Abstract
Introduction: Risk stratification in patients with COVID-19 is a challenging task. Early warning scores (EWSs) are commonly used tools in the initial assessment of critical patients. However, their utility in patients with COVID-19 is still undetermined. Aim: This study aimed to discover the most valuable predictive model among existing EWSs for ICU admissions and mortality in COVID-19 patients. Materials and methods: This was a single-center cohort study that included 3608 COVID-19 patients admitted to the University Clinical Hospital Center Bezanijska Kosa, Belgrade, Serbia, between 23 June 2020, and 14 April 2021. Various demographic, laboratory, and clinical data were collected to calculate several EWSs and determine their efficacy. For all 3608 patients, five EWSs were calculated (MEWS, NEWS, NEWS2, REMS, and qSOFA). Model discrimination performance was tested using sensitivity, specificity, and positive and negative predictive values. C statistic, representing the area under the receiver operating characteristic (ROC) curve, was used for the overall assessment of the predictive model. Results: Among the evaluated prediction scores for 3068 patients with COVID-19, REMS demonstrated the highest diagnostic performance with the sensitivity, PPV, specificity, and NPV of 72.1%, 20.6%, 74.9%, and 96.8%, respectively. In the multivariate logistic regression analysis, aside from REMS, age (p < 0.001), higher CT score (p < 0.001), higher values of urea (p < 0.001), and the presence of bacterial superinfection (p < 0.001) were significant predictors of mortality. Conclusions: Among all evaluated EWSs to predict mortality and ICU admission in COVID-19 patients, the REMS score demonstrated the highest efficacy.
1. Introduction
COVID-19 is a highly contagious disease caused by the SARS-CoV-2 virus. SARS-CoV-2 is easily spread and can cause a wide specter of diseases, from asymptomatic to acute respiratory failure and death. During the pandemic, healthcare workers face many challenges including recognition of those patients in greatest need of medical attention [1].
As a consequence of the large number of in-hospital patients with COVID-19 and limited health resources, the most important objective in clinical practice is to find the appropriate scoring system to evaluate those at higher risk of complications and lethal outcomes. There are many predictive factors including demographic, radiographic and laboratory parameters, but only a few of them can help in the early identification of patients at risk. Until now, it is demonstrated that cytokine regulation, inflammatory response, and micro- and macro-thromboembolic complications are the main pathophysiological mechanisms involved in poor clinical outcomes of patients with COVID-19 [2,3].
There is a complex network of regulatory mechanisms with an assignment to balance the production of pro-inflammatory and anti-inflammatory cytokines so that the reaction remains limited and sufficient for pathogenic noxa. The failure of one or more of these mechanisms can induce immune system overactivation and massive production of cytokines initiating a systemic inflammatory reaction with harmful consequences, which is widely known as a cytokine storm. A cytokine storm mainly displays as an influenza-like syndrome that may evolve or be complicated by multi-organ damage. For example, tachypnea and hypoxemia as symptoms are often present and can evolve into acute respiratory distress syndrome (ARDS), which is one of the most dangerous complications of COVID-19 infection [4]. Most deaths from COVID-19 ARDS have evidence of thrombotic disseminated intravascular coagulation. Coagulation dysfunction is regularly seen in COVID-19 and is detected by elevated D-dimer levels. Sadly, many cases with coagulation dysfunction have fatal outcomes where diffuse microvascular thrombosis is seen, suggesting thrombotic microangiopathy [5,6].
Having in mind the unpredictability of the disease and various pathophysiological mechanisms involved, making a proper risk stratification tool is a challenging task. Over time, various scores have been developed that are routinely used in community-acquired pneumonia and other conditions. Certain studies evaluated the diagnostic performance of these early warning scores (EWSs) in patients with COVID-19 but with controversial results. Martin-Rodriguez et al. demonstrated the best predictive capacity of NEWS2 early warning score, where patients with the score equal to or greater than 8 points had a high risk of clinical deterioration and a very high risk of two-day mortality [7]. The other study by Tsai et al. indicated that REMS score was superior to NEWS and MEWS for predicting the in-hospital mortality of COVID-19 patients [8]. In a study on 1501 patients, Veldhuis et al. reported that NEWS2 and the Quick COVID-19 Severity Index Score had the best diagnostic performance to predict ICU admission in COVID-19 patients [9]. As the COVID-19 pandemic progressed, the main focus was changed from more generic predictive scores to newly designed ones for patients with COVID-19 [10]. However, several predictive scores have been published, but only a few of them had been validated externally. Thus, the worldwide applicability of these prediction scores is still an unresolved question. All around the world, healthcare systems and patients profiles differ, which can impact these scores. Most of the scores have been validated in small populations, with a specific ethnic characterization, and do not appear to be effectively generalizable among different contexts [11].
Although there are no specific predictive scores for COVID-19, we mainly focused our research on early warning scores—EWSs. The EWSs were commonly used in an initial assessment of critical patients to help emergency physicians recognize those patients at greatest risk [2].
In this single-center study, we aimed to discover the most valuable predictive model among existing EWSs for ICU admissions and mortality in COVID-19 patients.
2. Materials and Methods
This is a single-center cohort study that included 3608 COVID-19 patients admitted to the University Clinical Hospital Center Bezanijska kosa, Belgrade, Serbia, between June 23, 2020 and April 14, 2021. The cohort included patients older than 18 years old with confirmed COVID-19 infection by positive real-time reverse-transcription polymerase chain reaction (RT-PCR) assay or antigen testing using nasal and pharyngeal swab specimens with clinical, radiographic or/and laboratory parameters that require hospitalization. The University Clinical Hospital Center Bezanijska kosa was one of the COVID-19 referent triage centers that treated more than 1000 patients per month and more than 100 patients in the ICU. Chest radiography (CXR) was performed on the day of admission and regularly controlled when needed. Chest CT to determine the severity of COVID-19 pneumonia was mandatory on admission day. The second control, CT chest, was indicated in patients with clinical signs of deterioration. The main criteria for ICU admission were radiographic, clinical and laboratory worsening, and oxygen saturation lower than 93% despite maximum oxygen support.
2.1. Data Collection
2.1.1. Demographic, Anthropometric Data, Laboratory and Clinically Significant Parameters
The data were collected through medical documentation and the hospital’s health informational system (Heliant, v7.3, r48602). Demographic data (age, gender, and BMI), past medical history (hypertension, diabetes mellitus, COPD, coronary heart disease, heart failure, and chronic kidney disease), laboratory values (IL-6, CRP, PCT, ferritin, D-dimer, serum albumin, lymphocytes, thrombocytes, prothrombin time, activated partial thromboplastin time, and fibrinogen), and CT severity score were analyzed. Clinical and laboratory parameters were followed upon admission to the hospital (GCS, respiratory and hemodynamic parameters). These parameters were obtained by doctors or emergency registered nurses. Collected data were used to calculate prognostic scores (all variables included in the scores are presented in Supplemental Table S1).
2.1.2. Prognostic Scores
For all 3608 patients, 5 early warning scores were calculated (MEWS, NEWS, NEWS2, REMS, and qSOFA). Parameters for every score, scoring system, and prognostic value are provided in Supplemental Table S1.
2.1.3. COVID-19 Treatment
Patients were treated by the National Protocol of the Republic of Serbia for the treatment of COVID-19 infection and in concordance with the protocol suggested by the World Health Organization (WHO).
2.1.4. Statistical Analysis
Numerical data were presented as mean with standard deviation or median with 25th and 75th percentiles. Categorical variables were summarized by absolute numbers with percentages. Differences between survivors and non-survivors were analyzed by Student’s t-test, Mann–Whitney U-test and Chi-square test for numerical and categorical data, respectively. Model discrimination performance was tested using sensitivity, specificity, and positive and negative predictive values. C statistic, representing the area under the receiver operating characteristic (ROC) curve, was used for an overall assessment of the predictive model. Univariate and multivariate logistic regression models were used to assess predictors of outcome as dependent variables. Significant variables from univariate analysis were included in multivariate regressions. Results were expressed as odds ratios (OR) and their corresponding 95% confidence intervals (CI). In all analyses, the significance level was set at 0.05. Statistical analysis was performed using IBM SPSS statistical software (SPSS for Windows, release 25.0, SPSS, Chicago, IL, USA).
2.1.5. Ethics
The study was organized according to the principles of the Declaration of Helsinki of 1975, as revised in 2008 and approved by the Ethics Committee of the University Clinical Hospital Center “Bezanijska kosa”.
3. Results
3.1. Baseline Characteristics
A total of 3608 patients with COVID-19 infection were included in the study. Women (p = 0.035), older patients (p < 0.001), patients with comorbidities (p < 0.001), such as hypertension (p < 0.001), diabetes mellitus (p < 0.001), COPD (p = 0.003), coronary artery disease (p < 0.001), cardiomyopathy (p < 0.001) and malignancies (p < 0.001) more often had negative outcome. Sociodemographic characteristics and comorbidities of the study population according to outcome are presented in Table 1.

Table 1.
Sociodemographic characteristics and comorbidities of the study population according to outcome.
3.2. Radiographic Findings and Clinical Parameters of the Study Group according to Outcome
Patients more often had negative outcomes if they had bilateral pneumonia (p = 0.005), had a higher CT score (p < 0.001), were admitted to the ICU (p < 0.001), were on NIV/IMV (p < 0.001), had hospital-acquired pneumonia (p < 0.001), moreover ventilator-associated pneumonia (p < 0.001), had bacterial superinfection (p < 0.001), had ARDS (p < 0.001) or were on corticosteroid therapy (p < 0.001). Radiographic findings, need for oxygen support, hospital-acquired pneumonia and superinfection, ARDS and administrated therapy according to outcome are presented in Table 2.
Table 2.
Radiographic findings, need for oxygen support, hospital-acquired pneumonia and superinfection, ARDS and therapy according to outcome.
3.3. Laboratory Parameters of the Study Group according to Outcome
Table 3 presents the laboratory parameters of the study population according to outcome.
Table 3.
Laboratory parameters of the study population according to outcome.
3.4. Glasgow Coma Score, Pulmonary and Hemodynamic Parameters
Patients with Glasgow Coma Score <15 (p < 0.001), FiO2 at admission >21 (p < 0.001), increased number of respirations (p < 0.001), lower oxygen saturation (p < 0.001) and diastolic blood pressure (p < 0.001), lower MAP (p < 0.001) and higher heart rate (p < 0.001) more often had negative outcomes (Table 4).
Table 4.
Glasgow Coma Score, pulmonary and hemodynamic parameters of the study population according to outcome.
3.5. Early Warning Scores (EWS) if the Study Group according to Outcome
Patients with higher MEWS (p < 0.001), NEWS (p < 0.001), NEWS2 (p < 0.001), REMS (p < 0.001) and qSOFA (p < 0.001) scores more often had negative outcome. Table 5 presents the prediction scores of the study population according to outcome.
Table 5.
Prediction scores of the study population according to outcome.
3.6. Diagnostic Performance of Early Warning Scores in the Study Group
The diagnostic performance of prediction scores used to predict mortality was tested. The sensitivity, PPV, specificity, and NPV of REMS were 72.1%, 20.6%, 74.9%, and 96.8%, respectively. Measures of diagnostics accuracy of other prediction scores are shown in Table 6.
Table 6.
Measures of diagnostics accuracy of prediction scores.
Based on the ROC curve analysis (Figure 1), the area under the curve (AUC) value for MEWS was 0.662, while for NEWS, it was 0.695, for NEWS2, it was 0.572, for REMS, it was 0.800 and for qSOFA, the AUC value was 0.626 (p < 0.001 for all). In Figure 1, an ROC analysis of the prediction scores is presented.
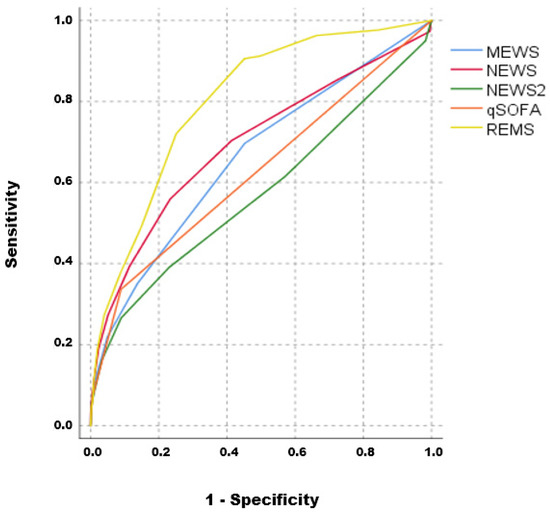
Figure 1.
ROC analysis of prediction scores; AUC: MEWS = 0.662; NEWS = 0.695; NEWS2 = 0.572; REMS = 0.800; qSOFA = 0.626.
3.7. Multivariate Logistic Regression Analysis
All variables significant in univariate logistic regression analysis were used in a multivariate model. Age (p < 0.001), higher CT score (p < 0.001), higher values of urea (p < 0.001), presence of bacterial superinfection (p < 0.001) and higher REMS score were significant independent predictors of mortality. Table 7 shows multivariate logistic regression analysis with outcome as a dependent variable.
Table 7.
Multivariate logistic regression analysis with outcome as a dependent variable.
4. Discussion
In the present study, we determined the prognostic utility of different risk scores in predicting negative outcomes among COVID-19 patients. Between several identified predictors of mortality, age, CT score, urea levels, and the presence of bacterial superinfection were marked as the most significant in the multivariate logistic regression analysis. Regarding the predictive scores, REMS score was identified as the independent predictor of mortality, with the highest sensitivity and specificity among all evaluated scores (MEWS, NEWS, NEWS2, qSOFA).
Up to this point, several EWS models have been developed in predicting in-hospital mortality and the risk of ICU admission [12,13]. Although the significance of these scores has been proven in different conditions, the prognostic utility of these scores in patients with COVID-19 is yet to be determined.
MEWS is based on four physiological parameters and one observation—systolic blood pressure, heart rate, respiratory rate, temperature and APVU (Alert, Voice, Pain, Unresponsive) score [14]. A total score of 5 or more is likely to be associated with a higher incidence of admission to an intensive care unit or death. The advantage of MEWS over other scores, mainly SOFA and qSOFA, is the inclusion of temperature, respiratory rate, oxygen therapy, and oxygen saturation, which are important parameters in patients with COVID-19. Barnett et al. presented an adjusted MEWS score to predict in-hospital mortality in patients with COVID-19 by implementing additional respiratory parameters to increase sensitivity and specificity (CEWS) [15].
NEWS (National Early Warning Score) determines the degree of illness of a patient using six physiological findings and one observation [16]. In comparison with MEWS, it includes oxygen saturation and supplemental oxygen support. There is a lack of evidence regarding the significance of this score in COVID-19 patients, as the adjusted NEWS2 score was predominantly used in studies with COVID-19 patients [17].
NEWS2 (National Early Warning Score 2) is an updated version of the original NEWS. NEWS2 has incorporated parameters for respiratory insufficiency, involving the partial pressure of CO2, in comparison with the standard NEWS score [18]. Veldhuis et al. showed that NEWS2 ≥6 discriminated COVID-19 patients needing ICU admission with 78.1% sensitivity and 56.3% specificity, which is higher compared to our cohort, but with a significantly lower study sample size [9]. Although the predictive power of this score was proven in our study, the NEWS2 score showed the lowest sensitivity and specificity among the evaluated scores. Certain studies were evaluating the efficacy of the initial score and maximum score in predicting poor outcomes, having in mind the unpredictability of the COVID-19 clinical course [19,20]. The risk of mortality and admission to ICU was also related to the change from baseline to maximum score, showing good predictability of the score regarding the short-term (2-day) mortality [21].
REMS (Rapid Emergency Medicine Score) is a composite score consisting of the Glasgow Coma Score (GCS), respiratory rate, oxygen saturation, mean arterial pressure (MAP), hazard ratio, and age [22]. All of the parameters are scored with grades from 0 to 4 with a maximum score of 26. This score is easy to implement into everyday clinical practice, as it combines standard parameters in evaluating patients’ conditions, without the need for certain extra procedures or laboratory parameters. It is superior in predicting in-hospital mortality and non-inferior to some other commonly used scores (APACHE-II and RASP score) [23]. Imhoff et al. validated the REMS in a retrospective study and found that a 1-point increase on the 26-point REMS scale was associated with an odds ratio of 1.40 for in-hospital death [24]. The superiority of REMS over other predictive scores might have been because of age as a component. It is shown that the analyses of patients older than 70 years demonstrated a better diagnostic and discrimination capacity of EDWs for both mortality outcomes than in younger patients [25]. This is important to underline, as age was an independent predictor of mortality in our study cohort, while REMS showed the highest sensitivity and specificity among evaluated scores (72.1 and 74.9%, respectively), with the highest negative predictive value of 96.8. Certain studies also proved the prognostic significance of this score in patients with COVID-19 [26]. Ruangsomboon et al. concluded that REMS had the highest prognostic utility as it outperformed qSOFA, MEWS, and NEWS in predicting in-hospital mortality in COVID-19 patients [27].
qSOFA (quick SOFA score) identifies high-risk patients for in-hospital mortality with suspected infection outside the ICU [28]. It incorporates systolic blood pressure, respiratory rate and GSC, and it is scored with a maximum of 3 points. A score greater than or equal to 2 represents a greater risk of a fatal outcome. Previous studies demonstrated excellent results in predicting in-hospital mortality in patients with COVID-19 [27,29]. It is shown that patients with a qSOFA score above 2 have an 11-fold higher mortality risk compared to patients with a score below 2 [28,30]. However, this score cannot be used to assume short-term stable or noncritical disease status in COVID-19, which is mainly because of its low sensitivity.
The development of COVID-19-dedicated risk scores to predict poor clinical outcomes was also an important task in several studies. Zdravkovic et al. developed a simple and effective score to predict mortality in patients admitted to ICU [31]. The score has a high discriminative value with a sensitivity of 82.4% (95% CI 76.7% to 87.1%), a specificity of 41.0%, and C statistic of 0.863. It is easy to implement into everyday clinical practice, as it includes four important parameters (age, IL-6, D-dimer, and serum albumin), reflecting the main pathophysiological mechanisms of the disease (inflammation, thromboembolism and cytokine storm).
The present study has some limitations to be taken into account. Considering that this is a single-center study, additional multicenter prospective studies are needed to validate the predictive accuracy of the evaluated scores. However, the study sample size included almost 4000 patients. The impact of vaccination is also undetermined, as the majority of the population did not finish the immunization until the end of the study period.
5. Conclusions
Among evaluated, widely used, early warning risk scores to predict mortality and ICU admission among COVID-19 patients, all evaluated predictive scores (MEWS, NEWS, NEWS2, REMS, qSOFA) showed significant diagnostic performance, with REMS being the most sensitive and specific. Larger, multicenter studies are needed to provide definitive evidence of the prognostic value of these scores in everyday clinical practice. Having in mind the variations in diagnostic performance of already derived early warning scores, the development of new, COVID-19 dedicated risk scores is mandatory. This can provide more sufficient risk stratification, less consumption of health care resources, and better clinical outcomes not only in terms of COVID-19 disease but also in terms of other diseases with global impact.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/diagnostics13162653/s1, Supplemental Table S1. Scoring and interpretation of evaluated Early Warning Scores (EWS).
Author Contributions
Conceptualization, M.B. (Marija Brankovic) and M.Z.; methodology, V.P. and S.N.; formal analysis, M.D., M.B. (Marija Brankovic) and A.S.; data curation, M.S., A.R. and L.M.-D.; writing—original draft preparation, M.B. (Milica Brajkovic) and V.P.; writing—review and editing, M.B. (Milica Brajkovic), N.R. and N.M.; supervision, M.V., S.T. and Z.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of the University Hospital Medical Center Bezanijska kosa (protocol code 5197/2, date of approval 21 March 2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author (MZ) upon reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Knight, S.R.; Harrison, E.M. Risk stratification of patients with COVID-19 in the community. Lancet Digit. Health 2022, 4, e628–e629. [Google Scholar] [CrossRef]
- Hu, H.; Yao, N.; Qiu, Y. Predictive Value of 5 Early Warning Scores for Critical COVID-19 Patients. Disaster Med. Public Health Prep. 2020, 16, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Cruz, A.S.; Mendes-Frias, A.; Oliveira, A.I.; Dias, L.; Matos, A.R.; Carvalho, A.; Capela, C.; Pedrosa, J.; Gil Castro, A.; Silvestre, R. Interleukin-6 Is a Biomarker for the Development of Fatal Severe Acute Respiratory Syndrome Coronavirus 2 Pneumonia. Front. Immunol. 2021, 12, 613422. [Google Scholar] [CrossRef] [PubMed]
- Zanza, C.; Romenskaya, T.; Manetti, A.C.; Franceschi, F.; La Russa, R.; Bertozzi, G.; Maiese, A.; Savioli, G.; Volonnino, G.; Longhitano, Y. Cytokine Storm in COVID-19: Immunopathogenesis and Therapy. Medicina 2022, 58, 144. [Google Scholar] [CrossRef] [PubMed]
- Al Sulaiman, K.; Aljuhani, O.; Badreldin, H.A.; Korayem, G.B.; Alenazi, A.A.; Alharbi, A.H.; Alghamdi, A.; Alhubaishi, A.; Altebainawi, A.F.; Bosaeed, M.; et al. The clinical outcomes of COVID-19 critically ill patients co-infected with other respiratory viruses: A multicenter, cohort study. BMC Infect Dis. 2023, 23, 75. [Google Scholar]
- Gibson, P.G.; Qin, L.; Puah, S.H. COVID-19 acute respiratory distress syndrome (ARDS): Clinical features and differences from typical pre-COVID-19 ARDS. Med. J. Aust. 2020, 213, 54–56.e1. [Google Scholar] [CrossRef]
- Martín-Rodríguez, F.; Martín-Conty, J.L.; Sanz-García, A.; Rodríguez, V.C.; Rabbione, G.O.; Ruíz, I.C.; Ramos, J.R.O.; Portillo, E.C.; Polonio-López, B.; Gambarra, R.E.d.S.; et al. Early Warning Scores in Patients with Suspected COVID-19 Infection in Emergency Departments. J. Pers. Med. 2021, 11, 170. [Google Scholar] [CrossRef]
- Tsai, W.; Chen, C.; Jo, S.-Y.; Hsiao, C.-H.; Chien, D.-K.; Chang, W.-H.; Chen, T.-H. Evaluation of Early Warning Scores on In-Hospital Mortality in COVID-19 Patients: A Tertiary Hospital Study from Taiwan. Medicina 2023, 59, 464. [Google Scholar] [CrossRef]
- Veldhuis, L.; Ridderikhof, M.L.; Schinkel, M.; van den Bergh, J.; Beudel, M.; Dormans, T.; Douma, R.; Oever, N.G.v.D.; de Haan, L.; Koopman, K.; et al. Early warning scores to assess the probability of critical illness in patients with COVID-19. Emerg. Med. J. 2021, 38, 901–905. [Google Scholar] [CrossRef]
- Innocenti, F.; De Paris, A.; Lagomarsini, A.; Pelagatti, L.; Casalini, L.; Gianno, A.; Montuori, M.; Bernardini, P.; Caldi, F.; Tassinari, I.; et al. Stratification of patients admitted for SARS-CoV2 infection: Prognostic scores in the first and second wave of the pandemic. Intern. Emerg. Med. 2022, 17, 2093–2101. [Google Scholar] [CrossRef]
- Lombardi, Y.; Azoyan, L.; Szychowiak, P.; Bellamine, A.; Lemaitre, G.; Bernaux, M.; Daniel, C.; Leblanc, J.; Riller, Q.; Steichen, O.; et al. External validation of prognostic scores for COVID-19: A multicenter cohort study of patients hospitalized in Greater Paris University Hospitals. Intensive Care Med. 2021, 47, 1426–1439. [Google Scholar] [CrossRef]
- Gerry, S.; Bonnici, T.; Birks, J.; Kirtley, S.; Virdee, P.S.; Watkinson, P.J.; Collins, G.S. Early warning scores for detecting deterioration in adult hospital patients: Systematic review and critical appraisal of methodology. BMJ 2020, 369, m1501. [Google Scholar] [CrossRef]
- Fu, L.-H.; Schwartz, J.; Moy, A.; Knaplund, C.; Kang, M.-J.; Schnock, K.O.; Garcia, J.P.; Jia, H.; Dykes, P.C.; Cato, K.; et al. Development and validation of early warning score system: A systematic literature review. J. Biomed. Inform. 2020, 105, 103410. [Google Scholar] [CrossRef] [PubMed]
- Mitsunaga, T.; Hasegawa, I.; Uzura, M.; Okuno, K.; Otani, K.; Ohtaki, Y.; Sekine, A.; Takeda, S. Comparison of the National Early Warning Score (NEWS) and the Modified Early Warning Score (MEWS) for predicting admission and in-hospital mortality in elderly patients in the pre-hospital setting and in the emergency department. PeerJ 2019, 7, e6947. [Google Scholar] [CrossRef] [PubMed]
- Barnett, W.R.; Radhakrishnan, M.; Macko, J.; Hinch, B.T.; Altorok, N.; Assaly, R. Initial MEWS score to predict ICU admission or transfer of hospitalized patients with COVID-19: A retrospective study. J. Infect. 2020, 82, 282–327. [Google Scholar] [CrossRef]
- Thorén, A.; Joelsson-Alm, E.; Spångfors, M.; Rawshani, A.; Kahan, T.; Engdahl, J.; Jonsson, M.; Djärv, T. The predictive power of the National Early Warning Score (NEWS) 2, as compared to NEWS, among patients assessed by a Rapid response team: A prospective multi-centre trial. Resusc. Plus 2022, 9, 100191. [Google Scholar] [CrossRef] [PubMed]
- Kostakis, I.; Smith, G.B.; Prytherch, D.; Meredith, P.; Price, C.; Chauhan, A.; Portsmouth Academic Consortium for Investigating COVID-19 (PACIFIC-19). The performance of the National Early Warning Score and National Early Warning Score 2 in hospitalised patients infected by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Resuscitation 2021, 159, 150–157. [Google Scholar] [CrossRef]
- Smith, G.; Redfern, O.; Pimentel, M.; Gerry, S.; Collins, G.; Malycha, J.; Prytherch, D.; Schmidt, P.; Watkinson, P. The National Early Warning Score 2 (NEWS2). Clin. Med. 2019, 19, 260. [Google Scholar] [CrossRef]
- Williams, B. Evaluation of the utility of NEWS2 during the COVID-19 pandemic. Clin. Med. 2022, 22, 539–543. [Google Scholar]
- Carr, E.; Bendayan, R.; Bean, D.; Stammers, M.; Wang, W.; Zhang, H.; Searle, T.; Kraljevic, Z.; Shek, A.; Phan, H.T.T.; et al. Evaluation and improvement of the National Early Warning Score (NEWS2) for COVID-19: A multi-hospital study. BMC Med. 2021, 19, 1–16. [Google Scholar] [CrossRef]
- Baker, K.F.; Hanrath, A.T.; van der Loeff, I.S.; Kay, L.J.; Back, J.; Duncan, C.J. National Early Warning Score 2 (NEWS2) to identify inpatient COVID-19 deterioration: A retrospective analysis. Clin. Med. 2021, 21, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Bidari, A.; Talachian, E. Rapid Emergency Medicine Score (REMS) As a Predictor of Early Mortality in the Setting of Emergency Department. Iran J. Med. Sci. 2022, 47, 81–82. [Google Scholar]
- Haruna, J.; Tatsumi, H.; Kazuma, S.; Kuroda, H.; Goto, Y.; Aisaka, W.; Terada, H.; Sonoda, T.; Masuda, Y. Comparison of the National Early Warning Scores and Rapid Emergency Medicine Scores with the APACHE II Scores as a Prediction of Mortality in Patients with Medical Emergency Team Activation: A Single-centre Retrospective Cohort Study. J. Crit. Care Med. 2021, 7, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Imhoff, B.F.; Thompson, N.J.; Hastings, M.A.; Nazir, N.; Moncure, M.; Cannon, C.M. Rapid Emergency Medicine Score (REMS) in the trauma population: A retrospective study. BMJ Open 2014, 4, e004738. [Google Scholar] [CrossRef] [PubMed]
- Vahdati, S.S.; Jalali, M.; Parsay, S.; Ala, A. Rapid Emergency Medicine Score as a Predictive Value for 30-day Outcome of Nonsurgical Patients Referred to the Emergency Department. Indian J. Crit. Care Med. 2020, 24, 418–422. [Google Scholar] [CrossRef] [PubMed]
- Bourn, S.S.; Crowe, R.P.; Fernandez, A.R.; Matt, S.E.; Brown, A.L.; Hawthorn, A.B.; Myers, J.B. Initial prehospital Rapid Emergency Medicine Score (REMS) to predict outcomes for COVID-19 patients. J. Am. Coll. Emerg. Physicians Open 2021, 2, e12483. [Google Scholar] [CrossRef]
- Ruangsomboon, O.; Phanprasert, N.; Jirathanavichai, S.; Puchongmart, C.; Boonmee, P.; Thirawattanasoot, N.; Dorongthom, T.; Praphruetkit, N.; Monsomboon, A. The utility of the Rapid Emergency Medicine Score (REMS) compared with three other early warning scores in predicting in-hospital mortality among COVID-19 patients in the emergency department: A multicenter validation study. BMC Emerg. Med. 2023, 23, 1–10. [Google Scholar] [CrossRef]
- Alencar, J.; Gómez, L.M.G.; Cortez, A.L.; de Souza, H.P.; Levin, A.S.; Salomão, M.C. Performance of NEWS, qSOFA, and SIRS Scores for Assessing Mortality, Early Bacterial Infection, and Admission to ICU in COVID-19 Patients in the Emergency Department. Front. Med. 2022, 9, 779516. [Google Scholar] [CrossRef] [PubMed]
- Raith, E.P.; Udy, A.A.; Bailey, M.; McGloughlin, S.; MacIsaac, C.; Bellomo, R.; Pilcher, D.V.; Australian and New Zealand Intensive Care Society (ANZICS) Centre for Outcomes and Resource Evaluation (CORE). Prognostic Accuracy of the SOFA Score, SIRS Criteria, and qSOFA Score for In-Hospital Mortality among Adults with Suspected Infection Admitted to the Intensive Care Unit. JAMA 2017, 317, 290–300. [Google Scholar] [CrossRef]
- Ys, A.; Ravi, K. Comparison of Quick Sequential Organ Failure Assessment (Qsofa) and National Early Warning Score (News) in Covid-19 Patients and its Correlation with the Outcome. J. Assoc. Physicians India 2022, 70, 11–12. [Google Scholar] [PubMed]
- Zdravkovic, M.; Popadic, V.; Klasnja, S.; Pavlovic, V.; Aleksic, A.; Milenkovic, M.; Crnokrak, B.; Balint, B.; Todorovic-Balint, M.; Mrda, D.; et al. Development and Validation of a Multivariable Predictive Model for Mortality of COVID-19 Patients Demanding High Oxygen Flow at Admission to ICU: AIDA Score. Oxidative Med. Cell. Longev. 2021, 2021, 6654388. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).