
The Significance of FilmArray Blood Culture Identification Panel (FA-BCID) for Managing Patients with Positive Blood Cultures

 ,
,
Abstract
:1. Introduction
2. Methods
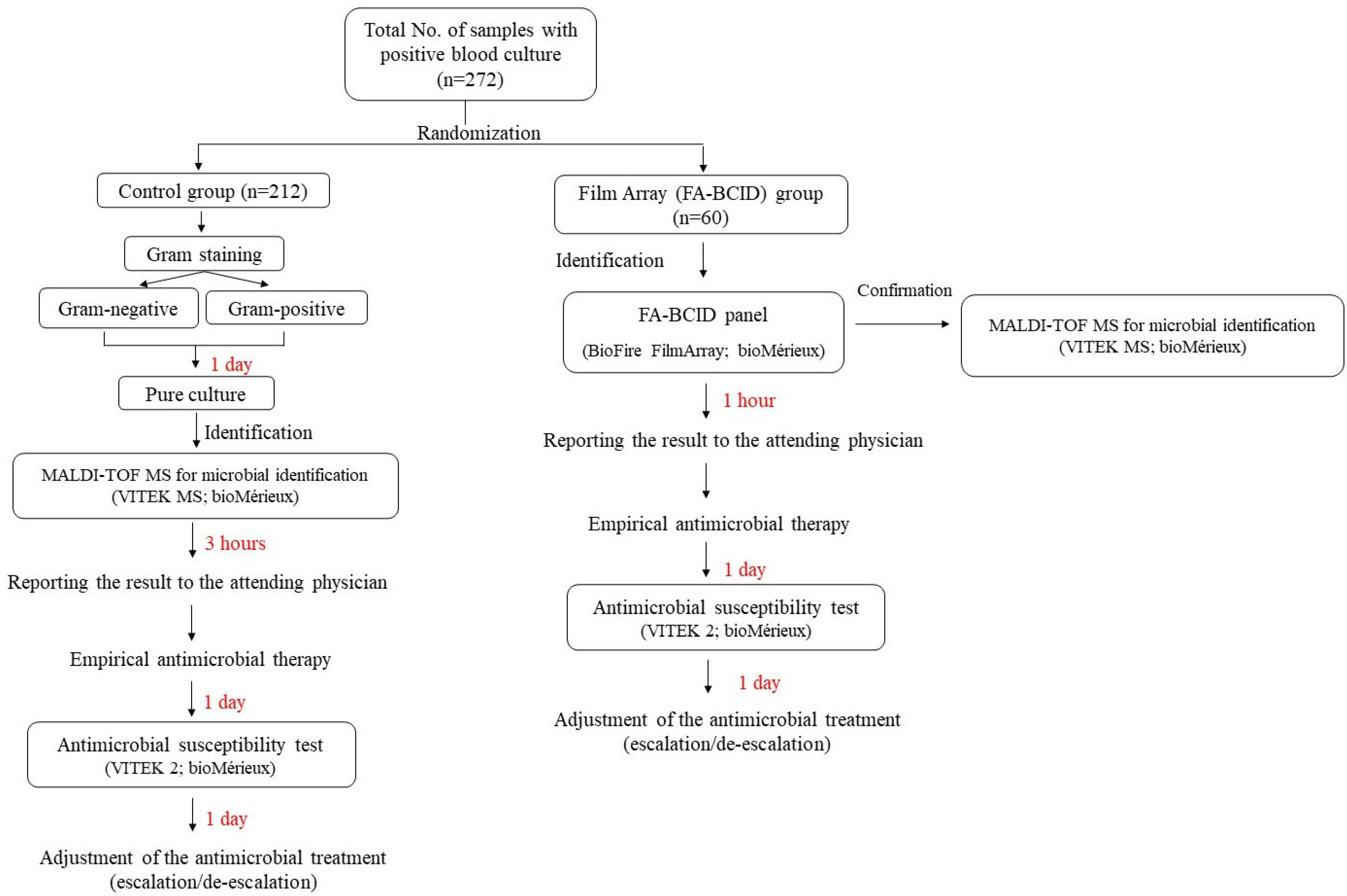
2.1. Study Design
2.2. Laboratory Test
2.2.1. Blood Culture
2.2.2. FilmArray Blood Culture Identification (FA-BCID)
2.2.3. MALDI-TOF MS
2.2.4. Antimicrobial Susceptibility Test (AST)
2.2.5. Analysis of the Clinical and Microbiological Outcomes
2.3. Statistical Analysis
3. Results
3.1. Study Participants
3.2. The Diversity of Clinical Isolates in the Blood Culture Detected Using MALDI-TOF and FA-BCID
3.3. Microorganisms Identified from the Positive Blood Samples According to the Target in the FA-BCID Panel
3.4. Clinical Efficacy of FA-BCID Detection for the Antimicrobial Stewardship Program
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Bauer, M.; Gerlach, H.; Vogelmann, T.; Preissing, F.; Stiefel, J.; Adam, D. Mortality in sepsis and septic shock in Europe, North America, and Australia between 2009 and 2019—Results from a systematic review and meta-analysis. Crit. Care 2020, 24, 239. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Calls for Global Action on Sepsis—Cause of 1 in 5 Deaths Worldwide. Available online: https://www.who.int/news/item/08-09-2020-who-calls-for-global-action-on-sepsis---cause-of-1-in-5-deaths-worldwide (accessed on 11 November 2022).
- Kim, J.; Kim, K.; Lee, H.; Ahn, S. Epidemiology of sepsis in Korea: A population-based study of incidence, mortality, cost and risk factors for death in sepsis. Clin. Exp. Emerg. Med. 2019, 6, 49. [Google Scholar] [CrossRef] [PubMed]
- Park, D.W.; Chun, B.C.; Kim, J.M.; Sohn, J.W.; Peck, K.R.; Kim, Y.S.; Choi, Y.H.; Choi, J.Y.; Kim, S.I.; Eom, J.S. Epidemiological and clinical characteristics of community-acquired severe sepsis and septic shock: A prospective observational study in 12 university hospitals in Korea. J. Korean Med. Sci. 2012, 27, 1308–1314. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Ku, N.S.; Kim, Y.J.; Kim, H.B.; Seok, H.; Lee, D.-G.; Lee, J.S.; Jeong, S.J.; Choi, J.-H.; Sohn, J.W. Korean Registry for Improving Sepsis Survival (KISS): Protocol for a Multicenter Cohort of Adult Patients with Sepsis or Septic Shock. Infect. Chemother. 2020, 52, 31. [Google Scholar] [CrossRef]
- Lee, C.-C.; Lee, C.-H.; Hong, M.-Y.; Tang, H.-J.; Ko, W.-C. Timing of appropriate empirical antimicrobial administration and outcome of adults with community-onset bacteremia. Crit. Care 2017, 21, 119. [Google Scholar] [CrossRef]
- Altun, O.; Almuhayawi, M.; Lüthje, P.; Taha, R.; Ullberg, M.; Özenci, V. Controlled evaluation of the new BacT/Alert Virtuo blood culture system for detection and time to detection of bacteria and yeasts. J. Clin. Microbiol. 2016, 54, 1148–1151. [Google Scholar] [CrossRef]
- Altun, O.; Almuhayawi, M.; Ullberg, M.; Özenci, V. Clinical evaluation of the FilmArray blood culture identification panel in the identification of bacteria and yeasts from positive blood culture bottles. J. Clin. Microbiol. 2013, 51, 4130–4136. [Google Scholar] [CrossRef] [PubMed]
- Sze, D.T.; Lau, C.C.; Chan, T.-M.; Ma, E.S.; Tang, B.S. Comparison of novel rapid diagnostic of blood culture identification and antimicrobial susceptibility testing by Accelerate Pheno system and BioFire FilmArray Blood Culture Identification and BioFire FilmArray Blood Culture Identification 2 panels. BMC Microbiol. 2021, 21, 350. [Google Scholar] [CrossRef]
- Diagnostics, B. BioFire FilmArray Blood Culture Identification (BCID) Panel. Instruction Booklet. Available online: https://www.biofiredx.com/support/documents/#toggle-id-4v (accessed on 8 December 2022).
- Biomerieux. FILMArray™ BCID Panel. Available online: https://www.biomerieux-nordic.com/product/filmarray-bcid-panel (accessed on 12 December 2022).
- Verroken, A.; Despas, N.; Rodriguez-Villalobos, H.; Laterre, P.-F. The impact of a rapid molecular identification test on positive blood cultures from critically ill with bacteremia: A pre-post intervention study. PLoS ONE 2019, 14, e0223122. [Google Scholar] [CrossRef]
- Schumann, J.; Johanns, U.; Ahmad-Nejad, P.; Ghebremedhin, B.; Woebker, G. The Impact of the FilmArray-Based Detection of Microbial Pathogens from Positive Blood Culture Vials on the Time to Optimal Antimicrobial Regimen in Intensive Care Units of the Helios University Clinic Wuppertal, Germany. J. Clin. Med. 2021, 10, 5880. [Google Scholar] [CrossRef]
- Biomerieux. BACT/ALERT® VIRTUO®. Available online: https://www.biomerieux-usa.com/biomerieux-virtuo-new-generation-blood-culture-system-ce-marked (accessed on 10 December 2022).
- Biomerieux. VITEK® MS: Healthcare Microbial Identification in Minutes. Available online: https://www.biomerieux-usa.com/clinical/vitek-ms-healthcare (accessed on 12 December 2022).
- Biomerieux. VITEK® 2 AST Cards. Available online: https://www.biomerieux-diagnostics.com/vitekr-2-advanced-expert-system (accessed on 8 December 2022).
- Rule, R.; Paruk, F.; Becker, P.; Neuhoff, M.; Chausse, J.; Said, M. Diagnostic accuracy of the BioFire FilmArray blood culture identification panel when used in critically ill patients with sepsis. J. Microbiol. Methods 2021, 189, 106303. [Google Scholar] [CrossRef]
- Rule, R.; Paruk, F.; Becker, P.; Neuhoff, M.; Chausse, J.; Said, M. Clinical utility of the BioFire FilmArray Blood Culture Identification panel in the adjustment of empiric antimicrobial therapy in the critically ill septic patient. PLoS ONE 2021, 16, e0254389. [Google Scholar] [CrossRef]
- Payne, M.; Champagne, S.; Lowe, C.; Leung, V.; Hinch, M.; Romney, M.G. Evaluation of the FilmArray Blood Culture Identification Panel compared to direct MALDI-TOF MS identification for rapid identification of pathogens. J. Med. Microbiol. 2018, 67, 1253–1256. [Google Scholar] [CrossRef] [PubMed]
- BioMérieux. Urgent Field Safety Notice 4593—FSCA—BioFire FilmArray® Blood Culture Identification (BCID) Panel. Available online: https://www.hpra.ie/docs/default-source/field-safety-notices/february-2020/v42803_fsn.pdf?sfvrsn=2 (accessed on 8 December 2022).
- Kang, C.-M.; Chen, X.-J.; Chih, C.-C.; Hsu, C.-C.; Chen, P.-H.; Fen Lee, T.; Teng, L.-J.; Hsueh, P.-R. Rapid identification of bloodstream bacterial and fungal pathogens and their antibiotic resistance determinants from positively flagged blood cultures using the BioFire FilmArray blood culture identification panel. J. Microbiol. Immunol. Infect. 2020, 53, 882–891. [Google Scholar] [CrossRef]
- Ghasemnejad, A.; Doudi, M.; Amirmozafari, N. The role of the blaKPC gene in antimicrobial resistance of Klebsiella pneumoniae. Iran. J. Microbiol. 2019, 11, 288. [Google Scholar]
- Kollef, M.H.; Shorr, A.F.; Bassetti, M.; Timsit, J.-F.; Micek, S.T.; Michelson, A.P.; Garnacho-Montero, J. Timing of antibiotic therapy in the ICU. Crit. Care 2021, 25, 360. [Google Scholar] [CrossRef] [PubMed]
- Ferrer, R.; Martin-Loeches, I.; Phillips, G.; Osborn, T.M.; Townsend, S.; Dellinger, R.P.; Artigas, A.; Schorr, C.; Levy, M.M. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: Results from a guideline-based performance improvement program. Crit. Care Med. 2014, 42, 1749–1755. [Google Scholar] [CrossRef] [PubMed]
- Masterton, R.G. Antibiotic de-escalation. Crit. Care Clin. 2011, 27, 149–162. [Google Scholar] [CrossRef]
- Tabah, A.; Bassetti, M.; Kollef, M.H.; Zahar, J.-R.; Paiva, J.-A.; Timsit, J.-F.; Roberts, J.A.; Schouten, J.; Giamarellou, H.; Rello, J. Antimicrobial de-escalation in critically ill patients: A position statement from a task force of the European Society of Intensive Care Medicine (ESICM) and European Society of Clinical Microbiology and Infectious Diseases (ESCMID) Critically Ill Patients Study Group (ESGCIP). Intensive Care Med. 2020, 46, 245–265. [Google Scholar]
- Tabah, A.; Cotta, M.O.; Garnacho-Montero, J.; Schouten, J.; Roberts, J.A.; Lipman, J.; Tacey, M.; Timsit, J.-F.; Leone, M.; Zahar, J.R. A systematic review of the definitions, determinants, and clinical outcomes of antimicrobial de-escalation in the intensive care unit. Clin. Infect. Dis. 2016, 62, 1009–1017. [Google Scholar] [CrossRef] [PubMed]
- Lew, K.Y.; Ng, T.M.; Tan, M.; Tan, S.H.; Lew, E.L.; Ling, L.M.; Ang, B.; Lye, D.; Teng, C.B. Safety and clinical outcomes of carbapenem de-escalation as part of an antimicrobial stewardship program in an ESBL-endemic setting. J. Antimicrob. Chemother. 2015, 70, 1219–1225. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Control Group (n = 212) | FA-BCID Group (n = 60) | p-Value | |
|---|---|---|---|
| Demographics | |||
| Male proportion (n, %) | 116 (54.7) | 35 (58.3) | 0.6194 |
| Age, mean ± SD | 69.6 ± 15.0 | 68.4 ± 14.2 | 0.5805 |
| Location at enrollment (n, %) | 0.3623 | ||
| Outpatient clinic | 1 (0.5) | 0 (0.0) | |
| General wards | 53 (25.0) | 20 (33.3) | |
| Emergency department | 135 (63.7) | 37 (61.7) | |
| ICU | 23 (10.8) | 3 (5.0) | |
| Comorbidities, (n, %) | |||
| Charlson comorbidity score, mean ± SD | 4.9 ± 2.6 | 4.4 ± 1.9 | 0.1071 |
| Diabetes mellitus | 73 (34.4) | 25 (41.7) | 0.3038 |
| Hypertension | 99 (46.7) | 21 (35.0) | 0.1078 |
| Cardiovascular disease | 35 (16.5) | 6 (10.2) | 0.2302 |
| Cerebrovascular disease | 35 (16.5) | 9 (15.0) | 0.7795 |
| Chronic heart disease | 49 (23.1) | 14 (23.3) | 0.9716 |
| Chronic liver disease | 17 (8.0) | 4 (6.7) | 0.7295 |
| Chronic lung disease | 19 (9.0) | 3 (5.0) | 0.3212 |
| Chronic renal disease | 32 (15.1) | 7 (11.7) | 0.5044 |
| Malignant tumor | 54 (25.5) | 15 (25.0) | 0.9410 |
| Renal replacement therapy | 15 (7.1) | 3 (5.0) | 0.5688 |
| Neutropenia | 4 (1.9) | 4 (6.7) | 0.0535 |
| Chemotherapy in the prior 30 days | 15 (7.1) | 6 (10.0) | 0.4545 |
| An immunosuppressant in the prior 30 days | 1 (0.5) | 0 (0.0) | 0.5947 |
| Surgery in the prior 30 days | 42 (19.8) | 6 (10.0) | 0.0790 |
| ICU admission | 44 (20.8) | 14 (23.3) | 0.6674 |
| Bacteremia at the time of ICU stay | 41 (19.3) | 10 (16.7) | 0.6402 |
| The severity of illness (n, %) | |||
| Pitt bacteremia score, mean ± SD | 1.4 ± 2.2 | 1.5 ± 1.7 | 0.8810 |
| Requiring mechanical ventilation | 28 (13.2) | 8 (13.3) | 0.9798 |
| Septic shock | 49 (23.1) | 8 (13.3) | 0.1010 |
| Category | Target a | MALDI-TOF Positive and FA-BCID Positive (n) | MALDI-TOF Positive and FA-BCID Negative (n) | MALDI-TOF Negative and FA-BCID Positive (n) |
|---|---|---|---|---|
| Gram-negative bacteria | Acinetobacter baumannii | |||
| Enterobacteriaceae | ||||
| Enterobacter cloacae complex | ||||
| Escherichia coli | 26 | 1 | ||
| Klebsiella oxytoca | 2 | |||
| Klebsiella pneumoniae | 8 | |||
| Proteus spp. | 8 * | |||
| Serratia marcescens | ||||
| Enterobacteriaceae, except for the above six targets | 2 | |||
| Haemophilus influenza | ||||
| Neisseria meningitidis | ||||
| Pseudomonas aeruginosa | 1 | 1 | ||
| Gram-positive bacteria | Enterococcus spp. | 6 | 1 | 2 |
| Listeria monocytogenes | ||||
| Staphylococcus spp. | ||||
| Staphylococcus aureus | 7 | 1 | ||
| Staphylococcus spp. except S. aureus | 2 | |||
| Streptococcus spp. | ||||
| Streptococcus agalactiae | 2 | |||
| Streptococcus pneumoniae | 1 | |||
| Streptococcus pyogenes | ||||
| Streptococcus spp. except for the above three targets | 3 | |||
| Yeasts | Candida albicans | |||
| Candida glabrata | ||||
| Candida krusei | ||||
| Candida parapsilosis | ||||
| Candida tropicalis | 3 | |||
| Antimicrobial resistance genes | KPC | 1 | 1 | |
| mecA | 7 | |||
| vanA/vanB | ||||
| Organisms not included in the FA BCID panel. | 3 ** |
| Control Group (n = 212) | FA-BCID Group (n = 60) | p-Value | |
|---|---|---|---|
| Clinical outcomes | |||
| Disposition (n, %) | 0.1258 | ||
| Recovery | 158 (74.5) | 45 (75.0) | |
| Hopeless discharge | 18 (8.5) | 1 (1.7) | |
| Death | 36 (17.0) | 14 (23.3) | |
| Length of stay (entire hospitalization) (day, median (IQR)) | 15 (9–32.75) | 18 (8–43) | 0.7201 |
| Length of stay (after enrollment) (day, median (IQR)) | 11 (6–21) | 14 (6–31.25) | 0.3576 |
| 30-day mortality (n, %) | 30 (14.2) | 10 (16.7) | 0.6278 |
| 30-day attributable mortality (n, %) | 21 (9.9) | 6 (10.0) | 0.9828 |
| 30-day readmission for infection with the same organism (n, %) | 1 (0.5) | 1 (1.7) | 0.3325 |
| Microbiological outcome | |||
| Acquisition of C. difficile or multidrug-resistant organisms within 30 days after enrollment | 52 (24.6) | 16 (26.7) | 0.7503 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Widyasari, K.; Lee, S.; Cho, O.-H.; Hong, S.-I.; Ryu, B.-H.; Kim, S. The Significance of FilmArray Blood Culture Identification Panel (FA-BCID) for Managing Patients with Positive Blood Cultures. Diagnostics 2023, 13, 3335. https://doi.org/10.3390/diagnostics13213335
Widyasari K, Lee S, Cho O-H, Hong S-I, Ryu B-H, Kim S. The Significance of FilmArray Blood Culture Identification Panel (FA-BCID) for Managing Patients with Positive Blood Cultures. Diagnostics. 2023; 13(21):3335. https://doi.org/10.3390/diagnostics13213335
Chicago/Turabian StyleWidyasari, Kristin, Seungjun Lee, Oh-Hyun Cho, Sun-In Hong, Byung-Han Ryu, and Sunjoo Kim. 2023. "The Significance of FilmArray Blood Culture Identification Panel (FA-BCID) for Managing Patients with Positive Blood Cultures" Diagnostics 13, no. 21: 3335. https://doi.org/10.3390/diagnostics13213335
APA StyleWidyasari, K., Lee, S., Cho, O.-H., Hong, S.-I., Ryu, B.-H., & Kim, S. (2023). The Significance of FilmArray Blood Culture Identification Panel (FA-BCID) for Managing Patients with Positive Blood Cultures. Diagnostics, 13(21), 3335. https://doi.org/10.3390/diagnostics13213335