
Long-Term Mortality in Critically Ill Tracheostomized Patients Based on Home Mechanical Ventilation at Discharge


Abstract
1. Introduction
2. Materials and Methods
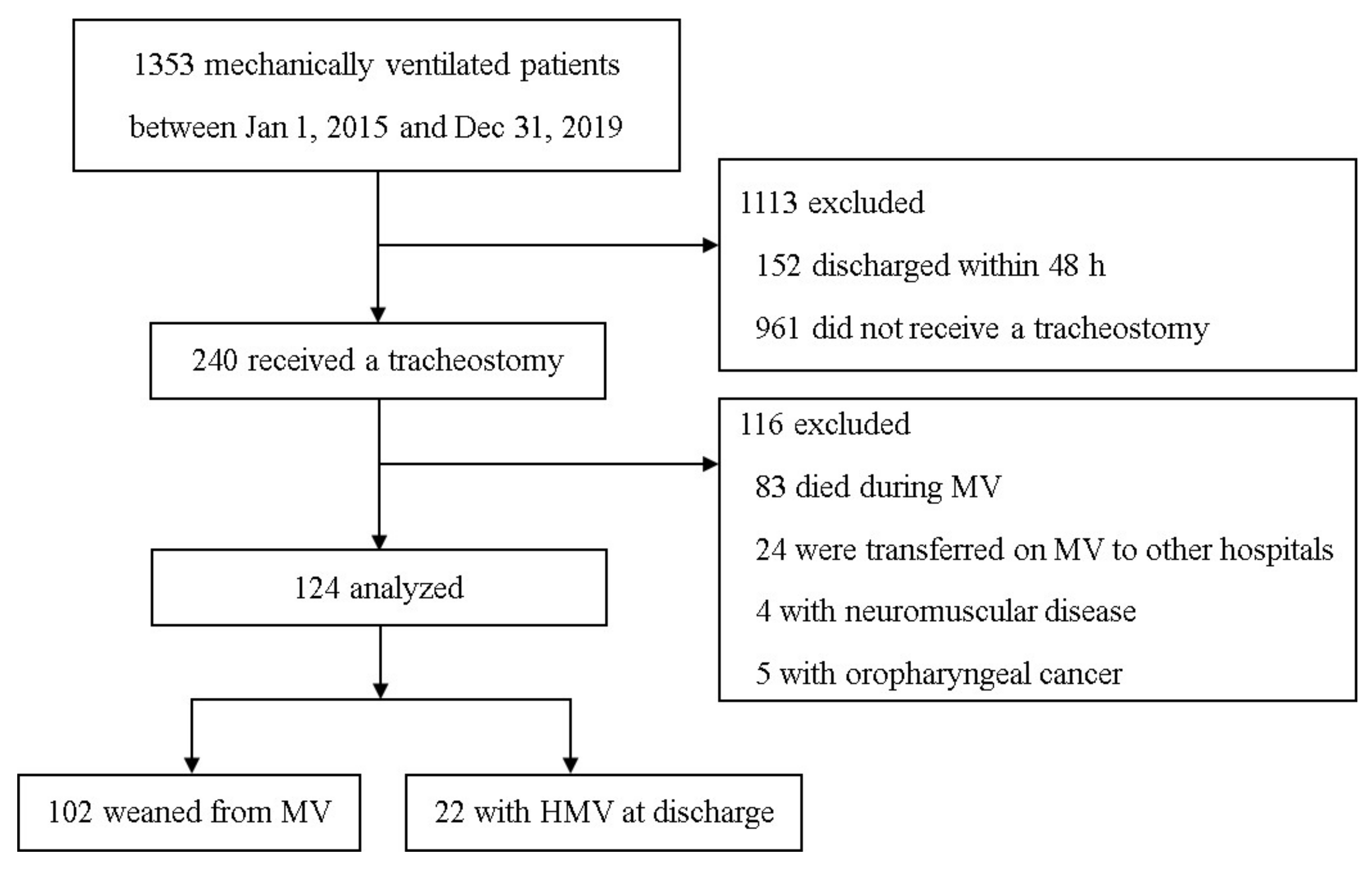
2.1. Study Design and Patients
2.2. Data Collection and Definitions
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
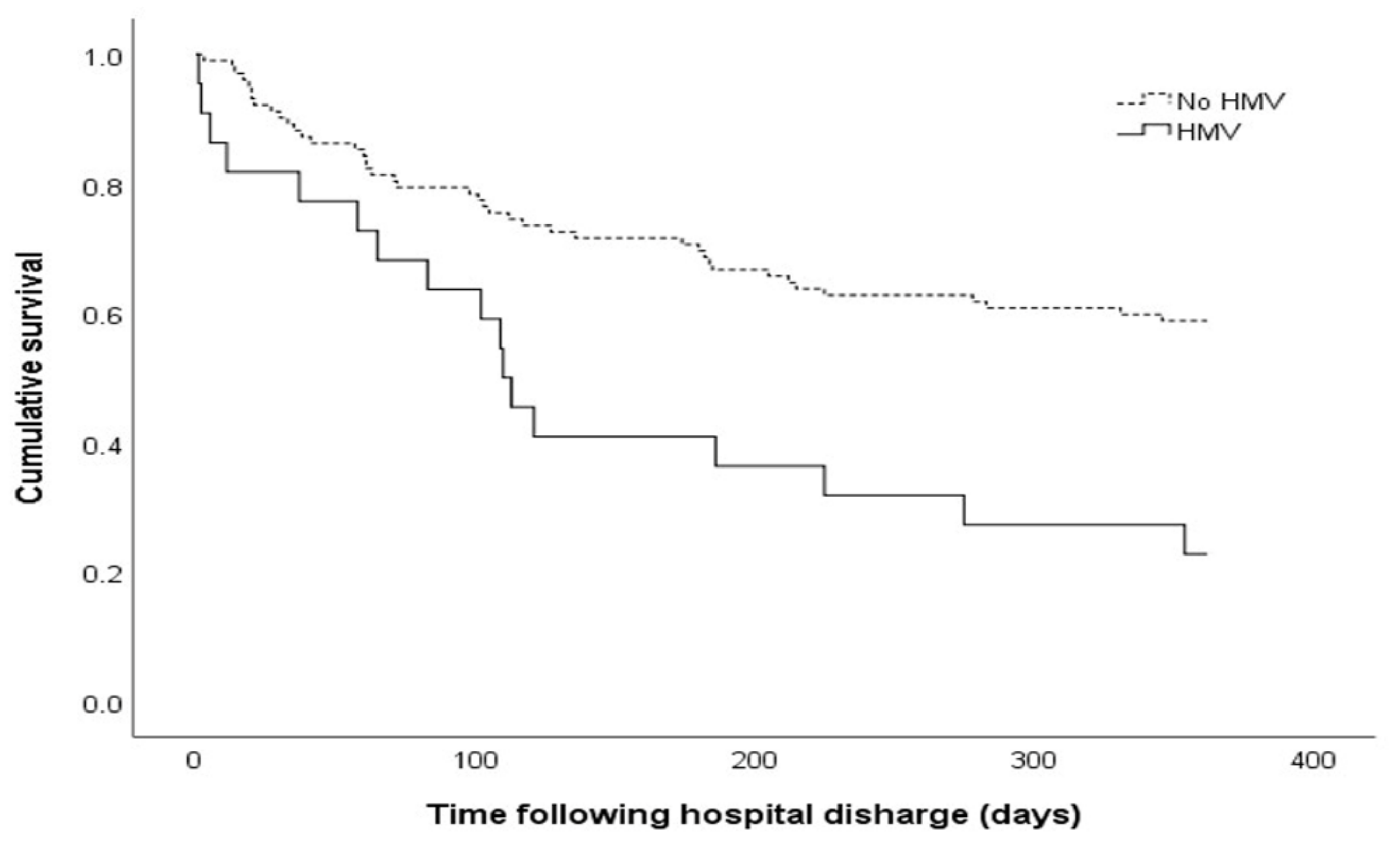
3.2. Outcomes of Patients Who Received a Tracheostomy
3.3. Predictive Factors for 1-Year Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Simonds, A.K. Home Mechanical Ventilation: An Overview. Ann. Am. Thorac. Soc. 2016, 13, 2035–2044. [Google Scholar] [CrossRef]
- Hind, M.; Polkey, M.I.; Simonds, A.K. AJRCCM: 100-Year Anniversary. Homeward Bound: A Centenary of Home Mechanical Ventilation. Am. J. Respir. Crit. Care Med. 2017, 195, 1140–1149. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.I.; Cho, J.H.; Park, S.Y.; Lee, Y.S.; Chang, Y.; Choi, W.I.; Sim, Y.S.; Moon, J.Y.; Lee, K.; Jung, K.S.; et al. Home Mechanical Ventilation Use in South Korea Based on National Health Insurance Service Data. Respir. Care 2019, 64, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, K.; Wahidi, M.M. The Changing Role for Tracheostomy in Patients Requiring Mechanical Ventilation. Clin. Chest Med. 2016, 37, 741–751. [Google Scholar] [CrossRef]
- Ambrosino, N.; Gabbrielli, L. The difficult-to-wean patient. Exp. Rev. Respir. Med. 2010, 4, 685–692. [Google Scholar] [CrossRef]
- Li, J.; Zhan, Q.Y.; Wang, C. Survey of Prolonged Mechanical Ventilation in Intensive Care Units in Mainland China. Respiratory Care 2016, 61, 1224–1231. [Google Scholar] [CrossRef]
- Damuth, E.; Mitchell, J.A.; Bartock, J.L.; Roberts, B.W.; Trzeciak, S. Long-term survival of critically ill patients treated with prolonged mechanical ventilation: A systematic review and meta-analysis. Lancet. Respir. Med. 2015, 3, 544–553. [Google Scholar] [CrossRef]
- Hill, A.D.; Fowler, R.A.; Burns, K.E.; Rose, L.; Pinto, R.L.; Scales, D.C. Long-Term Outcomes and Health Care Utilization after Prolonged Mechanical Ventilation. Ann. Am. Thorac. Soc. 2017, 14, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Vagheggini, G.; Vlad, E.P.; Mazzoleni, S.; Bortolotti, U.; Guarracino, F.; Ambrosino, N. Outcomes for difficult-to-wean subjects after cardiac surgery. Respir. Care 2015, 60, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Hough, C.L.; Caldwell, E.S.; Cox, C.E.; Douglas, I.S.; Kahn, J.M.; White, D.B.; Seeley, E.J.; Bangdiwala, S.I.; Rubenfeld, G.D.; Angus, D.C.; et al. Development and Validation of a Mortality Prediction Model for Patients Receiving 14 Days of Mechanical Ventilation. Crit. Care Med. 2015, 43, 2339–2345. [Google Scholar] [CrossRef]
- Carson, S.S.; Kahn, J.M.; Hough, C.L.; Seeley, E.J.; White, D.B.; Douglas, I.S.; Cox, C.E.; Caldwell, E.; Bangdiwala, S.I.; Garrett, J.M.; et al. A multicenter mortality prediction model for patients receiving prolonged mechanical ventilation. Crit. Care Med. 2012, 40, 1171–1176. [Google Scholar] [CrossRef] [PubMed]
- Boles, J.M.; Bion, J.; Connors, A.; Herridge, M.; Marsh, B.; Melot, C.; Pearl, R.; Silverman, H.; Stanchina, M.; Vieillard-Baron, A.; et al. Weaning from mechanical ventilation. Eur. Respir. J. 2007, 29, 1033–1056. [Google Scholar] [CrossRef] [PubMed]
- Dettmer, M.R.; Damuth, E.; Zarbiv, S.; Mitchell, J.A.; Bartock, J.L.; Trzeciak, S. Prognostic Factors for Long-Term Mortality in Critically Ill Patients Treated With Prolonged Mechanical Ventilation: A Systematic Review. Crit. Care Med. 2017, 45, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Cinotti, R.; Voicu, S.; Jaber, S.; Chousterman, B.; Paugam-Burtz, C.; Oueslati, H.; Damoisel, C.; Caillard, A.; Roquilly, A.; Feuillet, F.; et al. Tracheostomy and long-term mortality in ICU patients undergoing prolonged mechanical ventilation. PLoS ONE 2019, 14, e0220399. [Google Scholar] [CrossRef]
- Kojicic, M.; Li, G.; Ahmed, A.; Thakur, L.; Trillo-Alvarez, C.; Cartin-Ceba, R.; Gay, P.C.; Gajic, O. Long-term survival in patients with tracheostomy and prolonged mechanical ventilation in Olmsted County, Minnesota. Respiratory Care 2011, 56, 1765–1770. [Google Scholar] [CrossRef] [PubMed]
- Cohen, O.; Shapira-Galitz, Y.; Shnipper, R.; Stavi, D.; Halperin, D.; Adi, N.; Lahav, Y. Outcome and survival following tracheostomy in patients ≥ 85 years old. Eur. Arch. Oto-Rhino-Laryngol. 2019, 276, 1837–1844. [Google Scholar] [CrossRef]
- Depuydt, P.; Oeyen, S.; De Smet, S.; De Raedt, S.; Benoit, D.; Decruyenaere, J.; Derom, E. Long-term outcome and health-related quality of life in difficult-to-wean patients with and without ventilator dependency at ICU discharge: A retrospective cohort study. BMC Pulm. Med. 2016, 16, 133. [Google Scholar] [CrossRef]
- Lee, J.M.; Lee, S.M.; Song, J.H.; Kim, Y.S. Clinical outcomes of difficult-to-wean patients with ventilator dependency at intensive care unit discharge. Acute Crit. Care 2020, 35, 156–163. [Google Scholar] [CrossRef] [PubMed]
- O'Connor, H.H.; White, A.C. Tracheostomy decannulation. Respir. Care 2010, 55, 1076–1081. [Google Scholar]
- Kim, H.; Yoon, J.L.; Lee, A.; Jung, Y.; Kim, M.Y.; Cho, J.J.; Ju, Y.S. Prognostic effect of body mass index to mortality in Korean older persons. Geriatr. Gerontol. Int. 2018, 18, 538–546. [Google Scholar] [CrossRef]
- Lee, S.H.; Kim, D.H.; Park, J.H.; Kim, S.; Choi, M.; Kim, H.; Seul, D.E.; Park, S.G.; Jung, J.H.; Han, K.; et al. Association between body mass index and mortality in the Korean elderly: A nationwide cohort study. PLoS ONE 2018, 13, e0207508. [Google Scholar] [CrossRef]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric Nutritional Risk Index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef] [PubMed]
- Kissova, V.; Rosenberger, J.; Goboova, M.; Kiss, A. Ten-year all-cause mortality in hospitalized non-surgical patients based on nutritional status screening. Public Health Nutr. 2015, 18, 2609–2614. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Nasimi, N.; Dabbaghmanesh, M.H.; Sohrabi, Z. Nutritional status and body fat mass: Determinants of sarcopenia in community-dwelling older adults. Exp. Gerontol. 2019, 122, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.M.; Chen, D.; Xie, X.H.; Zhang, J.E.; Zeng, Y.; Cheng, A.S. Sarcopenia as a predictor of mortality among the critically ill in an intensive care unit: A systematic review and meta-analysis. BMC Geriatr. 2021, 21, 339. [Google Scholar] [CrossRef] [PubMed]
- Ambrosino, N.; Vitacca, M. The patient needing prolonged mechanical ventilation: A narrative review. Multidiscip. Respir. Med. 2018, 13, 6. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Total (n = 124) | No HMV (n = 102) | HMV (n = 22) | p Value |
|---|---|---|---|---|
| Age (years) | 77 (68–82) | 76 (69–82) | 78 (66–83) | 0.094 |
| Male (%) | 69 (55.6) | 55 (53.9) | 14 (63.6) | 0.405 |
| Body mass index (kg/m2) | 20.8 (18.4–24.4) | 20.8 (18.5–24.3) | 20.5 (17.7–24.5) | 0.014 |
| Before admission (%) | ||||
| Nursing home or hospital | 29 (23.4) | 26 (25.5) | 3 (13.6) | 0.234 |
| Bedridden status | 29 (23.4) | 26 (25.5) | 3 (13.6) | 0.234 |
| Tube feeding | 29 (23.4) | 24 (23.5) | 5 (22.7) | 0.936 |
| SOFA score | 8.5 (6–11) | 8 (5–11) | 9 (7–11) | 0.014 |
| ProVent 14 score | 2 (2–2) | 2 (2–2) | 2 (2–3) | 0.096 |
| Charlson Comorbidity Index | 4 (3–5) | 4 (3–5) | 3.5 (3–5) | 0.383 |
| Comorbidities (%) | ||||
| Diabetes | 11 (8.9) | 7 (6.9) | 4 (18.2) | 0.105 |
| Hypertension | 12 (9.7) | 9 (8.8) | 3 (13.6) | 0.445 |
| Chronic lung disease | 12 (9.7) | 6 (5.9) | 6 (27.3) | 0.007 |
| Chronic kidney disease | 6 (4.8) | 3 (2.9) | 3 (13.6) | 0.068 |
| Chronic liver disease | 2 (1.6) | 2 (2.0) | 0 (0.0) | 1.000 |
| Cardiovascular disorder | 24 (19.4) | 19 (18.6) | 5 (22.7) | 0.766 |
| Neurological disorder | 30 (24.2) | 25 (24.5) | 5 (22.7) | 1.000 |
| Malignancy | 6 (4.8) | 6 (5.9) | 0 (0.0) | 0.590 |
| Admission via ER (%) | 109 (87.9) | 92 (90.2) | 17 (77.3) | 0.141 |
| Reason for ICU admission (%) | 0.163 | |||
| Sepsis/septic shock | 18 (14.5) | 16 (15.7) | 2 (9.1) | |
| Pneumonia | 42 (33.9) | 38 (37.3) | 4 (18.2) | |
| Cardiovascular disease | 5 (4.0) | 5 (4.9) | 0 (0.0) | |
| ARDS/acute respiratory failure | 13 (10.5) | 10 (9.8) | 3 (13.6) | |
| Post-cardiac arrest care | 35 (28.2) | 26 (25.5) | 9 (40.9) | |
| Other | 11 (8.9) | 7 (6.9) | 4 (18.2) | |
| Tracheostomy type (%) | 0.184 | |||
| Surgical tracheostomy | 91 (73.4) | 72 (70.6) | 19 (86.4) | |
| Percutaneous dilatational tracheostomy | 33 (26.6) | 30 (29.4) | 3 (13.6) | |
| Initial vital signs | ||||
| Systolic blood pressure (mmHg) | 94 (87–107) | 94 (87–106) | 95.5 (90–110) | 0.739 |
| Diastolic blood pressure (mmHg) | 54 (48–60) | 54 (48–59) | 54 (46–65) | 0.622 |
| Heart rate (/min) | 94 (82–110) | 94 (80–106) | 108 (88–126) | 0.499 |
| Respiratory rate (/min) | 22.5 (20–26) | 22 (20–26) | 24 (19–28) | 0.725 |
| Body temperature (°C) | 36.7 (36.4–37.2) | 36.7 (36.5–37.2) | 36.7 (36.2–37.2) | 0.068 |
| Oxygen saturation (%) | 97 (95–99) | 97 (95–99) | 97 (94–99) | 0.762 |
| Glasgow coma scale | 7 (5–10) | 7 (5–10) | 7 (5–10) | 0.834 |
| PaO2/FiO2 | 171 (94–254) | 177 (99–258) | 153 (74–274) | 0.149 |
| Time of MV to tracheostomy (days) | 13 (8–17) | 13 (8–18) | 13 (10–15) | 0.272 |
| Vasopressor (%) | 63 (50.8) | 50 (49.0) | 13 (59.1) | 0.391 |
| CRRT (%) | 18 (14.5) | 12 (11.8) | 6 (27.3) | 0.090 |
| Neuromuscular blocker (%) | 10 (8.1) | 7 (6.9) | 3 (13.6) | 0.383 |
| Laboratory findings | ||||
| White blood cells (×109/L) | 12.4 (8.3–17.0) | 13.1 (8.4–16.9) | 10.3 (8.3–20.6) | 0.296 |
| Platelet (×109/L) | 226 (161–308) | 225 (162–295) | 228 (132–355) | 0.647 |
| Albumin (g/dL) | 3.0 (2.6–3.5) | 3.0 (2.5–3.5) | 3.2 (2.8–3.4) | 0.029 |
| Creatinine (mg/dL) | 0.91 (0.57–1.47) | 0.87 (0.55–1.46) | 1.04 (0.70–2.25) | 0.079 |
| C-reactive protein (mg/dL) | 94 (16–182) | 87 (17–177) | 110 (11–229) | 0.074 |
| Lactic acid (mmol/L) | 1.9 (1.0–3.5) | 1.9 (1.0–3.8) | 1.6 (1.1–2.4) | 0.371 |
| At discharge (%) | ||||
| Nursing home or hospital | 100 (80.6) | 78 (76.5) | 22 (100.0) | 0.007 |
| Tube feeding | 94 (75.8) | 72 (70.6) | 22 (100.0) | 0.003 |
| Decannulation of tracheostomy tube | 25 (20.2) | 25 (24.5) | 0 (0.0) | 0.007 |
| Length of hospital stay (days) | 68 (42–106) | 72 (42–106) | 62 (40–112) | 0.136 |
| Duration of ICU stay (days) | 29 (21–52) | 26 (18–43) | 52 (31–67) | 0.228 |
| Duration of MV (days) | 22 (13–34) | 19 (12–29) | 33 (26–52) | 0.082 |
| Duration of MV and HMV (days) | 23 (13–46) | 19 (12–29) | 75 (52–102) | 0.034 |
| Variables | Total (n = 124) | No HMV (n = 102) | HMV (n = 22) | p Value |
|---|---|---|---|---|
| Primary outcome | ||||
| 1-yr mortality (%) | 59 (47.6) | 42 (41.2) | 17 (77.3) | 0.002 |
| Secondary outcomes | ||||
| 3-m mortality (%) | 29 (23.4) | 21 (20.6) | 8 (36.4) | 0.162 |
| 6-m mortality (%) | 44 (35.5) | 31 (30.4) | 13 (59.1) | 0.014 |
| Variables | Univariate Analysis | Multivariable Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p value | HR (95% CI) | p value | |
| Age | 1.009 (0.989–1.029) | 0.388 | ||
| Male | 1.694 (0.993–2.889) | 0.053 | ||
| Body mass index | 0.917 (0.856–0.982) | 0.013 | 0.913 (0.850–0.980) | 0.012 |
| Bedridden status before admission | 1.150 (0.640–2.066) | 0.641 | ||
| Tube feeding before admission | 1.314 (0.740–2.332) | 0.352 | ||
| SOFA score | 1.080 (1.011–1.154) | 0.023 | 1.114 (1.040–1.193) | 0.002 |
| ProVent 14 score | 1.204 (0.881–1.644) | 0.244 | ||
| Charlson Comorbidity Index | 1.115 (0.971–1.279) | 0.123 | ||
| Vasopressor | 1.772 (1.048–2.995) | 0.033 | ||
| CRRT | 2.113 (1.139–3.918) | 0.018 | ||
| Neuromuscular blocker | 1.815 (0.823–4.004) | 0.140 | ||
| Transferred to a nursing facility | 6.156 (1.925–19.684) | 0.002 | 5.055 (1.558–16.400) | 0.007 |
| Tube feeding at discharge | 4.733 (1.891–11.843) | 0.001 | ||
| Decannulation of tracheostomy tube | 0.362 (0.156–0.843) | 0.018 | ||
| HMV at discharge | 2.560 (1.453–4.510) | 0.001 | 1.930 (1.082–3.444) | 0.026 |
| Length of hospital stay | 0.997 (0.993–1.001) | 0.171 | ||
| Duration of ICU stay | 1.006 (0.996–1.015) | 0.227 | ||
| Duration of MV and HMV | 1.004 (1.000–1.008) | 0.032 | ||
| Time from MV to tracheostomy | 0.993 (0.977–1.009) | 0.361 | ||
| PaO2/FiO2 | 0.999 (0.997–1.001) | 0.315 | ||
| Albumin | 0.619 (0.406–0.946) | 0.027 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, W.-Y.; Baek, M.S. Long-Term Mortality in Critically Ill Tracheostomized Patients Based on Home Mechanical Ventilation at Discharge. J. Pers. Med. 2021, 11, 1257. https://doi.org/10.3390/jpm11121257
Kim W-Y, Baek MS. Long-Term Mortality in Critically Ill Tracheostomized Patients Based on Home Mechanical Ventilation at Discharge. Journal of Personalized Medicine. 2021; 11(12):1257. https://doi.org/10.3390/jpm11121257
Chicago/Turabian StyleKim, Won-Young, and Moon Seong Baek. 2021. "Long-Term Mortality in Critically Ill Tracheostomized Patients Based on Home Mechanical Ventilation at Discharge" Journal of Personalized Medicine 11, no. 12: 1257. https://doi.org/10.3390/jpm11121257
APA StyleKim, W.-Y., & Baek, M. S. (2021). Long-Term Mortality in Critically Ill Tracheostomized Patients Based on Home Mechanical Ventilation at Discharge. Journal of Personalized Medicine, 11(12), 1257. https://doi.org/10.3390/jpm11121257