
Telomere Length and Arterial Stiffness Reflected by Brachial–Ankle Pulse Wave Velocity: A Population-Based Cross-Sectional Study

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
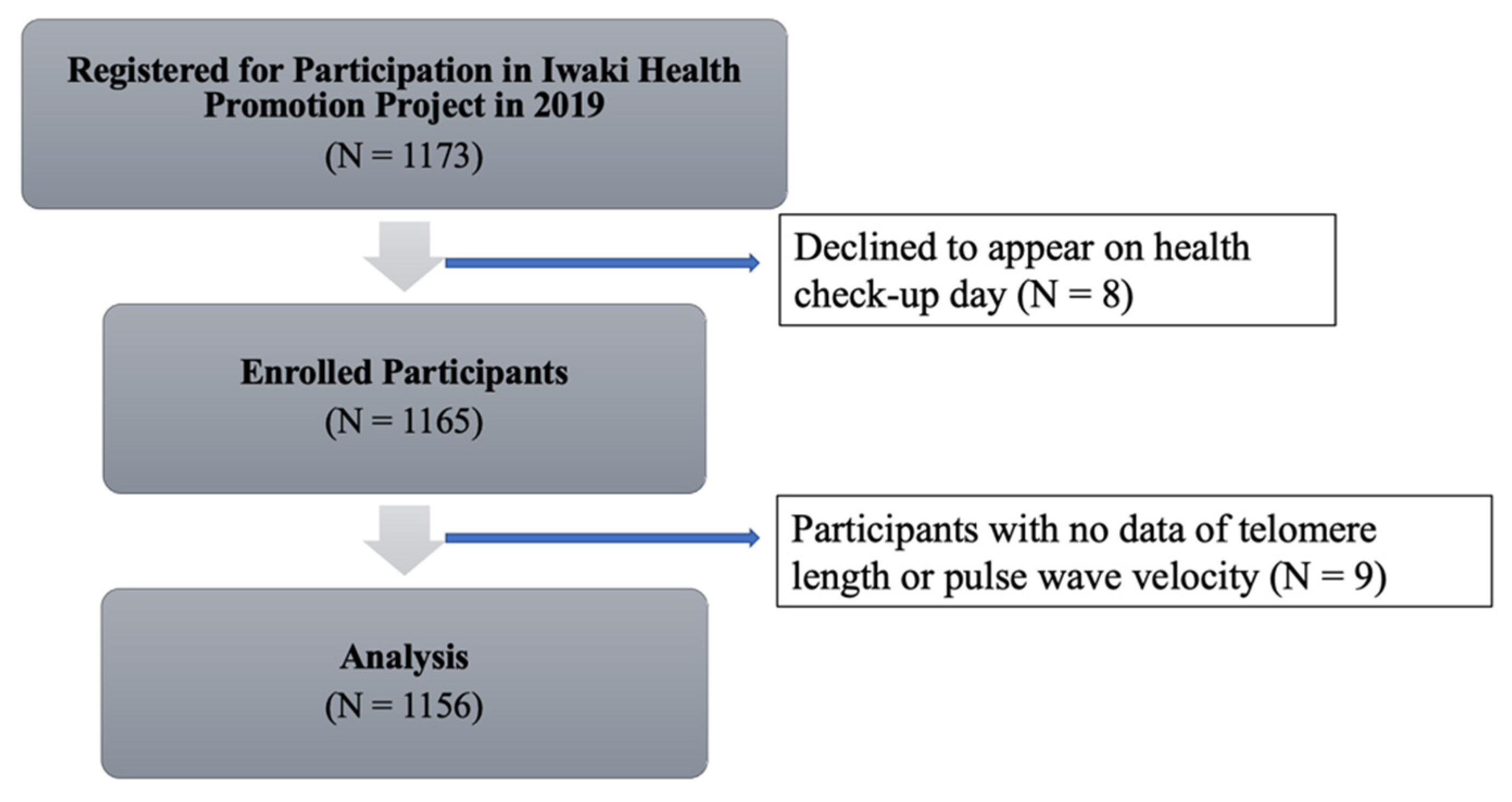
2.1. Study Design and Population
2.2. Body Anthropometry and Biochemical Measurements
2.3. Brachial–Ankle PWV Measurement
2.4. Telomere Length Measurement
2.5. Statistical Analysis
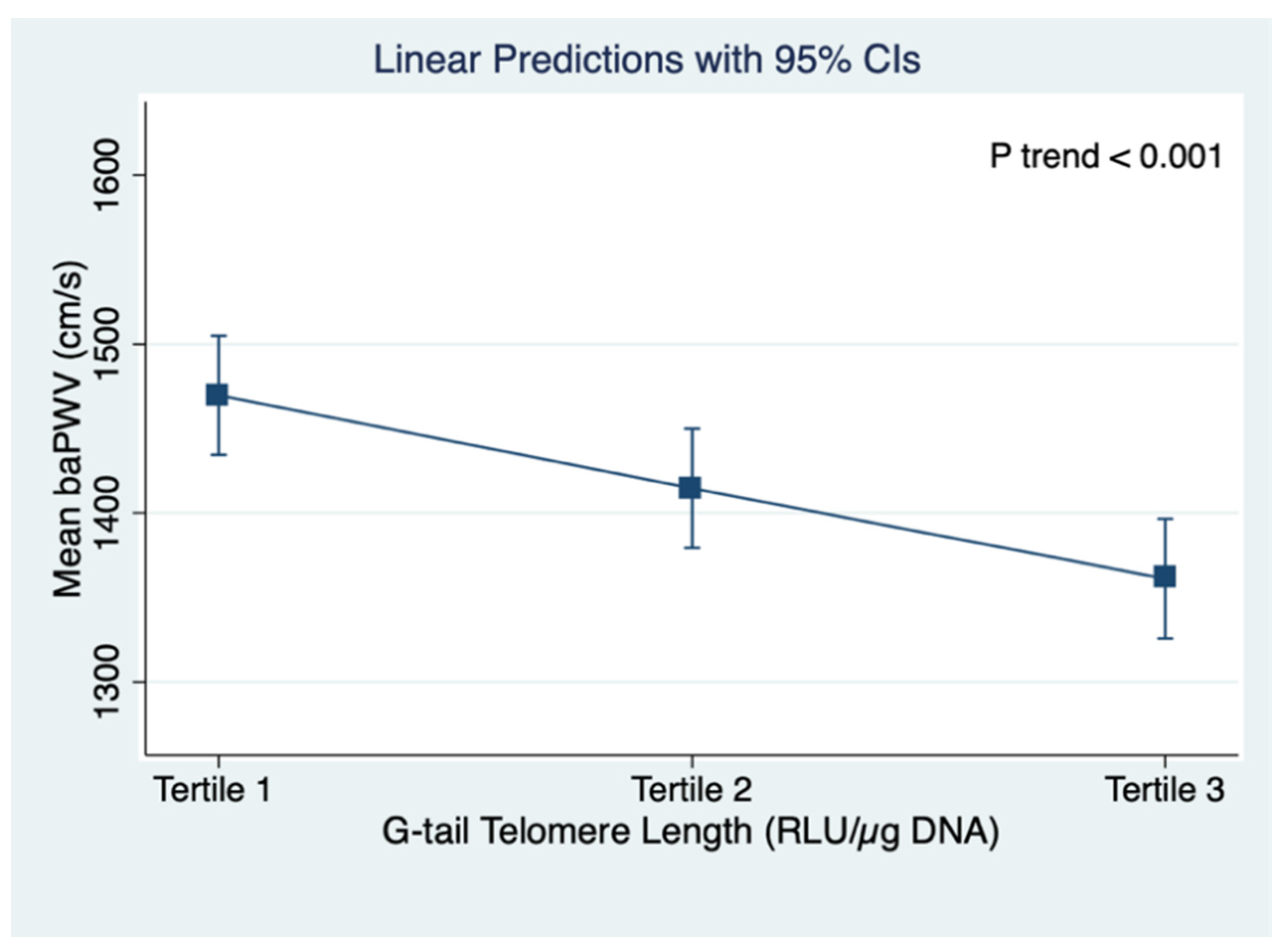
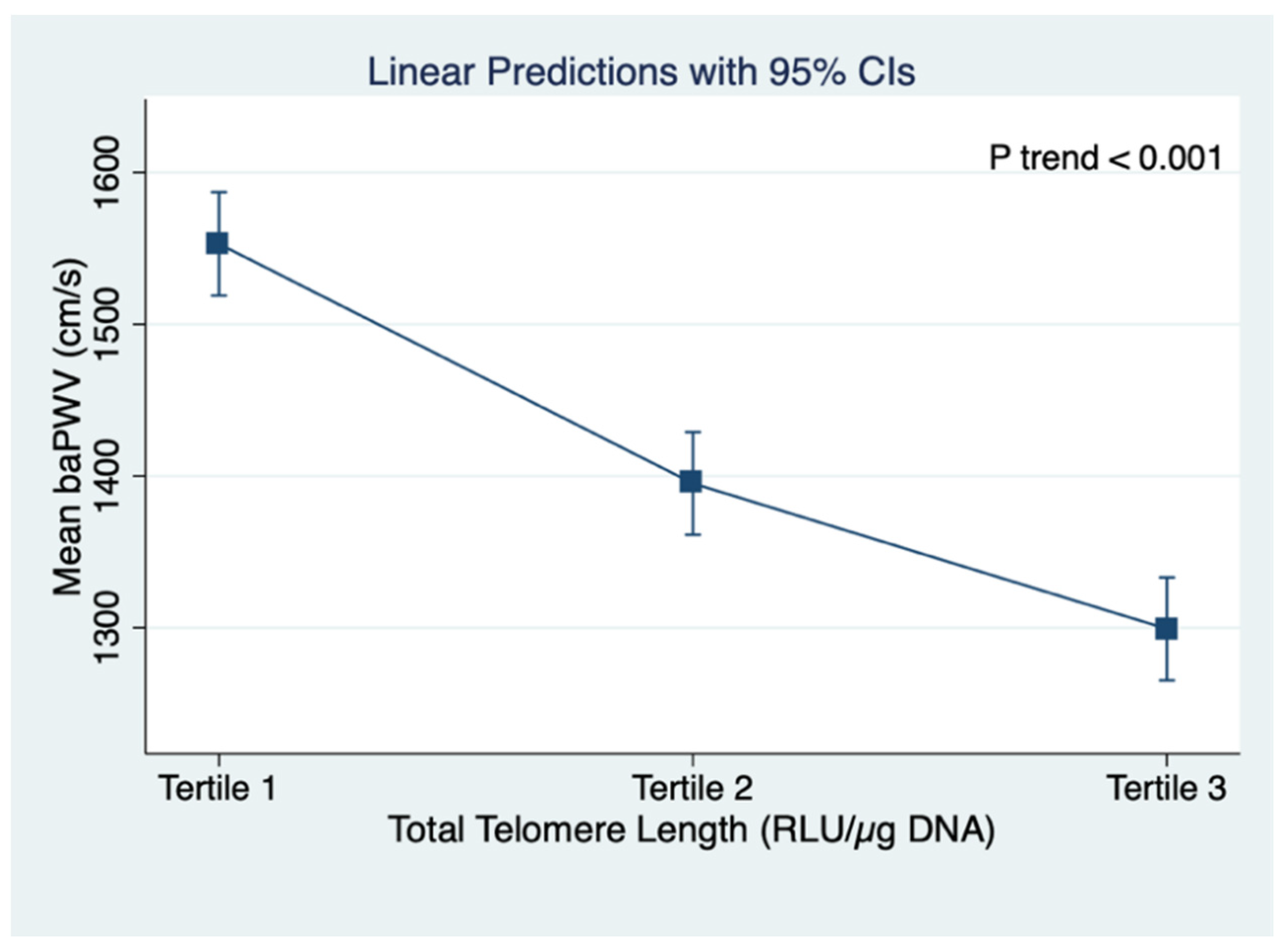
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blackburn, E.H. Structure and function of telomeres. Nature 1991, 350, 569–573. [Google Scholar] [CrossRef] [PubMed]
- de Lange, T. Shelterin: The protein complex that shapes and safeguards human telomeres. Genes Dev. 2005, 19, 2100–2110. [Google Scholar] [CrossRef] [PubMed]
- Murnane, J. Telomeres and chromosome instability. DNA Repair 2006, 5, 1082–1092. [Google Scholar] [CrossRef]
- Palm, W.; de Lange, T. How shelterin protects mammalian telomeres. Annu. Rev. Genet. 2008, 42, 301–334. [Google Scholar] [CrossRef]
- Stewart, S.A.; Ben-Porath, I.; Carey, V.J.; O’Connor, B.F.; Hahn, W.C.; Weinberg, R.A. Erosion of the telomeric single-strand overhang at replicative senescence. Nat. Genet. 2003, 33, 492–496. [Google Scholar] [CrossRef]
- Kovacic, J.C.; Moreno, P.; Nabel, E.G.; Hachinski, V.; Fuster, V. Cellular senescence, vascular disease, and aging: Part 1 of a 2-part review. Circulation 2011, 123, 1900–1910. [Google Scholar] [CrossRef] [PubMed]
- Cawthon, R.M.; Smith, K.R.; O’Brien, E.; Sivatchenko, A.; Kerber, R. Association between telomere length in blood and mortality in people aged 60 years or older. Lancet 2003, 361, 393–395. [Google Scholar] [CrossRef]
- Haycock, P.C.; Heydon, E.E.; Kaptoge, S.; Butterworth, A.S.; Thompson, A.; Willeit, P. Leucocyte telomere length and risk of cardiovascular disease: Systematic review and meta-analysis. BMJ 2014, 349, g4227. [Google Scholar] [CrossRef]
- von Zglinicki, T.; Serra, V.; Lorenz, M.; Saretzki, G.; Lenzen-Groβimlighaus, R.; Geβner, R.; Risch, A.; Steinhagen-Thiessen, E. Short telomeres in patients with vascular dementia: An indicator of low antioxidative capacity and a possible risk factor? Lab. Investig. 2000, 80, 1739–1747. [Google Scholar] [CrossRef]
- Rehkopf, D.H.; Needham, B.; Lin, J.; Blackburn, E.H.; Zota, A.; Wojcicki, J.M.; Epel, E.S. Leukocyte Telomere Length in Relation to 17 Biomarkers of Cardiovascular Disease Risk: A Cross-Sectional Study of US Adults. PLoS Med. 2016, 13, e1002188. [Google Scholar] [CrossRef]
- Fitzpatrick, A.L.; Kronmal, R.A.; Gardner, J.P.; Psaty, B.M.; Jenny, N.S.; Tracy, R.P.; Walston, J.; Kimura, M.; Alviv, A. Leukocyte telomere length and cardiovascular disease in the cardiovascular health study. Am. J. Epidemiol. 2007, 165, 14–21. [Google Scholar] [CrossRef]
- Houben, J.M.; Moonen, H.J.; van Schooten, F.J.; Hageman, G.J. Telomere length assessment: Biomarker of chronic oxidative stress? Free Radic. Biol. Med. 2008, 44, 235–246. [Google Scholar] [CrossRef] [PubMed]
- Amini, M.F.; Zayeri, Y.; Salehi, M. Trend analysis of cardiovascular disease mortality, incidence, and mortality-to-incidence ratio: Results from global burden of disease study 2017. BMC Public Health 2021, 21, 401. [Google Scholar] [CrossRef]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990-2019: Update From the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Tomiyama, H.; Matsumoto, C.; Shiina, K.; Yamashina, A. Brachial-Ankle PWV: Current Status and Future Directions as a Useful Marker in the Management of Cardiovascular Disease and/or Cardiovascular Risk Factors. J. Atheroscler. Thromb. 2016, 23, 128–146. [Google Scholar] [CrossRef] [PubMed]
- Yamashina, A.; Tomiyama, H.; Takeda, K.; Tsuda, H.; Alrai, T.; Hirose, K.; Koji, Y.; Hori, S.; Yamamoto, Y. Validity, reproducibility, and clinical significance of noninvasive brachial-ankle pulse wave velocity measurement. Hypertens. Res. 2002, 25, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Honkonen, M.; Vääräniemi, K.; Saijonmaa, O.; Nyman, A.; Tikkakoski, A.J.; Koskela, J.; Lehtimäki, T.; Kähönen, M.; Mustonen, J.; Fyhrquist, F.; et al. Leukocyte telomere length is inversely associated with arterial wave reflection in 566 normotensive and never-treated hypertensive subjects. Aging 2020, 12, 12376–12392. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.; Harley, C.B. Telomere length and replicative aging in human vascular tissues. Proc. Natl. Acad. Sci. USA 1995, 92, 11190–11194. [Google Scholar] [CrossRef] [PubMed]
- Benetos, A.; Okuda, K.; Lajemi, M.; Kimura, M.; Thomas, F.; Skurnick, J.; Labat, C.; Bean, K.; Aviv, A. Telomere length as an indicator of biological aging: The gender effect and relation with pulse pressure and pulse wave velocity. Hypertension 2001, 37, 381–385. [Google Scholar] [CrossRef]
- Hewitt, G.; Jurk, D.; Marques, F.M.; Correia-Melo, C.; Hardy, T.L.D.; Gackowska, A.; Anderson, R.; Taschuk, M.; Mann, J.; Passos, J.F. Telomeres are favoured targets of a persistent DNA damage response in ageing and stress-induced senescence. Nat. Commun. 2012, 3, 708. [Google Scholar] [CrossRef] [PubMed]
- Nakaji, S.; Ihara, K.; Sawada, K.; Parodi, S.; Umeda, T.; Talkahashi, I.; Murashita, K.; Kurauchi, S.; Tokuda, I. Social innovation for life expectancy extension utilizing a platform-centered system used in the Iwaki health promotion project: A protocol paper. SAGE Open Med. 2021, 9, 20503121211002606. [Google Scholar] [CrossRef] [PubMed]
- Tomiyama, H.; Shiina, K. State of the Art Review: Brachial-Ankle PWV. J. Atheroscler. Thromb. 2020, 27, 621–636. [Google Scholar] [CrossRef]
- Tahara, H.; Kusunoki, M.; Yamanaka, Y.; Matsumura, S.; Ide, T. G-tail telomere HPA: Simple measurement of human single-stranded telomeric overhangs. Nat. Methods 2005, 2, 829–831. [Google Scholar] [CrossRef]
- McDonnell, B.J.; Butcher, L.; Cockcroft, J.R.; Wilkinson, I.B.; Erusalimsky, J.D.; McEniery, C.M. The age-dependent association between aortic pulse wave velocity and telomere length. J. Physiol. 2017, 595, 1627–1635. [Google Scholar] [CrossRef] [PubMed]
- Raymond, A.R.; Norton, G.R.; Woodiwiss, A.J.; Brooksbank, R.L. Impact of gender and menopausal status on relationships between biological aging, as indexed by telomere length, and aortic stiffness. Am. J. Hypertens. 2015, 28, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Masi, S.; D’Aiuto, F.; Martin-Ruiz, C.; Khan, T.; Wong, A.; Ghosh, A.K.; Whincup, P.; Kuh, D.; Hughes, A.; von Zglinicki, T.; et al. Rate of telomere shortening and cardiovascular damage: A longitudinal study in the 1946 British Birth Cohort. Eur. Heart J. 2014, 35, 3296–3303. [Google Scholar] [CrossRef] [PubMed]
- Murillo-Ortiíz, B.; Albarrán-Tamayo, F.; Arenas-Aranda, D.; Benitez-Bribiesca, L.; Malacara-Hernández, J.; Martínez-Garza, S.; Hernández-González, M.; Solorio, S.; Garay-Sevilla, M.; Mora-Villalpando, C. Telomere length and type 2 diabetes in males, a premature aging syndrome. Aging Male 2012, 15, 54–58. [Google Scholar] [CrossRef]
- Hirashio, S.; Nakashima, A.; Doi, S.; Anno, K.; Aoki, E.; Shimamoto, A.; Yorioka, N.; Kohno, N.; Masaki, T.; Tahara, H. Telomeric g-tail length and hospitalization for cardiovascular events in hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2014, 9, 2117–2122. [Google Scholar] [CrossRef]
- Koi, Y.; Tsutani, Y.; Nishiyama, Y.; Kanda, M.; Shiroma, Y.; Yamamoto, Y.; Sasada, S.; Akita, T.; Masumoto, N.; Kadoya, T.; et al. Diagnostic performance of peripheral leukocyte telomere G-tail length for detecting breast cancer. Cancer Sci. 2020, 111, 1856–1861. [Google Scholar] [CrossRef]
- Nezu, T.; Hosomi, N.; Takahashi, T.; Alnno, K.; Aoki, S.; Shimamoto, A.; Maruyama, H.; Hayashi, T.; Matsumoto, M.; Tahara, H. Telomere G-tail Length is a Promising Biomarker Related to White Matter Lesions and Endothelial Dysfunction in Patients with Cardiovascular Risk: A Cross-sectional Study. EBioMedicine 2015, 2, 960–967. [Google Scholar] [CrossRef]
- Nakashima, H.; Ozono, R.; Suyama, C.; Sueda, T.; Kalmbe, M.; Oshima, T. Telomere attrition in white blood cell correlating with cardiovascular damage. Hypertens. Res. 2004, 27, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Thorin-Trescases, N.; Voghel, G.; Gendron, M.E.; Krummen, S.; Farhat, N.; Drouin, A.; Perrault, L.P.; Thorin, E. Pathological aging of the vascular endothelium: Are endothelial progenitor cells the sentinels of the cardiovascular system? Can. J. Cardiol. 2005, 21, 1019–1024. [Google Scholar] [PubMed]
- Rauscher, F.M.; Goldschmidt-Clermont, P.J.; Davis, B.H.; Wang, T.; Gregg, D.; Ramaswami, P.; Pippen, A.M.; Annex, B.H.; Dong, C.; Taylor, D.A. Aging, progenitor cell exhaustion, and atherosclerosis. Circulation 2003, 108, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Greenwald, S.E. Ageing of the conduit arteries. J. Pathol. 2007, 211, 157–172. [Google Scholar] [CrossRef]
- Vlachopoulos, C.; Aznaouridis, K.; Terentes-Printzios, D.; Ioakeimidis, N.; Stefanadis, C. Prediction of cardiovascular events and all-cause mortality with brachial-ankle elasticity index: A systematic review and meta-analysis. Hypertension 2012, 60, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Sugawara, J.; Hayashi, K.; Yokoi, T.; Cortez-Cooper, M.Y.; DeVan, A.E.; Anton, M.A.; Tanaka, H. Brachial-ankle pulse wave velocity: An index of central arterial stiffness? J. Hum. Hypertens. 2005, 19, 401–406. [Google Scholar] [CrossRef]
- Takashima, N.; Turin, T.; Matsui, K.; Rumana, N.; Nakamura, Y.; Kadota, A.; Saito, Y.; Sugihara, H.; Morita, Y.; Ichikawa, M.; et al. The relationship of brachial-ankle pulse wave velocity to future cardiovascular disease events in the general Japanese population: The Takashima Study. J. Hum. Hypertens. 2014, 28, 323–327. [Google Scholar] [CrossRef]
- Munakata, M.; Nunokawa, T.; Yoshinalga, K.; Toyota, T. Brachial-ankle pulse wave velocity is an independent risk factor for microalbuminuria in patients with essential hypertension--a Japanese trial on the prognostic implication of pulse wave velocity (J-TOPP). Hypertens. Res. 2006, 29, 515–521. [Google Scholar] [CrossRef][Green Version]
- Lin, W.Y.; Lai, M.-M.; Li, C.-I.; Lin, C.-C.; Li, T.-C.; Chen, C.-C.; Lin, T.; Liu, C.-S. In addition to insulin resistance and obesity, brachial-ankle pulse wave velocity is strongly associated with metabolic syndrome in Chinese—A population-based study (Taichung Community Health Study, TCHS). J. Atheroscler. Thromb. 2009, 16, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Hung, C.S.; Lin, J.-W.; Hsu, C.-N.; Chen, H.-M.; Tsai, R.-Y.; Chien, Y.-F.; Hwalng, J.-J. Using brachial-ankle pulse wave velocity to associate arterial stiffness with cardiovascular risks. Nutr. Metab. Cardiovasc. Dis. 2009, 19, 241–246. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Mean ± SD | n (%) |
|---|---|---|
| General Characteristics | ||
| Age (years) | 52.7 ± 15.2 | |
| Sex | ||
| Male | 435 (40.9) | |
| Female | 630 (59.1) | |
| Smoking status | ||
| Non-smokers | 673 (63.8) | |
| Current smokers | 182 (17.2) | |
| Past smokers | 200 (19.0) | |
| Alcohol drinking status | ||
| Non-drinkers | 504 (47.9) | |
| Current drinkers | 504 (48.0) | |
| Past drinkers | 43 (4.1) | |
| Body mass index (kg/m2) ‡ | 23.0 ± 3.6 | |
| Underweight | 82 (7.7) | |
| Normal | 700 (65.7) | |
| Overweight | 230 (21.6) | |
| Obese | 53 (4.9) | |
| Systolic blood pressure (mmHg) | 120.8 ± 16.9 | |
| Diastolic blood pressure (mmHg) | 76.8 ± 11.3 | |
| Diabetes, yes | 43 (4.0) | |
| Hypertension, yes | 202 (18.9) | |
| Right baPWV (cm/s) | 1411.2 ± 343.3 | |
| Left baPWV (cm/s) | 1419.3 ± 341.0 | |
| Mean PWV (cm/s) | 1415.2 ± 340.5 | |
| Laboratory Findings | ||
| Blood sugar (mg/dL) | 96.1 ± 16.3 | |
| Triglyceride (mg/dL) † | 77 (55–114) | |
| LDL Cholesterol (mg/dL) | 116.1 ± 29.8 | |
| HDL Cholesterol (mg/dL) | 65.0 ± 16.6 | |
| HbA1c (%) | 76.8 ± 11.3 | |
| C-reactive protein (mg/dL) † | 0.03 (0.02–0.08) | |
| Telomere G-tail length (RLU/µg DNA) | 31,664.2 ± 4744.3 | |
| Total telomere length (RLU/µg DNA) | 356,478.1 ± 50,678.3 |
| Variables | Right baPWV (cm/s) | Left baPWV (cm/s) | Mean baPWV (cm/s) |
|---|---|---|---|
| Right baPWV (cm/s) | 1 | ||
| Left baPWV (cm/s) | 0.981 * | 1 | |
| Mean baPWV (cm/s) | 0.995 * | 0.995 * | 1 |
| Variables | Telomere G Tail Length (RLU/µg DNA) a | p-Value † | Total Telomere Length (RLU/µg DNA) b | p-Value † | ||||
|---|---|---|---|---|---|---|---|---|
| Tertile 1 Mean ± SD | Tertile 2 Mean ± SD | Tertile 3 Mean ± SD | Tertile 1 Mean ± SD | Tertile 2 Mean ± SD | Tertile 3 Mean ± SD | |||
| Age (years) | 56.9 ± 14.9 | 52.7 ± 15.2 | 48.3 ± 14.5 | <0.001 | 59.7 ± 13.7 | 52.8 ± 14.8 | 45.5 ± 13.8 | <0.001 |
| Sex, male ‡ | 140 (13.2) | 144 (13.5) | 151 (14.2) | 0.676 | 168 (15.8) | 138 (12.9) | 129 (12.1) | 0.008 |
| Body mass index (kg/m2) | 23.0 ± 3.5 | 23.1 ± 3.6 | 22.8 ± 3.7 | 0.587 | 23.5 ± 3.6 | 23.0 ± 3.6 | 22.4 ± 3.6 | <0.001 |
| Systolic blood pressure (mmHg) | 122.5 ± 16.5 | 121.1 ± 17.1 | 118.8 ± 17.0 | 0.015 | 123.5 ± 17.0 | 121.9 ± 17.4 | 116.9 ± 15.7 | <0.001 |
| Diastolic blood pressure (mmHg) | 77.2 ± 10.6 | 76.8 ± 10.7 | 76.6 ± 12.6 | 0.771 | 77.9 ± 10.9 | 77.0 ± 11.8 | 75.6 ± 11.2 | 0.021 |
| Hypertension, yes ‡ | 74 (0.9) | 66 (6.2) | 62 (5.8) | 0.514 | 81 (7.6) | 74 (6.9) | 47 (4.4) | 0.003 |
| Right baPWV (cm/s) | 1467.6 ± 347.8 | 1408.8 ± 334.6 | 1356.8 ± 339.2 | <0.001 | 1547.4 ± 380.6 | 1390.5 ± 308.2 | 1297.1 ± 287.7 | <0.001 |
| Left baPWV (cm/s) | 1471.7 ± 344.0 | 1420.4 ± 335.4 | 1365.5 ± 336.2 | <0.001 | 1558.5 ± 374.5 | 1399.7 ± 306.8 | 1301.3 ± 286.2 | <0.001 |
| Mean baPWV (cm/s) | 1469.6 ± 343.9 | 1414.6 ± 333.3 | 1361.1 ± 336.3 | <0.001 | 1552.9 ± 375.3 | 1395.1 ± 306.1 | 1299.2 ± 285.4 | <0.001 |
| Blood sugar (mg/dL) | 96.7 ± 15.7 | 96.4 ± 16.6 | 95.0 ± 16.6 | 0.348 | 100.4 ± 20.1 | 95.3 ± 15.1 | 92.4 ± 11.4 | <0.001 |
| Triglyceride (mg/dL) § | 95.9 ± 99.1 | 103.6 ± 90.9 | 93.1 ± 58.5 | 0.233 | 108.8 ± 101.5 | 95.9 ± 78.1 | 88.0 ± 70.2 | 0.004 |
| LDL Cholesterol (mg/dL) | 116.1 ± 29.2 | 115.5 ± 29.5 | 116.8 ± 30.7 | 0.840 | 120.0 ± 28.6 | 116.3 ± 31.6 | 112.0 ± 28.6 | 0.002 |
| HDL Cholesterol (mg/dL) | 65.9 ± 16.6 | 64.1 ± 16.7 | 65.0 ± 16.5 | 0.357 | 63.7 ± 16.3 | 64.9 ± 16.1 | 66.4 ± 17.2 | 0.081 |
| HbA1c (%) | 5.8 ± 0.7 | 5.7 ± 0.5 | 5.7 ± 0.6 | 0.092 | 5.9 ± 0.7 | 5.7 ± 0.6 | 5.6 ± 0.5 | <0.001 |
| C-reactive protein (mg/dL) § | 0.1 ± 0.4 | 0.1 ± 0.3 | 0.2 ± 0.6 | 0.305 | 0.1 ± 0.4 | 0.1 ± 0.6 | 0.1 ± 0.3 | 0.411 |
| Variables | TL G-Tail and Mean baPWV | Total TL and Mean baPWV |
|---|---|---|
| Adjusted Beta (95% CI) | Adjusted Beta (95% CI) | |
| Telomere G-tail length (RLU/µg DNA) | ||
| Tertile 1 (11,854.32~29,611.05) | ref | |
| Tertile 2 (29,611.05~33,409.38) | −3.55 (−36.58, 29.48) | |
| Tertile 3 (33,409.38~53,575.06) | 1.88 (−31.99. 35.75) | |
| Total telomere length (RLU/µg DNA) | ||
| Tertile 1 (103,771.35~334,193.49) | ref | |
| Tertile 2 (334,193.49~376,734.07) | −52.44 (−86.06, −18.83) ** | |
| Tertile 3 (376,734.07~596,420.43) | −41.24 (−76.81, −5.68) * | |
| Age | ||
| ≤40 years | ref | ref |
| 40–60 years | 125.59 (90.43, 160.76) *** | 119.32 (83.92, 154.71) *** |
| ≥60 years | 455.01 (418.36, 491.67) *** | 441.47 (403.74, 479.20) *** |
| Sex (ref: male) | −93.58 (−125.58, −61.54) *** | −92.27 (−124.13, −60.40) *** |
| Smoking (ref: non-smokers vs. current smokers) | 17.64 (−19.98, 55.27) | 13.31 (−24.21, 50.83) |
| Alcohol drinking (ref: non-drinkers vs. current drinkers) | 4.44 (−25.65, 34.54) | 2.62 (−27.58, 32.84) |
| Hypertension (ref: no) | 193.43 (156.97, 229.91) *** | 195.62 (159.30, 231.93) *** |
| Triglyceride (mg/dL) | 0.19 (0.02, 0.36) * | 0.17 (0.01, 0.34) * |
| Blood sugar (mg/dL) | 3.54 (2.59, 4.47) *** | 3.40 (2.47, 4.34) *** |
| Body mass index (kg/m2) | −4.62 (−8.77, −0.47) * | −4.67 (−8.81, −0.54) * |
| C-reactive protein (mg/dL) | 56.95 (28.03, 85.87) *** | 57.62 (28.87, 86.36) *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wai, K.M.; Kaori, S.; Itoh, K.; Shinya, O.; Uchikawa, Y.; Hayashi, S.; Shiraki, A.; Murashita, K.; Nakaji, S.; Ihara, K. Telomere Length and Arterial Stiffness Reflected by Brachial–Ankle Pulse Wave Velocity: A Population-Based Cross-Sectional Study. J. Pers. Med. 2021, 11, 1278. https://doi.org/10.3390/jpm11121278
Wai KM, Kaori S, Itoh K, Shinya O, Uchikawa Y, Hayashi S, Shiraki A, Murashita K, Nakaji S, Ihara K. Telomere Length and Arterial Stiffness Reflected by Brachial–Ankle Pulse Wave Velocity: A Population-Based Cross-Sectional Study. Journal of Personalized Medicine. 2021; 11(12):1278. https://doi.org/10.3390/jpm11121278
Chicago/Turabian StyleWai, Kyi Mar, Sawada Kaori, Ken Itoh, Okuyama Shinya, Yuka Uchikawa, Sakura Hayashi, Akiko Shiraki, Koichi Murashita, Shigeyuki Nakaji, and Kazushige Ihara. 2021. "Telomere Length and Arterial Stiffness Reflected by Brachial–Ankle Pulse Wave Velocity: A Population-Based Cross-Sectional Study" Journal of Personalized Medicine 11, no. 12: 1278. https://doi.org/10.3390/jpm11121278
APA StyleWai, K. M., Kaori, S., Itoh, K., Shinya, O., Uchikawa, Y., Hayashi, S., Shiraki, A., Murashita, K., Nakaji, S., & Ihara, K. (2021). Telomere Length and Arterial Stiffness Reflected by Brachial–Ankle Pulse Wave Velocity: A Population-Based Cross-Sectional Study. Journal of Personalized Medicine, 11(12), 1278. https://doi.org/10.3390/jpm11121278