbrella Review with Implications for Evidence-Based Practice. J. Pers. Med. 2022, 12, 760. https://doi.org/10.3390/jpm12050760
Lange S, Mędrzycka-Dąbrowska W, Friganovic A, Oomen B, Krupa S. Non-Pharmacological Nursing Interventions to Prevent Delirium in ICU Patients—An Umbrella Review with Implications for Evidence-Based Practice. Journal of Personalized Medicine. 2022; 12(5):760. https://doi.org/10.3390/jpm12050760
Chicago/Turabian StyleLange, Sandra, Wioletta Mędrzycka-Dąbrowska, Adriano Friganovic, Ber Oomen, and Sabina Krupa. 2022. "Non-Pharmacological Nursing Interventions to Prevent Delirium in ICU Patients—An Umbrella Review with Implications for Evidence-Based Practice" Journal of Personalized Medicine 12, no. 5: 760. https://doi.org/10.3390/jpm12050760
APA StyleLange, S., Mędrzycka-Dąbrowska, W., Friganovic, A., Oomen, B., & Krupa, S. (2022). Non-Pharmacological Nursing Interventions to Prevent Delirium in ICU Patients—An Umbrella Review with Implications for Evidence-Based Practice. Journal of Personalized Medicine, 12(5), 760. https://doi.org/10.3390/jpm12050760