

Eosinophilic Esophagitis: Cytokines Expression and Fibrotic Markers in Comparison to Celiac Disease

 ,
,
Abstract
1. Introduction
2. Materials and Methods
3. Total RNA Extraction
4. Quantitative Real-Time PCR
5. Statistical Analysis
6. Results
7. mRNA Expression Analysis
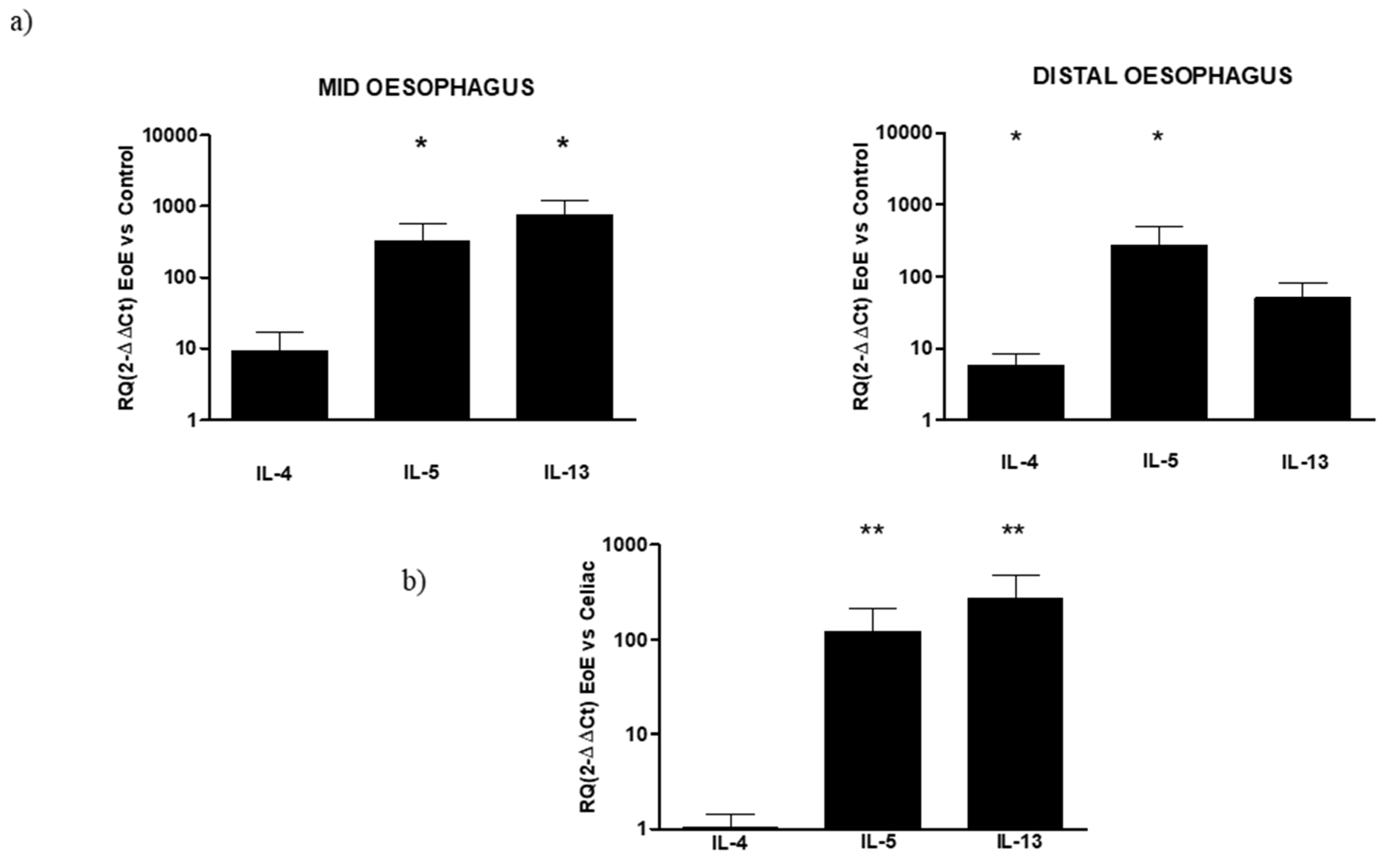
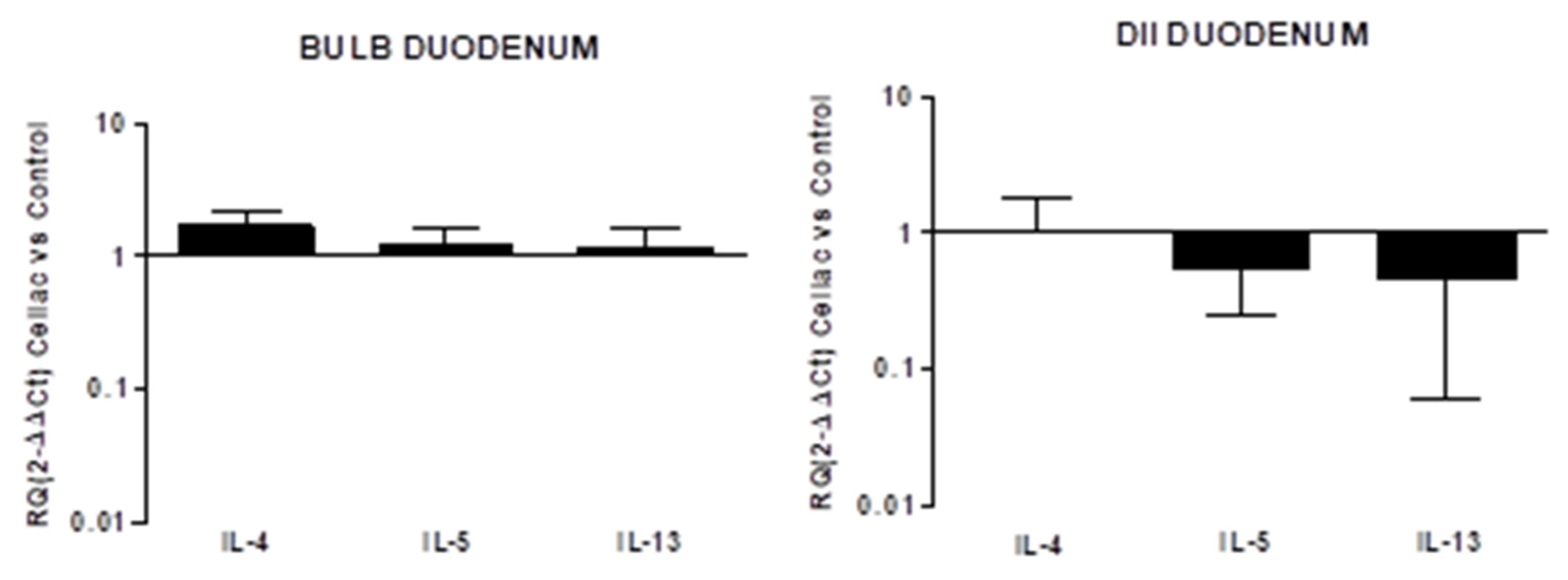
- (a)
- Inflammatory cytokines
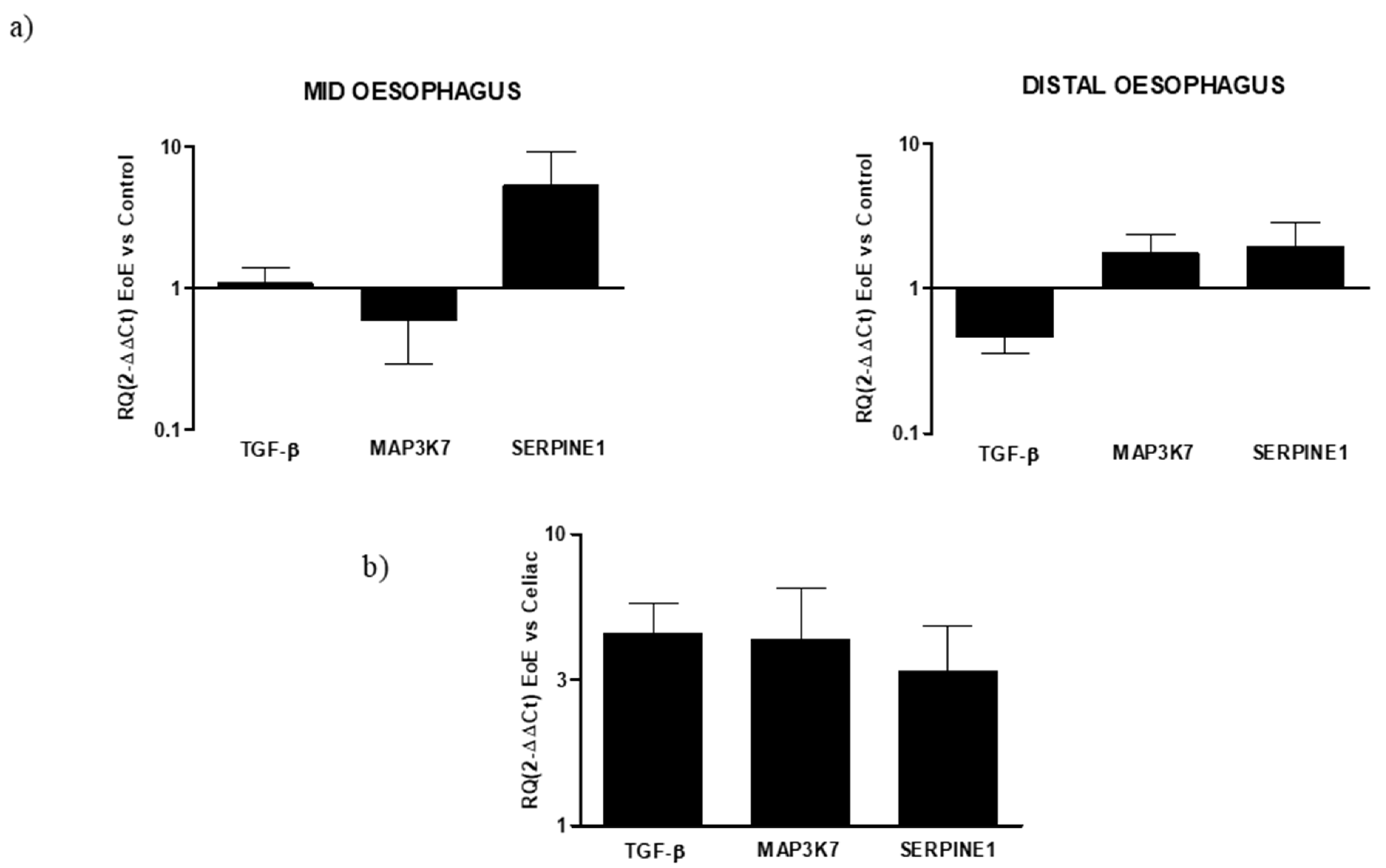
- (b)
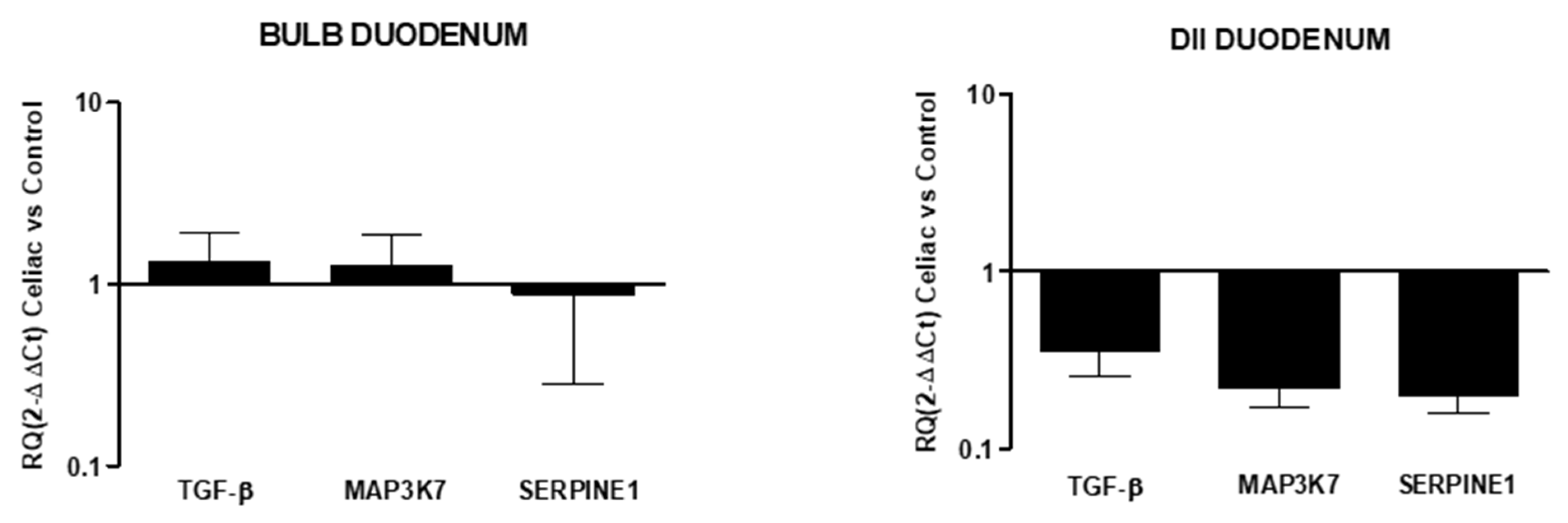
- Pro-fibrogenic mediators
- (c)
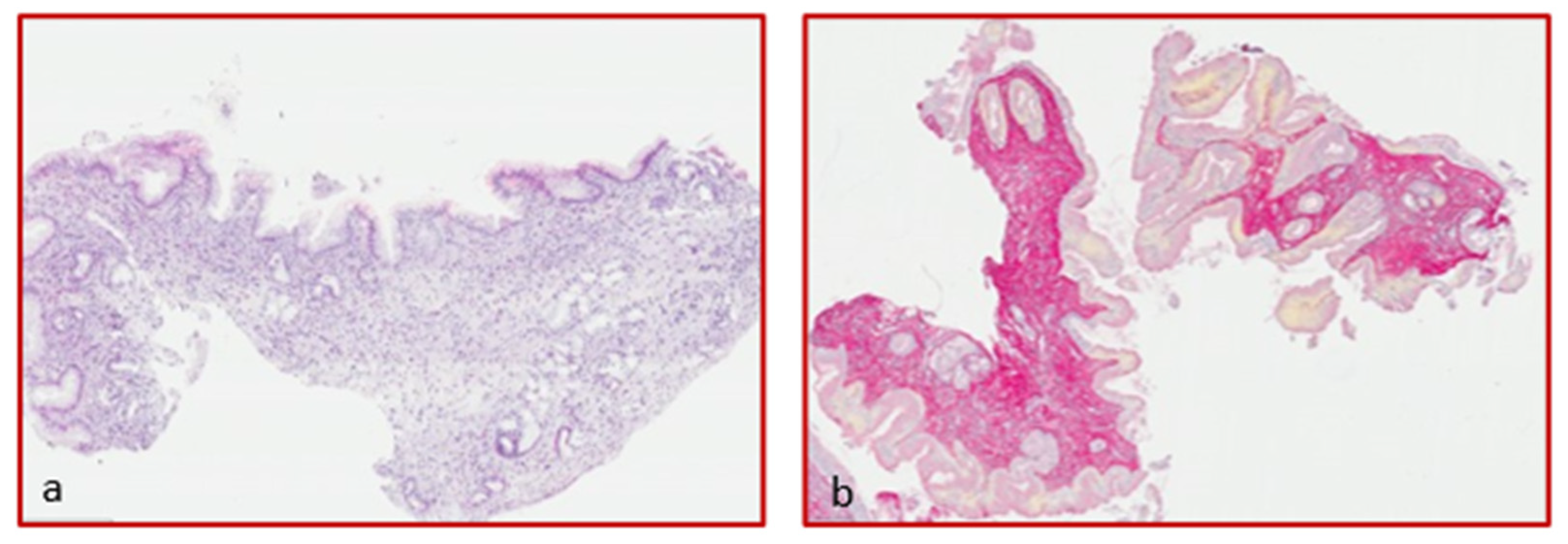
- Collagen deposition quantification
8. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liacouras, C.A.; Furuta, G.T.; Hirano, I.; Atkins, D.; Attwood, S.E.; Bonis, P.A.; Burks, A.W.; Chehade, M.; Collins, M.H.; Dellon, E.S.; et al. Eosinophilic esophagitis: Updated consensus recommendations for children and adults. J. Allergy Clin. Immunol. 2011, 128, 3–20.e6. [Google Scholar] [CrossRef] [PubMed]
- Furuta, G.T.; Katzka, D.A. Eosinophilic Esophagitis. N. Engl. J. Med. 2015, 373, 1640. [Google Scholar] [CrossRef] [PubMed]
- Sgouros, S.N.; Bergele, C.; Mantides, A. Eosinophilic esophagitis in adults: A systematic review. Eur. J. Gastroenterol. Hepatol. 2006, 18, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Pasha, S.F.; DiBaise, J.K.; Kim, H.J.; de Petris, G.; Crowell, M.; Fleischer, D.E.; Sharma, V.K. Patient characteristics, clinical, endoscopic, and histologic findings in adult eosinophilic esophagitis: A case series and systematic review of the medical literature. Dis. Esophagus 2007, 20, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Prasad, G.A.; Talley, N.J.; Romero, Y.; Arora, A.S.; Kryzer, L.A.; Smyrk, T.C.; Alexander, J.A. Prevalence and Predictive Factors of Eosinophilic Esophagitis in Patients Presenting with Dysphagia: A Prospective Study. Am. J. Gastroenterol. 2007, 102, 2627–2632. [Google Scholar] [CrossRef]
- García-Compeán, D.; González, J.A.G.; García, C.A.M.; Gutiérrez, J.P.F.; Quintana, O.B.; Rodríguez, G.G.; Ruiz, M.A.M.; Valdez, D.D.L.; Quintana, J.O.J.; Garza, H.J.M. Prevalence of eosinophilic esophagitis in patients with refractory gastroesophageal reflux disease symptoms: A prospective study. Dig. Liver Dis. 2011, 43, 204–208. [Google Scholar] [CrossRef]
- Mackenzie, S.H.; Go, M.; Chadwick, B.; Thomas, K.; Fang, J.; Kuwada, S.; Lamphier, S.; Hilden, K.; Peterson, K. Eosinophilic oesophagitis in patients presenting with dysphagia—A prospective analysis. Aliment. Pharmacol. Ther. 2008, 28, 1140–1146. [Google Scholar] [CrossRef]
- Rieder, F.; Nonevski, I.; Ma, J.; Ouyang, Z.; West, G.; Protheroe, C.; de Petris, G.; Schirbel, A.; Lapinski, J.; Goldblum, J.; et al. T-Helper 2 Cytokines, Transforming Growth Factor β1, and Eosinophil Products Induce Fibrogenesis and Alter Muscle Motility in Patients with Eosinophilic Esophagitis. Gastroenterology 2014, 146, 1266–1277.e9. [Google Scholar] [CrossRef]
- Blanchard, C.; Stucke, E.M.; Burwinkel, K.; Caldwell, J.M.; Collins, M.H.; Ahrens, A.; Buckmeier, B.K.; Jameson, S.C.; Greenberg, A.; Kaul, A.; et al. Coordinate Interaction between IL-13 and Epithelial Differentiation Cluster Genes in Eosinophilic Esophagitis. J. Immunol. 2010, 184, 4033–4041. [Google Scholar] [CrossRef]
- Zuo, L.; Fulkerson, P.C.; Finkelman, F.D.; Mingler, M.; Fischetti, C.A.; Blanchard, C.; Rothenberg, M.E. IL-13 induces esophageal remodeling and gene expression by an eosino-phil-independent, IL-13R alpha 2-inhibited pathway. J. Immunol. 2010, 185, 660. [Google Scholar] [CrossRef]
- Zhu, X.; Wang, M.; Mavi, P.; Rayapudi, M.; Pandey, A.K.; Kaul, A.; Putnam, P.E.; Rothenberg, M.E.; Mishra, A. Interleukin-15 Expression Is Increased in Human Eosinophilic Esophagitis and Mediates Pathogenesis in Mice. Gastroenterology 2010, 139, 182–193.e7. [Google Scholar] [CrossRef]
- Furuta, G.T.; Straumann, A. Review article: The pathogenesis and management of eosinophilic oesophagitis. Aliment. Pharmacol. Ther. 2006, 24, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J. T helper 2 (Th2) cell differentiation, type 2 innate lymphoid cell (ILC2) development and regulation of interleukin-4 (IL-4) and IL-13 production. Cytokine 2015, 75, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Mishra, A.; Wang, M.; Pemmaraju, V.R.; Collins, M.H.; Fulkerson, P.C.; Abonia, J.; Blanchard, C.; Putnam, P.E.; Rothenberg, M.E. Esophageal Remodeling Develops as a Consequence of Tissue Specific IL-5-Induced Eosinophilia. Gastroenterology 2008, 134, 204–214. [Google Scholar] [CrossRef] [PubMed]
- O’Shea, K.M.; Aceves, S.S.; Dellon, E.S.; Gupta, S.K.; Spergel, J.M.; Furuta, G.T.; Rothenberg, M.E. Pathophysiology of Eosinophilic Esophagitis. Gastroenterology 2018, 154, 333–345. [Google Scholar] [CrossRef] [PubMed]
- Smithgall, M.D.; Comeau, M.R.; Park Yoon, B.R.; Kaufman, D.; Armitage, R.; Smith, D.E. IL- amplifies both Th1- and Th2-type responses through its activity on human basophils, allergen- reactive Th2 cells, iNKT and NK cells. Int. Immunol. 2008, 20, 1019–1030. [Google Scholar] [CrossRef]
- Postlethwaite, A.E.; Shigemitsu, H.; Kanangat, S. Cellular origins of fibroblasts: Possible implications for organ fibrosis in systemic sclerosis. Curr. Opin. Rheumatol. 2010, 16, 733–738. [Google Scholar] [CrossRef]
- Humphreys, B.D.; Lin, S.-L.; Kobayashi, A.; Hudson, T.E.; Nowlin, B.T.; Bonventre, J.V.; Valerius, M.T.; McMahon, A.P.; Duffield, J.S. Fate Tracing Reveals the Pericyte and Not Epithelial Origin of Myofibroblasts in Kidney Fibrosis. Am. J. Pathol. 2010, 176, 85–97. [Google Scholar] [CrossRef]
- Kendall, R.T.; Feghali-Bostwick, C.A. Fibroblasts in fibrosis: Novel roles and mediators. Front. Pharmacol. 2014, 5, 123. [Google Scholar] [CrossRef]
- Wynn, T.A. Cellular and molecular mechanisms of fibrosis. J. Pathol. 2008, 214, 199–210. [Google Scholar] [CrossRef]
- Rosenbloom, J.; Castro, S.V.; Jiménez, S.A. Narrative Review: Fibrotic Diseases: Cellular and Molecular Mechanisms and Novel Therapies. Ann. Intern. Med. 2010, 152, 159. [Google Scholar] [CrossRef] [PubMed]
- Rockey, D.C.; Bell, P.D.; Hill, J.A. Fibrosis—A Common Pathway to Organ Injury and Failure. N. Engl. J. Med. 2015, 372, 1138–1149. [Google Scholar] [CrossRef] [PubMed]
- Rosenbloom, J.; Macarak, E.; Piera-Velazquez, S.; Jimenez, S.A. Human Fibrotic Diseases: Current Challenges in Fibrosis Research. Fibrosis: Methods and Protocols. Methods Mol. Biol. 2017, 2017, 1627. [Google Scholar]
- Goumans, M.J.; Liu, Z.; ten Dijke, P. TGF-beta signaling in vascular biology and dysfunction. Cell Res. 2009, 19, 116–127. [Google Scholar] [CrossRef] [PubMed]
- Medici, D.; Potenta, S.; Kalluri, R. Transforming growth factor-beta2 promotes Snail-mediated endothelial-mesenchymal transition through convergence of Smad-dependent and Smad-independent signalling. Biochem. J. 2011, 437, 515–520. [Google Scholar] [CrossRef]
- van Meeteren, L.A.; ten Dijke, P. Regulation of endothelial cell plasticity by TGF-beta. Cell Tissue Res. 2012, 347, 177–186. [Google Scholar] [CrossRef]
- Leask, A.; Abraham, D.J. TGF-beta signaling and the fibrotic response. FASEB J. 2004, 18, 816–827. [Google Scholar] [CrossRef]
- Ghosh, A.K.; Vaughan, D.E. PAI-1 in tissue fibrosis. J. Cell. Physiol. 2012, 227, 493–507. [Google Scholar] [CrossRef]
- Al-Toma, A.; Volta, U.; Auricchio, R.; Castillejo, G.; Sanders, D.S.; Cellier, C.; Mulder, C.J.; Lundin, K.E.A. European Society for the Study of Coeliac Disease (ESsCD) guideline for coeliac disease and other gluten-related disorders. United Eur. Gastroenterol. J. 2019, 7, 583–613. [Google Scholar] [CrossRef]
- Ulmasov, B.; Xu, Z.; Tetri, L.H.; Inagami, T.; Neuschwander-Tetri, B.A. Protective role of angiotensin II type 2 receptor signaling in a mouse model of pancreatic fibrosis. Am. J. Physiol. Liver Physiol. 2009, 296, G284–G294. [Google Scholar] [CrossRef][Green Version]
- Noel, R.J.; Putnam, P.E.; Rothenberg, M.E. Eosinophilic esophagitis. N. Engl. J. Med. 2004, 351, 940. [Google Scholar] [CrossRef]
- Straumann, A.; Simon, H.U. Eosinophilic esophagitis: Escalating epidemiology? J. Allergy Clin. Immunol. 2005, 115, 418. [Google Scholar] [CrossRef] [PubMed]
- Erwin, E.A.; Asti, L.; Hemming, T.; Kelleher, K.J. A Decade of Hospital Discharges Related to Eosinophilic Esophagitis. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 427–429. [Google Scholar] [CrossRef] [PubMed]
- Soon, I.S.; Butzner, J.D.; Kaplan, G.; Debruyn, J.C. Incidence and Prevalence of Eosinophilic Esophagitis in Children. J. Pediatr. Gastroenterol. Nutr. 2013, 57, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Navarro, P.; Arias, Á.; Arias-González, L.; Laserna-Mendieta, E.J.; Ruiz-Ponce, M.; Lucendo, A.J. Systematic review with meta-analysis: The growing incidence and prevalence of eosinophilic oesophagitis in children and adults in population-based studies. Aliment. Pharmacol. Ther. 2019, 49, 1116. [Google Scholar] [CrossRef] [PubMed]
- Rothenberg, M.E. Eosinophilia. N. Engl. J. Med. 1998, 338, 1592–1600. [Google Scholar] [CrossRef] [PubMed]
- Kagalwalla, A.F.; Akhtar, N.; Woodruff, S.A.; Rea, B.A.; Masterson, J.C.; Mukkada, V.; Parashette, K.R.; Du, J.; Fillon, S.; Protheroe, C.A.; et al. Eosinophilic esophagitis: Epithelial mesenchymal transition contributes to esophageal remodeling and reverses with treatment. J. Allergy Clin. Immunol. 2012, 129, 1387–1396.e7. [Google Scholar] [CrossRef]
- Straumann, A.; Conus, S.; Grzonka, P.; Kita, H.; Kephart, G.; Bussmann, C.; Beglinger, C.; Smith, D.A.; Patel, J.; Byrne, M.; et al. Anti-interleukin5 antibody treatment (mepolizumab) in active eosinophilic oe-sophagitis: A randomised, placebo-controlled, double-blind trial. Gut 2010, 59, 21–30. [Google Scholar] [CrossRef]
- Assa’Ad, A.H.; Gupta, S.K.; Collins, M.H.; Thomson, M.; Heath, A.T.; Smith, D.A.; Perschy, T.L.; Jurgensen, C.H.; Ortega, H.G.; Aceves, S.S. An Antibody Against IL-5 Reduces Numbers of Esophageal Intraepithelial Eosinophils in Children with Eosinophilic Esophagitis. Gastroenterology 2011, 141, 1593–1604. [Google Scholar] [CrossRef]
- Otani, I.M.; Anilkumar, A.A.; Newbury, R.O.; Bhagat, M.; Beppu, L.Y.; Dohil, R.; Broide, D.H.; Aceves, S.S. Anti–IL-5 therapy reduces mast cell and IL-9 cell numbers in pediatric patients with eosinophilic esophagitis. J. Allergy Clin. Immunol. 2013, 131, 1576–1582.e2. [Google Scholar] [CrossRef]
- Spergel, J.M.; Rothenberg, M.E.; Collins, M.H.; Furuta, G.T.; Markowitz, J.E.; Fuchs, G., III; O’Gorman, M.A.; Abonia, J.P.; Young, J.; Henkel, T.; et al. Reslizumab in children and adolescents with eosinophilic esophagitis: Results of a double-blind, randomized, placebo-controlled trial. Allergy Clin. Immunol. 2012, 129, 456–463. [Google Scholar] [CrossRef]
- Rothenberg, M.E. Eosinophilic gastrointestinal disorders (EGID). J. Allergy Clin. Immunol. 2004, 113, 11–28. [Google Scholar] [CrossRef] [PubMed]
- Hirano, I.; Collins, M.H.; Dayan, Y.A.; Evans, L.; Gupta, S.; Schoepfer, A.M.; Straumann, A.; Safroneeva, E.; Grimm, M.; Smith, H.; et al. RPC4046, a Monoclonal Antibody Against IL13, Reduces Histologic and Endoscopic Activity in Patients with Eosinophilic Esophagitis. Gastroenterology 2019, 156, 592–603.e10. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.A.; Hural, J. Functions of IL-4 and Control of Its Expression. Crit Rev. Immunol. 2017, 37, 181–212. [Google Scholar] [CrossRef] [PubMed]
- Rieder, F.; Fiocchi, C.; Rogler, G. Mechanisms, Management, and Treatment of Fibrosis in Patients with Inflammatory Bowel Diseases. Gastroenterology 2017, 152, 340–350.e6. [Google Scholar] [CrossRef]
- Wang, J.; Park, J.Y.; Huang, R.; Souza, R.F.; Spechler, S.J.; Cheng, E. Obtaining adequate lamina propria for subepithelial fibrosis evaluation in pediatric eosinophilic esophagitis. Gastrointest. Endosc. 2018, 87, 1207–1214.e3. [Google Scholar] [CrossRef]
- Rawson, R.; Yang, T.; Newbury, R.O.; Aquino, M.; Doshi, A.; Bell, B.; Broide, D.H.; Dohil, R.; Kurten, R.; Aceves, S.S. TGF-β1–induced PAI-1 contributes to a profibrotic network in patients with eosinophilic esophagitis. J. Allergy Clin. Immunol. 2016, 138, 791–800.e4. [Google Scholar] [CrossRef]
- Biernacka, A.; Dobaczewski, M. Frangogiannis NG.TGF-β signaling in fibrosis. Growth Factors 2011, 29, 196–202. [Google Scholar] [CrossRef]
- Gorelik, L.; Flavell, R.A. Abrogation of TGF beta signaling in T cells leads to spontaneous T cell differentiation and autoimmune disease. Immunity 2000, 12, 171–181. [Google Scholar] [CrossRef]
- Diebold, R.J.; Eis, M.J.; Yin, M.; Ormsby, I.; Boivin, G.P.; Darrow, B.J.; Saffitz, J.E.; Doetschman, T. Early-onset multifocal inflammation in the transforming growth factor beta 1-null mouse is lymphocyte mediated. Proc. Natl. Acad. Sci. USA 1995, 92, 12215–12219. [Google Scholar] [CrossRef]
- Ono, K.; Ohtomo, T.; Ninomiya-Tsuji, J.; Tsuchiya, M. A dominant negative TAK1 inhibits cellular fibrotic responses induced by TGF-β. Biochem. Biophys. Res. Commun. 2003, 307, 332–337. [Google Scholar] [CrossRef]
- Hocevar, B.A.; Prunier, C.; Howe, P.H. Disabled-2 (Dab2) Mediates Transforming Growth Factor β(TGFβ)-stimulated Fibronectin Synthesis through TGFβ-activated Kinase 1 and Activation of the JNK Pathway. J. Biol Chem. 2005, 280, 25920–25927. [Google Scholar] [CrossRef] [PubMed]
- Ninomiya-Tsuji, J.; Kishimoto, K.; Hiyama, A.; Inoue, J.; Cao, Z.; Matsumoto, K. The kinase TAK1 can activate the NIK-I kappaB as well as the MAP kinase cascade in the IL-1 signalling pathway. Nature 1999, 398, 252–256. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| EoE | Celiac Disease | Control (Oesophagus) | Control (Duodenum) | p-Value | |
|---|---|---|---|---|---|
| Patients(N) | 5 | 5 | 4 | 3 | |
| Biopsy specimens (N) | 20 | 20 | 16 | 12 | |
| Sex(M/F) | 4/1 | 0/5 | 1/3 | 1/2 | 0.01 |
| Age mean ± SE | 36.4 ± 6 | 42.2 ± 8 | 29.7 ± 2 | 37.6 ± 4 | 0.44 |
| Caucasian | 5 (100%) | 5 (100%) | 4 (100%) | 4 (100%) | 1 |
| Clinical symptoms | |||||
| Dysphagia | 5 (100%) | 0 | 0 | 0 | 0 |
| Bolus impact | 3 (60%) | 0 | 0 | 0 | 0.04 |
| Steroid in the last 4 weeks | 0 | 0 | 0 | 0 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pronio, A.; Covotta, F.; Pallotta, L.; Palma, R.; Badiali, D.; Sacchi, M.C.; Lamazza, A.; Severi, C. Eosinophilic Esophagitis: Cytokines Expression and Fibrotic Markers in Comparison to Celiac Disease. Diagnostics 2022, 12, 2092. https://doi.org/10.3390/diagnostics12092092
Pronio A, Covotta F, Pallotta L, Palma R, Badiali D, Sacchi MC, Lamazza A, Severi C. Eosinophilic Esophagitis: Cytokines Expression and Fibrotic Markers in Comparison to Celiac Disease. Diagnostics. 2022; 12(9):2092. https://doi.org/10.3390/diagnostics12092092
Chicago/Turabian StylePronio, Annamaria, Francesco Covotta, Lucia Pallotta, Rossella Palma, Danilo Badiali, Maria Carlotta Sacchi, Antonietta Lamazza, and Carola Severi. 2022. "Eosinophilic Esophagitis: Cytokines Expression and Fibrotic Markers in Comparison to Celiac Disease" Diagnostics 12, no. 9: 2092. https://doi.org/10.3390/diagnostics12092092
APA StylePronio, A., Covotta, F., Pallotta, L., Palma, R., Badiali, D., Sacchi, M. C., Lamazza, A., & Severi, C. (2022). Eosinophilic Esophagitis: Cytokines Expression and Fibrotic Markers in Comparison to Celiac Disease. Diagnostics, 12(9), 2092. https://doi.org/10.3390/diagnostics12092092