
Pregnancies and Neonatal Outcomes in Patients with Sickle Cell Disease (SCD): Still a (High-)Risk Constellation?

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Disease-Related Definitions, Methods, and Treatments
2.3. Sickle Cell-Associated Definitions
2.4. Pregnancy-Related Definitions
2.5. Treatments
2.6. Statistical Analysis
3. Results
3.1. Maternal, Fetal, and Neonatal Outcomes
3.2. Gestational-, Peri-, and Postpartum Phase in Patients with Severe Genotypes (HbSS, HbS/β-Thalassemia, and HbS/O-Arab Disease)
3.3. Gestational-, Peri-, and Postpartum Phase in Patients with HbS/C Disease
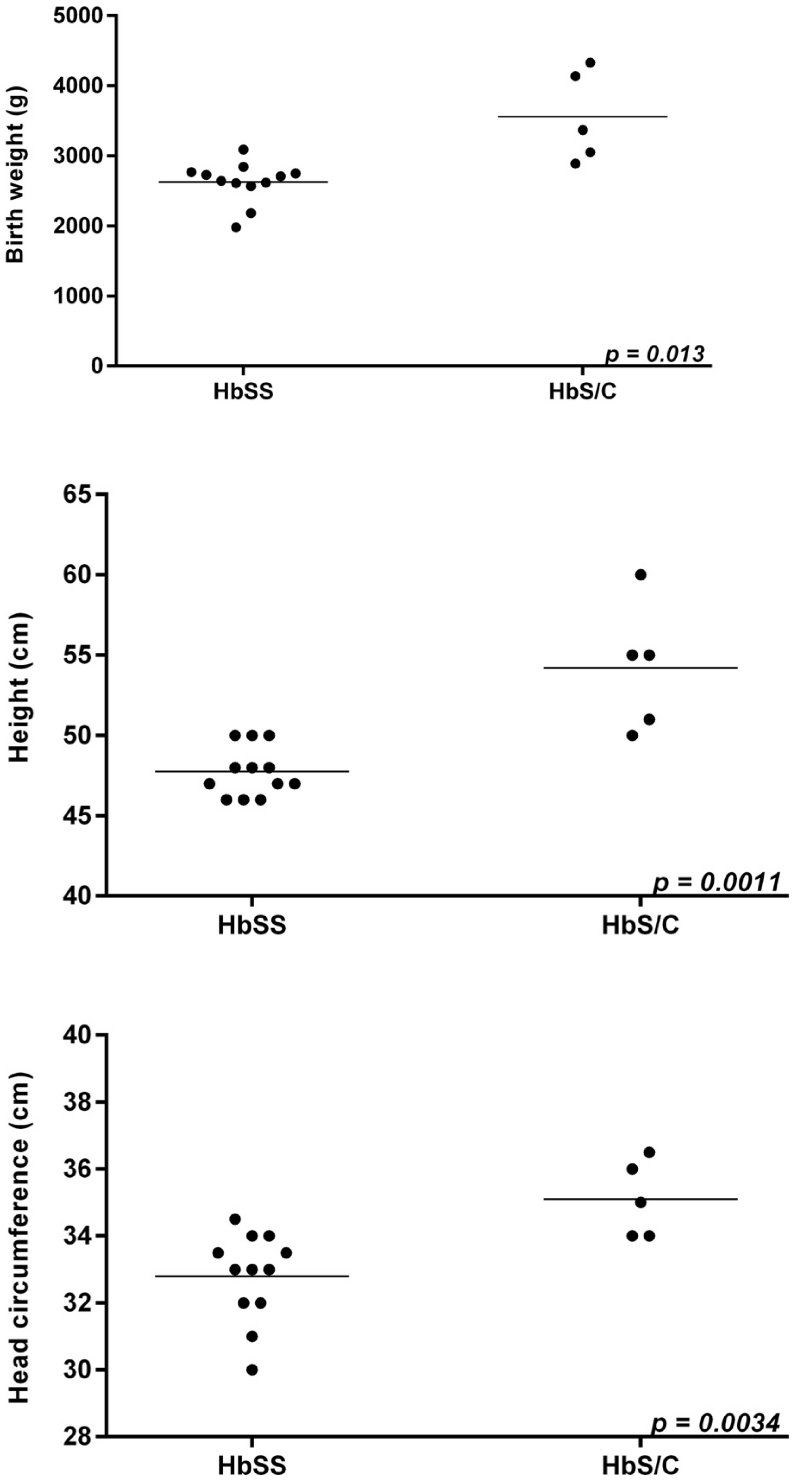
3.4. Neonatal Outcomes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vichinsky, E.P.; Earles, A.; Johnson, R.A.; Hoag, M.S.; Williams, A.; Lubin, B. Alloimmunization in Sickle Cell Anemia and Transfusion of Racially Unmatched Blood. N. Engl. J. Med. 1990, 322, 1617–1621. [Google Scholar] [CrossRef]
- Piel, F.B.; Steinberg, M.H.; Rees, D.C. Sickle Cell Disease. N. Engl. J. Med. 2017, 376, 1561–1573. [Google Scholar] [CrossRef] [Green Version]
- Smith, J.; Espeland, M.; Bellevue, R.; Bonds, D.; Brown, A.; Koshy, M. Pregnancy in Sickle Cell Disease: Experience of the Cooperative study of sickle cell disease. Obstet. Gynecol. 1996, 87, 199–204. [Google Scholar] [CrossRef]
- Oteng-Ntim, E.; Meeks, D.; Seed, P.T.; Webster, L.; Howard, J.; Doyle, P.; Chappell, L.C. Adverse maternal and perinatal outcomes in pregnant women with sickle cell disease: Systematic review and meta-analysis. Blood 2015, 125, 3316–3325. [Google Scholar] [CrossRef]
- EU/3/16/1769|European Medicines Agency. Available online: https://www.ema.europa.eu/en/medicines/human/orphan-designations/eu3161769 (accessed on 29 June 2021).
- Adakveo|European Medicines Agency. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/adakveo (accessed on 29 June 2021).
- Ballas, S.K. The Evolving Pharmacotherapeutic Landscape for the Treatment of Sickle Cell Disease. Mediterr. J. Hematol. Infect. Dis. 2020, 12, e2020010. [Google Scholar] [CrossRef] [PubMed]
- Smith-Whitley, K. Complications in pregnant women with sickle cell disease. Hematology 2019, 1, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Lobitz, S. Perspektive: Neugeborenen -screening auf Sichelzellkrankheiten in Deutschland. Kinder Jugendmed. 2017, 17, 82–86. [Google Scholar] [CrossRef]
- Wong, T.E.; Brandow, A.M.; Lim, W.; Lottenberg, R. Update on the use of hydroxyurea therapy in sickle cell disease. Blood 2014, 124, 3850–3857. [Google Scholar] [CrossRef] [Green Version]
- Siklos|European Medicines Agency. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/siklos (accessed on 29 June 2021).
- Boafor, T.K.; Olayemi, E.; Galadanci, N.; Hayfron-Benjamin, C.; Dei-Adomakoh, Y.; Segbefia, C.; Kassim, A.A.; Aliyu, M.H.; Galadanci, H.; Tuuli, M.G.; et al. Pregnancy outcomes in women with sickle-cell disease in low and high income countries: A systematic review and meta-analysis. BJOG Int. J. Obstet. Gynaecol. 2016, 123, 691–698. [Google Scholar] [CrossRef]
- Bakanay, S.M.; Dainer, E.; Clair, B.; Adekile, A.; Daitch, L.; Wells, L.; Holley, L.; Smith, D.; Kutlar, A. Mortality in sickle cell patients on hydroxyurea therapy. Blood 2005, 105, 545–547. [Google Scholar] [CrossRef] [Green Version]
- Ballas, S.K.; Barton, F.B.; Waclawiw, M.A.; Swerdlow, P.; Eckman, J.R.; Pegelow, C.H.; Koshy, M.; Barton, B.A.; Bonds, D.R. Hydroxyurea and sickle cell anemia: Effect on quality of life. Health Qual. Life Outcomes 2006, 4, 59. [Google Scholar] [CrossRef] [Green Version]
- Voskaridou, E.; Christoulas, D.; Bilalis, A.; Plata, E.; Varvagiannis, K.; Stamatopoulos, G.; Sinopoulou, K.; Balassopoulou, A.; Loukopoulos, D.; Terpos, E. The effect of prolonged administration of hydroxyurea on morbidity and mortality in adult patients with sickle cell syndromes: Results of a 17-year, single-center trial (LaSHS). Blood 2010, 115, 12–2354. [Google Scholar] [CrossRef]
- Jain, D.; Atmapoojya, P.; Colah, R.; Lodha, P. Sickle cell disease and Pregnancy. Mediterr. J. Hematol. Infect. Dis. 2019, 11, 2019040. [Google Scholar] [CrossRef] [PubMed]
- Sun, P.M.; Wilburn, W.; Raynor, B.; Jamieson, D. Sickle cell disease in pregnancy: Twenty years of experience at Grady Memorial Hospital, Atlanta, Georgia. Am. J. Obstet. Gynecol. 2001, 184, 6–1127. [Google Scholar] [CrossRef]
- Babah, O.A.; Aderolu, M.B.; Oluwole, A.A.; Afolabi, B.B. Towards zero mortality in sickle cell pregnancy: A prospective study comparing haemoglobin SS and AA women in Lagos, Nigeria. Niger. Postgrad. Med. J. 2019, 26, 1–7. [Google Scholar] [CrossRef]
- Gellen-Dautremer, J.; Le Jeune, S.; Receveur, M.-C.; Foïs, E. Hydroxyurea Exposure throughout Pregnancy in Patients with Sickle-Cell Disease: 4 Case Reports from European Non-Interventional, Multicentric, Prospective Escort-HU Study. Blood 2019, 134, 1027. [Google Scholar] [CrossRef]
- Galactéros, F.; Cannas, G.; Bartolucci, P.; Voskaridou, E.; Joseph, L.; Bernit, E.; Gellen-Dautremer, J.; Charneau, C.; Ngo, S.; Habibi, A. Outcomes of Pregnancies in Patients with Sickle-Cell Disease: Update from European Non-Interventional, Multicentric, Prospective Escort-HU Study. Blood 2019, 134, 891. [Google Scholar] [CrossRef]
- Malinowski, A.K.; Shehata, N.; D’Souza, R.; Kuo, K.H.M.; Ward, R.; Shah, P.S.; Murphy, K. Prophylactic transfusion for pregnant women with sickle cell disease: A systematic review and meta-analysis. Blood 2015, 126, 2424–2435. [Google Scholar] [CrossRef] [Green Version]
- Elenga, N.; Adeline, A.; Balcaen, J.; Vaz, T.; Calvez, M.; Terraz, A.; Accrombessi, L.; Carles, G. Pregnancy in Sickle Cell Disease Is a Very High-Risk Situation: An Observational Study. Obstet. Gynecol. Int. 2016, 2016, 9069054. [Google Scholar] [CrossRef] [Green Version]
- Whittington, J.R.; Magann, E.F.; Ounpraseuth, S.T.; Chang, J.N.; Whitcombe, D.D.; Morrison, J.C. Evidence for Prophylactic Transfusion during Pregnancy for Women with Sickle Cell Disease. South. Med. J. 2021, 114, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Driss, F.; Tertian, G.; Becquemont, L.; Haddad, B.; Cynober, T.; Raphael, M.; Tchernia, G. Prise en charge des grossesses à risque chez les femmes drépanocytaires: Intérêt d’une stratégie préventive par des transfusions de globules rouges ou des échanges érythrocytaires automatisés. Transfus. Clin. Biol. 2007, 14, 386–392. [Google Scholar] [CrossRef]
- Chou, S.T.; Jackson, T.; Vege, S.; Smith-Whitley, K.; Friedman, D.F.; Westhoff, C.M. High prevalence of red blood cell alloimmunization in sickle cell disease despite transfusion from Rh-matched minority donors. Blood 2013, 122, 1062–1071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sippert, E.; Fujita, C.R. Variant RH alleles and Rh immunisation in patients with sickle cell disease. Blood Transfus. 2015, 13, 72. [Google Scholar] [CrossRef]
- Chou, S.T.; Alsawas, M.; Fasano, R.M.; Field, J.J.; Hendrickson, J.E.; Howard, J.; Kameka, M.; Kwiatkowski, J.L.; Pirenne, F.; Shi, P.A.; et al. American Society of Hematology 2020 guidelines for sickle cell disease: Transfusion support. Blood Adv. 2020, 28, 327–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Natukunda, B.; Schonewille, H.; Ndugwa, C.; Brand, A. Red blood cell alloimmunization in sickle cell disease patients in Uganda. Transfusion 2010, 50, 20–25. [Google Scholar] [CrossRef]
- Tormey, C.A.; Stack, G. The persistence and evanescence of blood group alloantibodies in men. Transfusion 2009, 49, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Nickel, R.S.; Hendrickson, J.E.; Fasano, R.M.; Meyer, E.K.; Winkler, A.M.; Yee, M.M.; Lane, P.A.; Jones, Y.A.; Pashankar, F.D.; New, T.; et al. Impact of red blood cell alloimmunization on sickle cell disease mortality: A case series. Transfusion 2016, 56, 107–114. [Google Scholar] [CrossRef]
- Costa, D.C.D.; Pellegrino, J., Jr.; Guelsin, G.A.S.; Ribeiro, K.A.R.; Gilli, S.C.O.; Castilho, L. Molecular matching of red blood cells is superior to serological matching in sickle cell disease patients. Rev. Bras. Hematol. Hemoter. 2013, 35, 35–38. [Google Scholar] [CrossRef] [Green Version]
- Schonewille, H.; Prinsen-Zander, K.J.; Reijnart, M.; Van De Watering, L.; Zwaginga, J.-J.; Meerman, R.H.; Van Kamp, I.L.; Brand, A. Extended matched intrauterine transfusions reduce maternal Duffy, Kidd, and S antibody formation. Transfusion 2015, 55, 2912–2919. [Google Scholar] [CrossRef]
- Hendrickson, J.E.; Tormey, C.A. Understanding red blood cell alloimmunization triggers. Hematology 2016, 2016, 446–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oakley, L.L.; Awogbade, M.; Brien, S.; Briley, A.; Chorozoglou, M.; Drasar, E.; Johns, J.; Rhodes, E.; Robinson, V.; Seed, P.; et al. Serial prophylactic exchange blood transfusion in pregnant women with sickle cell disease (TAPS-2): Study protocol for a randomised controlled feasibility trial. Trials 2020, 21, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Vianello, A.; Vencato, E.; Cantini, M.; Zanconato, G.; Manfrin, E.; Zamo, A.; Zorzi, F.; Mazzi, F.; Martinelli, N.; Cavaliere, E.; et al. Improvement of maternal and fetal outcomes in women with sickle cell disease treated with early prophylactic erythrocytapheresis. Transfusion 2018, 58, 2192–2201. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Patient-ID | Genotype ((Genetic) Origin) | Gravida (G), Para (P); Age (Years) | Before Conception | Gestation Period | Country (Abortion/Stillbirth/Delivery) | Peripartum Period | Postpartum Period |
|---|---|---|---|---|---|---|---|
| SCD-Associated Complication (HC Dosage; Alloantibodies) | SCD-Associated Complications | SCD-Associated Complications | SCD-Associated Complications | ||||
| Exclusively succesful pregnancy outcomes | |||||||
| 1 | HbSS-α+-thalassemia (Nigeria) | G1, P0; 39 | recurrent VOCs/APCs, intermittent transfusion demand for RBCs (hemolytic/symtpomatic anemia, VOCs) (HC: 8 mg/kg BW; alloantibodies: anti-K) | VOCs, transfusion demand for RBCs (hemolytic/symptomatic anemia) | Germany | - | - |
| 2 | HbSS (Togo) | G1, P0; 32 | recurrent APCs | APCs, transfusion demand for RBCs (hemolytic/symptomatic anemia; 1 unit) | Germany | CS secondary to birth arrest in the active-phase arrest | Transfusion demand for RBCs (2 units) due to symptomatic anemia (Hb 5.6 g/dL); Wound infection of the cesarean scar |
| G2, P1; 38 | recurrent APCs, st. p. cholecystectomy (cholecystolithiasis) | APCs | Germany | APCs | - | ||
| 3 | HbSS (Guinea) | G1, P0; 14 | - | VOCs/APCs | Guinea | NDA | - |
| G2, P1; 20 | APCs (childhood), st. p. left hip joint endoprosthesis (left femoral head necrosis), st. p. cholecystectomy (cholecystolithiasis); HBV/HDV infection | VOCs, requiring inpatient admissions, UTIs | Germany | PROM, AIS | - | ||
| 4 | HbSS (Turkey) | G1, P0; 24 | recurrent VOCs/APCs; intermittent transfusion demand for RBCs (hemolytic/symtpomatic anemia/VOCs), right femoral head necrosis, st. p. cholecystectomy (cholecystolithiasis) | VOCs, including ACS (RBC-exchange transfusion (GW 15)), requiring inpatient admissions, recurrent transfusion demand for RBCs (hemolytic/symptomatic anemia), UTIs | Germany | AIS (GW 37) | Transfusion demand for RBCs (2 units) (symptomatic anemia (Hb 6.5 g/dL)) |
| G2, P1; 27 | VOCs, including ACS (RCE (GW 29+3)), requiring inpatient admissions, transfusion demand for RBCs (hemolytic/symptomatic anemia), UTIs | Germany | - | - | |||
| 5 | HbSS (Guinea) | G1, P0; 17 (Germany: GW 30; refugee status) | recurrent VOCs/APCs, intermittent transfusion demand for RBCs (hemolytic/symtpomatic anemia, VOCs (Guinea)) | GW 30: VOC, requiring inpatient admission, transfusion demand for RBCs (hemolytic/symptomatic anemia), UTI | Germany | - | - |
| 6 | HbSS (Nigeria) | G1, P0; 26 (refugee status) | - | - | Germany | CS secondary to active-phase arrest, transfusion demand for RBCs (hemolytic/symptomatic anemia; 2 units) | - |
| G2, P1; 28 | splenic sequestration (RBC transfusion), cholecystolithiasis (HC 15 mg/kg BW) | VOCs/APCs, requiring inpatient admissions, transfusion demand for RBCs (hemolytic/symptomatic anemia), UTIs | Germany | transfusion demand for RBCs (PROM/hemolytic/symptomatic anemia; 2 units) | - | ||
| 7 | HbSS (Togo) | G1, P0; 17 | recurrent VOCs/APCs, including ACS, intermittent transfusion demand for RBCs (hemolytic/symptomatic anemia, VOCs), cholecystolithiasis (27 mg/kg BW) | VOCs, requiring inpatient admissions (GW 9 and 27), transfusion demand for pRBCs (hemolytic/symptomatic anemia; 1 unit (GW 9)), UTI | Germany | Cervical insufficiency | - |
| 8 | HbS/β-thalassemia (Syria) | G1, P0; 33 | recurrent VOCs/APCs, including ACS (pulmonary embolism); st. p. splenectomy (transfusion demand for pRBCs, hemolytic/symptomatic anemia, VOCs (Syria)), cholecystolithiasis (HC: 20 mg/kg BW) | Transfusion demand for RBCs (hemolytic/symptomatic anemia; Hb <7 g/dl; 5 units, GW 20, 25, 30 (borderline doppler indices; intrauterine growth restriction), APC | Germany | CS (secondary to pathologic CTG and doppler indices, placental insufficiency) | Transfusion demand for RBCs (2 units) due to symptomatic anemia (Hb 8.5 g/dL) |
| 9 | HbS/C (Ghana) | G1, P0; 30 | - | - | Germany | - | - |
| G2, P1; 31 | - | - | Germany | - | - | ||
| G3, P2; 32 | - | - | Germany | AIS | - | ||
| 10 | HbS/C (Ghana) | G1, P0; 35 | APCs | APCs | Germany | - | - |
| Successful and unsuccessful pregnancy outcomes | |||||||
| 11 | HbSS-α+-thalassemia (Angola); Delta-storage pool disease (Diagnosis: 4th pregnancy) | G1, P0; 20 | VOCs/APCs, intermittent transfusion demand for RBCs (hemolytic/symptomatic anemia, VOCs) (childhood), cholecystolithiasis, st. p. splenectomy | - | Germany (spontaneous abortion, GW 6) | ||
| G2, P0; 21 | - | Germany (spontaneous abortion, GW 11) | |||||
| G3, P0; 22 | VOCs/APCs, transfusion demand for RBCs (1 unit) | Germany | VOC, transfusion demand for RBCs (hemolytic/symptomatic anemia; 1 unit) | - | |||
| G4, P1; 25 | VOCs/APCs, requiring inpatient admission (GW 26, 28), transfusion demand for RBCs (hemolytic/symptomatic anemia; 6 units); UTI-> urosepsis (GW 28) | Germany | CS (fetal subdural hematoma; GW 29 + 5); re-sectio (hematoma evacuation); re-re-sectio (post-bleeding); re-re-re-sectio (hysterectomy); re-re-re-re-sectio (hematoma evacuation); re-re-re-re-re-sectio (post-bleeding); hemorrhagic shock; DIC; ACS (pulmonary embolism); transfusion demand for RBCs (overall: 49 pRBC units) and platetes (16 units); postpartum cardiomyopathy (HFrEF; EF 20–35%) | ||||
| 12 | HbSS-α+-thalassemia (Nigeria) | G1, P0; 27 | VOCs/APCs | APCs | Nigeria | - | - |
| G2, P1; 30 | APCs | Germany (elective abortion) | |||||
| G2, P1; 33 | APCs | Germany (spontaneous abortion) | |||||
| 13 | HbSS-α+-thalassemia (Zaire) | G1, P0; 17 | VOCs/APCs, transfusion demand for RBCs (hemolytic symptomatic anemia, VOCs); st. p. splenectomy; st. p. cholecystectomy (cholecystolithiasis), infections (HC: 35 mg/kg BW) | - | Germany (elective abortion) | ||
| G2, P0; 19 | VOCs/APCs, transfusion demand for RBCs (hemolytic symptomatic anemia, VOCs), left DVT (HC: 25 mg/kg BW) | VOCs/APCs, requiring inpatient admissions (GW 16, 32), transfusion demand for pRBCs (hemolytic/symptomatic anemia; 6 units), febrile UTIs | Germany | PROM, CS secondary to active-phase arrest | Transfusion demand for RBCs (hemolytic/symptomatic anemia; 1 unit) | ||
| G3, P1; 22 | VOCs/APCs, including ACSs (3rd ACS: vvECMO), transfusion demand for RBCs (hemolytic/symptomatic anemia, VOCs), gram-negative port infection (HC: 25 mg/kg BW) | VOCs/APCs, requiring inpatient admissions (GW 8, 11, 24, 29, 33), transfusion demand for RBCs (hemolytic/symptomatic anemia; 4 units) | Germany | PROM | - | ||
| 14 | HbSS (Dominican Republic) | G1, P0; 18 | VOCs/APCs, including ACS, intermittent transfusion demand for RBCs (hemolytic/symptomatic anemia, VOCs), infections, cholecystolithiasis | VOCs/APCs, transfusion demand for RBCs (hemolytic/symptomatic anemia; 3 units) | Dominican Republic | - | - |
| G2, P1; 21 | - | Dominican Republic (spontaneous abortion) | |||||
| G3, P1; 25 | VOCs/APCs, transfusion demand for RBCs (hemolytic/symptomatic anemia; 2 units) | Dominican Republic | - | - | |||
| G4, P2; 30 | - | Germany (spontaneous abortion) | |||||
| 15 | HbSS (Congo) | G1, P0; 24 | VOCs/APCs, including ACS; 4 yr. history of transfusion therapy (20–24th years of age; Italy) | VOCs/APCs, requiring inpatient admissions (SP(E)BT, every 3 weeks) | Italy | - | Continuation of transfusion therapy |
| G2, P1; 29 | VOCs/APCs (HC: 20 mg/kg BW) | VOCs, requiring inpatient admissions, transfusion demand for RBCs (hemolytic/symptomatic anemia; 3 units) | Germany | HELLP-Syndrome | - | ||
| G3, P2; 32 | VOCs/APCs (HC: 20 mg/kg BW) | - | Germany (spontaneous abortion) | ||||
| 16 | HbSS (Angola) | G1, P0; 20 | VOCs/APCs, transfusion demand for RBCs (hemolytic/symptomatic anemia) (Angola/Belgium) (HC: 15 mg/kg BW; alloantibodies: anti- E, -M) | - | Belgium (sponatenous abortion) | ||
| G2, P1; 22 (Germany: GW 29, refugee status) | VOCs/APCs, requiring inpatient admissions (GW 29), transfusion demand for RBCs (hemolytic/symptomatic anemia; 2 units), possible DHTR (Anti-S) following RBC transfusion in the context of a VOC (DD febrile hyperhemolytic VOC (UTI)) (re-start HU (20 mg/kg BW), GW 34 + EPO) | Germany | vaginal bleedings (GW 35), PPROM | ||||
| G3, P2; 24 | VOCs/APCs, including ACS, transfusion demand for RBCs (hemolytic/symptomatic anemia) (HC: 20 mg/kg BW + EPO; alloantibodies: anti- E, -M, -S) | VOCs/APCs, requiring inpatient admissions (GW 13 and 17) (infectious-related), transfusion demand for RBCs (hemolytic/symptomatic anemia; 5 units) (EPO throughout pregnancy; re-start HU GW 30; 15 mg/kg BW) | Germany | - | - | ||
| 17 | HbS/C-α+-thalassemia (Ghana) | G1, P0; 17 | VOCs/APCs | - | Germany (elective abortion) | ||
| G2, P0; 22 | - | Germany | - | - | |||
| 18 | HbS/C (Nigeria) | G1, P0; 24 | VOCs/APCs | - | Germany (elective abortion) | ||
| G2, P0; 26 | APCs, transfusion demand for RBCs (hemolytic/symptomatic anemia; 2 units) | Germany | - | APCs | |||
| G3, P1; 28 | APCs | Germany | VOC-infectious related (UTI -> pyelonephritis) -> ACS | - | |||
| 19 | HbS/O-Ara (Kenya) | G1, P0; 28 | recurrent VOCs (child- and adulthood), including recurrent ACSs (childhood) and transfusion demand for RBCs (symptomatic/hemolytic anemia, VOCs) | DVT | Germany (stillbirth, GW 26) | ||
| G2, P0; 28 | - | Germany (spontaneous abortion, GW 11) | |||||
| G3, P0; 29 | VOCs | Germany | Placental abruption | - | |||
| Unsuccessful pregnancy outcomes | |||||||
| 20 | HbSS-α+-thalassemia (Suriname) | G1, P0; 31 | VOCs/APCs (childhood) | - | Germany (ectopic pregnancy (IVF); medical abortion) | ||
| G3, P0; 32 | - | - | Germany (spontaneous abortion, (IVF)) | ||||
| G3, P0; 32 | - | - | Germany (ectopic pregnancy (IVF); medical abortion) | ||||
| 21 | HbSS (Congo) | G1, P0; 22 | Recurrent VOCs/APCs, including ACS, intermittent transfusion demand for RBCs (hemolytic/symptomatic anemia, VOCs; 8 units), right femoral head necrosis | - | Germany (elective abortion) | ||
| G2, P0; 24 | recurrent VOCs/APCs, intermittent transfusion demand for RBCs (hemolytic/symptomatic anemia; 2 units), st. p. right hip joint endoprothesis (right femoral head necrosis), left humerus head necrosis (HC: 16 mg/kg BW) | - | Germany (elective abortion) | ||||
| G3, P0; 28 | recurrent VOCs/APCs, including ACS, intermittent transfusion demand for RBCs (hemolytic/symptomatic anemia; 2 units) (HC: 21 mg/kg BW) | - | Germany (elective abortion) | ||||
| G4, P0; 28 | recurrent VOCs/APCs (HC: 25 mg/kg BW) | - | Germany (spontaneous abortion) | ||||
| 22 | HbS-β-thalassemia (Cuba) | G1, P0; 18 | recurrent VOCs/APCs, including ACS, st. p. splenectomy (splenic sequestration), transfusion demand for RBCs (hemolytic/symptomatic anemia, VOCs) | - | Germany (elective abortion) | ||
| G2, P0; 39 | recurrent VOCs/APCs, including ACS, bi-femoral head necrosis (st. p. femoral head cannulation) | - | Germany (elective abortion) | ||||
| Patient-ID/Genotype (Mother) | Pregnancy | Delivery | Newborn | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Time a | Type | Country (Birth) | Apgar Score b | ApH | VpH | BE (mmol/l) | Weight (g) | Height (cm) | Head Circumference (cm) | ||
| HbSS (±α+-thalassemia) | |||||||||||
| 1 | 1st | 38 + 4 | CS | Germany | 9/10/10 | 7.25 | 7.3 | −1.2 | 3090 | 50 | 34 |
| 2 | 1st | 39 + 1 | CS | Germany | 8/10/10 | 7.16 | - | −11.5 | 2620 | 48 | 33 |
| 2nd | 38 + 1 | CS | Germany | 9/10/10 | 7.25 | - | −6.7 | 2730 | 50 | 33.5 | |
| 3 | 1st | 36 | CS | Guinea | - | - | - | - | - | - | - |
| 2nd | 37 + 1 | VD | Germany | 9/10 /10 | 7.2 | - | - | 2710 | 48 | 32 | |
| 4 | 1st | 37 + 5 | CS | Germany | 9/10/10 | 7.32 | 7.38 | - | 2610 | 47 | 34.5 |
| 2nd | 39 + 5 | VD | Germany | 9/10/10 | 7.29 | 7.36 | - | 2770 | 46 | 33.5 | |
| 5 | 1st | 37 + 5 | VD | Germany | 6/7/8 | 7.19 | - | −10 | 1980 | 46 | 31 |
| 6 | 1st | 38 + 3 | CS | Germany | 7/9/10 | 7.29 | - | −5.8 | 2570 | 47 | 33 |
| 2nd | 35 + 1 | CS | Germany | 7/8/9 | 7.34 | 7.37 | - | 1900 | 40 | 31 | |
| 7 | 1st | 37 + 1 | VD | Germany | 9/10/10 | 7.10 | 7.27 | 11 | 2185 | 46 | 32 |
| 11 | 3rd | 37 + 5 | CS | Germany | 9/10/10 | 7.33 | 7.37 | 0.4 | 2750 | 48 | 30 |
| 4th | 29 + 5 | CS | Germany | 7/8/8 | 7.37 | - | - | 1600 | 41 | 29 | |
| 12 | 1st | 36 | CS | Nigeria | - | - | - | - | - | - | - |
| 13 | 2nd | 38 + 6 | CS | Germany | 9/10/10 | 7.32 | 7.37 | −2.4 | 2845 | 47 | 33 |
| 3rd | 37 + 7 | VD | Germany | 9/10/10 | 7.29 | 7.31 | - | 2645 | 50 | 34 | |
| 14 | 1st | 39 | VD | Dominican Republic | - | - | - | - | - | - | - |
| 3rd | 40 | CS | Dominican Republic | - | - | - | - | - | - | - | |
| 15 | 1st | 32 | CS | Italy | - | - | - | - | - | - | - |
| 2nd | 34 + 1 | CS | Germany | 8/8/9 | 7.3 | 7.37 | 2320 | - | - | ||
| 16 | 2nd | 35 + 2 | VD | Germany | 10/10/10 | 7.27 | 7.28 | −5.6 | 2540 | 46 | 32 |
| 3rd | 34 + 4 | VD | Germany | 7/8/9 | 7.22 | 7.26 | −4.5 | 2300 | 42 | 31 | |
| HbS/β-thalassemia | |||||||||||
| 8 | 1st | 30 + 5 | CS | Germany | - | 7.21 | - | - | 946 | 36 | 27.2 |
| HbS/C | |||||||||||
| 9 | 1st | 39 + 0 | VD | Germany | 9/10/10 | 7.35 | - | - | 4140 | 55 | 36.5 |
| 2nd | 38 | VD | Germany | - | - | - | - | - | - | - | |
| 3rd | 40 + 6 | VD | Germany | 9/10/10 | 7.29 | - | −2.4 | 4330 | 55 | 36 | |
| 10 | 1st | 35 + 6 | VD | Germany | 9/10/10 | 7.38 | - | - | 2550 | 48 | 29.5 |
| 17 | 1st | 40 + 0 | VD | Germany | 10/10/10 | 7.28 | 7.35 | −3 | 3370 | 60 | 34 |
| 18 | 2nd | 38 + 5 | VD | Germany | 9/10/10 | 7.29 | - | - | 3050 | 50 | 35 |
| 3rd | 37 + 3 | CS | Germany | 7/9/10 | 7.31 | 7.33 | −2.6 | 2890 | 51 | 34 | |
| HbS/O-Arab | |||||||||||
| 19 | 3rd | 29 + 2 | CS | Germany | 7/8/9 | 7.32 | 1140 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Proske, P.; Distelmaier, L.; Aramayo-Singelmann, C.; Koliastas, N.; Iannaccone, A.; Papathanasiou, M.; Temme, C.; Klump, H.; Lenz, V.; Koldehoff, M.; et al. Pregnancies and Neonatal Outcomes in Patients with Sickle Cell Disease (SCD): Still a (High-)Risk Constellation? J. Pers. Med. 2021, 11, 870. https://doi.org/10.3390/jpm11090870
Proske P, Distelmaier L, Aramayo-Singelmann C, Koliastas N, Iannaccone A, Papathanasiou M, Temme C, Klump H, Lenz V, Koldehoff M, et al. Pregnancies and Neonatal Outcomes in Patients with Sickle Cell Disease (SCD): Still a (High-)Risk Constellation? Journal of Personalized Medicine. 2021; 11(9):870. https://doi.org/10.3390/jpm11090870
Chicago/Turabian StyleProske, Pia, Laura Distelmaier, Carmen Aramayo-Singelmann, Nikolaos Koliastas, Antonella Iannaccone, Maria Papathanasiou, Christian Temme, Hannes Klump, Veronika Lenz, Michael Koldehoff, and et al. 2021. "Pregnancies and Neonatal Outcomes in Patients with Sickle Cell Disease (SCD): Still a (High-)Risk Constellation?" Journal of Personalized Medicine 11, no. 9: 870. https://doi.org/10.3390/jpm11090870
APA StyleProske, P., Distelmaier, L., Aramayo-Singelmann, C., Koliastas, N., Iannaccone, A., Papathanasiou, M., Temme, C., Klump, H., Lenz, V., Koldehoff, M., Carpinteiro, A., Reinhardt, H. C., Köninger, A., Röth, A., Yamamoto, R., Dührsen, U., & Alashkar, F. (2021). Pregnancies and Neonatal Outcomes in Patients with Sickle Cell Disease (SCD): Still a (High-)Risk Constellation? Journal of Personalized Medicine, 11(9), 870. https://doi.org/10.3390/jpm11090870