A Child’s Perception of Their Developmental Difficulties in Relation to Their Adult Assessment. Analysis of the INPP Questionnaire


 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Examined Group
2.2. Questionnaire
2.3. Statistical Methods
3. Results
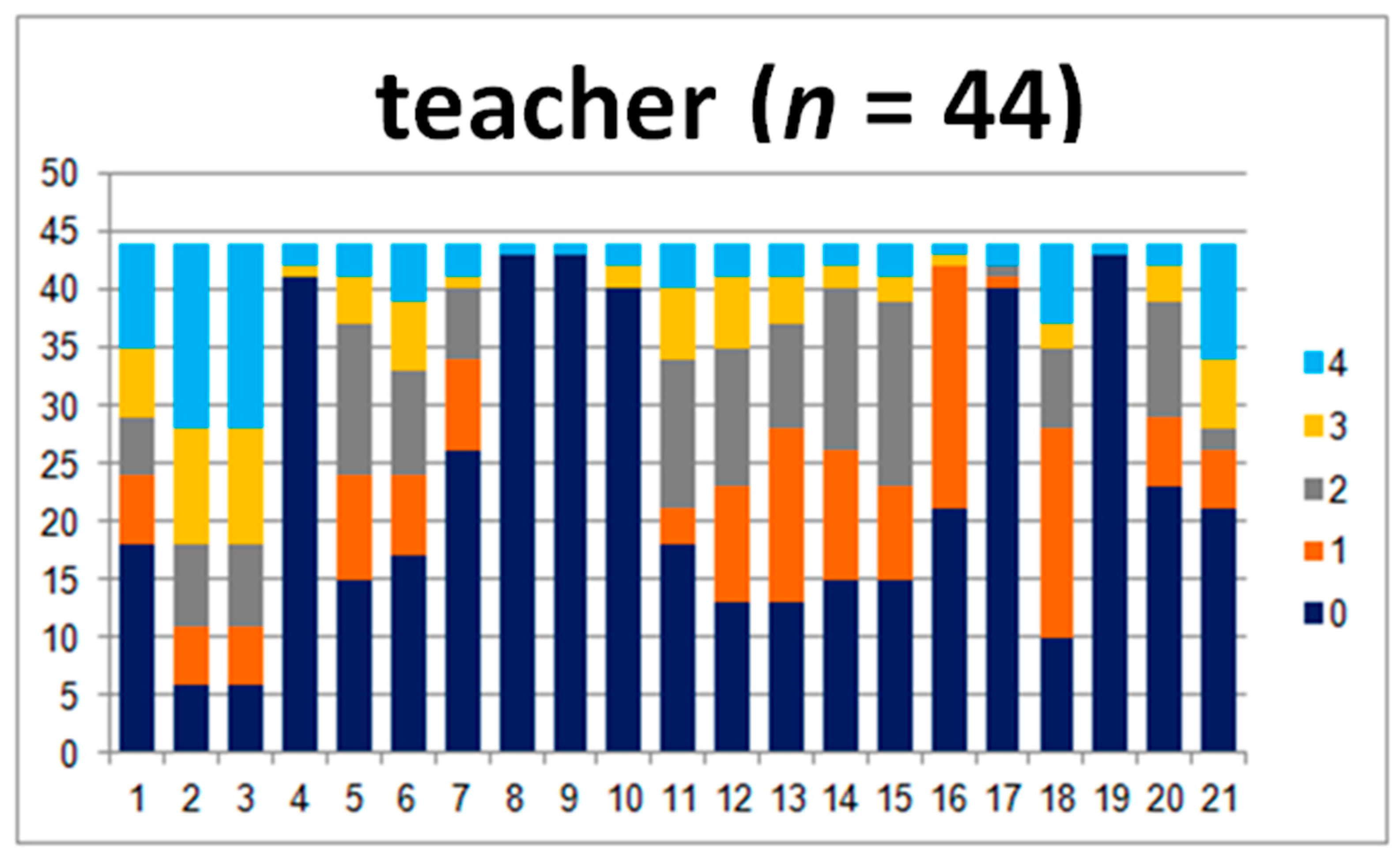
3.1. Child–Teacher Subgroup
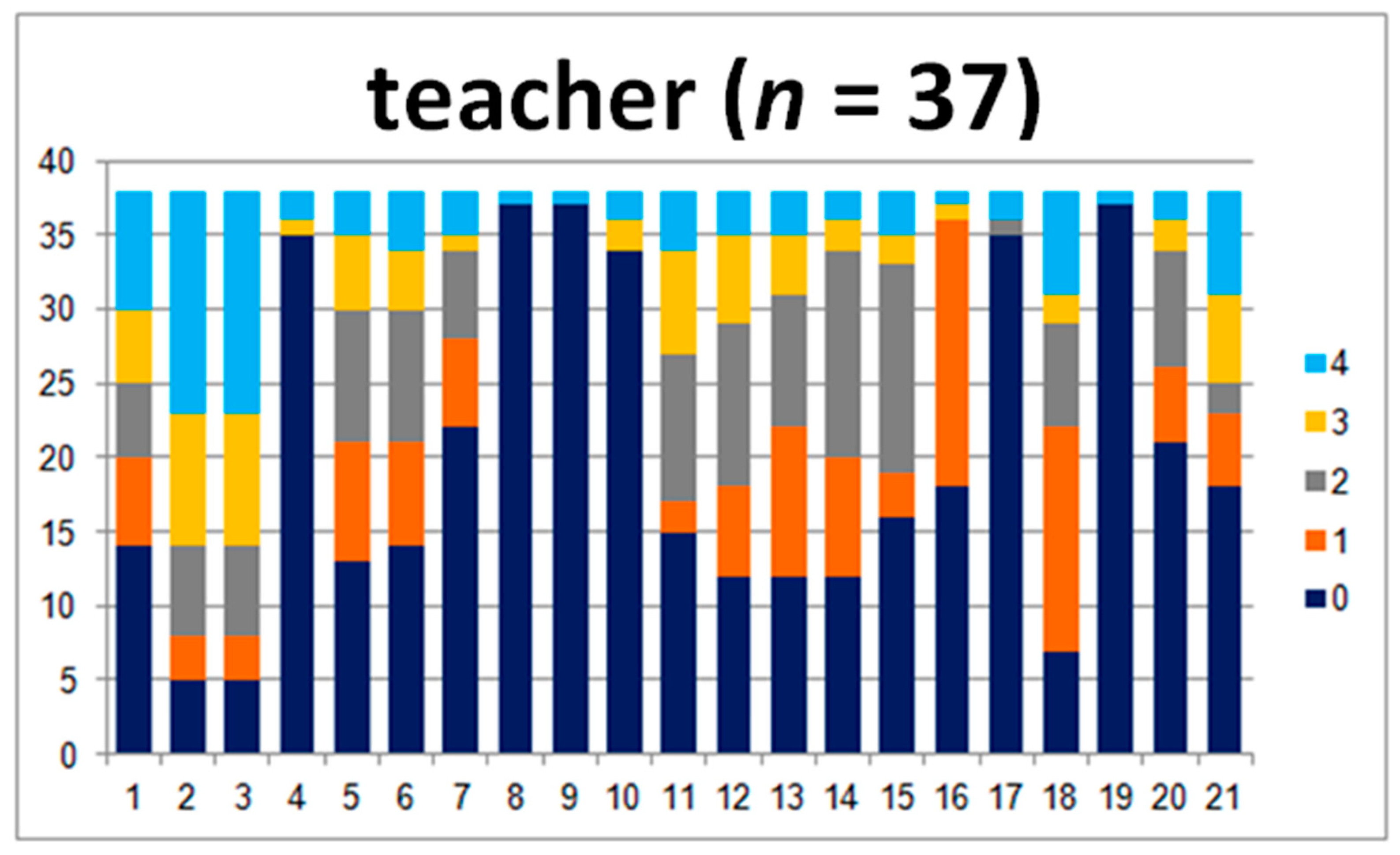
3.2. Parent–Teacher Subgroup
3.3. Child–Parent Subgroup
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Wiejak, K.; Krasowicz-Kupis, G.; Awramiuk, E. Linguistic determinants of early reading and writing skills based on the teacher’s assessment using the IBE Educational Forecasting Scale. Educ. Psychol. 2017, 11, 41–63. [Google Scholar]
- Bogdanowicz, M. Specific difficulties in reading and writing—Developmental dyslexia. In Speech Therapy: Questions and Answers; Gałkowski, T., Jastrzębowska, G., Eds.; University of Opole: Opole, Poland, 1999; pp. 815–859. [Google Scholar]
- Bogdanowicz, M. Risk of Dyslexia. Problem and Diagnosis; Harmonia Publishing House: Gdańsk, Poland, 2002. [Google Scholar]
- Grzywniak, C. Research on neuropsychological maturity for school learning. Rep. Own Res. Men Disabil. Soc. 2015, 2, 67–83. [Google Scholar]
- Pecuch, A.; Kołcz-Trzęsicka, A.; Żurowska, A.; Paprocka-Borowicz, M. Psychomotor disorders assessment in 4–6 year-old children with INPP test battery. Nurs. Public Health 2018, 8, 11–20. [Google Scholar] [CrossRef]
- Gieysztor, E.; Sadowska, L.; Choińska, A. The degree of primitive reflexes integration as a diagnostic tool to assess the neurological maturity of healthy preschool and early school age children. Nurs. Public Health 2017, 7, 5–11. [Google Scholar] [CrossRef]
- Goddart-Blythe, S. The role of primitive survival reflexes in the development of the visual system. J. Beh. Opt. 1995, 6, 31–35. [Google Scholar]
- Goddard-Blythe, S. Reflexes, Learning and Behavior: A Window into the Child’s Mind; Fern Ridge Press: Eugene, OR, USA, 2005. [Google Scholar]
- Goddard-Blythe, S. Attention, Balance and Coordination: The A.B.C. of Learning Success; Wiley: Hoboken, NJ, USA, 2009. [Google Scholar]
- Coyne, I. Consultation with children in hospital: Children, parents’ and nurses’ perspectives. J. Clin. Nurs. 2006, 15, 61–71. [Google Scholar] [CrossRef] [PubMed]
- Coyne, I. Children’s participation in consultations and decision-making at health service level: A review of the literature. Int. J. Nurs. Stud. 2008, 45, 1682–1689. [Google Scholar] [CrossRef] [PubMed]
- Crane, L.; Batty, R.; Adeyinka, H.; Goddard, L.; Henry, L.A.; Hill, E.L. Autism Diagnosis in the United Kingdom: Perspectives of Autistic Adults, Parents and Professionals. J. Autism. Dev. Disord. 2018, 48, 3761–3772. [Google Scholar] [CrossRef] [PubMed]
- Soneson, E.; Childs-Fegredo, J.; Anderson, J.K.; Stochl, J.; Fazel, M.; Ford, T.; Humphrey, A.; Jones, P.B.; Howarth, E. Acceptability of screening for mental health difficulties in primary schools: A survey of UK parents. BMC Public Health 2018, 18, 1404. [Google Scholar] [CrossRef] [PubMed]
- Trusz, S. Cognitive and Social Development of a Child in the Light of Interpersonal Expectations of Parents and Teachers; Institute of Educational Sciences, Pedagogical University of Cracow: Cracow, Poland, 2011. [Google Scholar]
- Sikorska, I. “The Diversity of Contexts of the Social Development of a Child” Department of Developmental and Educational Psychology Im. Stefan Szuman; Jagiellonian University Cracow, Developmental Psychology: Cracow, Poland, 2005. [Google Scholar]
- Frydrychowicz, A.; Misiorna, E.; Kozłowska, E.; Pietrzak-Kurzac, M.; Rusiak, P.; Szczepkowska-Szcześniak, K. Teacher’s advisor for six-year-olds: Methodological materials for teachers developed as a result of the project "Study of school readiness of six-year-olds" implemented at the Methodological Center of Psychological and Pedagogical Assistance. In Development and Assessment of Reading Skills of Six-Year-Old Children; Methodological Center for Psychological and Pedagogical Assistance: Warsaw, Poland, 2006. [Google Scholar]
- Peterson, J.; Bruce, J.; Patel, N.; Chamberlain, L.J. Parental Attitudes, Behaviors, and Barriers to School Readiness among Parents of Low-Income Latino Children. Int. J. Env. Res. Public Health 2018, 15, 188. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sum | Level | Degree of Disorder |
|---|---|---|
| 0 | 0 | no disorder |
| 1–21 | 1 | present to a minimum degree |
| 22–42 | 2 | present to a moderate degree |
| 43–63 | 3 | present to a great degree |
| 64–84 | 4 | present at a very high intensity |
| Children (n = 40) | Parents (n = 40) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Questionnaire | M | Me | SD | M | Me | SD | U | p | η2 |
| 1.Inability to sit still | 1.2 | 1 | 1.2 | 1.1 | 1 | 1.2 | 786 | 0.45 | 0.00 |
| 2.Attention problems | 1.3 | 1 | 1.3 | 1.1 | 1 | 1.1 | 753 | 0.33 | 0.00 |
| 3.Easy to distract | 1.6 | 1 | 1.4 | 1.4 | 1 | 1.1 | 740 | 0.28 | 0.00 |
| 4.Coordination problems | 1.0 | 0 | 1.4 | 0.8 | 0 | 1.1 | 780 | 0.35 | 0.00 |
| 5.Incorrect grip | 0.9 | 0 | 1.3 | 0.7 | 0 | 1.1 | 744 | 0.30 | 0.00 |
| 6.Incorrect sitting posture | 1.0 | 1 | 1.2 | 1.1 | 1 | 1.1 | 739 | 0.28 | 0.00 |
| 7.Difficulty catching the ball | 1.2 | 1 | 1.2 | 0.8 | 0 | 1.2 | 660 | 0.09 | 0.02 |
| 8. Difficulty learning to swim | 1.4 | 1 | 1.5 | 0.8 | 0 | 1.1 | 642 | 0.06 | 0.03 |
| 9.Diffiiculty riding a bike | 0.5 | 0 | 1.2 | 0.2 | 0 | 0.8 | 701 | 0.17 | 0.01 |
| 10.Travel sickness | 1.1 | 0 | 1.5 | 0.5 | 0 | 1.0 | 638 | 0.06 | 0.03 |
| 11.Reading problems | 1.4 | 1 | 1.4 | 0.8 | 0 | 1.1 | 589 | 0.02 | 0.05 |
| 12.Writing problems | 1.2 | 1 | 1.2 | 0.9 | 0.5 | 1.1 | 697 | 0.16 | 0.01 |
| 13.Rewriting problems | 0.9 | 0.5 | 1.2 | 0.7 | 0 | 1.1 | 718 | 0.22 | 0.01 |
| 14.Math problems | 1.1 | 1 | 1.2 | 0.5 | 0 | 1.0 | 546 | 0.00 | 0.08 |
| 15.Spelling problems | 1.4 | 1 | 1.4 | 1.1 | 1 | 1.2 | 713 | 0.16 | 0.01 |
| 16.Rearranging numbers or letters | 0.7 | 0 | 1.0 | 1.0 | 1 | 1.2 | 692 | 0.15 | 0.01 |
| 17.Difficulty reading the time | 1.5 | 1 | 1.6 | 1.1 | 0 | 1.4 | 669 | 0.08 | 0.02 |
| 18.Difficulty multi-tasking | 0.9 | 0.55 | 1.0 | 0.9 | 0 | 1.2 | 818 | 0.49 | 0.00 |
| 19.Recurring headaches | 1.0 | 1 | 1.1 | 0.2 | 0 | 0.7 | 437 | 0.00 | 0.15 |
| 20.Frequent fatigue | 1.1 | 1 | 1.1 | 0.6 | 0 | 1.0 | 570 | 0.01 | 0.06 |
| 21.Clear agitation | 1.2 | 1 | 1.3 | 1.0 | 1 | 1.1 | 767 | 0.37 | 0.00 |
| Sum | 23.3 | 23 | 13.2 | 17.3 | 16 | 12.1 | 681 | 0.05 | 0.02 |
| Level | 1.6 | 2 | 0.6 | 1.4 | 1 | 0.7 | 616 | 0.04 | 0.04 |
| Children (n = 44) | Teachers (n = 44) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Questionnaire | M | Me | SD | M | Me | SD | U | p | η2 |
| 1.Inability to sit still | 1.18 | 1 | 1.17 | 1.52 | 1 | 1.62 | 909 | 0.31 | 0.00 |
| 2.Attention problems | 1.34 | 1 | 1.22 | 2.57 | 3 | 1.44 | 506 | 0.00 | 0.15 |
| 3.Easy to distract | 1.66 | 1 | 1.41 | 2.57 | 3 | 1.44 | 637 | 0.00 | 0.09 |
| 4.Coordination problems | 0.78 | 0 | 1.19 | 0.25 | 0 | 0.94 | 725 | 0.02 | 0.05 |
| 5.Incorrect grip | 0.75 | 0 | 1.14 | 1.34 | 1 | 1.24 | 680 | 0.01 | 0.07 |
| 6.Incorrect sitting posture | 1.07 | 1 | 1.25 | 1.43 | 1 | 1.42 | 836 | 0.14 | 0.01 |
| 7.Difficulty catching the ball | 1.18 | 1 | 1.23 | 0.80 | 0 | 1.19 | 854 | 0.05 | 0.01 |
| 8.Difficulty learning to swim | 1.43 | 1 | 1.55 | 0.09 | 0 | 0.60 | 471 | 0.00 | 0.20 |
| 9.Diffiiculty riding a bike | 0.57 | 0 | 1.23 | 0.09 | 0 | 0.60 | 795 | 0.07 | 0.02 |
| 10.Travel sickness | 1.23 | 0 | 1.57 | 0.32 | 0 | 1.03 | 610 | 0.00 | 0.10 |
| 11.Reading problems | 1.25 | 1 | 1.28 | 1.43 | 2 | 1.39 | 905 | 0.30 | 0.00 |
| 12.Writing problems | 1.05 | 1 | 1.16 | 1.45 | 1 | 1.25 | 782 | 0.06 | 0.03 |
| 13.Rewriting problems | 0.89 | 1 | 1.19 | 1.30 | 1 | 1.19 | 745 | 0.03 | 0.04 |
| 14.Math problems | 1.12 | 1 | 1.19 | 1.20 | 1 | 1.11 | 945 | 0.36 | 0.00 |
| 15.Spelling problems | 1.46 | 1 | 1.28 | 1.32 | 1 | 1.20 | 945 | 0.36 | 0.00 |
| 16.Rearranging numbers or letters | 0.68 | 0 | 0.93 | 0.64 | 1 | 0.81 | 958 | 0.47 | 0.00 |
| 17.Difficulty reading the time | 1.46 | 1 | 1.53 | 0.25 | 0 | 0.89 | 514 | 0.00 | 0.16 |
| 18.Difficulty multi-tasking | 0.82 | 1 | 0.99 | 1.50 | 1 | 1.34 | 868 | 0.04 | 0.01 |
| 19.Recurring headaches | 0.87 | 1 | 1.05 | 0.09 | 0 | 0.60 | 474 | 0.00 | 0.19 |
| 20.Frequent fatigue | 1.14 | 1 | 1.12 | 0.98 | 0 | 1.21 | 861 | 0.15 | 0.01 |
| 21.Clear agitation | 1.18 | 1 | 1.30 | 1.52 | 1 | 1.70 | 926 | 0.36 | 0.00 |
| Sum | 23.1 | 23 | 12.6 | 22.70 | 22 | 13.30 | 1003 | 0.27 | 0.00 |
| Level | 1.61 | 2 | 0.65 | 1.90 | 2 | 0.73 | 794 | 0.07 | 0.02 |
| Parents (n = 38) | Teachers (n = 38) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Questionnaire | M | Me | SD | M | Me | SD | U | p | η2 |
| 1.Inability to sit still | 1.13 | 1 | 1.23 | 1.66 | 1 | 1.60 | 591 | 0.09 | 0.03 |
| 2.Attention problems | 1.11 | 1 | 1.03 | 2.68 | 3 | 1.42 | 284 | 0.00 | 0.27 |
| 3.Easy to distract | 1.32 | 1 | 1.09 | 2.68 | 3 | 1.42 | 329 | 0.00 | 0.22 |
| 4.Coordination problems | 0.76 | 0 | 1.08 | 0.29 | 0 | 1.01 | 496 | 0.01 | 0.07 |
| 5.Incorrect grip | 0.61 | 0 | 1.00 | 1.40 | 1 | 1.31 | 462 | 0.00 | 0.10 |
| 6.Incorrect sitting posture | 1.08 | 1 | 1.12 | 1.40 | 1 | 1.37 | 640 | 0.20 | 0.01 |
| 7.Difficulty catching the ball | 0.84 | 0 | 1.15 | 0.87 | 0 | 1.26 | 715 | 0.47 | 0.00 |
| 8. Difficulty learning to swim | 0.79 | 0 | 1.14 | 0.11 | 0 | 0.65 | 463 | 0.00 | 0.10 |
| 9.Diffiiculty riding a bike | 0.21 | 0 | 0.81 | 0.11 | 0 | 0.65 | 685 | 0.35 | 0.00 |
| 10.Travel sickness | 0.51 | 0 | 1.02 | 0.37 | 0 | 1.10 | 602 | 0.14 | 0.02 |
| 11.Reading problems | 0.79 | 0 | 1.04 | 1.55 | 2 | 1.45 | 517 | 0.02 | 0.06 |
| 12.Writing problems | 1.00 | 1 | 1.16 | 1.53 | 2 | 1.31 | 557 | 0.04 | 0.04 |
| 13.Rewriting problems | 0.76 | 0 | 1.15 | 1.37 | 1 | 1.26 | 504 | 0.01 | 0.07 |
| 14.Math problems | 0.58 | 0 | 1.08 | 1.32 | 1 | 1.14 | 431 | 0.00 | 0.12 |
| 15.Spelling problems | 1.21 | 1 | 1.28 | 1.29 | 1.5 | 1.29 | 697 | 0.40 | 0.00 |
| 16.Rearranging numbers or letters | 1.05 | 1 | 1.18 | 0.66 | 1 | 0.85 | 604 | 0.11 | 0.02 |
| 17.Difficulty reading the time | 1.11 | 0 | 1.45 | 0.26 | 0 | 0.95 | 485 | 0.01 | 0.08 |
| 18.Difficulty multi-tasking | 0.90 | 0 | 1.25 | 1.66 | 1 | 1.36 | 462 | 0.00 | 0.10 |
| 19.Recurring headaches | 0.24 | 0 | 0.68 | 0.11 | 0 | 0.65 | 649 | 0.22 | 0.01 |
| 20.Frequent fatigue | 0.55 | 0 | 0.95 | 0.92 | 0 | 1.22 | 613 | 0.13 | 0.02 |
| 21.Clear agitation | 1.00 | 1 | 1.09 | 1.45 | 1 | 1.64 | 648 | 0.22 | 0.01 |
| Sum | 17.53 | 16.5 | 12.17 | 23.66 | 22 | 13.91 | 503 | 0.01 | 0.07 |
| Level | 1.29 | 1 | 0.65 | 1.71 | 2 | 0.73 | 489 | 0.01 | 0.08 |
| Child | Teacher | Parent | Teacher | Child | Parent | |
|---|---|---|---|---|---|---|
| Average sum of results | 23.3 | 22.73 | 17.5 | 23.66 | 20.16 | 14.84 |
| Level 0 * | 0 | 0 | 2 | 0 | 6 | 10 |
| Level 1 | 22 | 19 | 25 | 17 | 22 | 26 |
| Level 2 | 19 | 23 | 9 | 19 | 18 | 11 |
| Level 3 | 3 | 0 | 2 | 0 | 3 | 2 |
| Level 4 | 0 | 2 | 0 | 2 | 0 | 0 |
| Average levels | 1.57 | 1.65 | 1.32 | 1.70 | 1.36 | 1.1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Demiy, A.; Kalemba, A.; Lorent, M.; Pecuch, A.; Wolańska, E.; Telenga, M.; Gieysztor, E.Z. A Child’s Perception of Their Developmental Difficulties in Relation to Their Adult Assessment. Analysis of the INPP Questionnaire. J. Pers. Med. 2020, 10, 156. https://doi.org/10.3390/jpm10040156
Demiy A, Kalemba A, Lorent M, Pecuch A, Wolańska E, Telenga M, Gieysztor EZ. A Child’s Perception of Their Developmental Difficulties in Relation to Their Adult Assessment. Analysis of the INPP Questionnaire. Journal of Personalized Medicine. 2020; 10(4):156. https://doi.org/10.3390/jpm10040156
Chicago/Turabian StyleDemiy, Alina, Agata Kalemba, Maria Lorent, Anna Pecuch, Ewelina Wolańska, Marlena Telenga, and Ewa Z. Gieysztor. 2020. "A Child’s Perception of Their Developmental Difficulties in Relation to Their Adult Assessment. Analysis of the INPP Questionnaire" Journal of Personalized Medicine 10, no. 4: 156. https://doi.org/10.3390/jpm10040156
APA StyleDemiy, A., Kalemba, A., Lorent, M., Pecuch, A., Wolańska, E., Telenga, M., & Gieysztor, E. Z. (2020). A Child’s Perception of Their Developmental Difficulties in Relation to Their Adult Assessment. Analysis of the INPP Questionnaire. Journal of Personalized Medicine, 10(4), 156. https://doi.org/10.3390/jpm10040156