
Application of Machine Learning for Predicting Anastomotic Leakage in Patients with Gastric Adenocarcinoma Who Received Total or Proximal Gastrectomy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Variables
2.2. Outcome
2.3. Machine Learning Algorithms
2.4. Statistical Analysis
3. Results
3.1. Summary of Demographic and Clinical Characteristics for Training and Testing Sets
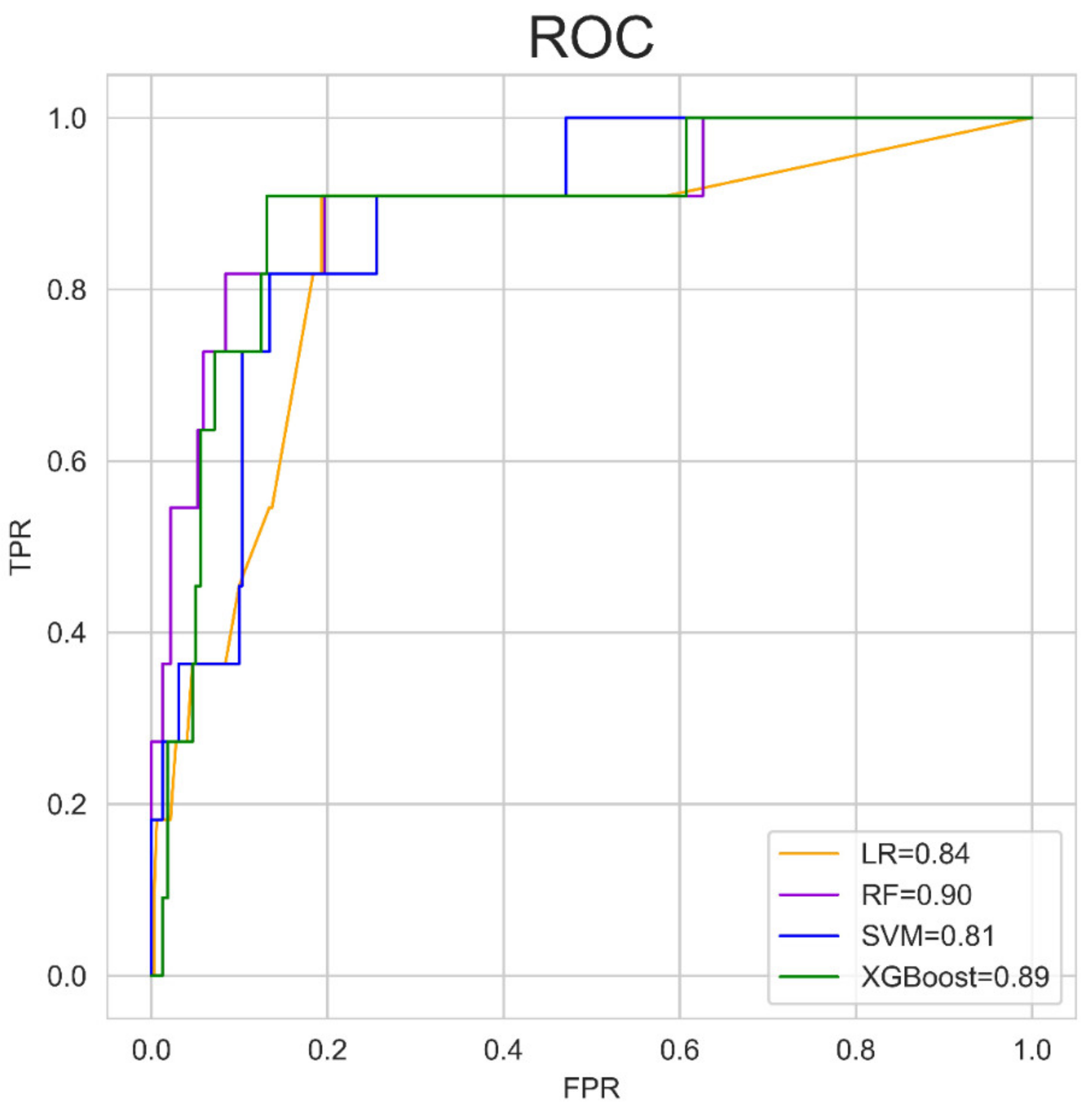
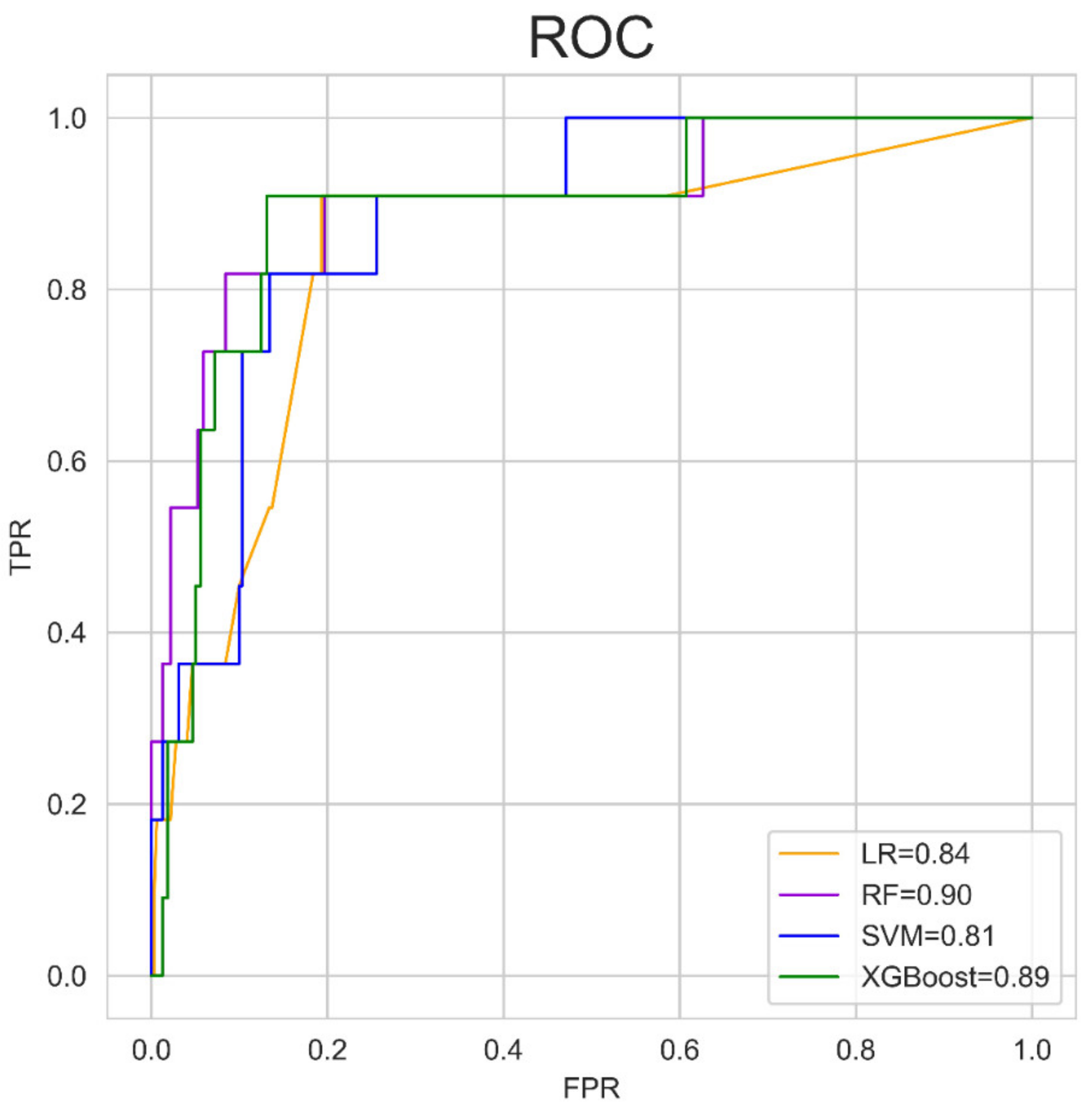
3.2. Performance of the Machine Learning Algorithms
3.3. Predictive Abilities of the Machine Learning Models
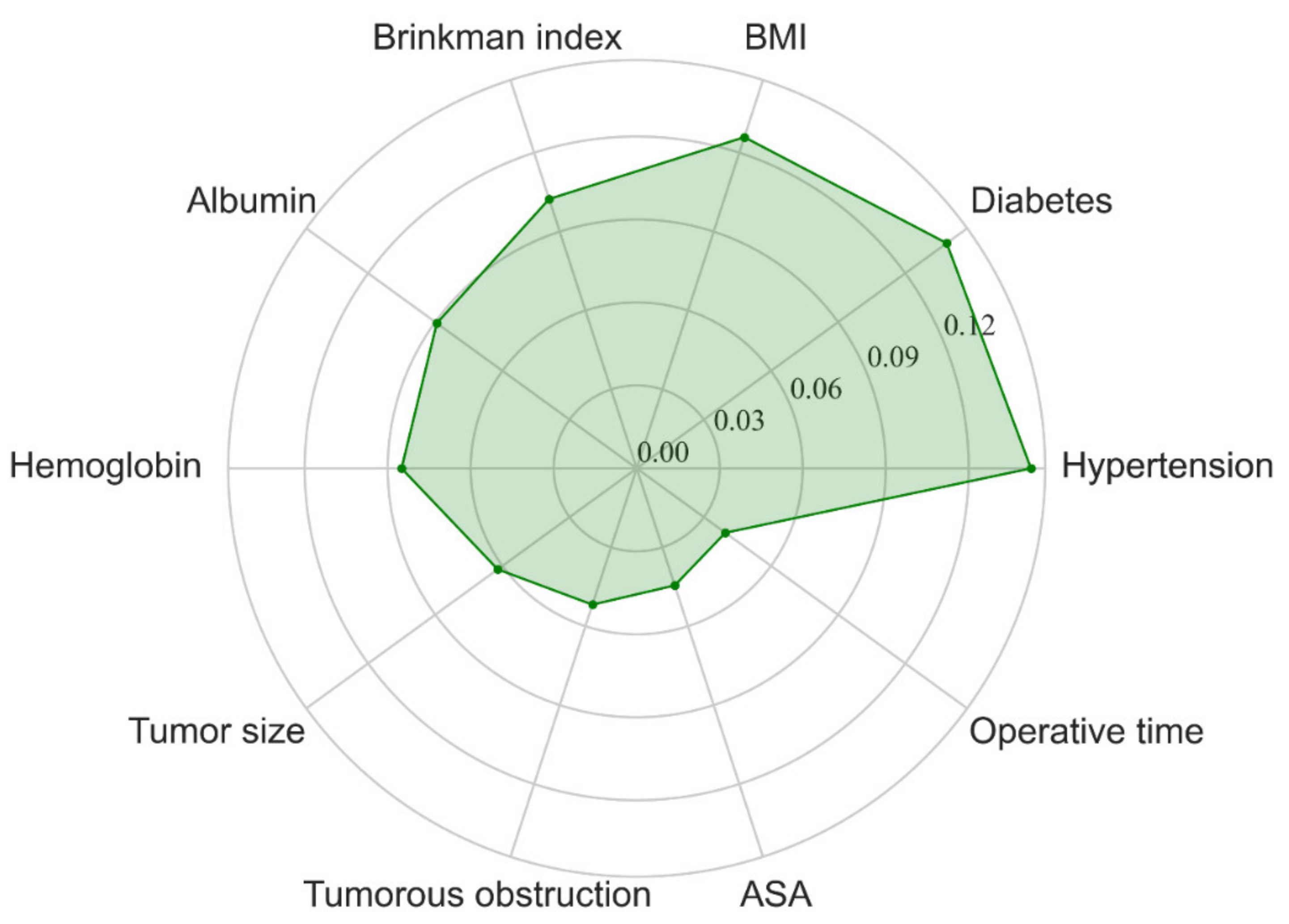
3.4. Feature Importance Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.H.; Hyung, W.J.; Cho, G.S.; Kim, M.C.; Han, S.U.; Kim, W.; Ryu, S.W.; Lee, H.J.; Song, K.Y. Morbidity and mortality of laparoscopic gastrectomy versus open gastrectomy for gastric cancer: An interim report--A phase III multicenter, prospective, randomized Trial (KLASS Trial). Ann. Surg. 2010, 251, 417–420. [Google Scholar] [CrossRef] [PubMed]
- Aurello, P.; Berardi, G.; Moschetta, G.; Cinquepalmi, M.; Antolino, L.; Nigri, G.; D’Angelo, F.; Valabrega, S.; Ramacciato, G. Recurrence Following Anastomotic Leakage After Surgery for Carcinoma of the Distal Esophagus and Gastroesophageal Junction: A Systematic Review. Anticancer Res. 2019, 39, 1651–1660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gong, W.; Li, J. Combat with esophagojejunal anastomotic leakage after total gastrectomy for gastric cancer: A critical review of the literature. Int. J. Surg. 2017, 47, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Tu, R.H.; Lin, J.X.; Zheng, C.H.; Li, P.; Xie, J.W.; Wang, J.B.; Lu, J.; Chen, Q.Y.; Cao, L.L.; Lin, M.; et al. Development of a nomogram for predicting the risk of anastomotic leakage after a gastrectomy for gastric cancer. Eur. J. Surg. Oncol. 2017, 43, 485–492. [Google Scholar] [CrossRef]
- Makuuchi, R.; Irino, T.; Tanizawa, Y.; Bando, E.; Kawamura, T.; Terashima, M. Esophagojejunal anastomotic leakage following gastrectomy for gastric cancer. Surg. Today 2019, 49, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, Y.; Kanda, M.; Tanaka, C.; Kobayashi, D.; Mizuno, A.; Iwata, N.; Hayashi, M.; Niwa, Y.; Takami, H.; Yamada, S.; et al. Usefulness of preoperative estimated glomerular filtration rate to predict complications after curative gastrectomy in patients with clinical T2-4 gastric cancer. Gastric Cancer 2017, 20, 736–743. [Google Scholar] [CrossRef] [Green Version]
- Bhinder, B.; Gilvary, C.; Madhukar, N.S.; Elemento, O. Artificial Intelligence in Cancer Research and Precision Medicine. Cancer Discov. 2021, 11, 900–915. [Google Scholar] [CrossRef] [PubMed]
- Quer, G.; Arnaout, R.; Henne, M.; Arnaout, R. Machine Learning and the Future of Cardiovascular Care: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2021, 77, 300–313. [Google Scholar] [CrossRef]
- Shung, D.L.; Au, B.; Taylor, R.A.; Tay, J.K.; Laursen, S.B.; Stanley, A.J.; Dalton, H.R.; Ngu, J.; Schultz, M.; Laine, L. Validation of a Machine Learning Model That Outperforms Clinical Risk Scoring Systems for Upper Gastrointestinal Bleeding. Gastroenterology 2020, 158, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Kudo, S.E.; Ichimasa, K.; Villard, B.; Mori, Y.; Misawa, M.; Saito, S.; Hotta, K.; Saito, Y.; Matsuda, T.; Yamada, K.; et al. Artificial Intelligence System to Determine Risk of T1 Colorectal Cancer Metastasis to Lymph Node. Gastroenterology 2020. [Google Scholar] [CrossRef]
- Luo, H.; Xu, G.; Li, C.; He, L.; Luo, L.; Wang, Z.; Jing, B.; Deng, Y.; Jin, Y.; Li, Y.; et al. Real-time artificial intelligence for detection of upper gastrointestinal cancer by endoscopy: A multicentre, case-control, diagnostic study. Lancet Oncol. 2019, 20, 1645–1654. [Google Scholar] [CrossRef]
- Kather, J.N.; Pearson, A.T.; Halama, N.; Jäger, D.; Krause, J.; Loosen, S.H.; Marx, A.; Boor, P.; Tacke, F.; Neumann, U.P.; et al. Deep learning can predict microsatellite instability directly from histology in gastrointestinal cancer. Nat. Med. 2019, 25, 1054–1056. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, R.; Long, J.; Longacre, T.; Peng, L.; Berry, G.; Martin, B.; Higgins, J.; Rubin, D.L.; Shen, J. Deep learning model for the prediction of microsatellite instability in colorectal cancer: A diagnostic study. Lancet Oncol. 2021, 22, 132–141. [Google Scholar] [CrossRef]
- Kawakami, E.; Tabata, J.; Yanaihara, N.; Ishikawa, T.; Koseki, K.; Iida, Y.; Saito, M.; Komazaki, H.; Shapiro, J.S.; Goto, C.; et al. Application of Artificial Intelligence for Preoperative Diagnostic and Prognostic Prediction in Epithelial Ovarian Cancer Based on Blood Biomarkers. Clin. Cancer Res. 2019, 25, 3006–3015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oshi, M.; Kunisaki, C.; Miyamoto, H.; Kosaka, T.; Akiyama, H.; Endo, I. Risk Factors for Anastomotic Leakage of Esophagojejunostomy after Laparoscopy-Assisted Total Gastrectomy for Gastric Cancer. Dig. Surg. 2018, 35, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Kunisaki, C.; Miyata, H.; Konno, H.; Saze, Z.; Hirahara, N.; Kikuchi, H.; Wakabayashi, G.; Gotoh, M.; Mori, M. Modeling preoperative risk factors for potentially lethal morbidities using a nationwide Japanese web-based database of patients undergoing distal gastrectomy for gastric cancer. Gastric Cancer 2017, 20, 496–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kann, B.H.; Hosny, A.; Aerts, H. Artificial intelligence for clinical oncology. Cancer Cell 2021, 39, 916–927. [Google Scholar] [CrossRef] [PubMed]
- Ngiam, K.Y.; Khor, I.W. Big data and machine learning algorithms for health-care delivery. Lancet Oncol. 2019, 20, e262–e273. [Google Scholar] [CrossRef]
- Goecks, J.; Jalili, V.; Heiser, L.M.; Gray, J.W. How Machine Learning Will Transform Biomedicine. Cell 2020, 181, 92–101. [Google Scholar] [CrossRef]
- Ichimasa, K.; Kudo, S.E.; Mori, Y.; Misawa, M.; Matsudaira, S.; Kouyama, Y.; Baba, T.; Hidaka, E.; Wakamura, K.; Hayashi, T.; et al. Artificial intelligence may help in predicting the need for additional surgery after endoscopic resection of T1 colorectal cancer. Endoscopy 2018, 50, 230–240. [Google Scholar] [CrossRef] [PubMed]
- Nudel, J.; Bishara, A.M.; de Geus, S.W.L.; Patil, P.; Srinivasan, J.; Hess, D.T.; Woodson, J. Development and validation of machine learning models to predict gastrointestinal leak and venous thromboembolism after weight loss surgery: An analysis of the MBSAQIP database. Surg. Endosc. 2021, 35, 182–191. [Google Scholar] [CrossRef] [PubMed]
- Inokuchi, M.; Otsuki, S.; Fujimori, Y.; Sato, Y.; Nakagawa, M.; Kojima, K. Systematic review of anastomotic complications of esophagojejunostomy after laparoscopic total gastrectomy. World J. Gastroenterol. 2015, 21, 9656–9665. [Google Scholar] [CrossRef]
- Nakagawa, M.; Tokunaga, M.; Aburatani, T.; Sato, Y.; Matsuyama, T.; Nakajima, Y.; Kinugasa, Y. Feasibility and Safety of Early Oral Intake and Discharge After Total or Proximal Gastrectomy: An Analysis of Consecutive Cases Without Exclusion Criteria. Ann. Surg. Oncol. 2020, 27, 812–821. [Google Scholar] [CrossRef] [PubMed]
- Miyawaki, Y.; Sato, H.; Fujiwara, N.; Sugita, H.; Sakuramoto, S.; Okamoto, K.; Yamaguchi, S.; Koyama, I. Evaluation of the Associations between Gastric Tube Preparation Methods and the Incidence of Cervical Anastomotic Leakage after Esophagectomy for Thoracic Esophageal Cancer. Dig. Surg. 2020, 37, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Li, S.J.; Wang, Z.Q.; Li, Y.J.; Fan, J.; Zhang, W.B.; Che, G.W.; Liu, L.X.; Chen, L.Q. Diabetes mellitus and risk of anastomotic leakage after esophagectomy: A systematic review and meta-analysis. Dis. Esophagus 2017, 30, 1–12. [Google Scholar] [CrossRef]
- Hasegawa, T.; Kubo, N.; Ohira, M.; Sakurai, K.; Toyokawa, T.; Yamashita, Y.; Yamazoe, S.; Kimura, K.; Nagahara, H.; Amano, R.; et al. Impact of body mass index on surgical outcomes after esophagectomy for patients with esophageal squamous cell carcinoma. J. Gastrointest. Surg. 2015, 19, 226–233. [Google Scholar] [CrossRef]
- Ji, L.; Wang, T.; Tian, L.; Gao, M. The early diagnostic value of C-reactive protein for anastomotic leakage post radical gastrectomy for esophagogastric junction carcinoma: A retrospective study of 97 patients. Int. J. Surg. 2016, 27, 182–186. [Google Scholar] [CrossRef]
- Deguchi, Y.; Fukagawa, T.; Morita, S.; Ohashi, M.; Saka, M.; Katai, H. Identification of Risk Factors for Esophagojejunal Anastomotic Leakage after Gastric Surgery. World J. Surg. 2012, 36, 1617–1622. [Google Scholar] [CrossRef]
- Zhao, G.F.; Zhang, K.P.; Gao, S.G.; Mu, J.W.; Mao, Y.S.; Wang, D.L.; Gao, Y.S.; Lyu, F.; Zhao, L.; Xue, Q. Analysis of the risk factors for postoperative cervical anastomotic leakage after McKeown’s esophagectomy. Zhonghua Zhong Liu Za Zhi [Chin. J. Oncol.] 2017, 39, 287–292. [Google Scholar] [CrossRef]
- Dong, T.S.; Kalani, A.; Aby, E.S.; Le, L.; Luu, K.; Hauer, M.; Kamath, R.; Lindor, K.D.; Tabibian, J.H. Machine Learning-based Development and Validation of a Scoring System for Screening High-Risk Esophageal Varices. Clin. Gastroenterol. Hepatol. 2019, 17, 1894–1901.e1891. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.C.; Yeh, W.C.; Hsu, W.D.; Islam, M.M.; Nguyen, P.A.A.; Poly, T.N.; Wang, Y.C.; Yang, H.C.; Jack Li, Y.C. Prediction of fatty liver disease using machine learning algorithms. Comput. Methods Programs Biomed. 2019, 170, 23–29. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variables | Training Set (n = 1328) | Testing Set (n = 332) | p Value |
|---|---|---|---|
| Male, n (%) | 983 (74.0%) | 242 (72.9%) | 0.626 |
| Age, mean (SD), years | 58.94 (9.80) | 59.66 (10.71) | 0.242 |
| BMI, mean (SD), kg/m2 | 21.01 (2.65) | 21.02 (2.76) | 0.930 |
| Hypertension, n (%) | 312 (23.5%) | 67 (20.2%) | 0.214 |
| Diabetes, n (%) | 88 (6.6%) | 23 (6.9%) | 0.807 |
| Previous abdominal surgery, n (%) | 260 (19.6%) | 60 (18.1%) | 0.586 |
| Brinkman index, mean (SD) | 221.34 (412.59) | 199.94 (316.26) | 0.388 |
| Alcohol use, n (%) | 272 (20.5%) | 64 (19.3%) | 0.648 |
| Hemoglobin, mean (SD), g/L | 119.96 (22.17) | 120.24 (23.73) | 0.839 |
| Albumin, mean (SD), g/L | 38.46 (4.57) | 38.74 (4.90) | 0.325 |
| Tumor size, mean (SD), cm | 4.34 (2.33) | 4.36 (2.40) | 0.881 |
| Tumorous obstruction, n (%) | 226 (17.0%) | 58 (17.5%) | 0.871 |
| Neoadjuvant, n (%) | 33 (2.5%) | 7 (2.1%) | 0.842 |
| Total gastrectomy, n (%) | 898 (67.6%) | 237 (71.4%) | 0.210 |
| Esophagogastrostomy, n (%) | 424 (31.9%) | 89 (26.8%) | 0.073 |
| Combined resection, n (%) | 68 (5.1%) | 21 (6.3%) | 0.413 |
| Laparoscopic surgery, n (%) | 1133 (85.3%) | 283 (85.2%) | 1.000 |
| Blood loss, mean (SD), ml | 146.95 (252.80) | 140.66 (222.05) | 0.678 |
| Intraperitoneal chemotherapy, n (%) | 979 (73.7%) | 254 (76.5%) | 0.326 |
| Nasogastric tube, n (%) | 1305 (98.3%) | 323 (97.3%) | 0.263 |
| Indwelling drainage tube, n (%) | 1317 (99.2%) | 325 (97.9%) | 0.068 |
| Operative time, mean (SD), minutes | 304.28 (60.71) | 312.17 (63.11) | 0.036 |
| ASA | 0.083 | ||
| 1 | 205 (15.4%) | 48 (14.5%) | |
| 2 | 971 (73.1%) | 233 (70.2%) | |
| 3 | 145 (10.9%) | 51 (15.4%) | |
| 4 | 7 (0.5%) | 0 (0.0%) | |
| Clinical stages | 0.353 | ||
| 1 | 200 (15.0%) | 49 (14.8%) | |
| 2 | 454 (34.2%) | 108 (32.5%) | |
| 3 | 608 (45.8%) | 150 (45.2%) | |
| 4 | 66 (5.0%) | 25 (7.5%) | |
| AL | 25 (1.9%) | 11 (3.3%) | 0.087 |
| Predictions | True Label | |
|---|---|---|
| Cases with AL | Cases without AL | |
| LR | ||
| AL(+) | 10 | 74 |
| AL(−) | 1 | 247 |
| RF | ||
| AL(+) | 9 | 57 |
| AL(−) | 2 | 264 |
| SVM | ||
| AL(+) | 10 | 96 |
| AL(−) | 1 | 225 |
| XGBoost | ||
| AL(+) | 10 | 89 |
| AL(−) | 1 | 232 |
| RF | LR | SVM | XGBoost | p Valve (RF vs.) | |||
|---|---|---|---|---|---|---|---|
| LR | SVM | XGBoost | |||||
| Sensitivity (95% CI) | 0.818 (0.478–0.968) | 0.909 (0.572–0.995) | 0.909 (0.572–0.995) | 0.909 (0.572–0.995) | 0.534 | 0.534 | 0.534 |
| Specificity (95% CI) | 0.822 (0.775–0.862) | 0.770 (0.719–0.814) | 0.701 (0.647–0.750) | 0.723 (0.670–0.770) | 0.096 | <0.001 | 0.003 |
| PPV (95% CI) | 0.137 (0.068–0.248) | 0.119(0.062–0.212) | 0.094 (0.049–0.171) | 0.101 (0.052–0.182) | 0.752 | 0.392 | 0.486 |
| NPV (95% CI) | 0.992 (0.970–0.999) | 0.996 (0.974–1.000) | 0.996 (0.972–1.000) | 0.996 (0.973–1.000) | 0.978 | 0.981 | 0.98 |
| Accuracy (95% CI) | 0.822 (0.776–0.861) | 0.774(0.725–0.818) | 0.708 (0.656–0.756) | 0.729 (0.678–0.776) | 0.122 | <0.001 | 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shao, S.; Liu, L.; Zhao, Y.; Mu, L.; Lu, Q.; Qin, J. Application of Machine Learning for Predicting Anastomotic Leakage in Patients with Gastric Adenocarcinoma Who Received Total or Proximal Gastrectomy. J. Pers. Med. 2021, 11, 748. https://doi.org/10.3390/jpm11080748
Shao S, Liu L, Zhao Y, Mu L, Lu Q, Qin J. Application of Machine Learning for Predicting Anastomotic Leakage in Patients with Gastric Adenocarcinoma Who Received Total or Proximal Gastrectomy. Journal of Personalized Medicine. 2021; 11(8):748. https://doi.org/10.3390/jpm11080748
Chicago/Turabian StyleShao, Shengli, Lu Liu, Yufeng Zhao, Lei Mu, Qiyi Lu, and Jichao Qin. 2021. "Application of Machine Learning for Predicting Anastomotic Leakage in Patients with Gastric Adenocarcinoma Who Received Total or Proximal Gastrectomy" Journal of Personalized Medicine 11, no. 8: 748. https://doi.org/10.3390/jpm11080748
APA StyleShao, S., Liu, L., Zhao, Y., Mu, L., Lu, Q., & Qin, J. (2021). Application of Machine Learning for Predicting Anastomotic Leakage in Patients with Gastric Adenocarcinoma Who Received Total or Proximal Gastrectomy. Journal of Personalized Medicine, 11(8), 748. https://doi.org/10.3390/jpm11080748