
High Expression of Interferon Pathway Genes CXCL10 and STAT2 Is Associated with Activated T-Cell Signature and Better Outcome of Oral Cancer Patients



Abstract
:1. Introduction
2. Materials and Methods
2.1. Oral Cancer Data Sets
2.1.1. Discovery Data Sets
2.1.2. Validation Data Sets
2.2. Gene Set Enrichment Analysis
2.3. Kaplan-Meier Survival and Statistical Analyses
2.4. Analysis of Tumor Infiltration Score
3. Results
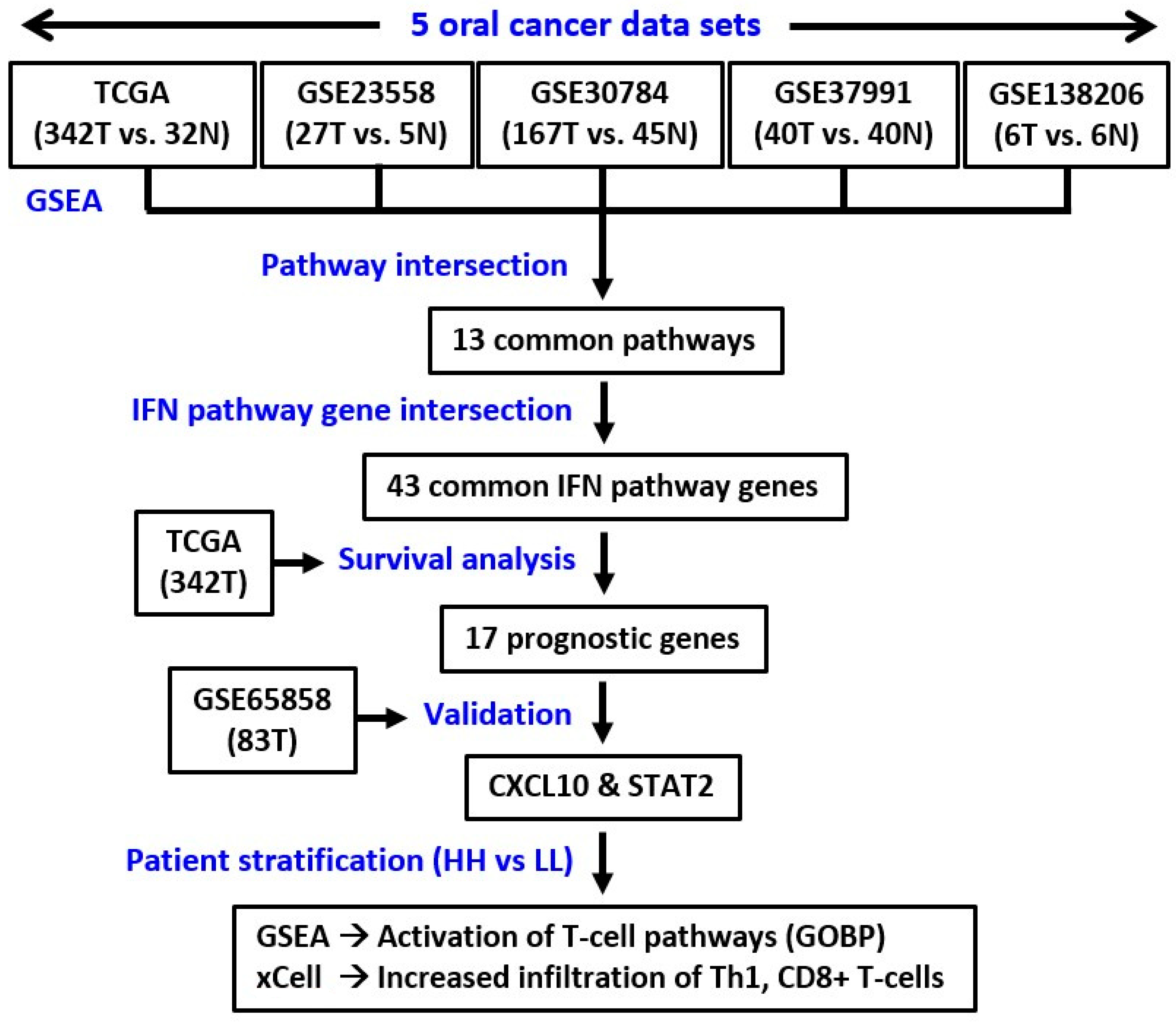
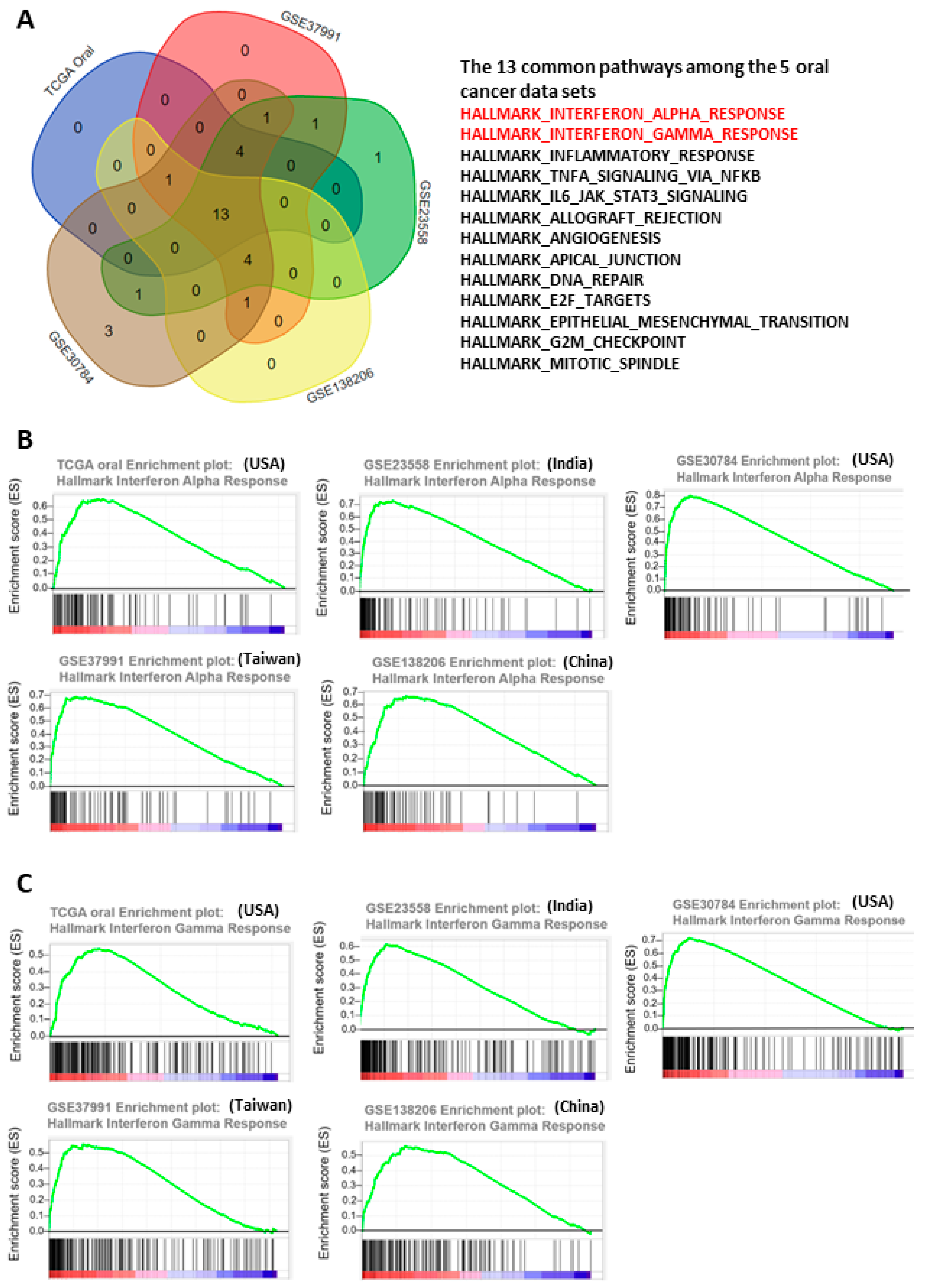
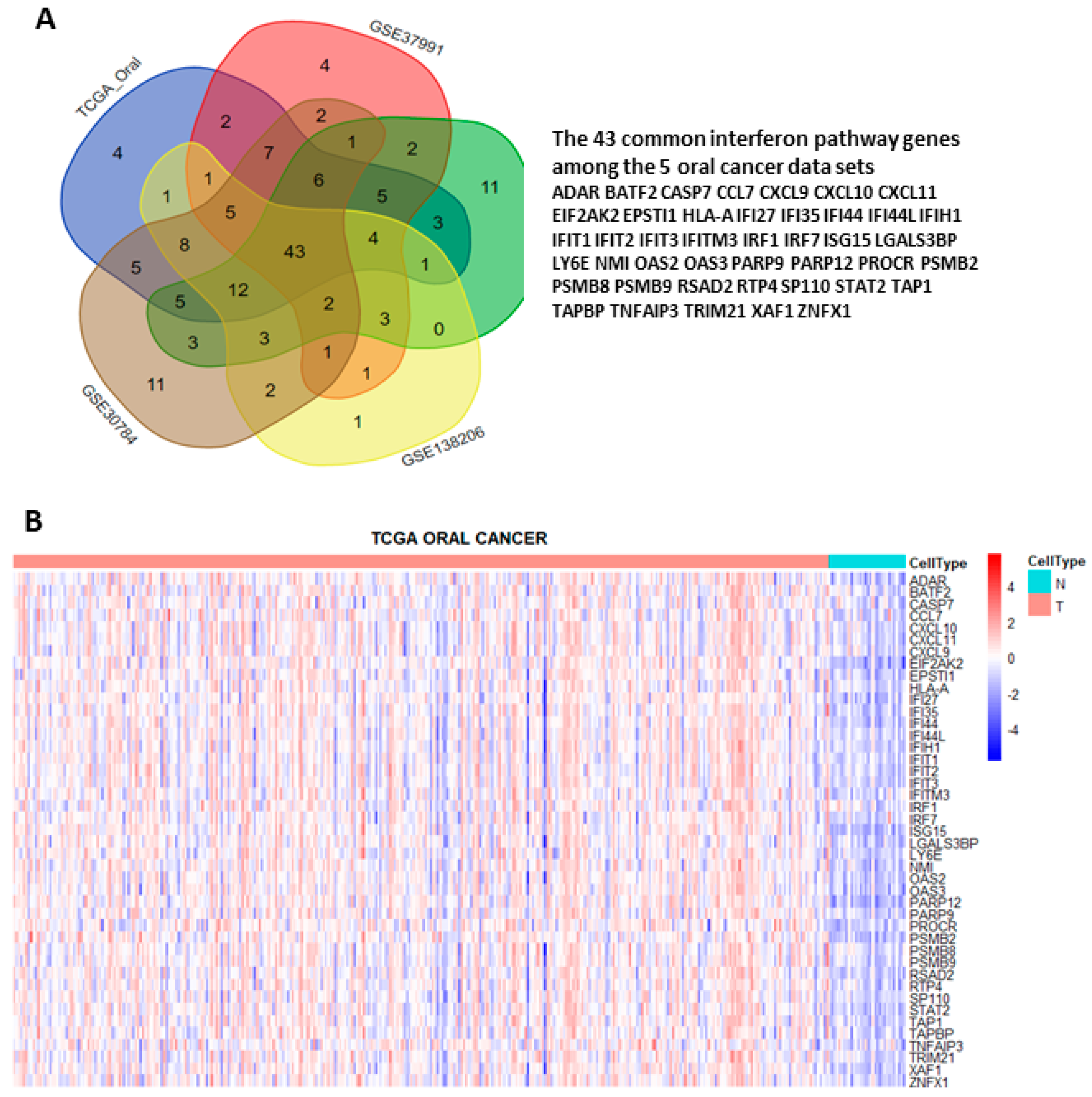
3.1. Interferon Pathways Were Upregulated in Oral Cancer
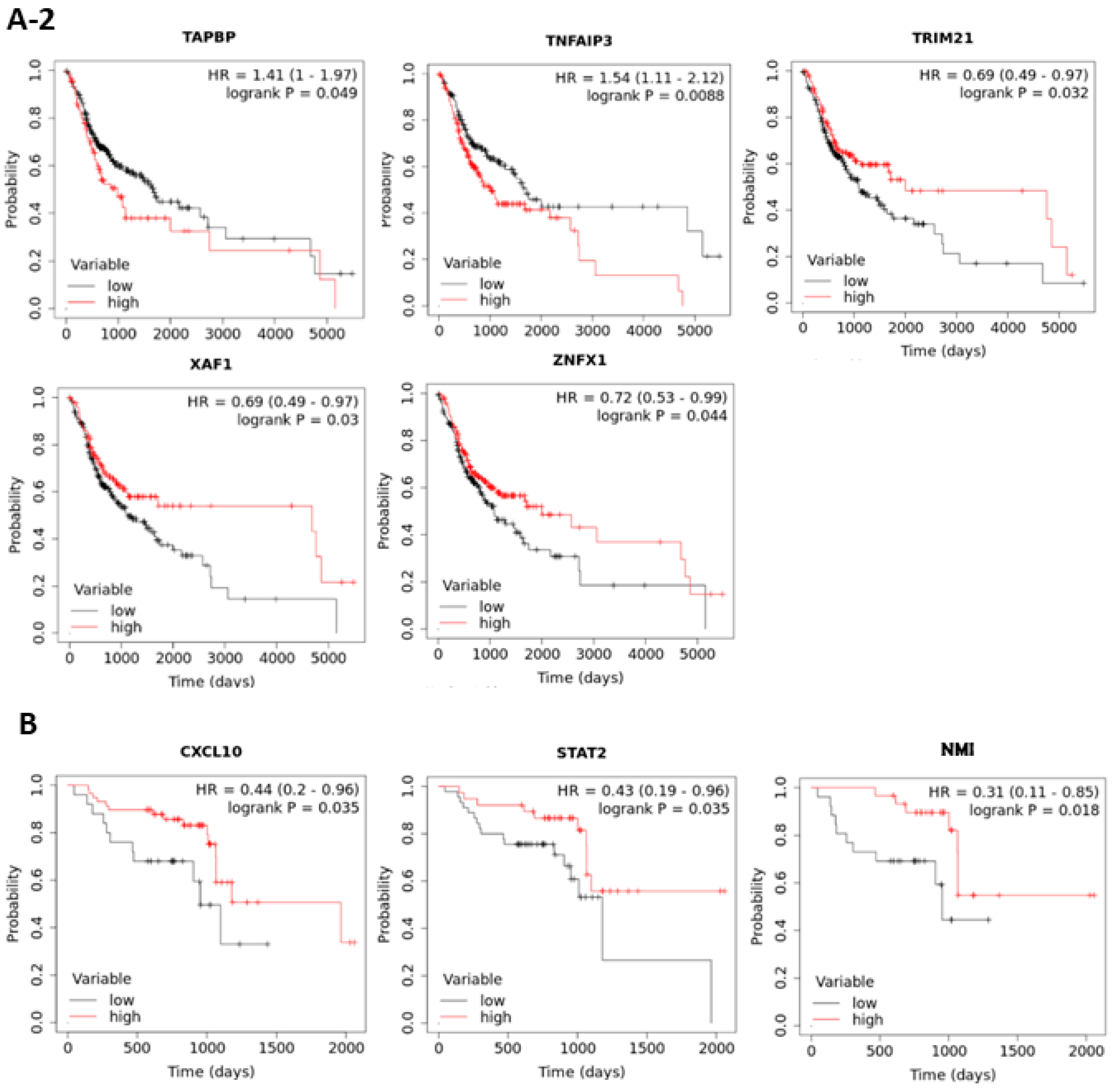
3.2. The Prognostic Roles of Interferon-Related Genes in Oral Cancer
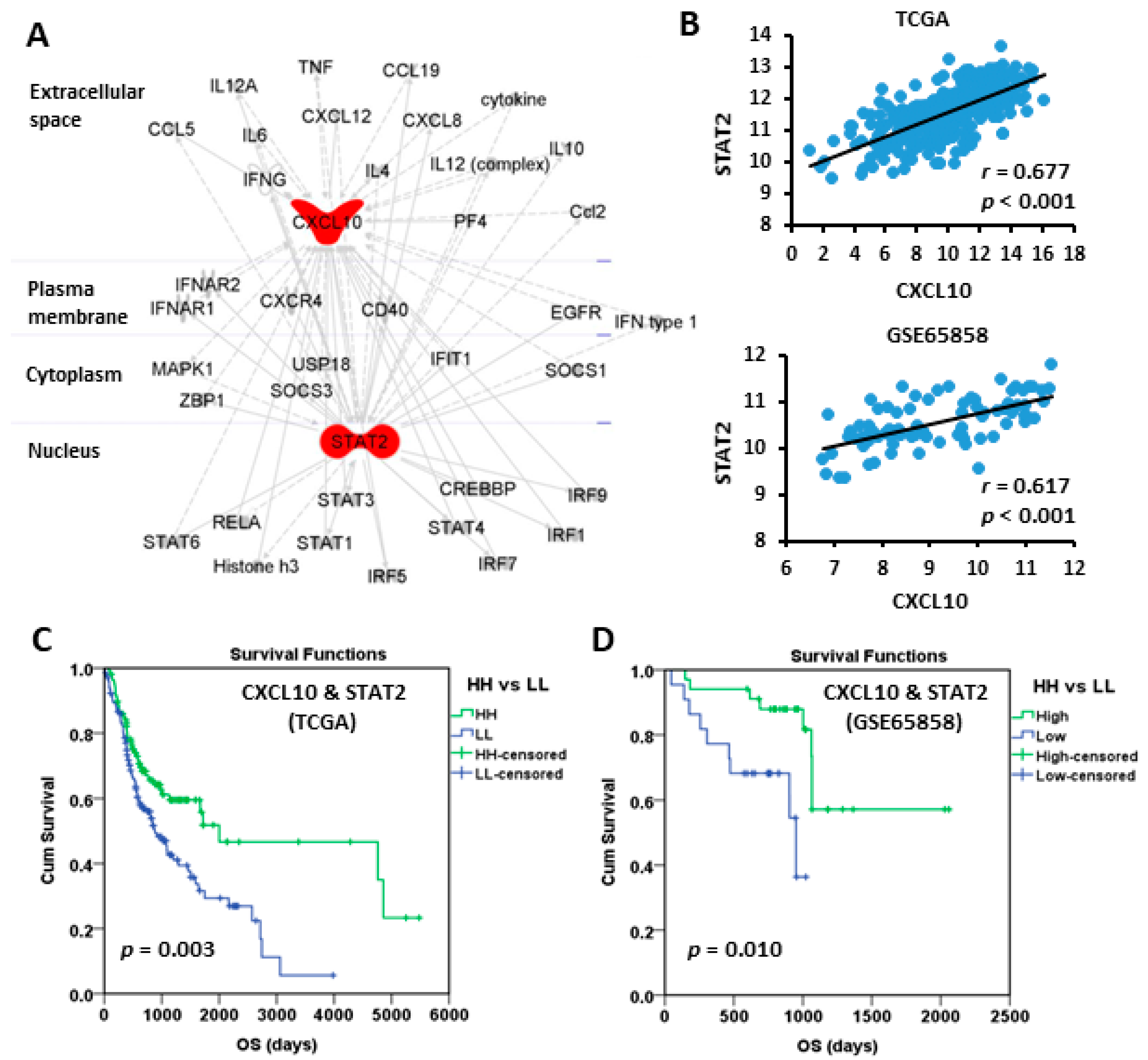
3.3. High Expressions of CXCL10 and STAT2 Were Good Prognostic Factors
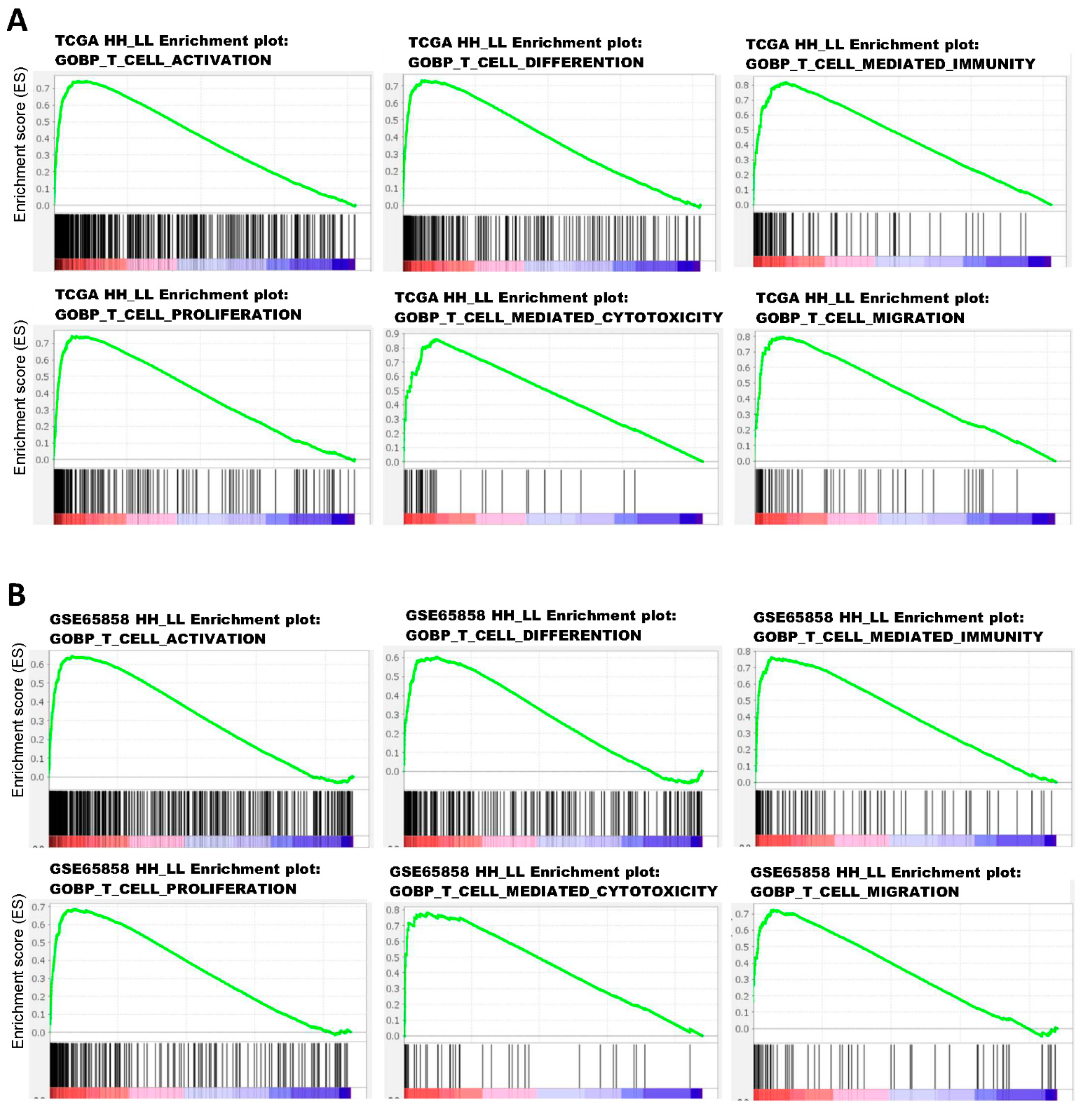
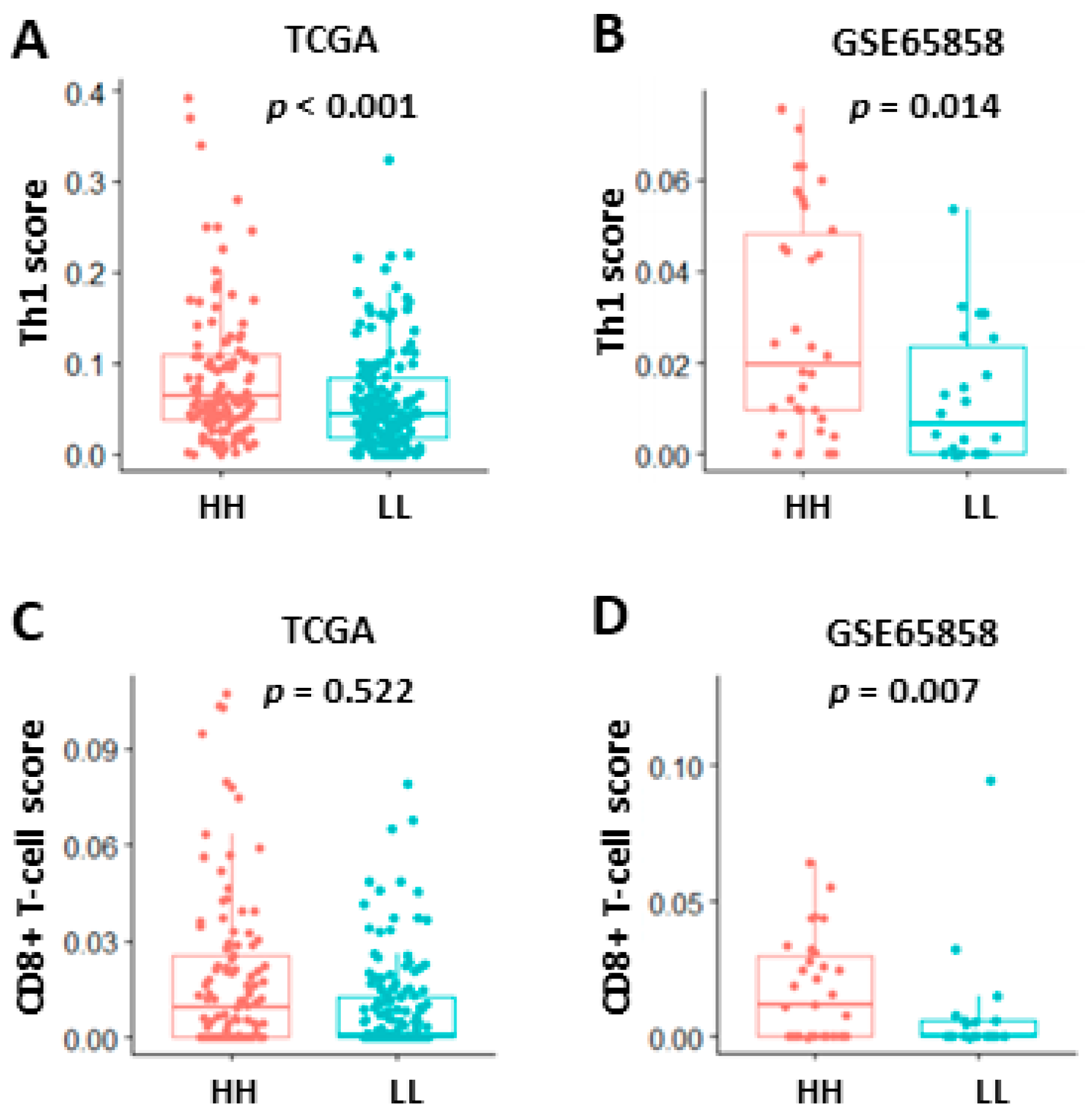
3.4. Activation of T-Cell Pathways in the Patients with High CXCL10/STAT2 Expression
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vermorken, J.B.; Budach, V.; Leemans, C.R.; Machiels, J.-P.; Nicolai, P.; O’Sullivan, B. Critical Issues in Head and Neck Oncology: Key Concepts from the Seventh THNO Meeting; SpringerLink (Online Service); Springer: Cham, Switzerland, 2021; p. 1. [Google Scholar]
- Cristescu, R.; Mogg, R.; Ayers, M.; Albright, A.; Murphy, E.; Yearley, J.; Sher, X.; Liu, X.Q.; Lu, H.; Nebozhyn, M.; et al. Pan-tumor genomic biomarkers for PD-1 checkpoint blockade-based immunotherapy. Science 2018, 362, eaar3593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manzano-Moreno, F.J.; Costela-Ruiz, V.J.; García-Recio, E.; Olmedo-Gaya, M.V.; Ruiz, C.; Reyes-Botella, C. Role of Salivary MicroRNA and Cytokines in the Diagnosis and Prognosis of Oral Squamous Cell Carcinoma. Int. J. Mol. Sci. 2021, 22, 12215. [Google Scholar] [CrossRef]
- Rapado-González, Ó.; López-Cedrún, J.L.; López-López, R.; Rodríguez-Ces, A.M.; Suárez-Cunqueiro, M.M. Saliva Gene Promoter Hypermethylation as a Biomarker in Oral Cancer. J. Clin. Med. 2021, 10, 1931. [Google Scholar] [CrossRef] [PubMed]
- Ronnblom, L.; Leonard, D. Interferon pathway in SLE: One key to unlocking the mystery of the disease. Lupus Sci. Med. 2019, 6, e000270. [Google Scholar] [CrossRef] [Green Version]
- Fenton, S.E.; Saleiro, D.; Platanias, L.C. Type I and II Interferons in the Anti-Tumor Immune Response. Cancers 2021, 13, 1037. [Google Scholar] [CrossRef]
- Schoggins, J.W. Interferon-Stimulated Genes: What Do They All Do? Annu. Rev. Virol. 2019, 6, 567–584. [Google Scholar] [CrossRef]
- Zitvogel, L.; Galluzzi, L.; Kepp, O.; Smyth, M.J.; Kroemer, G. Type I interferons in anticancer immunity. Nature reviews. Immunology 2015, 15, 405–414. [Google Scholar] [CrossRef]
- Shaw, A.E.; Hughes, J.; Gu, Q.; Behdenna, A.; Singer, J.B.; Dennis, T.; Orton, R.J.; Varela, M.; Gifford, R.J.; Wilson, S.J.; et al. Fundamental properties of the mammalian innate immune system revealed by multispecies comparison of type I interferon responses. PLoS Biol. 2017, 15, e2004086. [Google Scholar] [CrossRef]
- Makowska, A.; Franzen, S.; Braunschweig, T.; Denecke, B.; Shen, L.; Baloche, V.; Busson, P.; Kontny, U. Interferon beta increases NK cell cytotoxicity against tumor cells in patients with nasopharyngeal carcinoma via tumor necrosis factor apoptosis-inducing ligand. Cancer Immunol. Immunother. CII 2019, 68, 1317–1329. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.M.; Yuan, J.; Cheung, P.; Chau, D.; Wong, B.W.; McManus, B.M.; Yang, D. Gamma interferon-inducible protein 10 induces HeLa cell apoptosis through a p53-dependent pathway initiated by suppression of human papillomavirus type 18 E6 and E7 expression. Mol. Cell Biol. 2005, 25, 6247–6258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romero-Weaver, A.L.; Wang, H.W.; Steen, H.C.; Scarzello, A.J.; Hall, V.L.; Sheikh, F.; Donnelly, R.P.; Gamero, A.M. Resistance to IFN-alpha-induced apoptosis is linked to a loss of STAT2. Mol. Cancer Res. MCR 2010, 8, 80–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ambatipudi, S.; Gerstung, M.; Pandey, M.; Samant, T.; Patil, A.; Kane, S.; Desai, R.S.; Schaffer, A.A.; Beerenwinkel, N.; Mahimkar, M.B. Genome-wide expression and copy number analysis identifies driver genes in gingivobuccal cancers. Genes Chromosomes Cancer 2012, 51, 161–173. [Google Scholar] [CrossRef] [Green Version]
- Sheu, J.J.; Lee, C.C.; Hua, C.H.; Li, C.I.; Lai, M.T.; Lee, S.C.; Cheng, J.; Chen, C.M.; Chan, C.; Chao, S.C.; et al. LRIG1 modulates aggressiveness of head and neck cancers by regulating EGFR-MAPK-SPHK1 signaling and extracellular matrix remodeling. Oncogene 2014, 33, 1375–1384. [Google Scholar] [CrossRef] [PubMed]
- Goldman, M.J.; Craft, B.; Hastie, M.; Repecka, K.; McDade, F.; Kamath, A.; Banerjee, A.; Luo, Y.; Rogers, D.; Brooks, A.N.; et al. Visualizing and interpreting cancer genomics data via the Xena platform. Nat. Biotechnol. 2020, 38, 675–678. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, A.; Tamayo, P.; Mootha, V.K.; Mukherjee, S.; Ebert, B.L.; Gillette, M.A.; Paulovich, A.; Pomeroy, S.L.; Golub, T.R.; Lander, E.S.; et al. Gene set enrichment analysis: A knowledge-based approach for interpreting genome-wide expression profiles. Proc. Natl. Acad. Sci. USA 2005, 102, 15545–15550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gyorffy, B. Survival analysis across the entire transcriptome identifies biomarkers with the highest prognostic power in breast cancer. Comput. Struct. Biotechnol. J. 2021, 19, 4101–4109. [Google Scholar] [CrossRef] [PubMed]
- Aran, D.; Hu, Z.; Butte, A.J. xCell: Digitally portraying the tissue cellular heterogeneity landscape. Genome Biol. 2017, 18, 220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buttmann, M.; Berberich-Siebelt, F.; Serfling, E.; Rieckmann, P. Interferon-beta is a potent inducer of interferon regulatory factor-1/2-dependent IP-10/CXCL10 expression in primary human endothelial cells. J. Vasc. Res. 2007, 44, 51–60. [Google Scholar] [CrossRef]
- Watanabe, T.; Asano, N.; Fichtner-Feigl, S.; Gorelick, P.L.; Tsuji, Y.; Matsumoto, Y.; Chiba, T.; Fuss, I.J.; Kitani, A.; Strober, W. NOD1 contributes to mouse host defense against Helicobacter pylori via induction of type I IFN and activation of the ISGF3 signaling pathway. J. Clin. Investig. 2010, 120, 1645–1662. [Google Scholar] [CrossRef] [Green Version]
- Karin, N. CXCR3 Ligands in Cancer and Autoimmunity, Chemoattraction of Effector T Cells, and Beyond. Front. Immunol. 2020, 11, 976. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, N.; Ye, J.; Hirakawa, J.; Kawashima, H. Forced Expression of CXCL10 Prevents Liver Metastasis of Colon Carcinoma Cells by the Recruitment of Natural Killer Cells. Biol. Pharm. Bull. 2019, 42, 57–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, C.C.; Kotredes, K.P.; Cremers, T.; Patel, S.; Afanassiev, A.; Slifker, M.; Gallucci, S.; Gamero, A.M. Targeted Stat2 deletion in conventional dendritic cells impairs CTL responses but does not affect antibody production. Oncoimmunology 2020, 10, 1860477. [Google Scholar] [CrossRef] [PubMed]
- Yue, C.; Xu, J.; Tan Estioko, M.D.; Kotredes, K.P.; Lopez-Otalora, Y.; Hilliard, B.A.; Baker, D.P.; Gallucci, S.; Gamero, A.M. Host STAT2/type I interferon axis controls tumor growth. Int. J. Cancer 2015, 136, 117–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Q.; He, Q.; Zhuang, L.; Wang, K.; Yin, C.; He, L. IP10-CDR3 Reduces The Viability And Induces The Apoptosis Of Ovarian Cancer Cells By Down-Regulating The Expression Of Bcl-2 And Caspase 3. Onco Targets Ther. 2019, 12, 9697–9706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Yu, C. Prognostic values of signal transducers activators of transcription in gastric cancer. Biosci. Rep. 2019, 39, BSR20181695. [Google Scholar] [CrossRef] [Green Version]
- Wu, H.T.; Liu, J.; Li, G.W.; Shen, J.X.; Huang, Y.T. The transcriptional STAT3 is a potential target, whereas transcriptional STAT5A/5B/6 are new biomarkers for prognosis in human breast carcinoma. Oncotarget 2017, 8, 36279–36288. [Google Scholar] [CrossRef] [Green Version]
- Ji, W.; Liu, Y.; Xu, B.; Mei, J.; Cheng, C.; Xiao, Y.; Yang, K.; Huang, W.; Jiao, J.; Liu, H.; et al. Bioinformatics Analysis of Expression Profiles and Prognostic Values of the Signal Transducer and Activator of Transcription Family Genes in Glioma. Front. Genet. 2021, 12, 625234. [Google Scholar] [CrossRef]
- Li, C.; Zhou, Y.; Deng, H.; Ye, Y.; Zhao, S.; Liang, S.; Cai, S.; Lin, J.; Tang, Y.; Wu, Y. Mining database for the therapeutic targets and prognostic biomarkers among STAT family in glioblastoma. Cancer Biomark. Sect. A Dis. Markers 2021, 30, 179–191. [Google Scholar] [CrossRef]
- Ni, H.; Sun, H.; Zheng, M.; Bian, T.; Liu, J.; Li, X.; Zhang, J.; Liu, Y. Mining database for the expression and clinical significance of STAT family in head and neck squamous cell carcinomas. Transl. Oncol. 2021, 14, 100976. [Google Scholar] [CrossRef]
- Flores, R.J.; Kelly, A.J.; Li, Y.; Nakka, M.; Barkauskas, D.A.; Krailo, M.; Wang, L.L.; Perlaky, L.; Lau, C.C.; Hicks, M.J.; et al. A novel prognostic model for osteosarcoma using circulating CXCL10 and FLT3LG. Cancer 2017, 123, 144–154. [Google Scholar] [CrossRef] [Green Version]
- Lunardi, S.; Jamieson, N.B.; Lim, S.Y.; Griffiths, K.L.; Carvalho-Gaspar, M.; Al-Assar, O.; Yameen, S.; Carter, R.C.; McKay, C.J.; Spoletini, G.; et al. IP-10/CXCL10 induction in human pancreatic cancer stroma influences lymphocytes recruitment and correlates with poor survival. Oncotarget 2014, 5, 11064–11080. [Google Scholar] [CrossRef] [Green Version]
- Huang, H.; Zhou, W.; Chen, R.; Xiang, B.; Zhou, S.; Lan, L. CXCL10 is a Tumor Microenvironment and Immune Infiltration Related Prognostic Biomarker in Pancreatic Adenocarcinoma. Front. Mol. Biosci. 2021, 8, 611508. [Google Scholar] [CrossRef]
- Li, Y.; Liang, M.; Lin, Y.; Lv, J.; Chen, M.; Zhou, P.; Fu, F.; Wang, C. Transcriptional Expressions of CXCL9/10/12/13 as Prognosis Factors in Breast Cancer. J. Oncol. 2020, 2020, 4270957. [Google Scholar] [CrossRef]
- Bronger, H.; Singer, J.; Windmuller, C.; Reuning, U.; Zech, D.; Delbridge, C.; Dorn, J.; Kiechle, M.; Schmalfeldt, B.; Schmitt, M.; et al. CXCL9 and CXCL10 predict survival and are regulated by cyclooxygenase inhibition in advanced serous ovarian cancer. Br. J. Cancer 2016, 115, 553–563. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Chen, J.; Guan, G.W.; Zhang, T.; Lu, F.M.; Chen, X.M. Expression and clinical significance of chemokine CXCL10 and its receptor CXCR3 in hepatocellular carcinoma. Beijing Da Xue Xue Bao Yi Xue Ban 2019, 51, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Z.; Xu, Y.; Cai, S. CXCL10 expression and prognostic significance in stage II and III colorectal cancer. Mol. Biol. Rep. 2010, 37, 3029–3036. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Wang, Z.; Liu, F.; Zhu, J.; Yang, L.; Cai, G.; Zhang, Z.; Huang, W.; Cai, S.; Xu, Y. CXCL10 mRNA expression predicts response to neoadjuvant chemoradiotherapy in rectal cancer patients. Tumour. Biol. 2014, 35, 9683–9691. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Li, F.; Ping, Y.; Wang, L.; Chen, X.; Wang, D.; Cao, L.; Zhao, S.; Li, B.; Kalinski, P.; et al. Local production of the chemokines CCL5 and CXCL10 attracts CD8+ T lymphocytes into esophageal squamous cell carcinoma. Oncotarget 2015, 6, 24978–24989. [Google Scholar] [CrossRef] [Green Version]
- Qin, X.J.; Lin, X.; Xue, G.; Fan, H.L.; Wang, H.Y.; Wu, J.F.; Pei, D. CXCL10 is a potential biomarker and associated with immune infiltration in human papillary thyroid cancer. Biosci. Rep. 2021, 41, BSR20203459. [Google Scholar] [CrossRef]
- Li, Y.; Wu, T.; Gong, S.; Zhou, H.; Yu, L.; Liang, M.; Shi, R.; Wu, Z.; Zhang, J.; Li, S. Analysis of the Prognosis and Therapeutic Value of the CXC Chemokine Family in Head and Neck Squamous Cell Carcinoma. Front. Oncol. 2021, 10, 570736. [Google Scholar] [CrossRef]
- Korpela, S.P.; Hinz, T.K.; Oweida, A.; Kim, J.; Calhoun, J.; Ferris, R.; Nemenoff, R.A.; Karam, S.D.; Clambey, E.T.; Heasley, L.E. Role of epidermal growth factor receptor inhibitor-induced interferon pathway signaling in the head and neck squamous cell carcinoma therapeutic response. J. Transl. Med. 2021, 19, 43. [Google Scholar] [CrossRef]
- House, I.G.; Savas, P.; Lai, J.; Chen, A.X.Y.; Oliver, A.J.; Teo, Z.L.; Todd, K.L.; Henderson, M.A.; Giuffrida, L.; Petley, E.V.; et al. Macrophage-Derived CXCL9 and CXCL10 Are Required for Antitumor Immune Responses Following Immune Checkpoint Blockade. Clin. Cancer Res. 2020, 26, 487–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, Z.; Shen, J.; Qiu, J.; Zhao, Q.; Hua, K.; Wang, H. CXCL10 potentiates immune checkpoint blockade therapy in homologous recombination-deficient tumors. Theranostics 2021, 11, 7175–7187. [Google Scholar] [CrossRef] [PubMed]
- Reschke, R.; Yu, J.; Flood, B.; Higgs, E.F.; Hatogai, K.; Gajewski, T.F. Immune cell and tumor cell-derived CXCL10 is indicative of immunotherapy response in metastatic melanoma. J. Immunother. Cancer 2021, 9, e003521. [Google Scholar] [CrossRef] [PubMed]
- Seier, J.A.; Reinhardt, J.; Saraf, K.; Ng, S.S.; Layer, J.P.; Corvino, D.; Althoff, K.; Giordano, F.A.; Schramm, A.; Fischer, M.; et al. Druggable epigenetic suppression of interferon-induced chemokine expression linked to MYCN amplification in neuroblastoma. J. Immunother. Cancer 2021, 9, e001335. [Google Scholar] [CrossRef]
- Rentoft, M.; Coates, P.J.; Loljung, L.; Wilms, T.; Laurell, G.; Nylander, K. Expression of CXCL10 is associated with response to radiotherapy and overall survival in squamous cell carcinoma of the tongue. Tumour. Biol. 2014, 35, 4191–4198. [Google Scholar] [CrossRef]
- Li, G.; Li, X.; Yang, M.; Xu, L.; Deng, S.; Ran, L. Prediction of biomarkers of oral squamous cell carcinoma using microarray technology. Sci. Rep. 2017, 7, 42105. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cohort | TCGA 1 (USA) | GSE23558 (India) | GSE30784 (USA) | GSE37991 (Taiwan) | GSE138206 (China) | |
|---|---|---|---|---|---|---|
| Case number | Tumor | 342 | 27 | 167 | 40 2 | 6 2 |
| Normal | 32 | 5 | 45 | 40 | 6 | |
| Gender (male/female) | Tumor | 236/106 | 20/7 | 120/47 | 40/0 | 5/1 |
| Normal | 20/12 | 3/1 3 | 32/13 | 40/0 | 5/1 | |
| Age (yr) | Tumor | 19–90 | 31–78 | 19–88 | - | - |
| Normal | 29–87 | 25–56 | 19–88 | - | - | |
| TCGA | GSE65858 | p-Value | ||
|---|---|---|---|---|
| Total case No. | 342 | 83 | ||
| Gender | Male | 236 (69.0%) | 64 (77.1%) | 0.146 |
| Female | 106 (31.0%) | 19 (22.9%) | ||
| Age (yr) | median (range) | 61 (19–90) | 57 (35–87) | |
| >60 | 187 (54.7%) | 36 (43.4%) | 0.042 | |
| <60 | 148 (43.3%) | 47 (56.6%) | ||
| T stage | T1 | 34 (9.9%) | 14 (16.9%) | 0.022 |
| T2 | 100 (29.2%) | 22 (26.5%) | ||
| T3 | 68 (19.9%) | 8 (9.6%) | ||
| T4 | 113 (33.0%) | 39 (47.0%) | ||
| N stage | N0 | 123 (36.0%) | 36 (43.4%) | 0.352 |
| N1 | 51 (14.9%) | 9 (10.8%) | ||
| N2 | 109 (31.9%) | 36 (43.4%) | ||
| N3 | 3 (0.9%) | 2 (2.4%) | ||
| Status | Alive | 188 (55.0%) | 56 (67.5%) | 0.039 |
| Dead | 154 (45.0%) | 27 (32.5%) | ||
| OS 2 (day) | median (range) | 641 (11–5480) | 831 (46–2059) | |
| Smoking | Yes | 180 (52.6%) | 66 (79.5%) | <0.001 |
| No | 162 (47.4%) | 17 (20.5%) |
| TCGA | Case No. | HR | 95% CI | p |
|---|---|---|---|---|
| HH vs. LL 1 | 108 vs. 144 | 0.568 | 0.389–0.828 | 0.003 |
| T3–4 vs. T1–2 | 141 vs. 97 | 2.448 | 1.602–3.740 | <0.001 |
| N1–3 vs. N0 | 126 vs. 97 | 1.776 | 1.187–2.657 | 0.005 |
| Male vs. Female | 177 vs. 75 | 1.146 | 0.779–1.685 | 0.189 |
| >60-yr vs. <60-yr | 147 vs. 105 | 1.159 | 0.808–1.163 | 0.423 |
| GSE65858 | Case No. | HR | 95% CI | p |
| HH vs. LL 1 | 34 vs. 22 | 0.225 | 0.072–0.705 | 0.010 |
| T3–4 vs. T1–2 | 29 vs. 27 | 4.985 | 1.428–17.397 | 0.012 |
| N1–3 vs. N0 | 31 vs. 25 | 2.271 | 0.798–6.467 | 0.124 |
| Male vs. Female | 42 vs. 14 | 0.743 | 0.274–2.017 | 0.560 |
| >60-yr vs. <60-yr | 25 vs. 31 | 0.747 | 0.272–2.054 | 0.572 |
| TCGA (HH vs. LL) 1 | SIZE | ES | NES | NOM-p | FDR-q |
|---|---|---|---|---|---|
| HALLMARK_INTERFERON_GAMMA_RESPONSE | 196 | 0.8661 | 3.2608 | 0.0000 | 0.0000 |
| HALLMARK_ALLOGRAFT_REJECTION | 195 | 0.8450 | 3.1759 | 0.0000 | 0.0000 |
| HALLMARK_INTERFERON_ALPHA_RESPONSE | 92 | 0.8889 | 3.0438 | 0.0000 | 0.0000 |
| HALLMARK_INFLAMMATORY_RESPONSE | 197 | 0.7469 | 2.8229 | 0.0000 | 0.0000 |
| HALLMARK_IL6_JAK_STAT3_SIGNALING | 87 | 0.7571 | 2.5515 | 0.0000 | 0.0000 |
| HALLMARK_COMPLEMENT | 195 | 0.6451 | 2.4374 | 0.0000 | 0.0000 |
| HALLMARK_TNFA_SIGNALING_VIA_NFKB | 197 | 0.6280 | 2.3792 | 0.0000 | 0.0000 |
| HALLMARK_IL2_STAT5_SIGNALING | 194 | 0.6107 | 2.2753 | 0.0000 | 0.0000 |
| GSE65858 (HH vs. LL) 1 | SIZE | ES | NES | NOM-p | FDR-q |
| HALLMARK_INTERFERON_GAMMA_RESPONSE | 194 | 0.8920 | 3.0061 | 0.0000 | 0.0000 |
| HALLMARK_INTERFERON_ALPHA_RESPONSE | 91 | 0.9404 | 2.8835 | 0.0000 | 0.0000 |
| HALLMARK_ALLOGRAFT_REJECTION | 178 | 0.8150 | 2.7355 | 0.0000 | 0.0000 |
| HALLMARK_INFLAMMATORY_RESPONSE | 189 | 0.7444 | 2.5251 | 0.0000 | 0.0000 |
| HALLMARK_COMPLEMENT | 183 | 0.7261 | 2.4306 | 0.0000 | 0.0000 |
| HALLMARK_IL6_JAK_STAT3_SIGNALING | 82 | 0.7646 | 2.3251 | 0.0000 | 0.0000 |
| HALLMARK_TNFA_SIGNALING_VIA_NFKB | 192 | 0.6421 | 2.1593 | 0.0000 | 0.0000 |
| HALLMARK_IL2_STAT5_SIGNALING | 184 | 0.5779 | 1.9426 | 0.0000 | 0.0000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Y.-C.; Huang, J.-L.; Tseng, L.-C.; Yu, P.-H.; Chen, S.-Y.; Lin, C.-S. High Expression of Interferon Pathway Genes CXCL10 and STAT2 Is Associated with Activated T-Cell Signature and Better Outcome of Oral Cancer Patients. J. Pers. Med. 2022, 12, 140. https://doi.org/10.3390/jpm12020140
Huang Y-C, Huang J-L, Tseng L-C, Yu P-H, Chen S-Y, Lin C-S. High Expression of Interferon Pathway Genes CXCL10 and STAT2 Is Associated with Activated T-Cell Signature and Better Outcome of Oral Cancer Patients. Journal of Personalized Medicine. 2022; 12(2):140. https://doi.org/10.3390/jpm12020140
Chicago/Turabian StyleHuang, Yun-Cian, Jau-Ling Huang, Lu-Chia Tseng, Ping-Hung Yu, Si-Yun Chen, and Chang-Shen Lin. 2022. "High Expression of Interferon Pathway Genes CXCL10 and STAT2 Is Associated with Activated T-Cell Signature and Better Outcome of Oral Cancer Patients" Journal of Personalized Medicine 12, no. 2: 140. https://doi.org/10.3390/jpm12020140
APA StyleHuang, Y.-C., Huang, J.-L., Tseng, L.-C., Yu, P.-H., Chen, S.-Y., & Lin, C.-S. (2022). High Expression of Interferon Pathway Genes CXCL10 and STAT2 Is Associated with Activated T-Cell Signature and Better Outcome of Oral Cancer Patients. Journal of Personalized Medicine, 12(2), 140. https://doi.org/10.3390/jpm12020140