
IBD Monitor: Romanian National Mobile Application for Inflammatory Bowel Disease Personalized Treatment and Monitoring


 , and
, and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Research and Development Strategy
2.2. Activities
2.3. Technologies
3. Results
3.1. Details of the Project
3.2. App Description
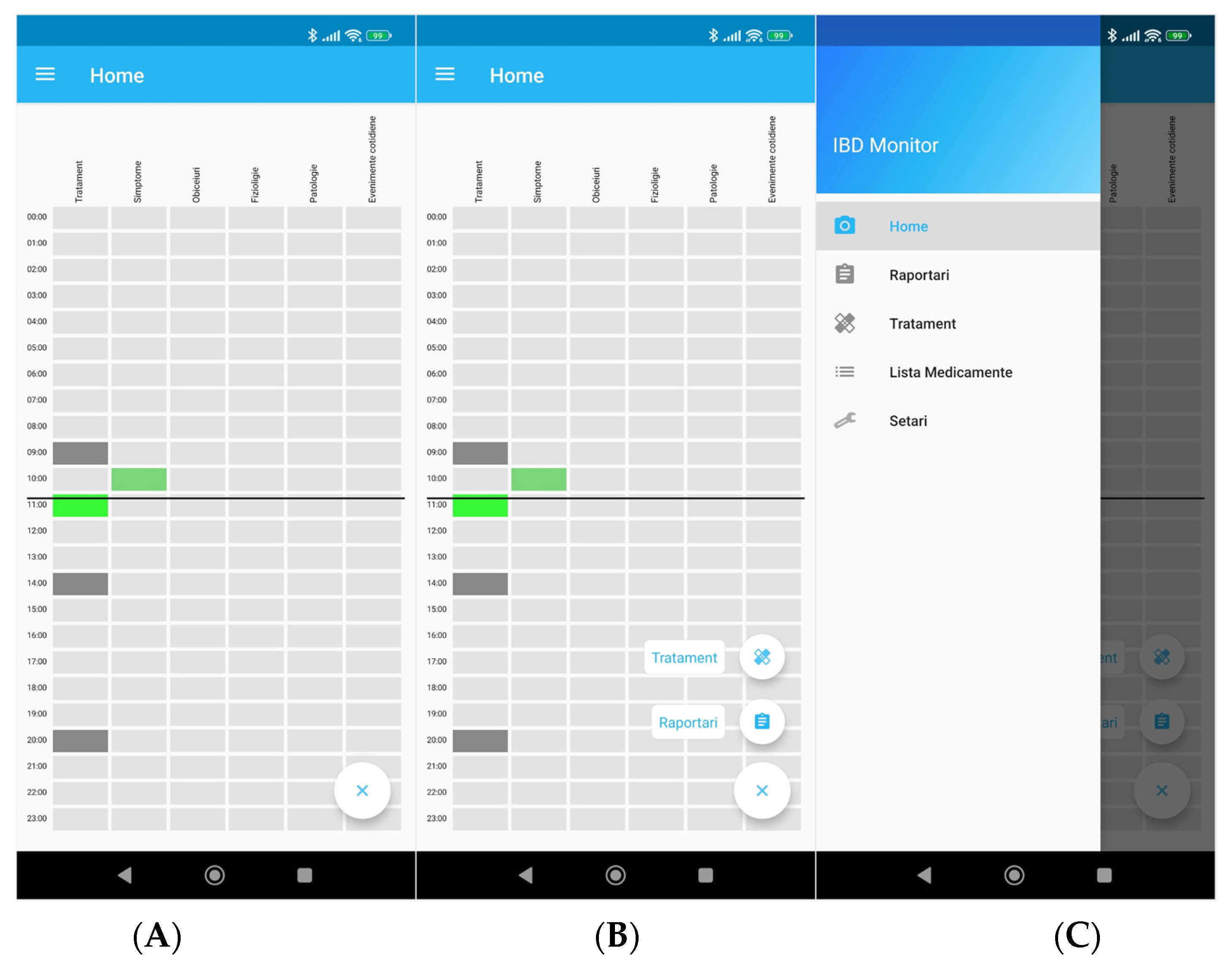
3.3. Home Screen
3.4. Reporting Screen
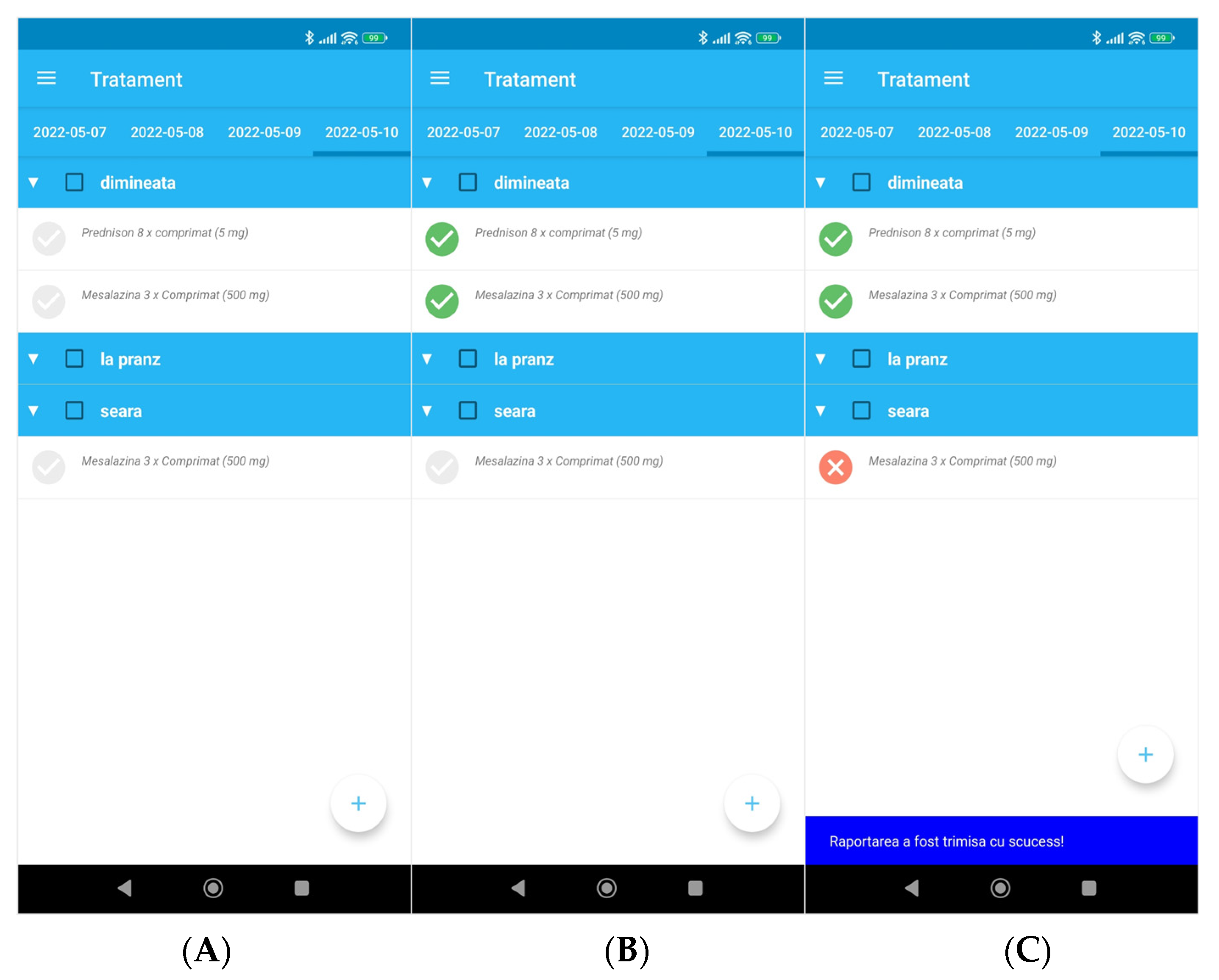
3.5. Medication Administration Reminders and Reporting
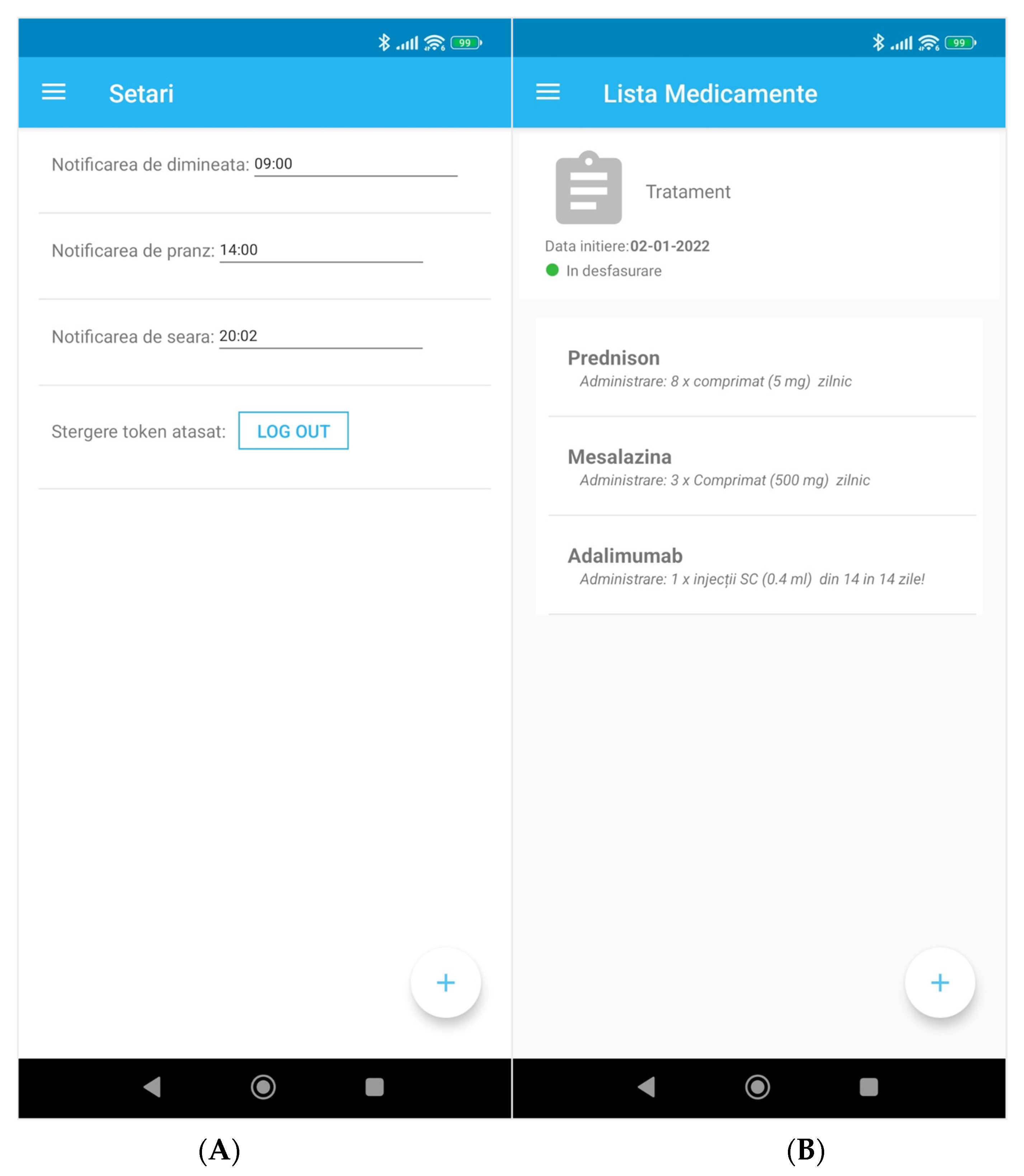
3.6. Other App Functions
3.7. The Smartwatch App
4. Discussion
Current Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2017 Inflammatory Bowel Disease Collaborators. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 17–30. [Google Scholar] [CrossRef] [Green Version]
- Johnston, R.D.; Logan, R.F. What is the peak age for onset of IBD? Inflamm. Bowel Dis. 2008, 14 (Suppl. 2), S4–S5, Erratum in: Inflamm. Bowel Dis. 2009, 15, 1438–1447. [Google Scholar] [CrossRef]
- PEW Research Center. Available online: https://www.pewresearch.org/internet/fact-sheet/mobile/ (accessed on 30 April 2022).
- Hamilton, M.J. The Use of Mobile Applications in the Management of Patients with Inflammatory Bowel Disease. Gastroenterol. Hepatol. 2018, 14, 529–531. [Google Scholar]
- Popa, D.E.; Manea, N.C.; Gheonea, D.I.; PÎrlog, M.C. Development of a Software for Treat-To-Target Strategy Implementation and Increasing Quality of Life in Patients with Inflammatory Bowel Disease. Curr. Health Sci. J. 2020, 46, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Con, D.; De Cruz, P. Mobile Phone Apps for Inflammatory Bowel Disease Self-Management: A Systematic Assessment of Content and Tools. JMIR Mhealth Uhealth 2016, 4, e13. [Google Scholar] [CrossRef] [PubMed]
- Kelso, M.; Feagins, L.A. Can Smartphones Help Deliver Smarter Care for Patients with Inflammatory Bowel Disease? Inflamm. Bowel Dis. 2018, 24, 1453–1459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cima, R.R.; Anderson, K.J.; Larson, D.W.; Dozois, E.J.; Hassan, I.; Sandborn, W.J.; Loftus, E.; Pemberton, J.H. Internet use by patients in an inflammatory bowel disease specialty clinic. Inflamm. Bowel Dis. 2007, 13, 1266–1270. [Google Scholar] [CrossRef] [PubMed]
- Bernard, A.; Langille, M.; Hughes, S.; Rose, C.; Leddin, D.; Van Zanten, S.V. A systematic review of patient inflammatory bowel disease information resources on the world wide web. Am. J. Gastroenterol. 2007, 102, 2070–2077. [Google Scholar] [CrossRef] [PubMed]
- Stone, J.H. Communication between physicians and patients in the era of E-medicine. N. Engl. J. Med. 2007, 356, 2451–2454. [Google Scholar] [CrossRef] [PubMed]
- Charpentier, G.; Benhamou, P.Y.; Dardari, D.; Clergeot, A.; Franc, S.; Schaepelynck-Belicar, P.; Catargi, B.; Melki, V.; Chaillous, L.; Farret, A.; et al. The Diabeo software enabling individualized insulin dose adjustments combined with telemedicine support improves HbA1c in poorly controlled type 1 diabetic patients: A 6-month, randomized, open-label, parallel-group, multicenter trial (TeleDiab 1 Study). Diabetes Care 2011, 34, 533–539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhee, H.; Allen, J.; Mammen, J.; Swift, M. Mobile phone-based asthma self-management aid for adolescents (mASMAA): A feasibility study. Patient Prefer. Adherence 2014, 8, 63–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jowett, S.L.; Seal, C.J.; Pearce, M.S.; Phillips, E.; Gregory, W.; Barton, J.R.; Welfare, M.R. Influence of dietary factors on the clinical course of ulcerative colitis: A prospective cohort study. Gut 2004, 53, 1479–1484. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.-L.; Li, Y.-C.J.; Chou, Y.-C.; Hsieh, Y.-W.; Kuo, F.; Tsai, W.-C.; Chai, S.D.; Lin, B.Y.-J.; Kung, P.-T.; Chuang, C.-J. Effects of and satisfaction with short message service reminders for patient medication adherence: A randomized controlled study. BMC Med. Inform. Decis. Mak. 2013, 13, 127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fenerty, S.D.; West, C.; Davis, S.A.; Kaplan, S.G.; Feldman, S.R. The effect of reminder systems on patients’ adherence to treatment. Patient Prefer. Adherence 2012, 6, 127–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenley, R.N.; Kunz, J.H.; Walter, J.; Hommel, K.A. Practical strategies for enhancing adherence to treatment regimen in inflammatory bowel disease. Inflamm. Bowel Dis. 2013, 19, 1534–1545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dayer, L.; Heldenbrand, S.; Anderson, P.; Gubbins, P.O.; Martin, B.C. Smartphone medication adherence apps: Potential benefits to patients and providers. J. Am. Pharm. Assoc. 2013, 53, 172–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whelan, T.; Levine, M.; Willan, A.; Gafni, A.; Sanders, K.; Mirsky, D.; Chambers, S.; O’Brien, M.A.; Reid, S.; Dubois, S. Effect of a decision aid on knowledge and treatment decision making for breast cancer surgery: A randomized trial. JAMA 2004, 292, 435–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molenaar, S.; Sprangers, M.A.; Rutgers, E.J.T.; Luiten, E.J.; Mulder, J.; Bossuyt, P.M.; Van Everdingen, J.J.; Oosterveld, P.; De Haes, H.C. Decision support for patients with early-stage breast cancer: Effects of an interactive breast cancer CDROM on treatment decision, satisfaction, and quality of life. J. Clin. Oncol. 2001, 19, 1676–1687. [Google Scholar] [CrossRef] [PubMed]
- De Jong, M.J.; van der Meulen-de, A.E.; Romberg-Camps, M.J.; Becx, M.C.; Maljaars, J.P.; Cilissen, M.; van Bodegraven, A.A.; Mahmmod, N.; Markus, T.; Hameeteman, W.M.; et al. Telemedicine for management of inflammatory bowel disease (myIBDcoach): A pragmatic, multicentre, randomised controlled trial. Lancet 2017, 390, 959–968. [Google Scholar] [CrossRef]
- Atreja, A.; Khan, S.; Rogers, J.D.; Otobo, E.; Patel, N.P.; Ullman, T.; Colombel, J.F.; Moore, S.; Sands, B.E.; HealthPROMISE Consortium Group. Impact of the Mobile HealthPROMISE Platform on the Quality of Care and Quality of Life in Patients with Inflammatory Bowel Disease: Study Protocol of a Pragmatic Randomized Controlled Trial. JMIR Res. Protoc. 2015, 4, e23. [Google Scholar] [CrossRef] [PubMed] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oancea, C.-N.; Statie, R.-C.; Gheonea, D.-I.; Ciurea, T.; Șerbănescu, M.-S.; Streba, C.-T. IBD Monitor: Romanian National Mobile Application for Inflammatory Bowel Disease Personalized Treatment and Monitoring. Diagnostics 2022, 12, 1345. https://doi.org/10.3390/diagnostics12061345
Oancea C-N, Statie R-C, Gheonea D-I, Ciurea T, Șerbănescu M-S, Streba C-T. IBD Monitor: Romanian National Mobile Application for Inflammatory Bowel Disease Personalized Treatment and Monitoring. Diagnostics. 2022; 12(6):1345. https://doi.org/10.3390/diagnostics12061345
Chicago/Turabian StyleOancea, Carmen-Nicoleta, Răzvan-Cristian Statie, Dan-Ionuț Gheonea, Tudorel Ciurea, Mircea-Sebastian Șerbănescu, and Costin-Teodor Streba. 2022. "IBD Monitor: Romanian National Mobile Application for Inflammatory Bowel Disease Personalized Treatment and Monitoring" Diagnostics 12, no. 6: 1345. https://doi.org/10.3390/diagnostics12061345
APA StyleOancea, C.-N., Statie, R.-C., Gheonea, D.-I., Ciurea, T., Șerbănescu, M.-S., & Streba, C.-T. (2022). IBD Monitor: Romanian National Mobile Application for Inflammatory Bowel Disease Personalized Treatment and Monitoring. Diagnostics, 12(6), 1345. https://doi.org/10.3390/diagnostics12061345