This contains all of the outcomes obtained using the proposed model. On the Kaggle dataset, the model is tested. Various performance criteria such as precision, sensitivity, F1 Score, and accuracy are taken into account when analyzing the suggested model. An exploratory investigation is carried out using various hyper parameters, which are described in detail below.
3.1. Hyper Parameters Tuning
Different parameters such as optimizer [
37], batch size and epochs are used for hyper parameters tuning on dermoscopy images. The Adam optimizer is a frequently used optimizer that has replaced the Stochastic Gradient Descent optimizer in terms of training the deep learning algorithms. Adam combines the various characteristics of RMSProp and AdaGrad optimizers. The expression of Adam optimizer is given in Equations (1) and (2):
α1 and α2 are the decay rates, δL is loss function derivative, δwt is weights derivative at t, wt signifies the weights, pt is gradients collection, and qt is past gradients sum of squares. Batch size is the most significant hyper parameter that is used for tuning any deep learning system. A large batch size causes the computational speedups during training of a deep learning model because of parallelism of GPUs but it may cause poor generalization. A small batch size causes faster convergence to good solutions. Hence there is always a competition between large and small batch size. In this paper, the proposed model is simulated with different batch sizes like 8, 16, 32, 64, and 128 to analyze which batch size will be suitable for better accuracy.
Epoch is the overall amount of times the whole dataset is received by neural network. When a model is trained for one epoch, it means that training dataset had one chance to update the internal parameters of the model. Therefore, the number of epochs should be more so that error can be minimized during learning of the model. But more epochs increase the computational time period. Hence, there should be a trade-off between a high and a small number of epochs. In this paper, the presented model is simulated using 10 and 20 epochs.
Table 5 shows the name of hyper tuning parameters and their values.
3.2. Model Accuracy and Model Loss Analysis
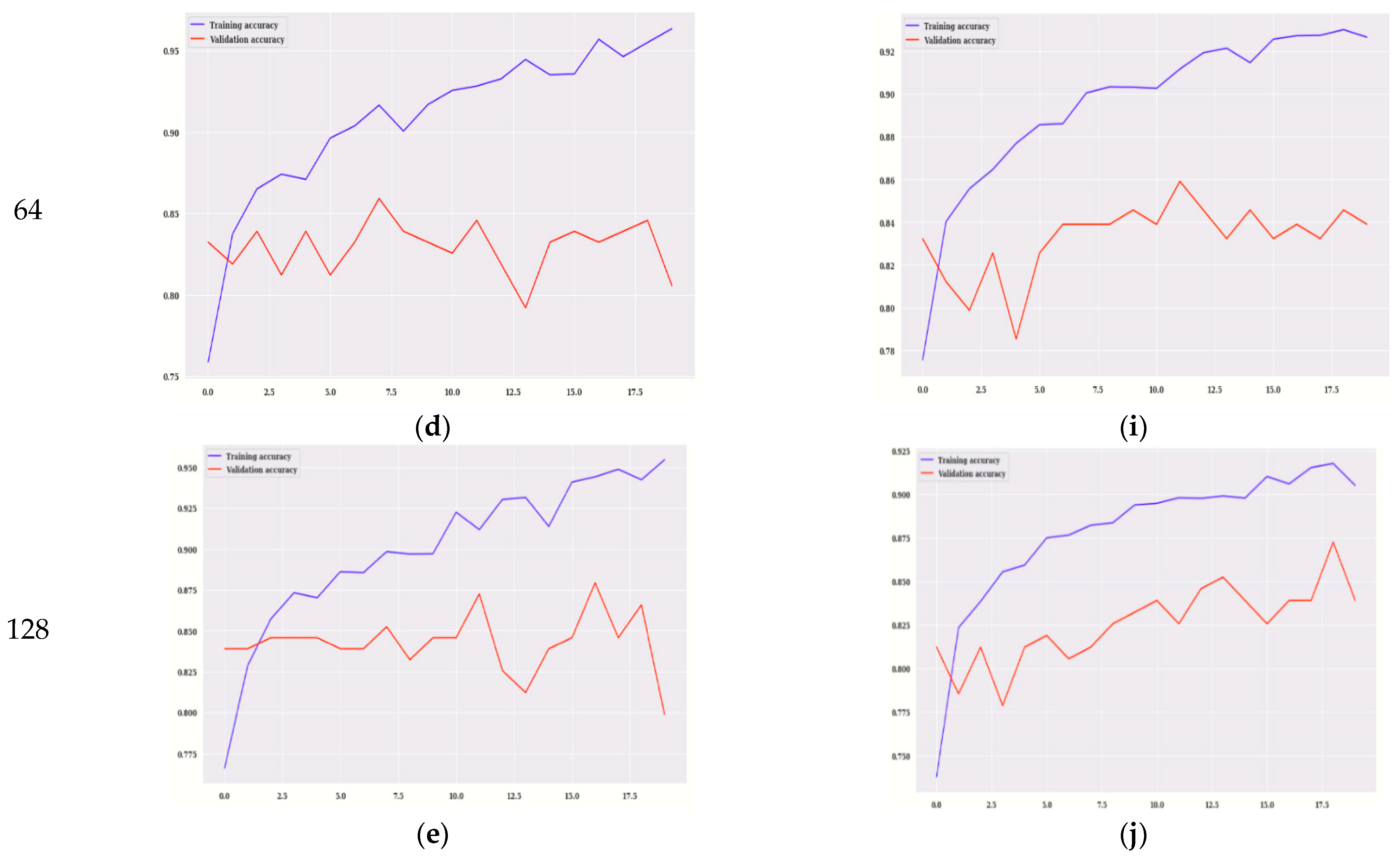
Training accuracy, validation accuracy for VGG16 and modified VGG16 is performed on the basis of model accuracy and model loss
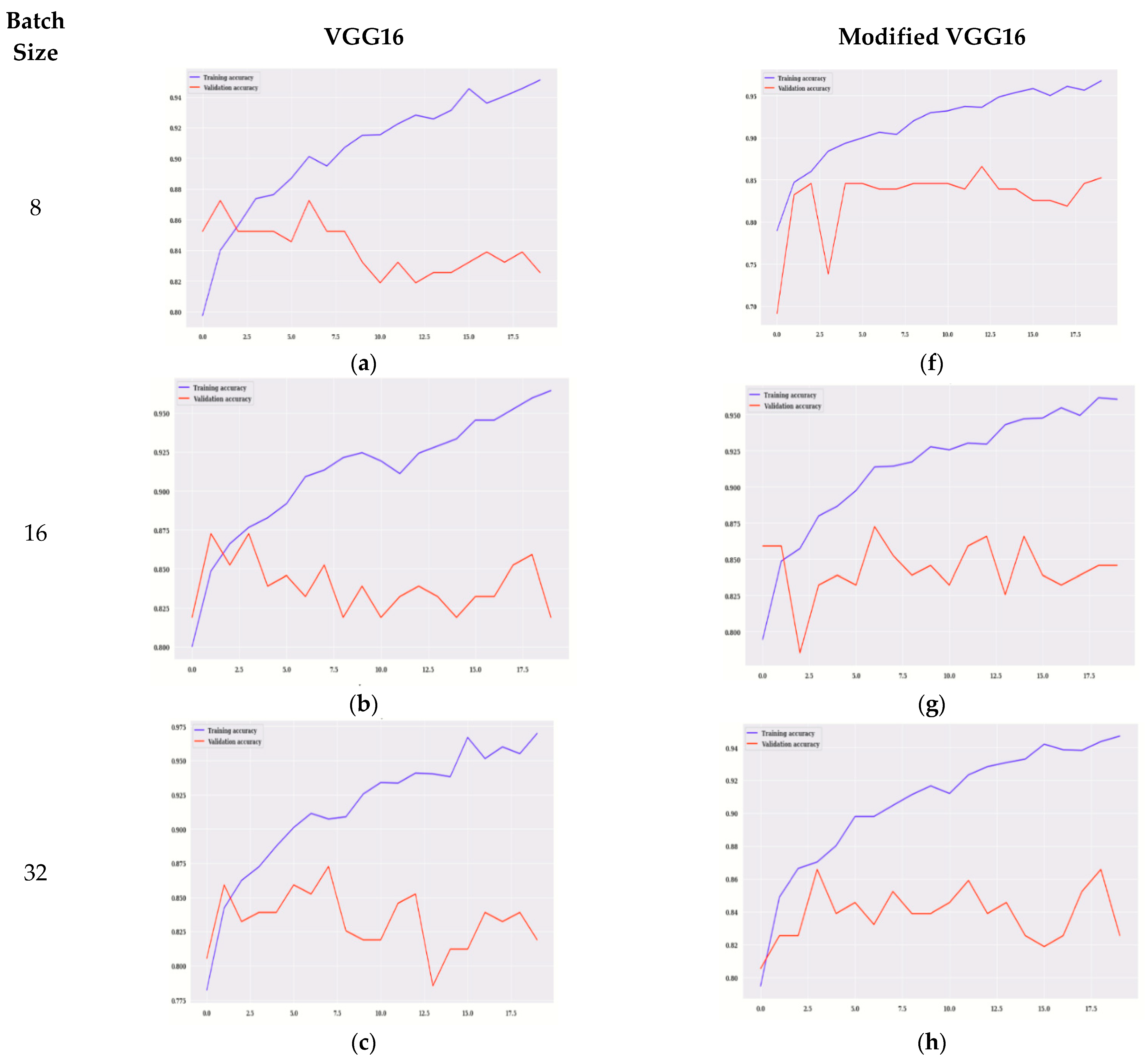
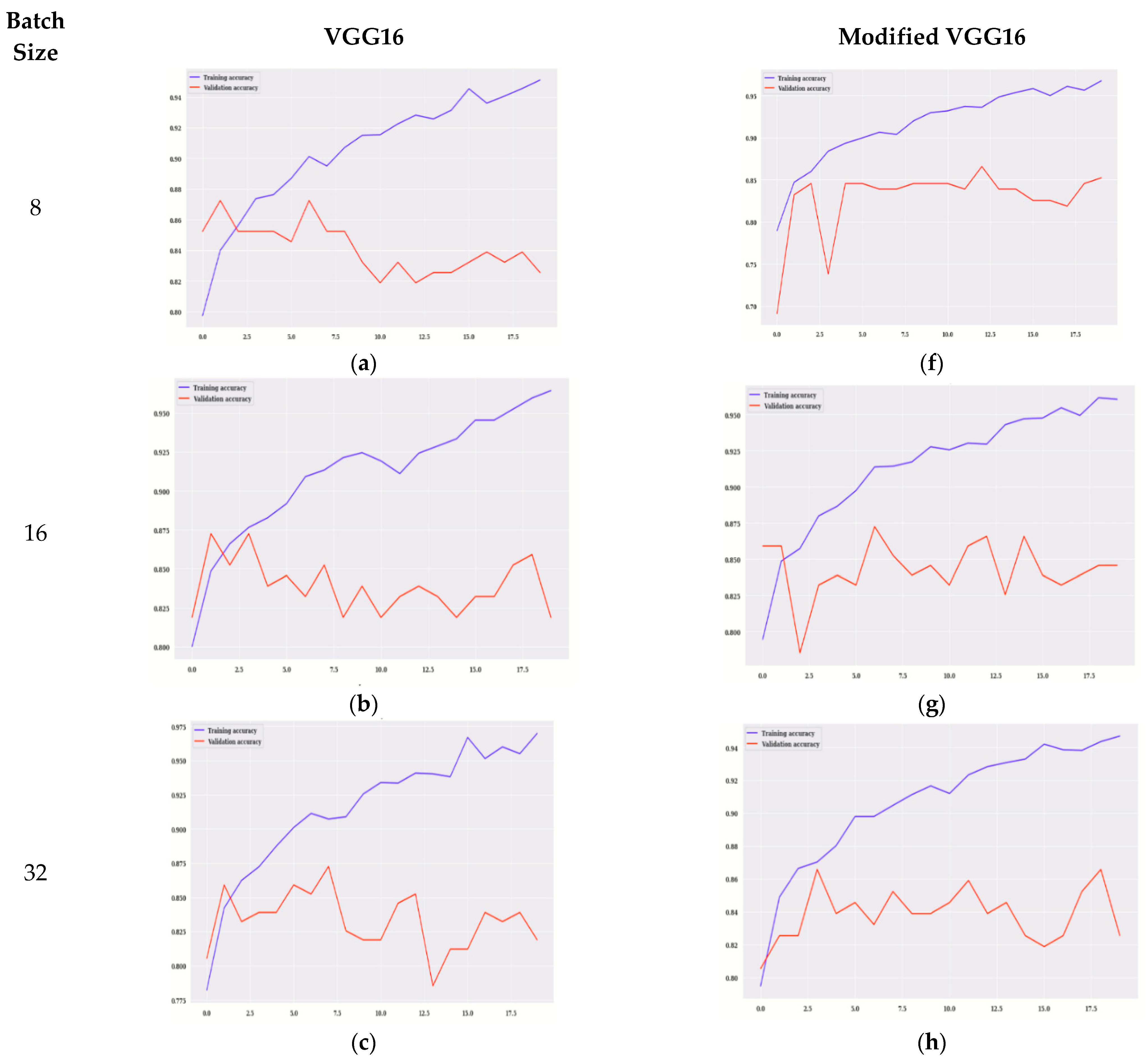
Figure 6 displays the graphs of training accuracy, validation accuracy for VGG16, and modified VGG16.
Figure 6a–e displays the accuracy for VGG16 and
Figure 6f–j displays the training, validation accuracy of modified VGG16. The model is evaluated on 20 epochs.
Figure 6a,f shows the graph of training and validation accuracy on 8 batch size for VGG16 and the modified VGG16 model, respectively.
It is observed that, for modified VGG16, the values of validation accuracy are more in comparison to the VGG16 model. The highest value is on the 11th epoch that is approximately 87% for the modified VGG16 model.
Figure 6b,g shows the graph of validation and training accuracy on 16 batch size for VGG16 and the modified VGG16 model, respectively. It is observed that, for modified VGG16, the values of validation accuracy are more in comparison to VGG16 model. The highest value is on the 6th epoch that is approximately 87% for the modified VGG16 model.
Figure 6c,h shows the graph of validation and training accuracy on 32 batch size for VGG16 and the modified VGG16 model, respectively. It is observed that, for modified VGG16, the values of validation accuracy are more in comparison to the VGG16 model. The highest value is on the 3rd and 18th epoch that is approximately 86% for the modified VGG16 model.
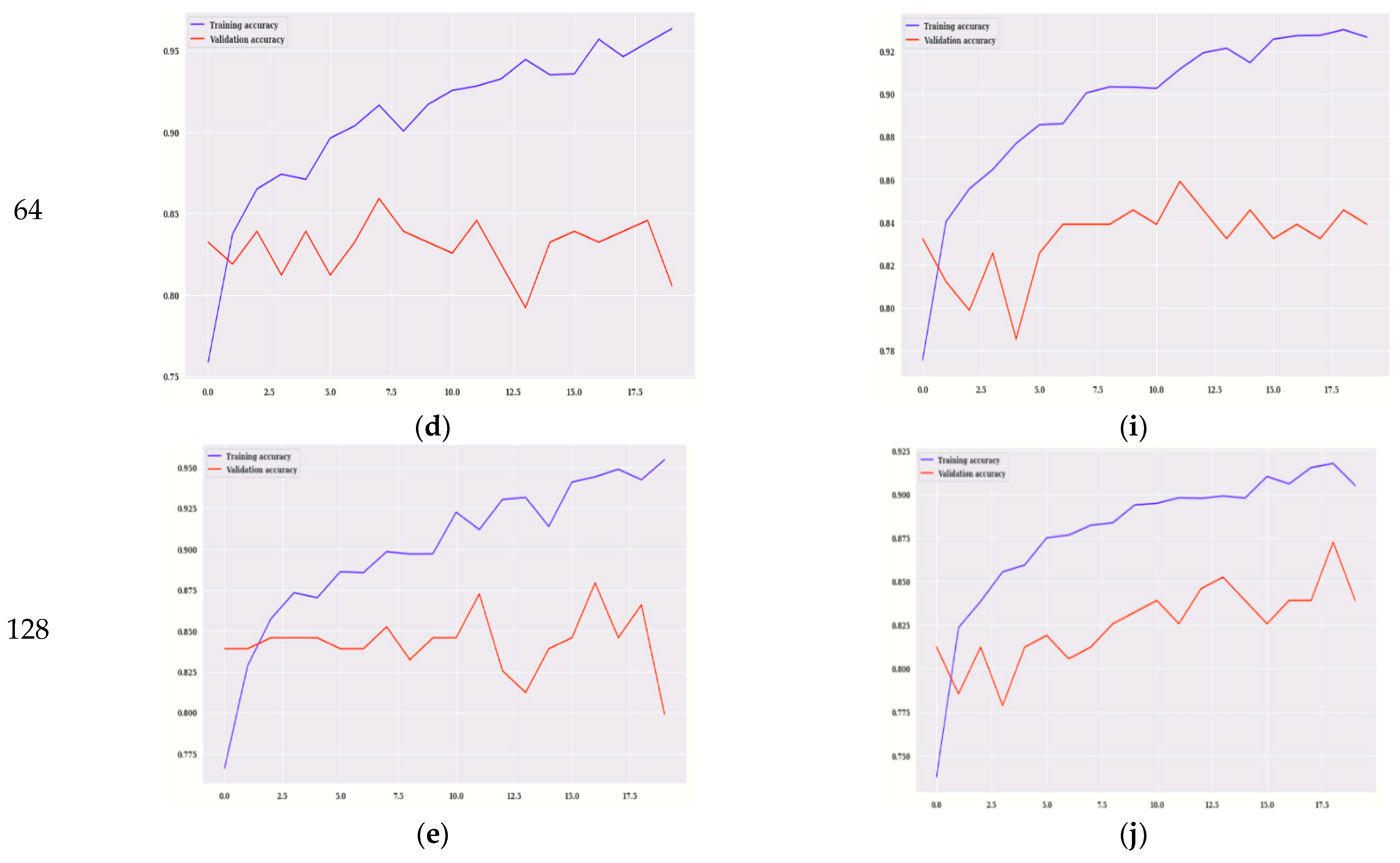
Figure 6d,i shows the graph of validation and training accuracy on 64 batch size for VGG16 and the modified VGG16 model, respectively. It is observed that, for modified VGG16, the values of validation accuracy are more in comparison to the VGG16 model. The highest value is on the 11th epoch that is 86% for the modified VGG16 model.
Figure 6e,j shows the graph of validation and training accuracy on 128 batch size for VGG16 and the modified VGG16 model, respectively. It is observed that, for modified VGG16, the values of validation accuracy are more in comparison to the VGG16 model. The highest value is on the 18th epoch that is approximately 87.5% for the modified VGG16 model. It can be analyzed from
Figure 6 that, for all the batch sizes as well as each epoch, validation accuracy is better for modified VGG16 as compared to VGG16. In any deep learning model, training and validation loss reduces as the number of epochs increases. Starting from 0 to 20 epoch values, peak points are shown in all the figures.
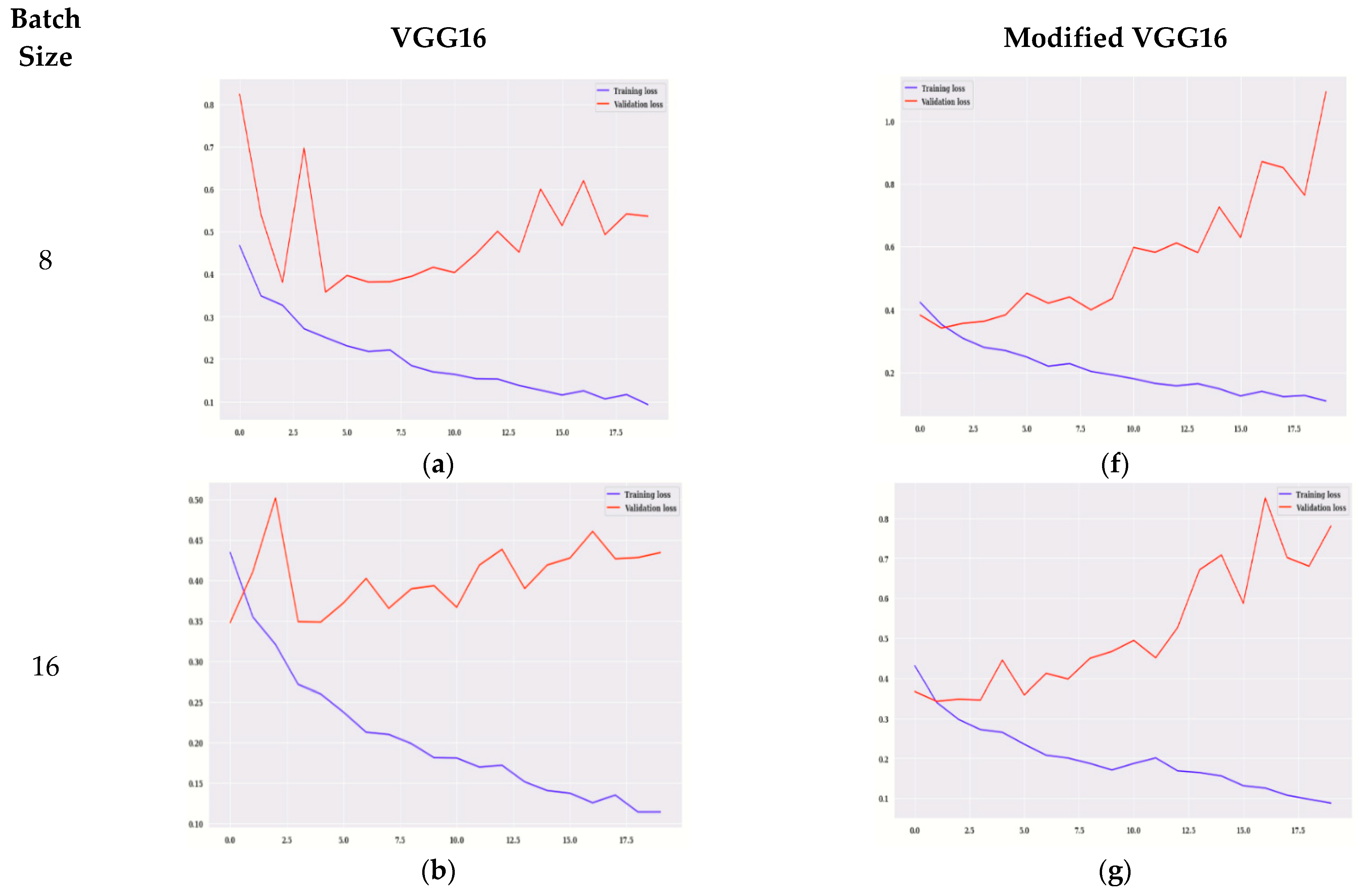
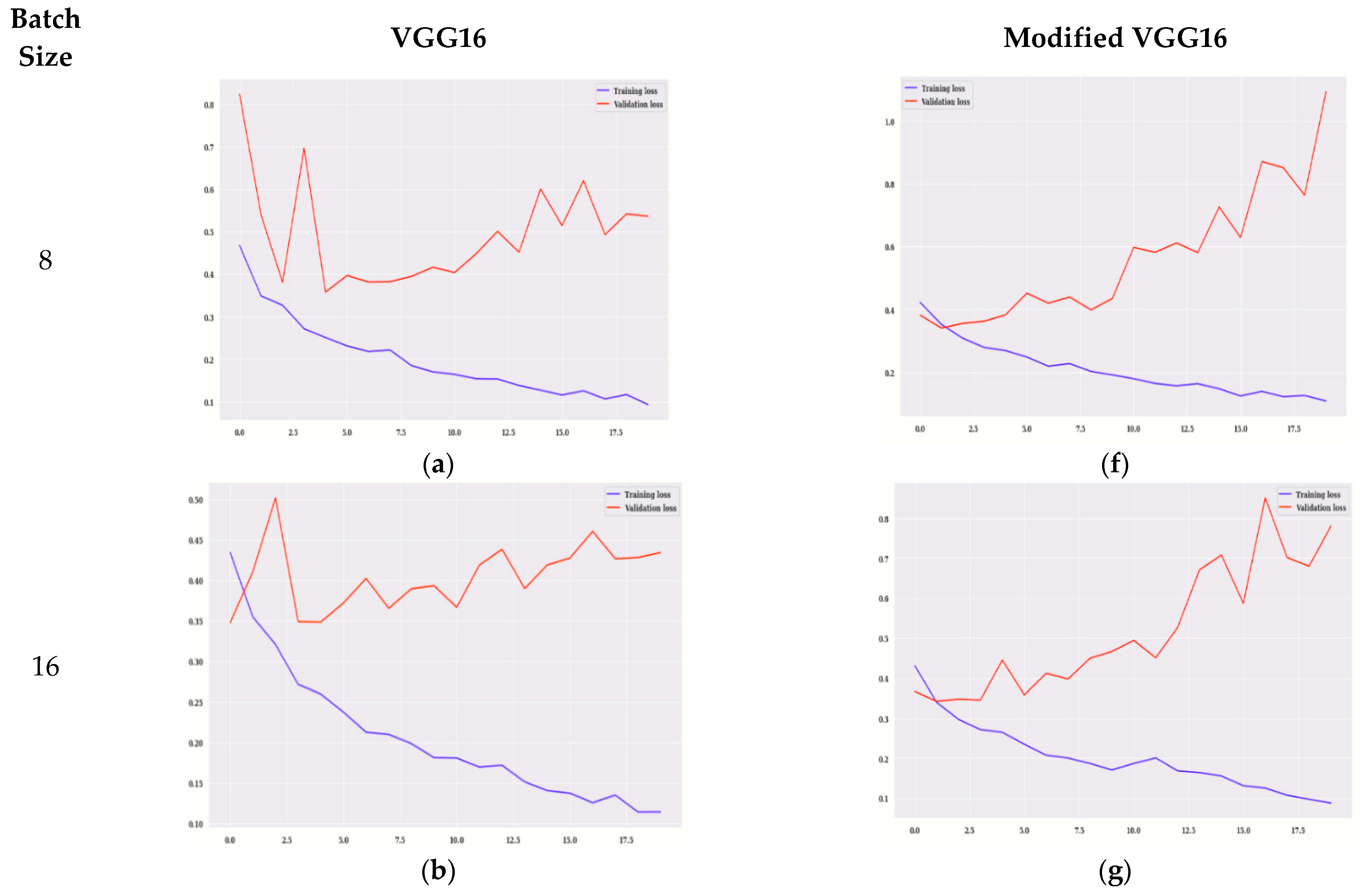
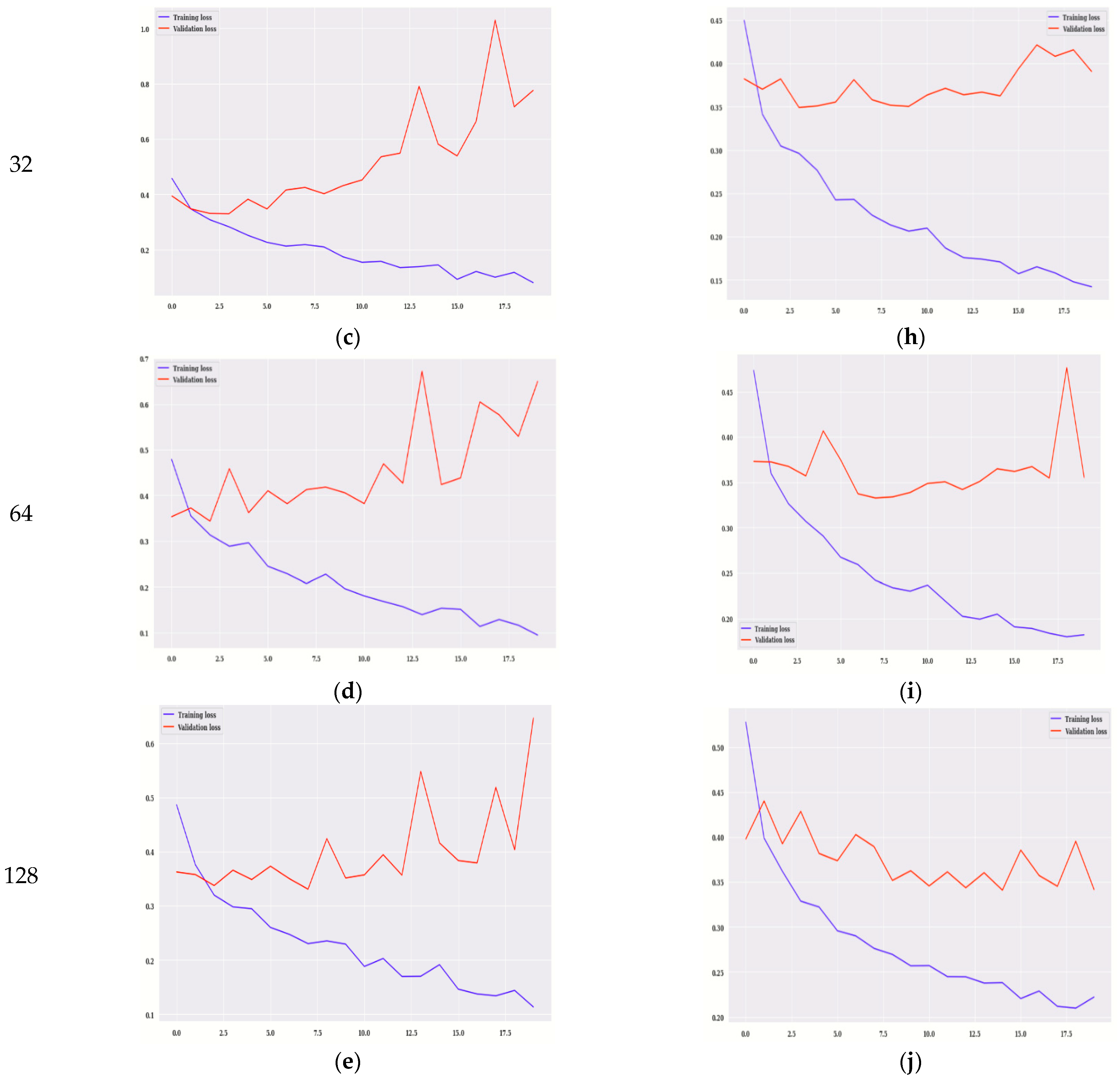
Figure 7 shows the graphs of loss for VGG16 and modified VGG16.
Figure 7a–e shows the training loss for VGG16, and
Figure 7f–j shows the training loss, validation loss for modified VGG16. The values of training loss are compared to validation loss. The model is evaluated on 20 epochs.
Figure 7a,f shows the graph of training and validation loss on 8 batch size for VGG16 and the modified VGG16 model, respectively. It is observed that, for modified VGG16, the values of validation loss are less in comparison to the VGG16 model. Similarly, for all the batch sizes modified VGG16 is showing better results as compared to VGG16 in terms of validation loss. Starting from 0 to 20 epoch values, peak points are shown in all the figures.
Table 6 shows the loss and accuracy for training and validation of the modified VGG16 model for two different epoch values, 10 and 20. The model is simulated with the Adam optimizer at five different batch sizes (i.e., 8, 16, 32, 64, and 128). It can be seen that, on the 10th epoch, the training accuracy is maximum at batch size 32, which is 0.9255 whereas training loss is minimum (i.e., 0.1736). Whereas, on the same epoch value, validation accuracy is maximum (i.e., 84.56%), and the validation loss is less (i.e., 0.3514) for batch size 32. From
Table 6, it is also analyzed that, on 20th epoch, the value of training accuracy is maximum at batch size 32, which is 0.9698, whereas training loss is minimum (i.e., 0.0801). Whereas, on the same epoch, value validation accuracy is maximum (i.e., 82.55%) at batch size 8, and the validation loss is minimum (i.e., 0.6468) at batch size 128.
Overall, it can be concluded from this table that, on the 10th and 20th epoch, the training results are best at batch size 32, whereas, validation results are best on the 10th epoch at batch size 128.
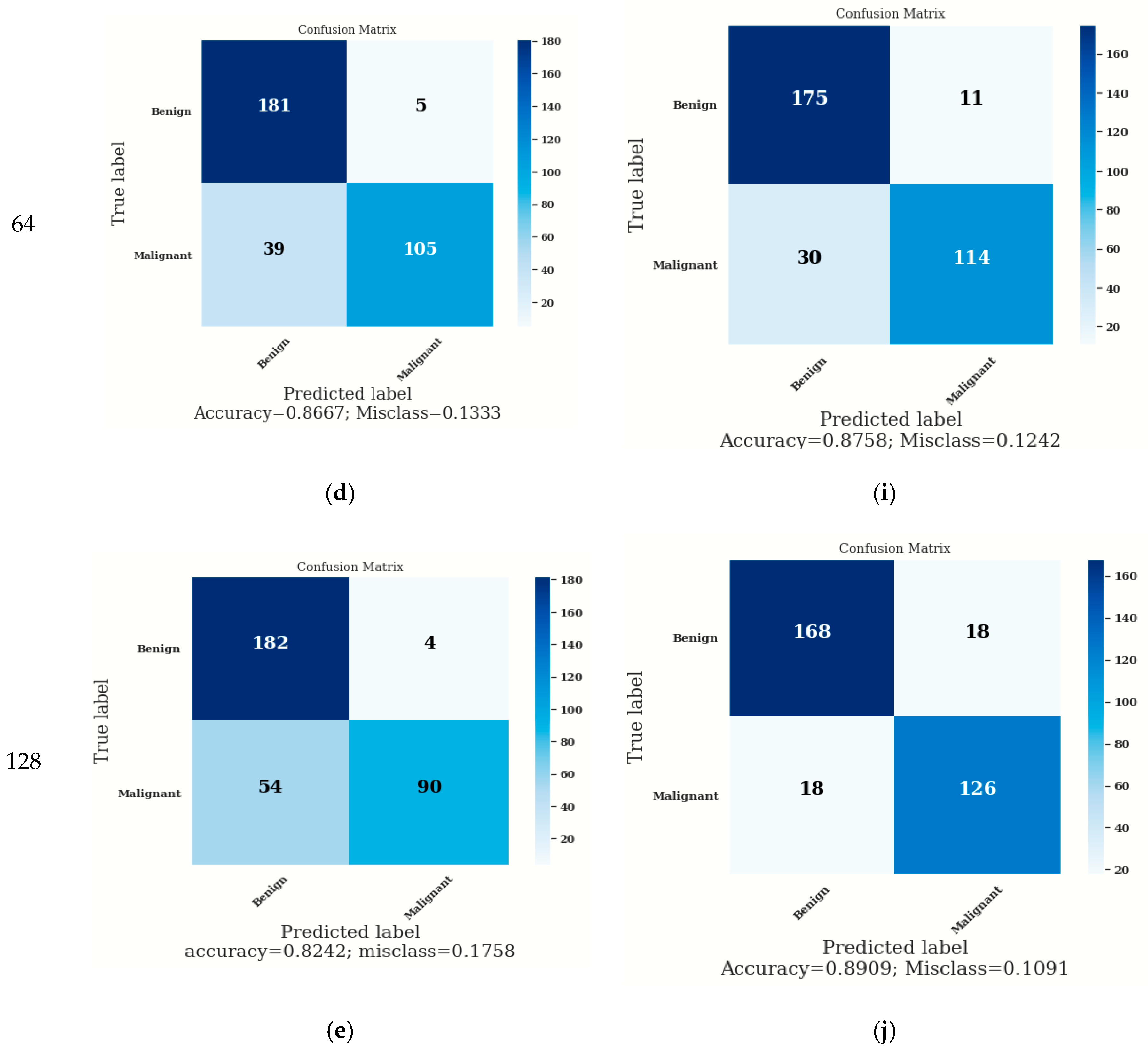
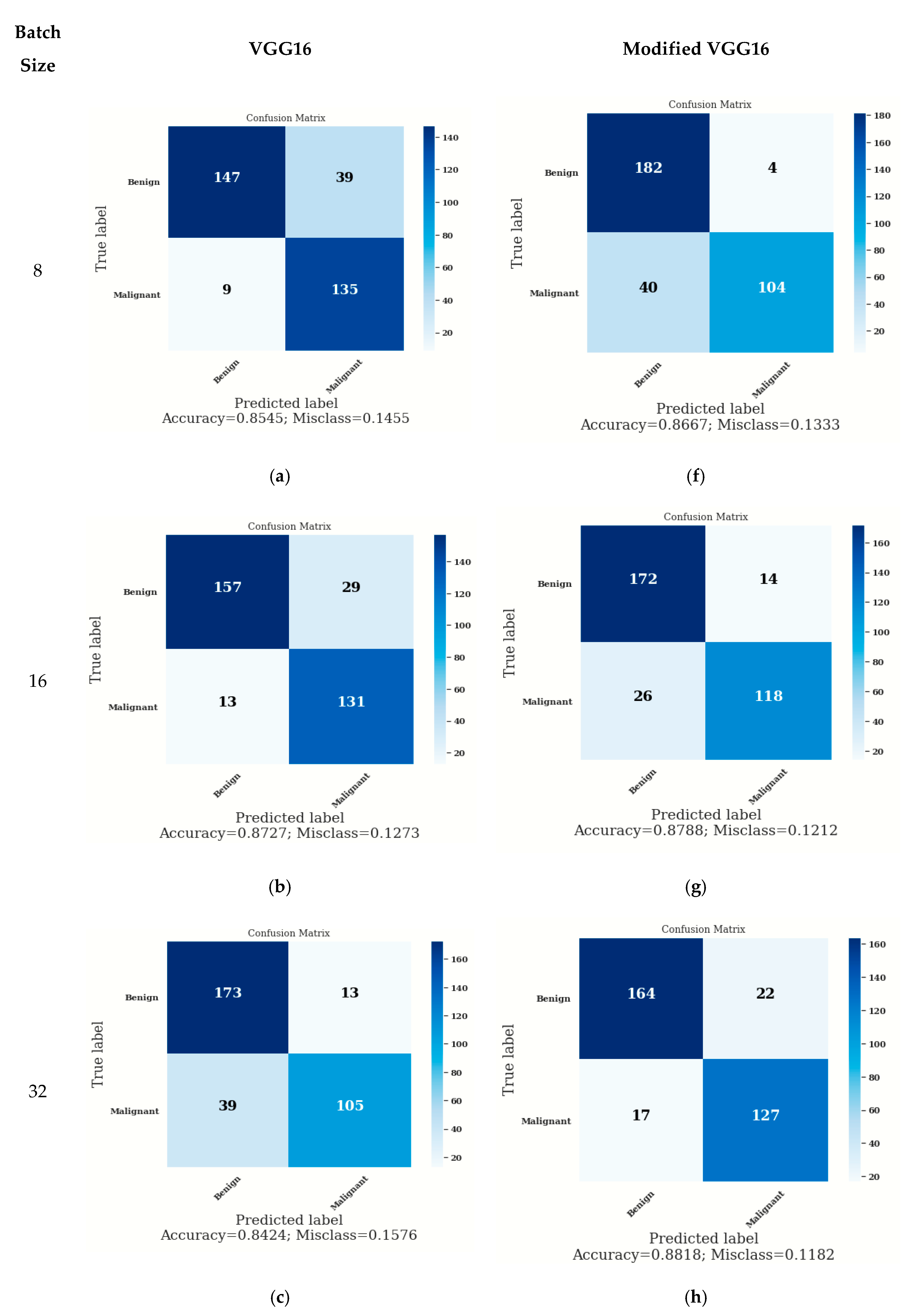
3.3. Confusion Matrix
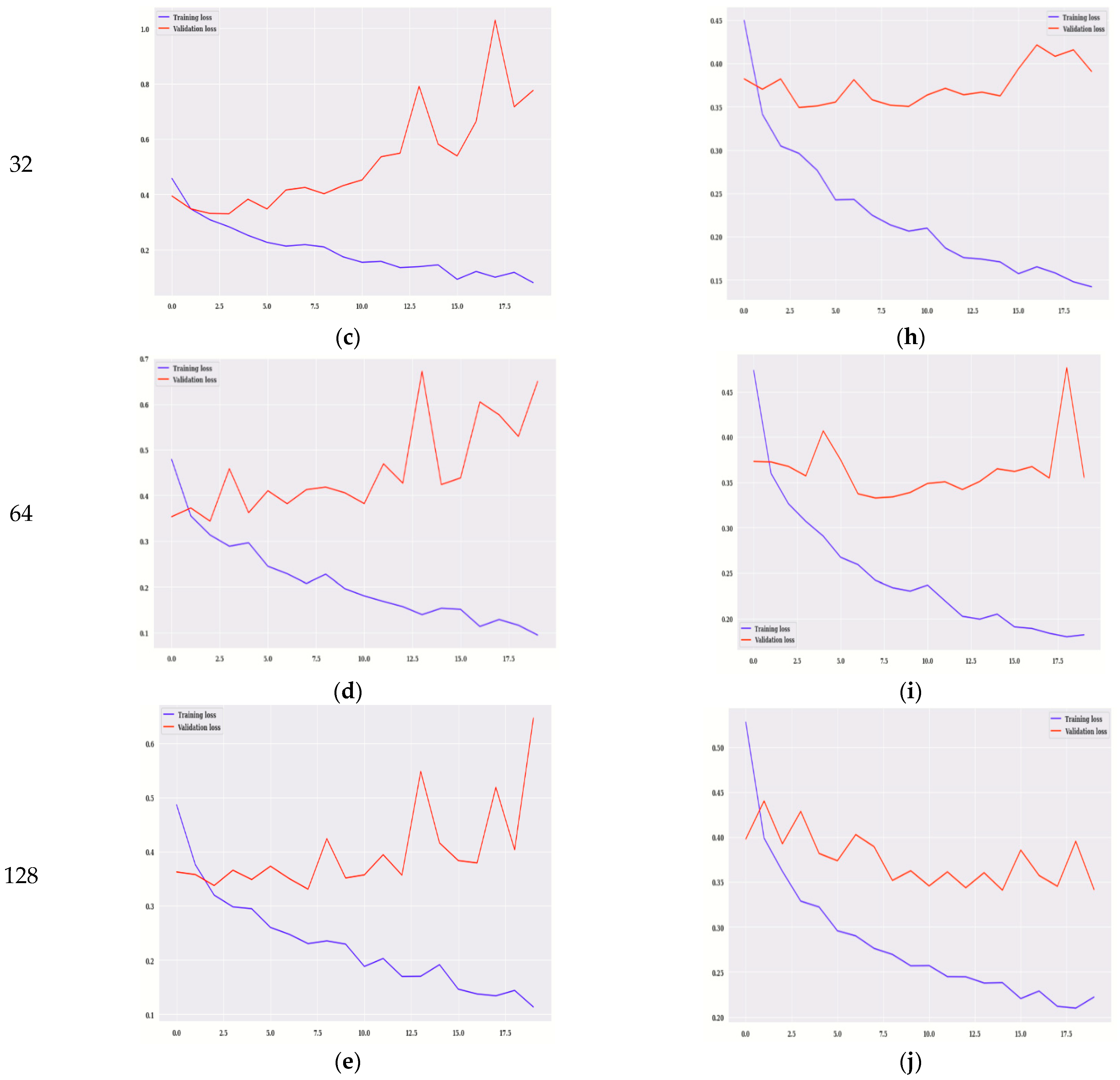
The confusion matrix provided predictions of true and false values as shown in
Figure 8. True labels are indicated vertically, and predicted labels are indicated horizontally from which False Negatives (FN), False Positives (FP), True Positives (TP), and True Negatives (TN) can be calculated. The parameter accuracy is calculated using TP, TN, FP, and FN as given in Equation (3)
Figure 8a–e shows the confusion matrix for VGG16, and
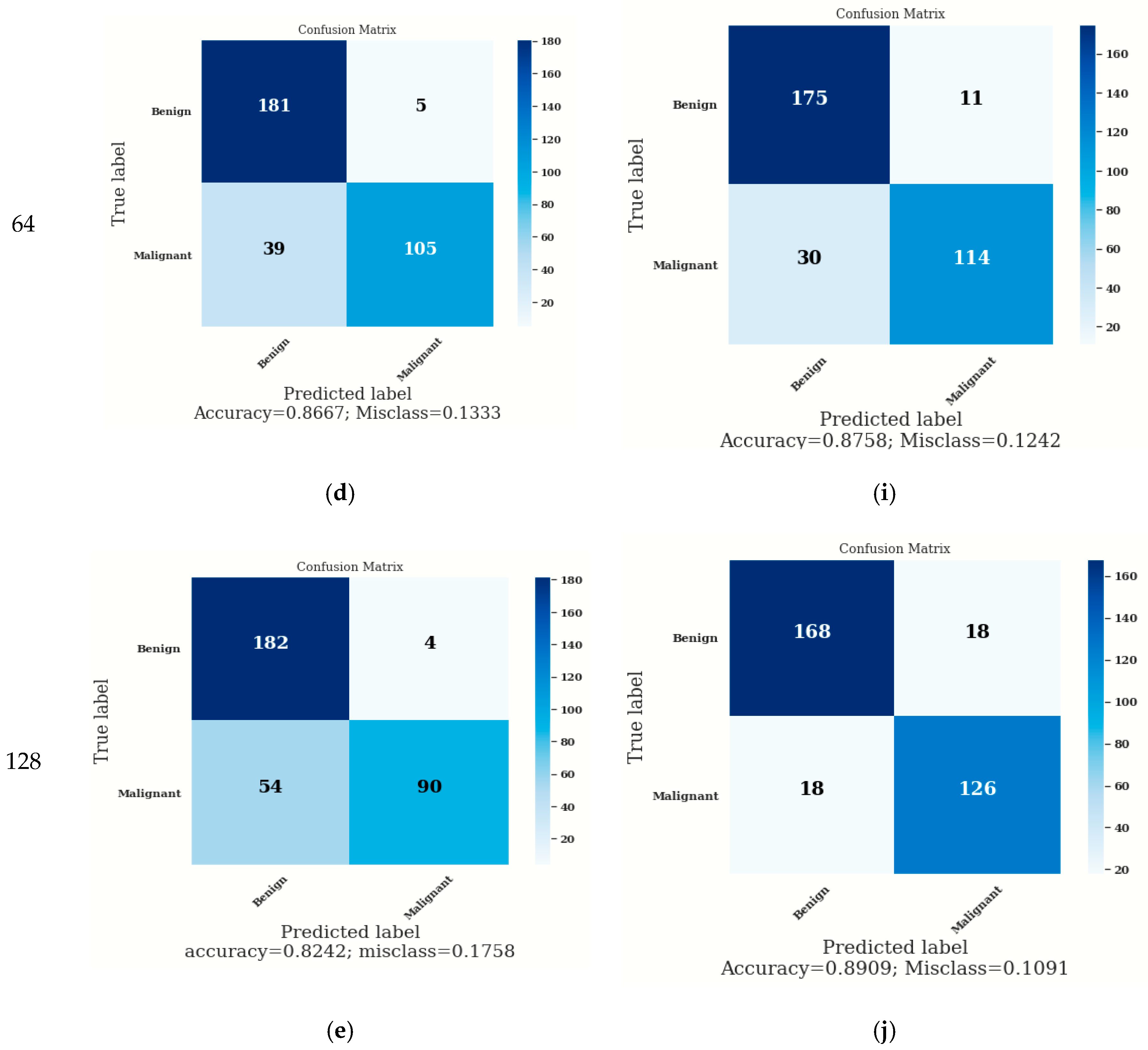
Figure 8f–j shows the confusion matrix for modified VGG16. In the case of modified VGG16, the values of accuracy are higher in comparison to the VGG16 model. On batch size 8, the accuracy on the modified VGG16 model is 86.67%, whereas, on the VGG16 model, it is 85.45%. On batch size 16, the accuracy is approximately similar to the VGG16 model and the modified VGG16 model as shown in
Figure 8b,g. with batch size 32, the accuracy on the modified VGG16 model is better (i.e., 88.18%), whereas, on the VGG16 model, it is 84.24%. On batch size 64, the accuracy on the modified VGG16 model is 87.58%, whereas, on the VGG16 model, it is 86.67%. On batch size 128, the accuracy on the modified VGG16 model is 89.09%, whereas, on the VGG16 model, it is 82.42%. From
Figure 8, it can be concluded that the modified VGG16 model is showing better accuracy as compared to VGG16 for each batch size (i.e., 8, 16, 32, 64, and 128).
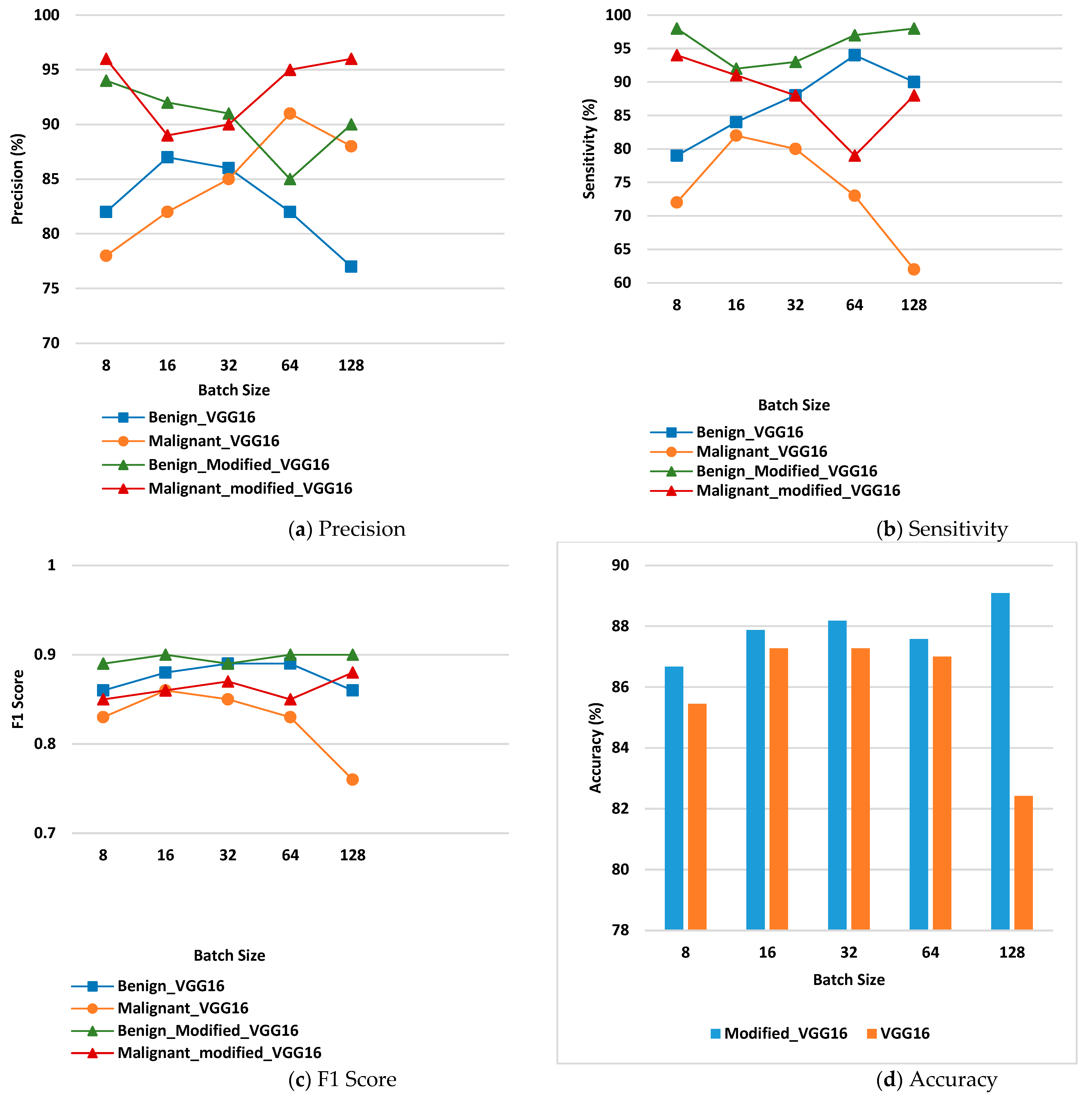
3.4. Confusion Matrix Parameter Analysis
The confusion matrix parameter values are calculated by using Equations (4), (5), and (6), respectively.
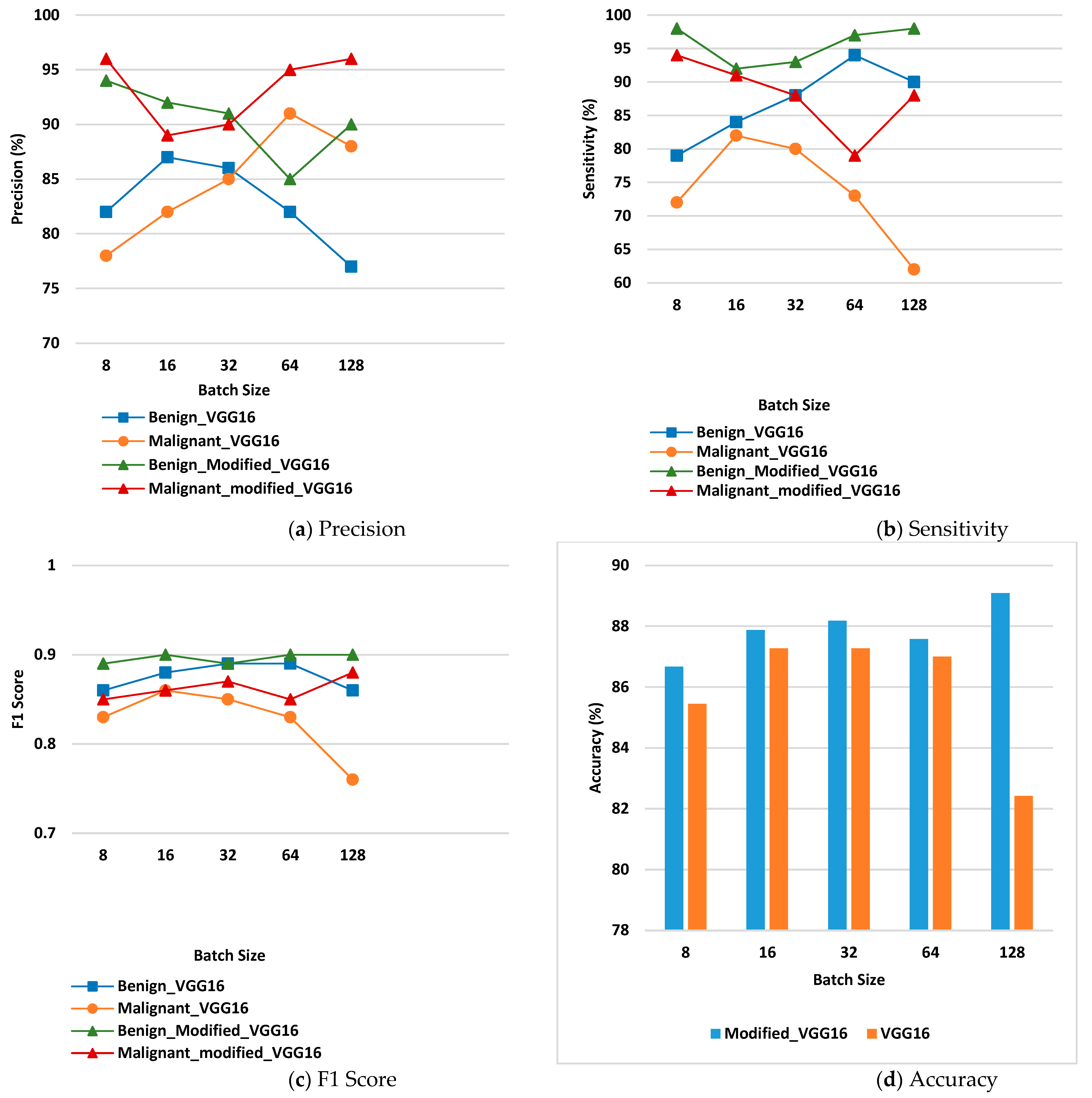
Figure 9 displays the values of confusion matrix parameter analysis for the benign and malignant class.
Figure 9a displays precision for benign and malignant disease class on the VGG16 model and the modified VGG16 model. From the figure, it can be seen that the values of precision are higher in case of the modified VGG16 model at each batch size for benign as well as malignant class. For benign class, modified VGG16 is working best for batch size 8, whereas, for malignant class, it is working best for batch size 8 and 128.
Figure 9b shows the values of sensitivity for the benign and malignant disease classes on the VGG16 model and the modified VGG16 model. From the figure, it can be seen that the values of sensitivity are higher in the case of the modified VGG16 model at each batch size for benign as well as malignant class. For benign class, modified VGG16 is working best for batch size 8 and 128 whereas, for malignant class, it is working best for batch size 8 and 16.
Figure 9c shows the values of F1 score for VGG16 and the modified VGG16 model. The values of F1 Score are higher in the case of the modified VGG16 model at each batch size for benign as well as malignant class as compared to the VGG16 model. For benign class, modified VGG16 is working best for batch size 16, 64 and 128 whereas; for malignant class, it is working best for batch size 128.
Figure 9d shows the accuracy values of benign and malignant disease class on VGG16 and the modified VGG16 model. From the figure, it is detected that the overall ac-curacy is high in the case of the modified VGG16 model at each batch size as compared to the VGG16 model. Modified VGG16 is working best for batch size 128 in terms of overall accuracy, and the value is 89.09%.



 and
and 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}