
COVID-Net CXR-S: Deep Convolutional Neural Network for Severity Assessment of COVID-19 Cases from Chest X-ray Images

 , , and
, , and 
Abstract
:1. Introduction
2. Material and Methods
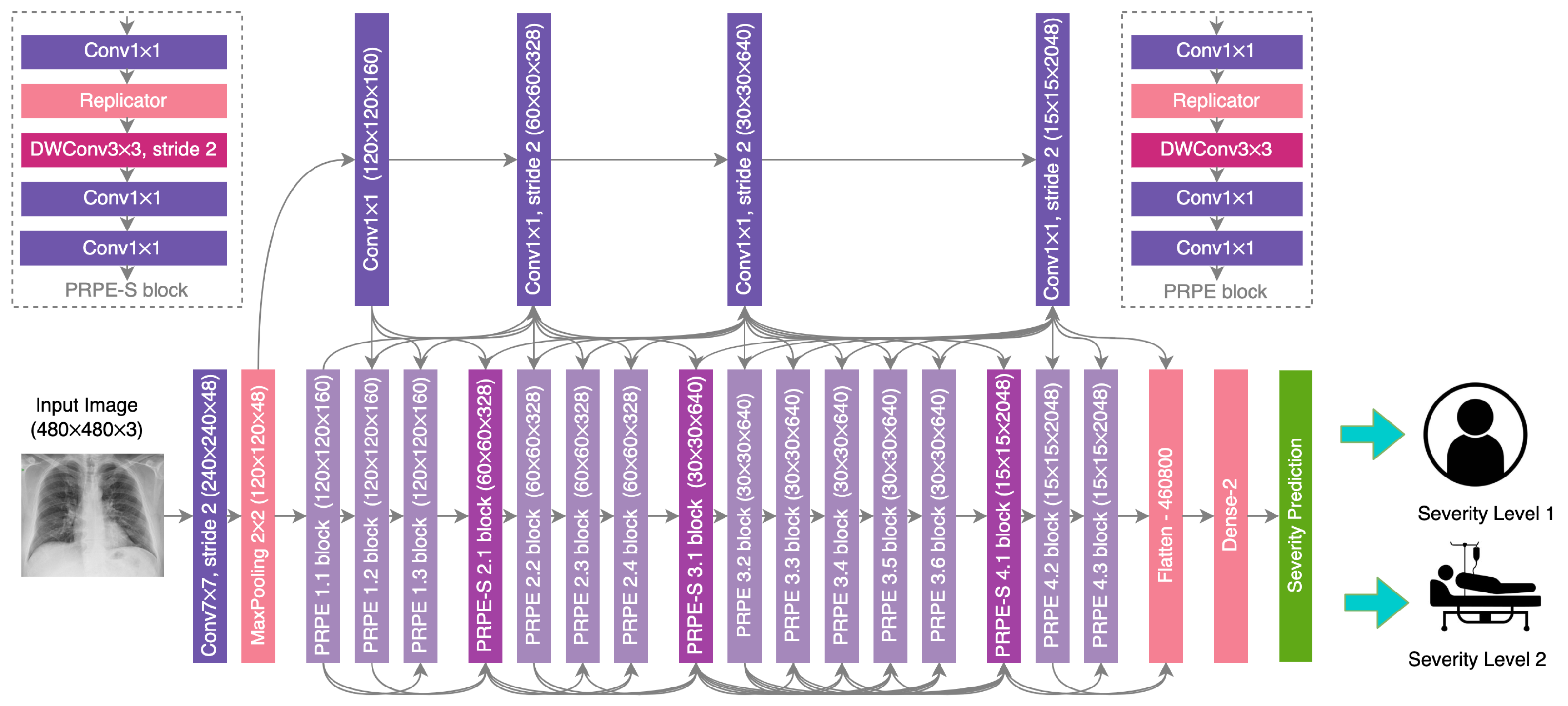
2.1. Network Design
2.2. Data Preparation
2.3. Network Training
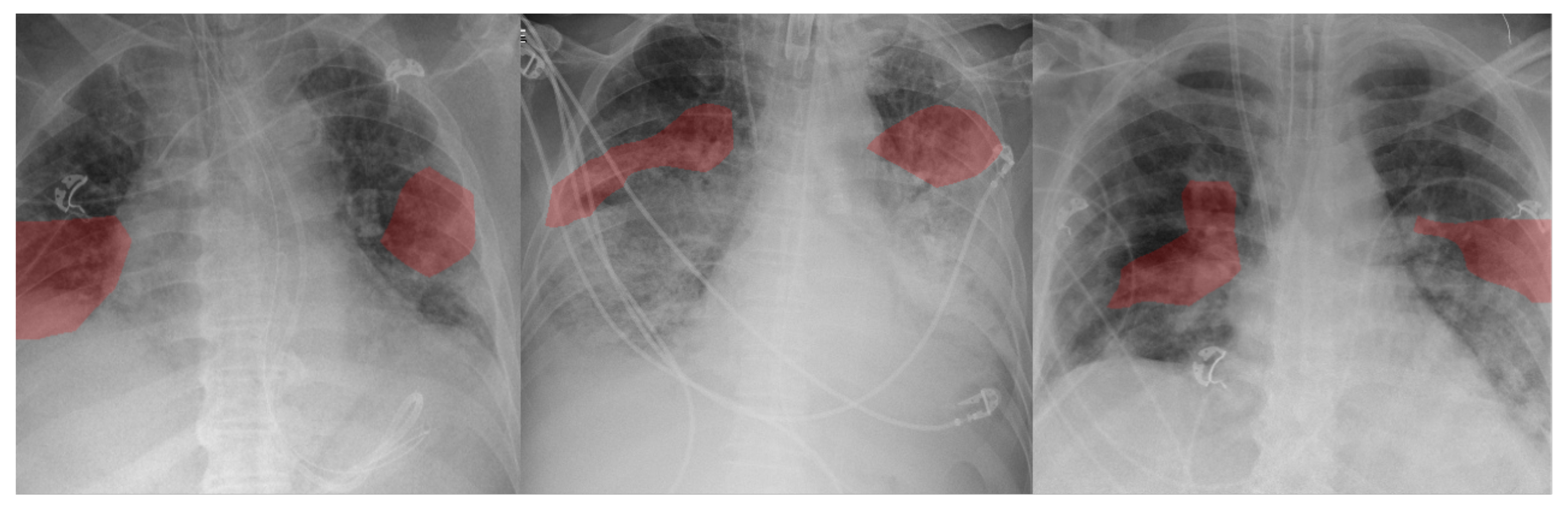
2.4. Explainability-Driven Performance Validation
2.5. Radiologist Validation
3. Results and Discussion
3.1. Quantitative Results
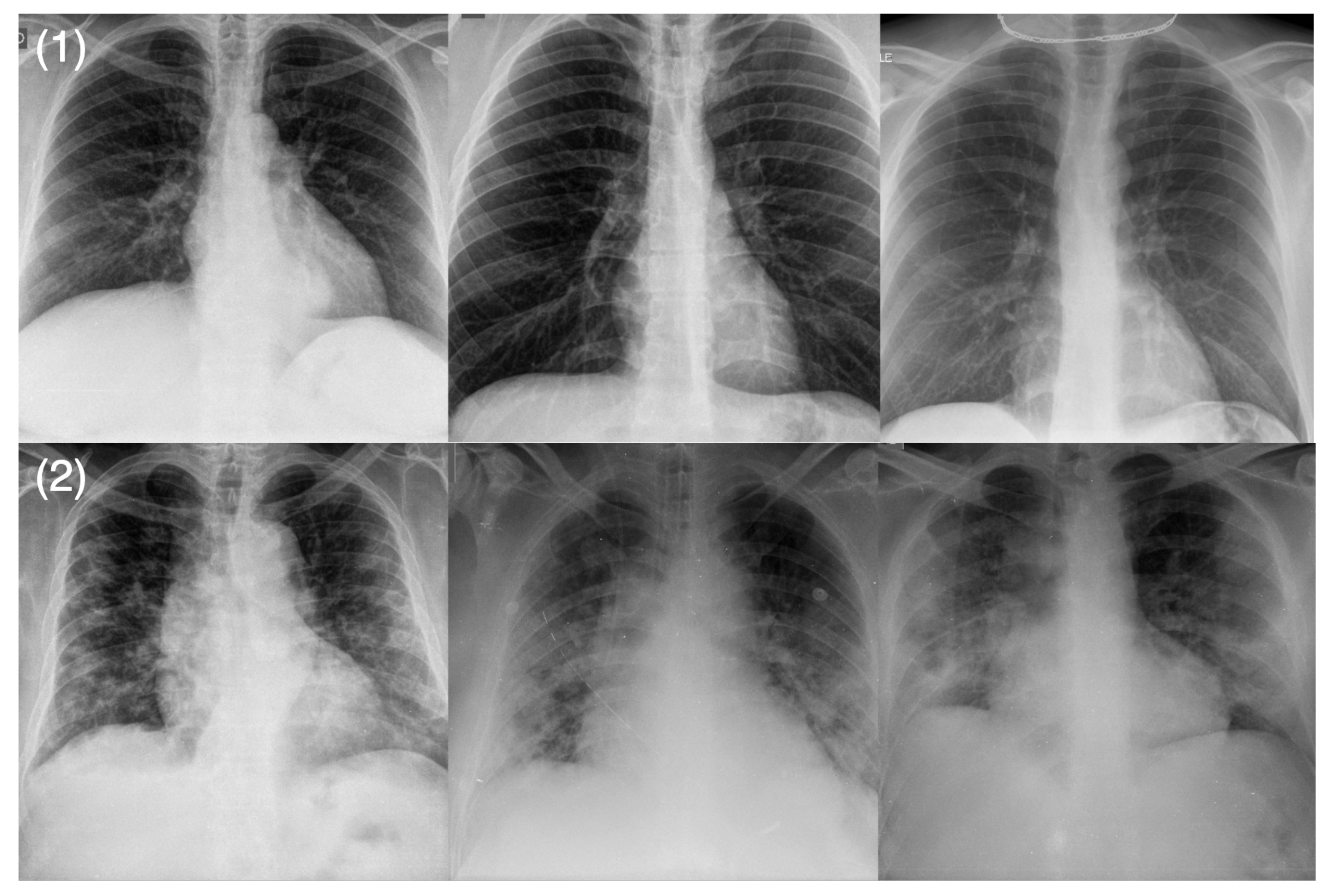
3.2. Qualitative Results
3.3. Radiologist Analysis
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pak, A.; Adegboye, O.A.; Adekunle, A.I.; Rahman, K.M.; McBryde, E.S.; Eisen, D.P. Economic consequences of the COVID-19 outbreak: The need for epidemic preparedness. Front. Public Health 2020, 8, 241. [Google Scholar] [CrossRef] [PubMed]
- Azoulay, E.; Beloucif, S.; Guidet, B.; Pateron, D.; Vivien, B.; Le Dorze, M. Admission decisions to intensive care units in the context of the major COVID-19 outbreak: Local guidance from the COVID-19 Paris-region area. Crit. Care 2020, 24, 293. [Google Scholar] [CrossRef] [PubMed]
- Tyrrell, C.S.; Mytton, O.T.; Gentry, S.V.; Thomas-Meyer, M.; Allen, J.L.Y.; Narula, A.A.; McGrath, B.; Lupton, M.; Broadbent, J.; Ahmed, A.; et al. Managing intensive care admissions when there are not enough beds during the COVID-19 pandemic: A systematic review. Thorax 2021, 76, 302–312. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Lin, Z.Q.; Wong, A. COVID-Net: A Tailored Deep Convolutional Neural Network Design for Detection of COVID-19 Cases from Chest X-ray Images. Sci. Rep. 2020, 10, 19549. [Google Scholar] [CrossRef] [PubMed]
- Jain, R.; Gupta, M.; Taneja, S.; Hemanth, D.J. Deep learning based detection and analysis of COVID-19 on chest X-ray images. Appl. Intell. 2021, 51, 1690–1700. [Google Scholar] [CrossRef] [PubMed]
- Sahlol, A.T.; Yousri, D.; Ewees, A.A.; Al-Qaness, M.A.; Damasevicius, R.; Abd Elaziz, M. COVID-19 image classification using deep features and fractional-order marine predators algorithm. Sci. Rep. 2020, 10, 15364. [Google Scholar]
- Gunraj, H.; Sabri, A.; Koff, D.; Wong, A. COVID-Net CT-2: Enhanced Deep Neural Networks for Detection of COVID-19 from Chest CT Images Through Bigger, More Diverse Learning. arXiv 2021, arXiv:2101.07433. [Google Scholar]
- Gunraj, H.; Wang, L.; Wong, A. COVIDNet-CT: A Tailored Deep Convolutional Neural Network Design for Detection of COVID-19 Cases from Chest CT Images. Front. Med. 2020, 7, 608525. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Yang, X.; Zhang, S.; Zhao, J.; Zhang, Y.; Xing, E.; Xie, P. Sample-efficient deep learning for covid-19 diagnosis based on ct scans. MedRxiv 2020. [Google Scholar] [CrossRef]
- Zhang, K.; Liu, X.; Shen, J.; Li, Z.; Sang, Y.; Wu, X.; Zha, Y.; Liang, W.; Wang, C.; Wang, K.; et al. Clinically applicable AI system for accurate diagnosis, quantitative measurements, and prognosis of COVID-19 pneumonia using computed tomography. Cell 2020, 181, 1423–1433. [Google Scholar] [CrossRef]
- Wong, A.; Lin, Z.Q.; Wang, L.; Chung, A.G.; Shen, B.; Abbasi, A.; Hoshmand-Kochi, M.; Duong, T.Q. COVIDNet-S: Towards computer-aided severity assessment via training and validation of deep neural networks for geographic extent and opacity extent scoring of chest X-rays for SARS-CoV-2 lung disease severity. arXiv 2020, arXiv:2005.12855. [Google Scholar]
- Cohen, J.P.; Dao, L.; Roth, K.; Morrison, P.; Bengio, Y.; Abbasi, A.F.; Shen, B.; Mahsa, H.K.; Ghassemi, M.; Li, H.; et al. Predicting covid-19 pneumonia severity on chest x-ray with deep learning. Cureus 2020, 12, e9448. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.; Shafiee, M.J.; Chwyl, B.; Li, F. FermiNets: Learning generative machines to generate efficient neural networks via generative synthesis. arXiv 2018, arXiv:1809.05989. [Google Scholar]
- Wong, A. NetScore: Towards Universal Metrics for Large-scale Performance Analysis of Deep Neural Networks for Practical On-Device Edge Usage. arXiv 2018, arXiv:1806.05512. [Google Scholar]
- Radiological Society of North America. RSNA Pneumonia Detection Challenge. Available online: https://www.kaggle.com/c/rsna-pneumonia-detection-challenge/data (accessed on 1 January 2021).
- Radiological Society of North America. COVID-19 Radiography Database. Available online: https://www.kaggle.com/tawsifurrahman/covid19-radiography-database (accessed on 1 January 2021).
- Chung, A. Figure 1 COVID-19 Chest X-ray Data Initiative. Available online: https://github.com/agchung/Figure1-COVID-chestxray-dataset (accessed on 1 January 2021).
- Chung, A. ActualMed COVID-19 Chest X-ray Data Initiative. Available online: https://github.com/agchung/Actualmed-COVID-chestxray-dataset (accessed on 1 January 2021).
- Cohen, J.P.; Morrison, P.; Dao, L. COVID-19 image data collection. arXiv 2020, arXiv:2003.11597. [Google Scholar]
- Tsai, E.B.; Simpson, S.; Lungren, M.; Hershman, M.; Roshkovan, L.; Colak, E.; Erickson, B.J.; Shih, G.; Stein, A.; Kalpathy-Cramer, J.; et al. The RSNA International COVID-19 Open Annotated Radiology Database (RICORD). Radiology 2021, 299, 203957. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.Q.; Shafiee, M.J.; Bochkarev, S.; Jules, M.S.; Wang, X.Y.; Wong, A. Do Explanations Reflect Decisions? A Machine-centric Strategy to Quantify the Performance of Explainability Algorithms. arXiv 2019, arXiv:1910.07387. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 30 June 2016; pp. 770–778. [Google Scholar]
- Rajpurkar, P.; Irvin, J.; Zhu, K.; Yang, B.; Mehta, H.; Duan, T.; Ding, D.; Bagul, A.; Langlotz, C.; Shpanskaya, K.; et al. CheXNet: Radiologist-Level Pneumonia Detection on Chest X-rays with Deep Learning. arXiv 2017, arXiv:1711.05225. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Layer Name | Output Size | Specs (Filter Shape, Filter Number) |
|---|---|---|
| Conv1 | , 48 | |
| PRPE 1.1 | , 160 | |
| PRPE 1.2 | , 160 | |
| PRPE 1.3 | , 160 | |
| PRPE 2.1 | , 328 | |
| PRPE 2.2 | , 328 | |
| PRPE 2.3 | , 328 | |
| PRPE 2.4 | , 328 | |
| PRPE 3.1 | , 640 | |
| PRPE 3.2 | , 640 | |
| PRPE 3.3 | , 640 | |
| PRPE 3.4 | , 640 | |
| PRPE 3.5 | , 640 | |
| PRPE 3.6 | , 640 | |
| PRPE 4.1 | , 2048 | |
| PRPE 4.2 | , 2048 | |
| PRPE 4.3 | , 2048 | |
| Dense | 2 | , 2 |
| Age | Mean ± Std | |
|---|---|---|
| <20 | 2 (0.8%) | |
| 20–29 | 7 (2.7%) | |
| 30–39 | 26 (10.1%) | |
| 40–49 | 37 (14.3%) | |
| 50–59 | 58 (22.5%) | |
| 60–69 | 58 (22.5%) | |
| 70–79 | 42 (16.3%) | |
| 80–89 | 22 (8.5%) | |
| 90+ | 6 (2.3%) | |
| Sex | ||
| Male | 161 (62.4%) | |
| Female | 97 (37.6%) | |
| Imaging view | ||
| AP | 505 (55.6%) | |
| PA | 5 (0.6%) | |
| Unknown | 399 (43.9%) |
| Metric | Sensitivity (Level 1) | Sensitivity (Level 2) | PPV (Level 1) | PPV (Level 2) | AUC | Accuracy | |
|---|---|---|---|---|---|---|---|
| Network | |||||||
| CheXNet [23] | 93.88% | 63.46% | 82.88% | 84.62% | 83.62 % | 83.33% | |
| ResNet-50 [22] | 91.84% | 78.85% | 89.11% | 83.67% | 91.88% | 87.33% | |
| COVID-Net CXR-S | 92.3% | 92.85% | 87.27% | 95.78% | 96.09% | 92.66% | |
| Network | Parameters (M) | FLOPs (G) |
|---|---|---|
| CheXNet [23] | 8.1 | 26.0 |
| ResNet-50 [22] | 23.6 | 35.5 |
| COVID-Net CXR-S | 8.8 | 11.1 |
| Severity Level | Level 1 | Level 2 |
|---|---|---|
| Level 1 | 48 | 4 |
| Level 2 | 7 | 91 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aboutalebi, H.; Pavlova, M.; Shafiee, M.J.; Sabri, A.; Alaref, A.; Wong, A. COVID-Net CXR-S: Deep Convolutional Neural Network for Severity Assessment of COVID-19 Cases from Chest X-ray Images. Diagnostics 2022, 12, 25. https://doi.org/10.3390/diagnostics12010025
Aboutalebi H, Pavlova M, Shafiee MJ, Sabri A, Alaref A, Wong A. COVID-Net CXR-S: Deep Convolutional Neural Network for Severity Assessment of COVID-19 Cases from Chest X-ray Images. Diagnostics. 2022; 12(1):25. https://doi.org/10.3390/diagnostics12010025
Chicago/Turabian StyleAboutalebi, Hossein, Maya Pavlova, Mohammad Javad Shafiee, Ali Sabri, Amer Alaref, and Alexander Wong. 2022. "COVID-Net CXR-S: Deep Convolutional Neural Network for Severity Assessment of COVID-19 Cases from Chest X-ray Images" Diagnostics 12, no. 1: 25. https://doi.org/10.3390/diagnostics12010025
APA StyleAboutalebi, H., Pavlova, M., Shafiee, M. J., Sabri, A., Alaref, A., & Wong, A. (2022). COVID-Net CXR-S: Deep Convolutional Neural Network for Severity Assessment of COVID-19 Cases from Chest X-ray Images. Diagnostics, 12(1), 25. https://doi.org/10.3390/diagnostics12010025