
Semi-Quantitative Multiplex Profiling of the Complement System Identifies Associations of Complement Proteins with Genetic Variants and Metabolites in Age-Related Macular Degeneration

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Results
2.1. Complement Peptide Levels Are Associated with Age, Sex, and BMI
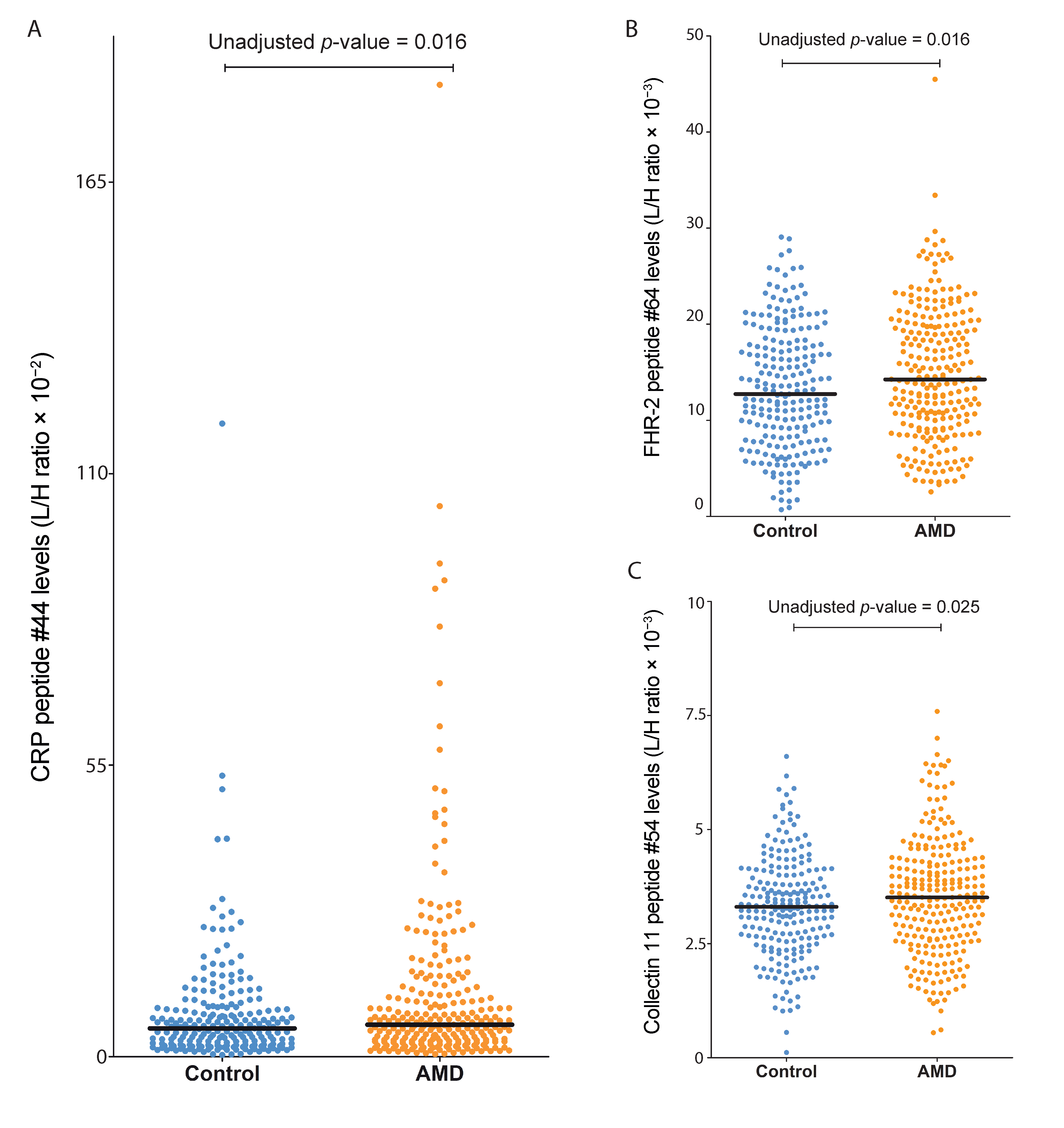
2.2. Association Analysis of Complement Peptide Levels with AMD
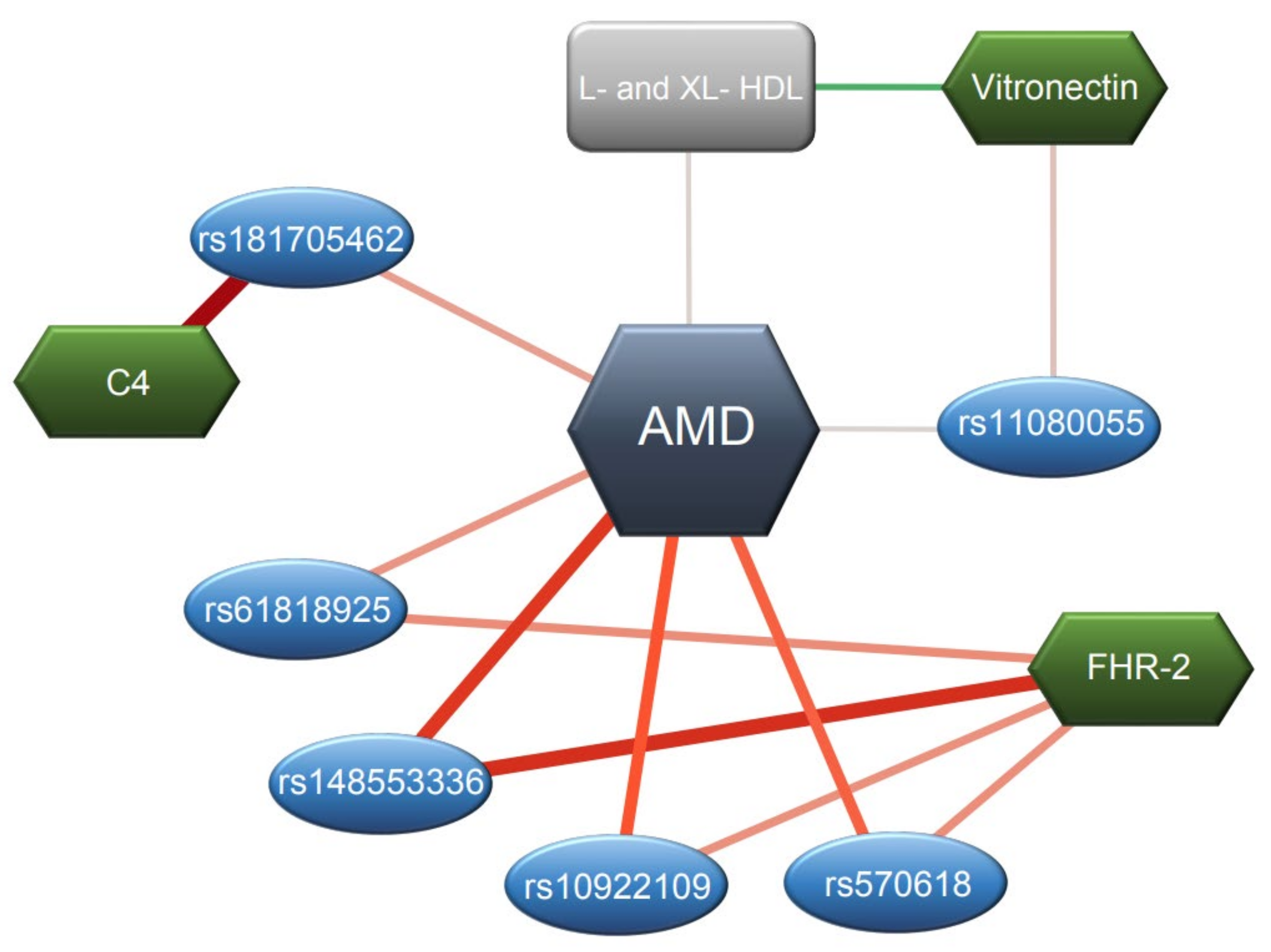
2.3. Complement Peptide Levels Are Associated with AMD Variants
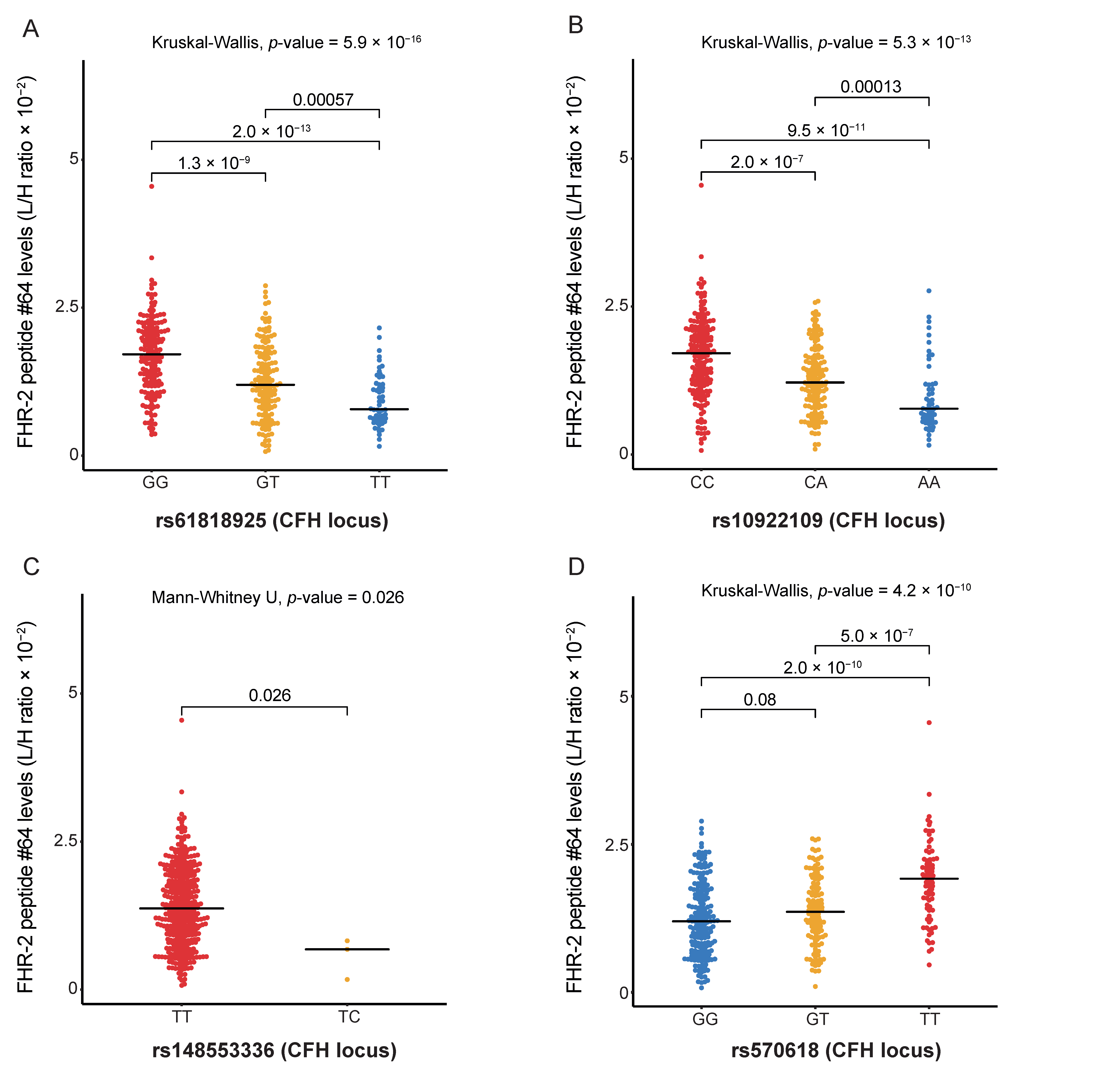
2.3.1. FHR-2 Peptide Levels Are Associated with AMD Variants at the CFH Locus
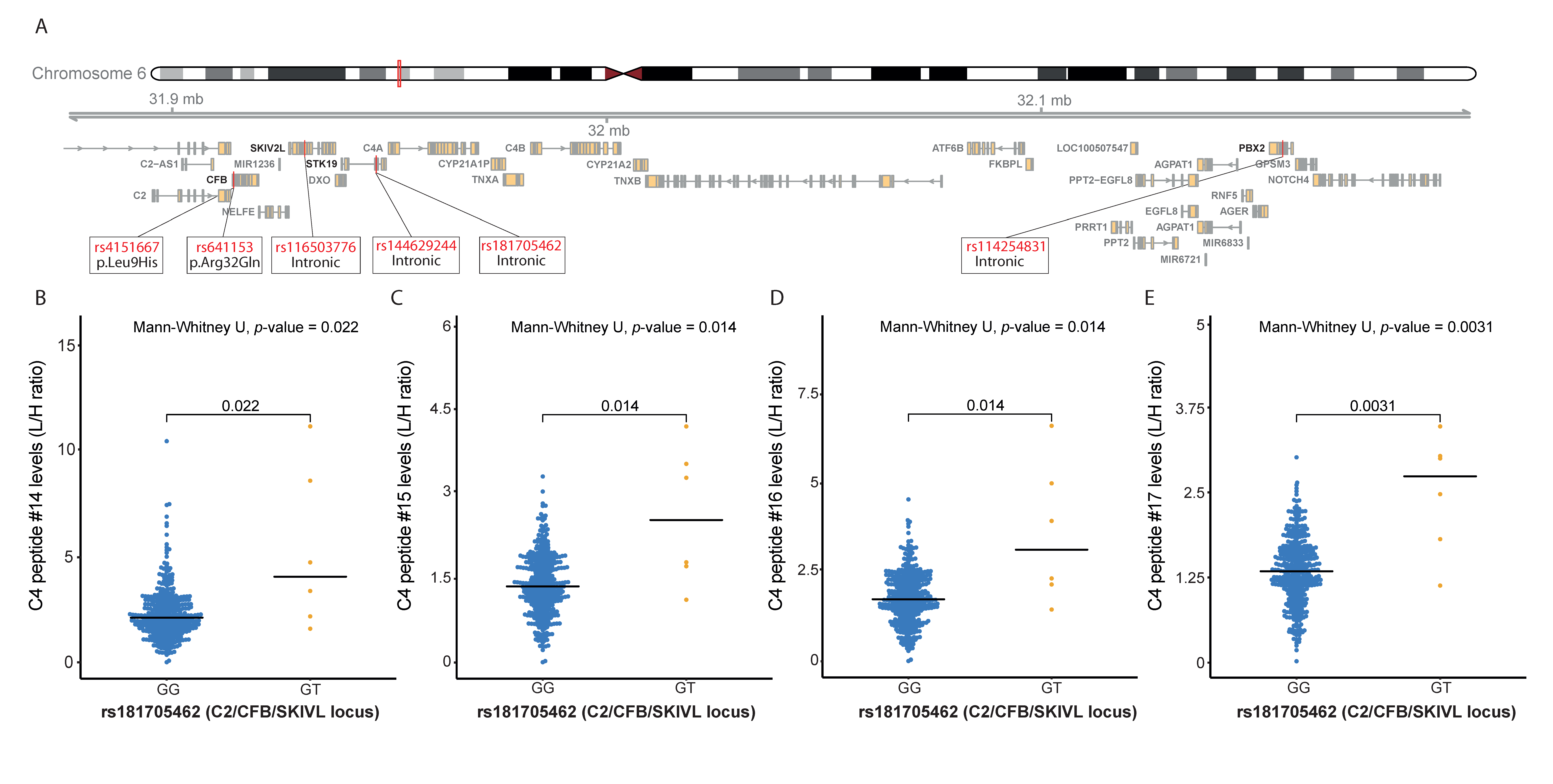
2.3.2. C4 Peptide Levels Are Associated with AMD Variants at the C2/CFB/SKIV2L Locus
2.3.3. VTN Peptide Levels Are Associated with AMD Variants at the TMEM97/VTN Locus
2.3.4. FI Peptide Levels Are Associated with AMD Variants at the CFI Locus
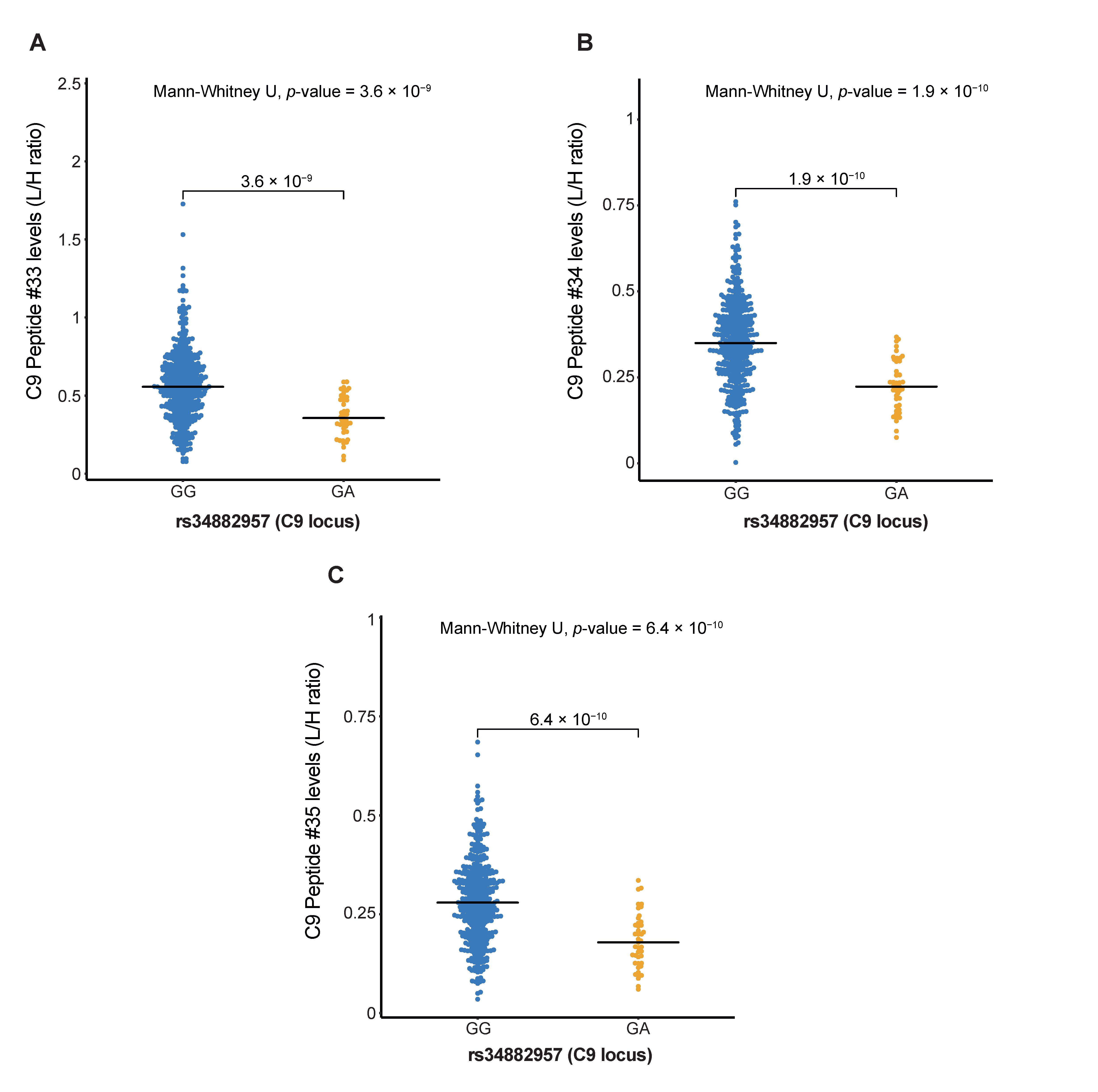
2.3.5. C9 Peptide Levels Are Associated with AMD Variants at the C9 Locus
2.3.6. Association Analysis of C3 Peptide Levels with AMD Variants at the C3 Locus
2.3.7. Association Analysis of Complement Peptide Levels with AMD-Associated Genetic Variants at Other Loci
2.4. Complement Peptides Are Associated with Lipoproteins and Other AMD Metabolites
3. Discussion
4. Materials and Methods
4.1. The Study Samples
4.2. Genotyping
4.3. Metabolomic Analysis
4.4. Complement Targeted Multiplex Assay
4.5. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wong, W.L.; Su, X.; Li, X.; Cheung, C.M.; Klein, R.; Cheng, C.Y.; Wong, T.Y. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: A systematic review and meta-analysis. Lancet Glob. Health 2014, 2, e106–e116. [Google Scholar] [CrossRef] [Green Version]
- Rudnicka, A.R.; Jarrar, Z.; Wormald, R.; Cook, D.G.; Fletcher, A.; Owen, C.G. Age and gender variations in age-related macular degeneration prevalence in populations of European ancestry: A meta-analysis. Ophthalmology 2012, 119, 571–580. [Google Scholar] [CrossRef] [PubMed]
- Coleman, A.L.; Seitzman, R.L.; Cummings, S.R.; Yu, F.; Cauley, J.A.; Ensrud, K.E.; Stone, K.L.; Hochberg, M.C.; Pedula, K.L.; Thomas, E.L.; et al. The association of smoking and alcohol use with age-related macular degeneration in the oldest old: The Study of Osteoporotic Fractures. Am. J. Ophthalmol. 2010, 149, 160–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Q.Y.; Tie, L.J.; Wu, S.S.; Lv, P.L.; Huang, H.W.; Wang, W.Q.; Wang, H.; Ma, L. Overweight, Obesity, and Risk of Age-Related Macular Degeneration. Investig. Ophthalmol. Vis. Sci. 2016, 57, 1276–1283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, W.; Assink, J.; Klein, R.; Mitchell, P.; Klaver, C.C.; Klein, B.E.; Hofman, A.; Jensen, S.; Wang, J.J.; de Jong, P.T. Risk factors for age-related macular degeneration: Pooled findings from three continents. Ophthalmology 2001, 108, 697–704. [Google Scholar] [CrossRef]
- Fritsche, L.G.; Igl, W.; Bailey, J.N.; Grassmann, F.; Sengupta, S.; Bragg-Gresham, J.L.; Burdon, K.P.; Hebbring, S.J.; Wen, C.; Gorski, M.; et al. A large genome-wide association study of age-related macular degeneration highlights contributions of rare and common variants. Nat. Genet. 2016, 48, 134–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, A.O.; Ritter, R., 3rd; Abel, K.J.; Manning, A.; Panhuysen, C.; Farrer, L.A. Complement factor H polymorphism and age-related macular degeneration. Science 2005, 308, 421–424. [Google Scholar] [CrossRef] [Green Version]
- Hageman, G.S.; Anderson, D.H.; Johnson, L.V.; Hancox, L.S.; Taiber, A.J.; Hardisty, L.I.; Hageman, J.L.; Stockman, H.A.; Borchardt, J.D.; Gehrs, K.M.; et al. A common haplotype in the complement regulatory gene factor H (HF1/CFH) predisposes individuals to age-related macular degeneration. Proc. Natl. Acad. Sci. USA 2005, 102, 7227–7232. [Google Scholar] [CrossRef] [Green Version]
- Haines, J.L.; Hauser, M.A.; Schmidt, S.; Scott, W.K.; Olson, L.M.; Gallins, P.; Spencer, K.L.; Kwan, S.Y.; Noureddine, M.; Gilbert, J.R.; et al. Complement factor H variant increases the risk of age-related macular degeneration. Science 2005, 308, 419–421. [Google Scholar] [CrossRef] [Green Version]
- Klein, R.J.; Zeiss, C.; Chew, E.Y.; Tsai, J.Y.; Sackler, R.S.; Haynes, C.; Henning, A.K.; SanGiovanni, J.P.; Mane, S.M.; Mayne, S.T.; et al. Complement factor H polymorphism in age-related macular degeneration. Science 2005, 308, 385–389. [Google Scholar] [CrossRef]
- Dewan, A.; Liu, M.; Hartman, S.; Zhang, S.S.; Liu, D.T.; Zhao, C.; Tam, P.O.; Chan, W.M.; Lam, D.S.; Snyder, M.; et al. HTRA1 promoter polymorphism in wet age-related macular degeneration. Science 2006, 314, 989–992. [Google Scholar] [CrossRef]
- Rivera, A.; Fisher, S.A.; Fritsche, L.G.; Keilhauer, C.N.; Lichtner, P.; Meitinger, T.; Weber, B.H. Hypothetical LOC387715 is a second major susceptibility gene for age-related macular degeneration, contributing independently of complement factor H to disease risk. Hum. Mol. Genet. 2005, 14, 3227–3236. [Google Scholar] [CrossRef] [Green Version]
- Yang, Z.; Camp, N.J.; Sun, H.; Tong, Z.; Gibbs, D.; Cameron, D.J.; Chen, H.; Zhao, Y.; Pearson, E.; Li, X.; et al. A variant of the HTRA1 gene increases susceptibility to age-related macular degeneration. Science 2006, 314, 992–993. [Google Scholar] [CrossRef]
- Gold, B.; Merriam, J.E.; Zernant, J.; Hancox, L.S.; Taiber, A.J.; Gehrs, K.; Cramer, K.; Neel, J.; Bergeron, J.; Barile, G.R.; et al. Variation in factor B (BF) and complement component 2 (C2) genes is associated with age-related macular degeneration. Nat. Genet. 2006, 38, 458–462. [Google Scholar] [CrossRef] [Green Version]
- Yates, J.R.; Sepp, T.; Matharu, B.K.; Khan, J.C.; Thurlby, D.A.; Shahid, H.; Clayton, D.G.; Hayward, C.; Morgan, J.; Wright, A.F.; et al. Complement C3 variant and the risk of age-related macular degeneration. N. Engl. J. Med. 2007, 357, 553–561. [Google Scholar] [CrossRef] [Green Version]
- Seddon, J.M.; Yu, Y.; Miller, E.C.; Reynolds, R.; Tan, P.L.; Gowrisankar, S.; Goldstein, J.I.; Triebwasser, M.; Anderson, H.E.; Zerbib, J.; et al. Rare variants in CFI, C3 and C9 are associated with high risk of advanced age-related macular degeneration. Nat. Genet. 2013, 45, 1366–1370. [Google Scholar] [CrossRef] [Green Version]
- Triebwasser, M.P.; Roberson, E.D.; Yu, Y.; Schramm, E.C.; Wagner, E.K.; Raychaudhuri, S.; Seddon, J.M.; Atkinson, J.P. Rare Variants in the Functional Domains of Complement Factor H Are Associated With Age-Related Macular Degeneration. Investig. Ophthalmol. Vis. Sci. 2015, 56, 6873–6878. [Google Scholar] [CrossRef] [Green Version]
- Geerlings, M.J.; de Jong, E.K.; den Hollander, A.I. The complement system in age-related macular degeneration: A review of rare genetic variants and implications for personalized treatment. Mol. Immunol. 2017, 84, 65–76. [Google Scholar] [CrossRef]
- de Breuk, A.; Acar, I.E.; Kersten, E.; Schijvenaars, M.; Colijn, J.M.; Haer-Wigman, L.; Bakker, B.; de Jong, S.; Meester-Smoor, M.A.; Verzijden, T.; et al. Development of a Genotype Assay for Age-Related Macular Degeneration: The EYE-RISK Consortium. Ophthalmology 2021, 128, 1604–1617. [Google Scholar] [CrossRef]
- Van der Schaft, T.L.; Mooy, C.M.; de Bruijn, W.C.; de Jong, P.T. Early stages of age-related macular degeneration: An immunofluorescence and electron microscopy study. Br. J. Ophthalmol. 1993, 77, 657–661. [Google Scholar] [CrossRef] [Green Version]
- Johnson, L.V.; Ozaki, S.; Staples, M.K.; Erickson, P.A.; Anderson, D.H. A potential role for immune complex pathogenesis in drusen formation. Exp. Eye Res. 2000, 70, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Mullins, R.F.; Russell, S.R.; Anderson, D.H.; Hageman, G.S. Drusen associated with aging and age-related macular degeneration contain proteins common to extracellular deposits associated with atherosclerosis, elastosis, amyloidosis, and dense deposit disease. FASEB J. 2000, 14, 835–846. [Google Scholar] [CrossRef] [PubMed]
- Scholl, H.P.; Charbel Issa, P.; Walier, M.; Janzer, S.; Pollok-Kopp, B.; Borncke, F.; Fritsche, L.G.; Chong, N.V.; Fimmers, R.; Wienker, T.; et al. Systemic complement activation in age-related macular degeneration. PLoS ONE 2008, 3, e2593. [Google Scholar] [CrossRef]
- Reynolds, R.; Hartnett, M.E.; Atkinson, J.P.; Giclas, P.C.; Rosner, B.; Seddon, J.M. Plasma complement components and activation fragments: Associations with age-related macular degeneration genotypes and phenotypes. Investig. Ophthalmol. Vis. Sci. 2009, 50, 5818–5827. [Google Scholar] [CrossRef]
- Smailhodzic, D.; Klaver, C.C.; Klevering, B.J.; Boon, C.J.; Groenewoud, J.M.; Kirchhof, B.; Daha, M.R.; den Hollander, A.I.; Hoyng, C.B. Risk alleles in CFH and ARMS2 are independently associated with systemic complement activation in age-related macular degeneration. Ophthalmology 2012, 119, 339–346. [Google Scholar] [CrossRef]
- Hecker, L.A.; Edwards, A.O.; Ryu, E.; Tosakulwong, N.; Baratz, K.H.; Brown, W.L.; Charbel Issa, P.; Scholl, H.P.; Pollok-Kopp, B.; Schmid-Kubista, K.E.; et al. Genetic control of the alternative pathway of complement in humans and age-related macular degeneration. Hum. Mol. Genet. 2010, 19, 209–215. [Google Scholar] [CrossRef] [Green Version]
- Van de Ven, J.P.; Nilsson, S.C.; Tan, P.L.; Buitendijk, G.H.; Ristau, T.; Mohlin, F.C.; Nabuurs, S.B.; Schoenmaker-Koller, F.E.; Smailhodzic, D.; Campochiaro, P.A.; et al. A functional variant in the CFI gene confers a high risk of age-related macular degeneration. Nat. Genet. 2013, 45, 813–817. [Google Scholar] [CrossRef]
- Geerlings, M.J.; Kremlitzka, M.; Bakker, B.; Nilsson, S.C.; Saksens, N.T.; Lechanteur, Y.T.; Pauper, M.; Corominas, J.; Fauser, S.; Hoyng, C.B.; et al. The Functional Effect of Rare Variants in Complement Genes on C3b Degradation in Patients With Age-Related Macular Degeneration. JAMA Ophthalmol. 2017, 135, 39–46. [Google Scholar] [CrossRef]
- Mc Mahon, O.; Hallam, T.M.; Patel, S.; Harris, C.L.; Menny, A.; Zelek, W.M.; Widjajahakim, R.; Java, A.; Cox, T.; Tzoumas, N.; et al. The Rare C9 P167S Risk Variant for Age-related Macular Degeneration Increases Polymerization of the Terminal Component of the Complement Cascade. Hum. Mol. Genet. 2021, 30, 1188–1199. [Google Scholar] [CrossRef]
- Cipriani, V.; Lores-Motta, L.; He, F.; Fathalla, D.; Tilakaratna, V.; McHarg, S.; Bayatti, N.; Acar, I.E.; Hoyng, C.B.; Fauser, S.; et al. Increased circulating levels of Factor H-Related Protein 4 are strongly associated with age-related macular degeneration. Nat. Commun. 2020, 11, 778. [Google Scholar] [CrossRef] [Green Version]
- Lores-Motta, L.; van Beek, A.E.; Willems, E.; Zandstra, J.; van Mierlo, G.; Einhaus, A.; Mary, J.L.; Stucki, C.; Bakker, B.; Hoyng, C.B.; et al. Common haplotypes at the CFH locus and low-frequency variants in CFHR2 and CFHR5 associate with systemic FHR concentrations and age-related macular degeneration. Am. J. Hum. Genet. 2021, 108, 1367–1384. [Google Scholar] [CrossRef]
- Cipriani, V.; Tierney, A.; Griffiths, J.R.; Zuber, V.; Sergouniotis, P.I.; Yates, J.R.W.; Moore, A.T.; Bishop, P.N.; Clark, S.J.; Unwin, R.D. Beyond factor H: The impact of genetic-risk variants for age-related macular degeneration on circulating factor-H-like 1 and factor-H-related protein concentrations. Am. J. Hum. Genet. 2021, 108, 1385–1400. [Google Scholar] [CrossRef]
- Acar, I.E.; Lores-Motta, L.; Colijn, J.M.; Meester-Smoor, M.A.; Verzijden, T.; Cougnard-Gregoire, A.; Ajana, S.; Merle, B.M.J.; de Breuk, A.; Heesterbeek, T.J.; et al. Integrating Metabolomics, Genomics, and Disease Pathways in Age-Related Macular Degeneration: The EYE-RISK Consortium. Ophthalmology 2020, 127, 1693–1709. [Google Scholar] [CrossRef]
- Willems, E.; Alkema, W.; Keizer-Garritsen, J.; Suppers, A.; van der Flier, M.; Philipsen, R.; van den Heuvel, L.P.; Volokhina, E.; van der Molen, R.G.; Herberg, J.A.; et al. Biosynthetic homeostasis and resilience of the complement system in health and infectious disease. EBioMedicine 2019, 45, 303–313. [Google Scholar] [CrossRef] [Green Version]
- Lores-Motta, L.; Paun, C.C.; Corominas, J.; Pauper, M.; Geerlings, M.J.; Altay, L.; Schick, T.; Daha, M.R.; Fauser, S.; Hoyng, C.B.; et al. Genome-Wide Association Study Reveals Variants in CFH and CFHR4 Associated with Systemic Complement Activation: Implications in Age-Related Macular Degeneration. Ophthalmology 2018, 125, 1064–1074. [Google Scholar] [CrossRef] [Green Version]
- Gaya da Costa, M.; Poppelaars, F.; van Kooten, C.; Mollnes, T.E.; Tedesco, F.; Wurzner, R.; Trouw, L.A.; Truedsson, L.; Daha, M.R.; Roos, A.; et al. Age and Sex-Associated Changes of Complement Activity and Complement Levels in a Healthy Caucasian Population. Front. Immunol. 2018, 9, 2664. [Google Scholar] [CrossRef]
- Moreno-Navarrete, J.M.; Martinez-Barricarte, R.; Catalan, V.; Sabater, M.; Gomez-Ambrosi, J.; Ortega, F.J.; Ricart, W.; Bluher, M.; Fruhbeck, G.; Rodriguez de Cordoba, S.; et al. Complement factor H is expressed in adipose tissue in association with insulin resistance. Diabetes 2010, 59, 200–209. [Google Scholar] [CrossRef] [Green Version]
- Higgins, V.; Omidi, A.; Tahmasebi, H.; Asgari, S.; Gordanifar, K.; Nieuwesteeg, M.; Adeli, K. Marked Influence of Adiposity on Laboratory Biomarkers in a Healthy Cohort of Children and Adolescents. J. Clin. Endocrinol. Metab. 2020, 105, e1781–e1797. [Google Scholar] [CrossRef]
- Kersten, E.; Paun, C.C.; Schellevis, R.L.; Hoyng, C.B.; Delcourt, C.; Lengyel, I.; Peto, T.; Ueffing, M.; Klaver, C.C.W.; Dammeier, S.; et al. Systemic and ocular fluid compounds as potential biomarkers in age-related macular degeneration. Surv. Ophthalmol. 2018, 63, 9–39. [Google Scholar] [CrossRef] [Green Version]
- Fanelli, G.; Gonzalez-Cordero, A.; Gardner, P.J.; Peng, Q.; Fernando, M.; Kloc, M.; Farrar, C.A.; Naeem, A.; Garred, P.; Ali, R.R.; et al. Human stem cell-derived retinal epithelial cells activate complement via collectin 11 in response to stress. Sci. Rep. 2017, 7, 14625. [Google Scholar] [CrossRef]
- Grassmann, F.; Cantsilieris, S.; Schulz-Kuhnt, A.S.; White, S.J.; Richardson, A.J.; Hewitt, A.W.; Vote, B.J.; Schmied, D.; Guymer, R.H.; Weber, B.H.; et al. Multiallelic copy number variation in the complement component 4A (C4A) gene is associated with late-stage age-related macular degeneration (AMD). J. Neuroinflamm. 2016, 13, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biasella, F.; PLoSsl, K.; Karl, C.; Weber, B.H.F.; Friedrich, U. Altered Protein Function Caused by AMD-associated Variant rs704 Links Vitronectin to Disease Pathology. Investig. Ophthalmol. Vis. Sci. 2020, 61, 2. [Google Scholar] [CrossRef] [PubMed]
- Orozco, L.D.; Chen, H.H.; Cox, C.; Katschke, K.J., Jr.; Arceo, R.; Espiritu, C.; Caplazi, P.; Nghiem, S.S.; Chen, Y.J.; Modrusan, Z.; et al. Integration of eQTL and a Single-Cell Atlas in the Human Eye Identifies Causal Genes for Age-Related Macular Degeneration. Cell Rep. 2020, 30, 1246–1259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Jong, S.; Volokhina, E.B.; de Breuk, A.; Nilsson, S.C.; de Jong, E.K.; van der Kar, N.; Bakker, B.; Hoyng, C.B.; van den Heuvel, L.P.; Blom, A.M.; et al. Effect of rare coding variants in the CFI gene on Factor I expression levels. Hum. Mol. Genet. 2020, 29, 2313–2324. [Google Scholar] [CrossRef]
- Willems, E.; Lores-Motta, L.; Zanichelli, A.; Suffritti, C.; van der Flier, M.; van der Molen, R.G.; Langereis, J.D.; van Drongelen, J.; van den Heuvel, L.P.; Volokhina, E.; et al. Quantitative multiplex profiling of the complement system to diagnose complement-mediated diseases. Clin. Transl. Immunol. 2020, 9, e1225. [Google Scholar] [CrossRef]
- Colijn, J.M.; den Hollander, A.I.; Demirkan, A.; Cougnard-Gregoire, A.; Verzijden, T.; Kersten, E.; Meester-Smoor, M.A.; Merle, B.M.J.; Papageorgiou, G.; Ahmad, S.; et al. Increased High-Density Lipoprotein Levels Associated with Age-Related Macular Degeneration: Evidence from the EYE-RISK and European Eye Epidemiology Consortia. Ophthalmology 2019, 126, 393–406. [Google Scholar] [CrossRef] [Green Version]
- De Jong, S.; Gagliardi, G.; Garanto, A.; de Breuk, A.; Lechanteur, Y.T.E.; Katti, S.; van den Heuvel, L.P.; Volokhina, E.B.; den Hollander, A.I. Implications of genetic variation in the complement system in age-related macular degeneration. Prog. Retin. Eye Res. 2021, 84, 100952. [Google Scholar] [CrossRef]
- Kumar-Singh, R. The role of complement membrane attack complex in dry and wet AMD - From hypothesis to clinical trials. Exp. Eye Res. 2019, 184, 266–277. [Google Scholar] [CrossRef]
- Fauser, S.; Smailhodzic, D.; Caramoy, A.; van de Ven, J.P.; Kirchhof, B.; Hoyng, C.B.; Klevering, B.J.; Liakopoulos, S.; den Hollander, A.I. Evaluation of serum lipid concentrations and genetic variants at high-density lipoprotein metabolism loci and TIMP3 in age-related macular degeneration. Investig. Ophthalmol. Vis. Sci. 2011, 52, 5525–5528. [Google Scholar] [CrossRef] [Green Version]
- MacLean, B.; Tomazela, D.M.; Shulman, N.; Chambers, M.; Finney, G.L.; Frewen, B.; Kern, R.; Tabb, D.L.; Liebler, D.C.; MacCoss, M.J. Skyline: An open source document editor for creating and analyzing targeted proteomics experiments. Bioinformatics 2010, 26, 966–968. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic | Peptide ID | Protein | Pearson’s r | p-Value | p-ValueFDR |
|---|---|---|---|---|---|
| Age | 39 | FD | 0.25 | 2.50 × 10−8 | 1.60 × 10−6 |
| 46 | MASP1/3 | −0.19 | 2.78 × 10−5 | 8.89 × 10−4 | |
| 52 | FCN3 | −0.18 | 9.94 × 10−5 | 2.12 × 10−3 | |
| 35 | C9 | 0.14 | 1.65 × 10−3 | 2.64 × 10−2 | |
| 32 | C8G | −0.14 | 2.80 × 10−3 | 2.94 × 10−2 | |
| 31 | C8G | −0.14 | 2.85 × 10−3 | 2.94 × 10−2 | |
| 48 | MASP1 | −0.13 | 3.21 × 10−3 | 2.94 × 10−2 | |
| 25 | C7 | 0.13 | 3.87 × 10−3 | 3.10 × 10−2 | |
| 27 | C8A | −0.13 | 4.94 × 10−3 | 3.16 × 10−2 | |
| 26 | C8A | −0.13 | 4.64 × 10−3 | 3.16 × 10−2 | |
| 55 | C4BPA | −0.12 | 7.62 × 10−3 | 4.07 × 10−2 | |
| 60 | Clusterin | −0.12 | 7.07 × 10−3 | 4.07 × 10−2 | |
| Sex | 23 | C6 | 0.19 | 3.17 × 10−5 | 2.03 × 10−3 |
| 50 | MBL2 | −0.18 | 9.60 × 10−5 | 3.07 × 10−3 | |
| 51 | MBL2 | −0.17 | 2.06 × 10−4 | 3.29 × 10−3 | |
| 57 | C4BPB | 0.17 | 1.69 × 10−4 | 3.29 × 10−3 | |
| 58 | IC1 | 0.16 | 6.38 × 10−4 | 8.17 × 10−3 | |
| 59 | IC1 | 0.15 | 7.97 × 10−4 | 8.50 × 10−3 | |
| 43 | FI | 0.14 | 2.61 × 10−3 | 1.86 × 10−2 | |
| 61 | Clusterin | 0.14 | 2.47 × 10−3 | 1.86 × 10−2 | |
| 60 | Clusterin | 0.14 | 2.58 × 10−3 | 1.86 × 10−2 | |
| 39 | FD | −0.14 | 2.95 × 10−3 | 1.89 × 10−2 | |
| 27 | C8A | 0.13 | 5.85 × 10−3 | 3.40 × 10−2 | |
| BMI | 44 | CRP | 0.28 | 9.49 × 10−9 | 6.07 × 10−7 |
| 12 | C3 | 0.24 | 1.20 × 10−6 | 3.85 × 10−5 | |
| 41 | FH | 0.21 | 1.05 × 10−5 | 2.25 × 10−4 | |
| 43 | FI | 0.20 | 5.55 × 10−5 | 8.88 × 10−4 | |
| 42 | FH | 0.19 | 1.27 × 10−4 | 1.63 × 10−3 | |
| 40 | FH | 0.18 | 1.77 × 10−4 | 1.89 × 10−3 | |
| 63 | Vitronectin | 0.17 | 4.03 × 10−4 | 3.69 × 10−3 | |
| 13 | C3 | 0.14 | 5.40 × 10−3 | 4.32 × 10−2 | |
| 38 | FB | 0.13 | 6.53 × 10−3 | 4.64 × 10−2 |
| Peptide id | Protein | B | SE | p-Value | p-ValueFDR |
|---|---|---|---|---|---|
| 64 | FHR-2 | 0.234 | 0.094 | 0.013 | 0.517 |
| 44 | CRP | 0.226 | 0.094 | 0.016 | 0.517 |
| 54 | Collectin 11 | 0.187 | 0.094 | 0.046 | 0.913 |
| Peptide Id | Protein | AMD Variant * | Allele | AF | Locus Gene(s) ^ | B | SE | p-Value | p-ValueFDR | OR AMD # | p-Value AMD # |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 64 | FHR-2 | rs61818925 | G | 0.639 | CFH (CFHR3/CFHR1) | 0.570 | 0.075 | 2.84 × 10−13 | 1.13 × 10−12 | 1.667 | 6.0 × 10−165 |
| 64 | FHR-2 | rs570618 | T | 0.442 | CFH | 0.560 | 0.074 | 3.24 × 10−13 | 1.13 × 10−12 | 2.380 | 2.0 × 10−590 |
| 64 | FHR-2 | rs10922109 | C | 0.617 | CFH | 0.540 | 0.078 | 2.20 × 10−11 | 5.13 × 10−11 | 2.632 | 9.6 × 10−618 |
| 64 | FHR-2 | rs148553336 | T | 0.996 | CFH | 1.320 | 0.585 | 0.025 | 0.044 | 3.448 | 8.6 × 10−26 |
| 41 | FH | rs148553336 | T | 0.996 | CFH | 1.669 | 0.573 | 0.004 | 0.084 | 3.448 | 8.6 × 10−26 |
| 40 | FH | rs148553336 | T | 0.996 | CFH | 1.399 | 0.576 | 0.016 | 0.112 | 3.448 | 8.6 × 10−26 |
| 42 | FH | rs148553336 | T | 0.996 | CFH | 1.403 | 0.581 | 0.016 | 0.112 | 3.448 | 8.6 × 10−26 |
| 41 | FH | rs61818925 | G | 0.639 | CFH (CFHR3/CFHR1) | 0.179 | 0.079 | 0.024 | 0.126 | 1.667 | 6.0 × 10−165 |
| 42 | FH | rs10922109 | C | 0.617 | CFH | −0.164 | 0.082 | 0.047 | 0.197 | 2.632 | 9.6 × 10−618 |
| 17 | C4 | rs181705462 | T | 0.009 | C2/CFB/SKIV2L | 1.713 | 0.401 | 2.55 × 10−5 | 0.001 | 1.550 | 3.1 × 10−10 |
| 15 | C4 | rs181705462 | T | 0.009 | C2/CFB/SKIV2L | 1.485 | 0.406 | 2.91 × 10−4 | 0.003 | 1.550 | 3.1 × 10−10 |
| 16 | C4 | rs181705462 | T | 0.009 | C2/CFB/SKIV2L | 1.468 | 0.409 | 3.73 × 10−4 | 0.003 | 1.550 | 3.1 × 10−10 |
| 14 | C4 | rs181705462 | T | 0.009 | C2/CFB/SKIV2L | 1.318 | 0.410 | 0.001 | 0.006 | 1.550 | 3.1 × 10−10 |
| 63 | Vitronectin | rs11080055 | A | 0.522 | TMEM97/VTN | 0.206 | 0.072 | 0.005 | 0.010 | 1.099 | 1.0 × 10−8 |
| Metabolite | ORAMD * | Peptide Id | Protein | B | SE | p-Value | p-ValueFDR |
|---|---|---|---|---|---|---|---|
| XL-HDL-C | 1.082 | 12 | C3 | −0.250 | 0.044 | 2.79 × 10−8 | 3.70 × 10−5 |
| XL-HDL-L | 1.102 | 12 | C3 | −0.246 | 0.044 | 2.81 × 10−8 | 3.70 × 10−5 |
| XL-HDL-P | 1.105 | 12 | C3 | −0.249 | 0.044 | 2.89 × 10−8 | 3.70 × 10−5 |
| XL-HDL-FC | 1.092 | 12 | C3 | −0.240 | 0.044 | 6.61 × 10−8 | 6.34 × 10−5 |
| XL-HDL-C | 1.082 | 42 | FH | −0.239 | 0.044 | 9.93 × 10−8 | 6.71 × 10−5 |
| XL-HDL-P | 1.105 | 42 | FH | −0.237 | 0.044 | 1.05 × 10−7 | 6.71 × 10−5 |
| XL-HDL-FC | 1.092 | 42 | FH | −0.233 | 0.044 | 1.48 × 10−7 | 7.12 × 10−5 |
| XL-HDL-L | 1.102 | 42 | FH | −0.233 | 0.044 | 1.37 × 10−7 | 7.12 × 10−5 |
| XL-HDL-PL | 1.123 | 12 | C3 | −0.229 | 0.043 | 1.89 × 10−7 | 8.06 × 10−5 |
| Phe | 0.857 | 34 | C9 | 0.227 | 0.044 | 2.97 × 10−7 | 9.97 × 10−5 |
| L-HDL-P | 1.092 | 12 | C3 | −0.218 | 0.042 | 2.65 × 10−7 | 9.97 × 10−5 |
| L-HDL-CE | 1.095 | 12 | C3 | −0.219 | 0.042 | 3.38 × 10−7 | 9.97 × 10−5 |
| L-HDL-FC | 1.097 | 12 | C3 | −0.224 | 0.043 | 3.14 × 10−7 | 9.97 × 10−5 |
| L-HDL-C | 1.095 | 12 | C3 | −0.218 | 0.042 | 3.90 × 10−7 | 1.07 × 10−4 |
| XL-HDL-P | 1.105 | 63 | Vitronectin | −0.225 | 0.044 | 5.01 × 10−7 | 1.13 × 10−4 |
| XL-HDL-PL | 1.123 | 42 | FH | −0.220 | 0.043 | 5.29 × 10−7 | 1.13 × 10−4 |
| L-HDL-P | 1.092 | 42 | FH | −0.213 | 0.042 | 4.51 × 10−7 | 1.13 × 10−4 |
| L-HDL-CE | 1.095 | 42 | FH | −0.214 | 0.042 | 5.27 × 10−7 | 1.13 × 10−4 |
| L-HDL-FC | 1.097 | 42 | FH | −0.218 | 0.043 | 5.66 × 10−7 | 1.14 × 10−4 |
| L-HDL-C | 1.095 | 42 | FH | −0.213 | 0.042 | 6.12 × 10−7 | 1.18 × 10−4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Acar, I.E.; Willems, E.; Kersten, E.; Keizer-Garritsen, J.; Kragt, E.; Bakker, B.; Galesloot, T.E.; Hoyng, C.B.; Fauser, S.; van Gool, A.J.; et al. Semi-Quantitative Multiplex Profiling of the Complement System Identifies Associations of Complement Proteins with Genetic Variants and Metabolites in Age-Related Macular Degeneration. J. Pers. Med. 2021, 11, 1256. https://doi.org/10.3390/jpm11121256
Acar IE, Willems E, Kersten E, Keizer-Garritsen J, Kragt E, Bakker B, Galesloot TE, Hoyng CB, Fauser S, van Gool AJ, et al. Semi-Quantitative Multiplex Profiling of the Complement System Identifies Associations of Complement Proteins with Genetic Variants and Metabolites in Age-Related Macular Degeneration. Journal of Personalized Medicine. 2021; 11(12):1256. https://doi.org/10.3390/jpm11121256
Chicago/Turabian StyleAcar, I. Erkin, Esther Willems, Eveline Kersten, Jenneke Keizer-Garritsen, Else Kragt, Bjorn Bakker, Tessel E. Galesloot, Carel B. Hoyng, Sascha Fauser, Alain J. van Gool, and et al. 2021. "Semi-Quantitative Multiplex Profiling of the Complement System Identifies Associations of Complement Proteins with Genetic Variants and Metabolites in Age-Related Macular Degeneration" Journal of Personalized Medicine 11, no. 12: 1256. https://doi.org/10.3390/jpm11121256
APA StyleAcar, I. E., Willems, E., Kersten, E., Keizer-Garritsen, J., Kragt, E., Bakker, B., Galesloot, T. E., Hoyng, C. B., Fauser, S., van Gool, A. J., Lechanteur, Y. T. E., Koertvely, E., Nogoceke, E., Gloerich, J., de Jonge, M. I., Lorés-Motta, L., & den Hollander, A. I. (2021). Semi-Quantitative Multiplex Profiling of the Complement System Identifies Associations of Complement Proteins with Genetic Variants and Metabolites in Age-Related Macular Degeneration. Journal of Personalized Medicine, 11(12), 1256. https://doi.org/10.3390/jpm11121256