
Feasibility of Portable Microwave Imaging Device for Breast Cancer Detection

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. MG, US, DCE-MRI, and FDG-PET/CT Protocol
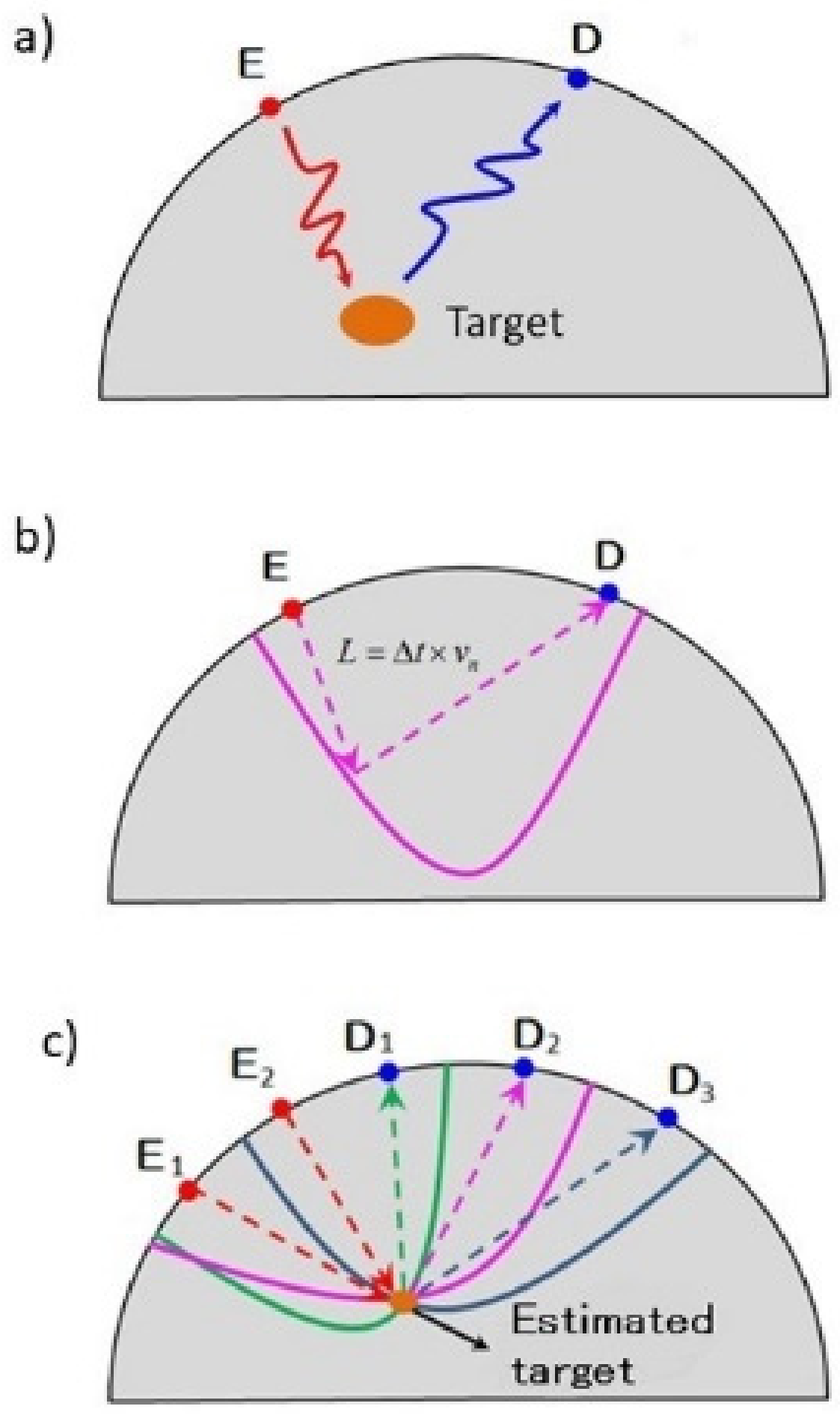
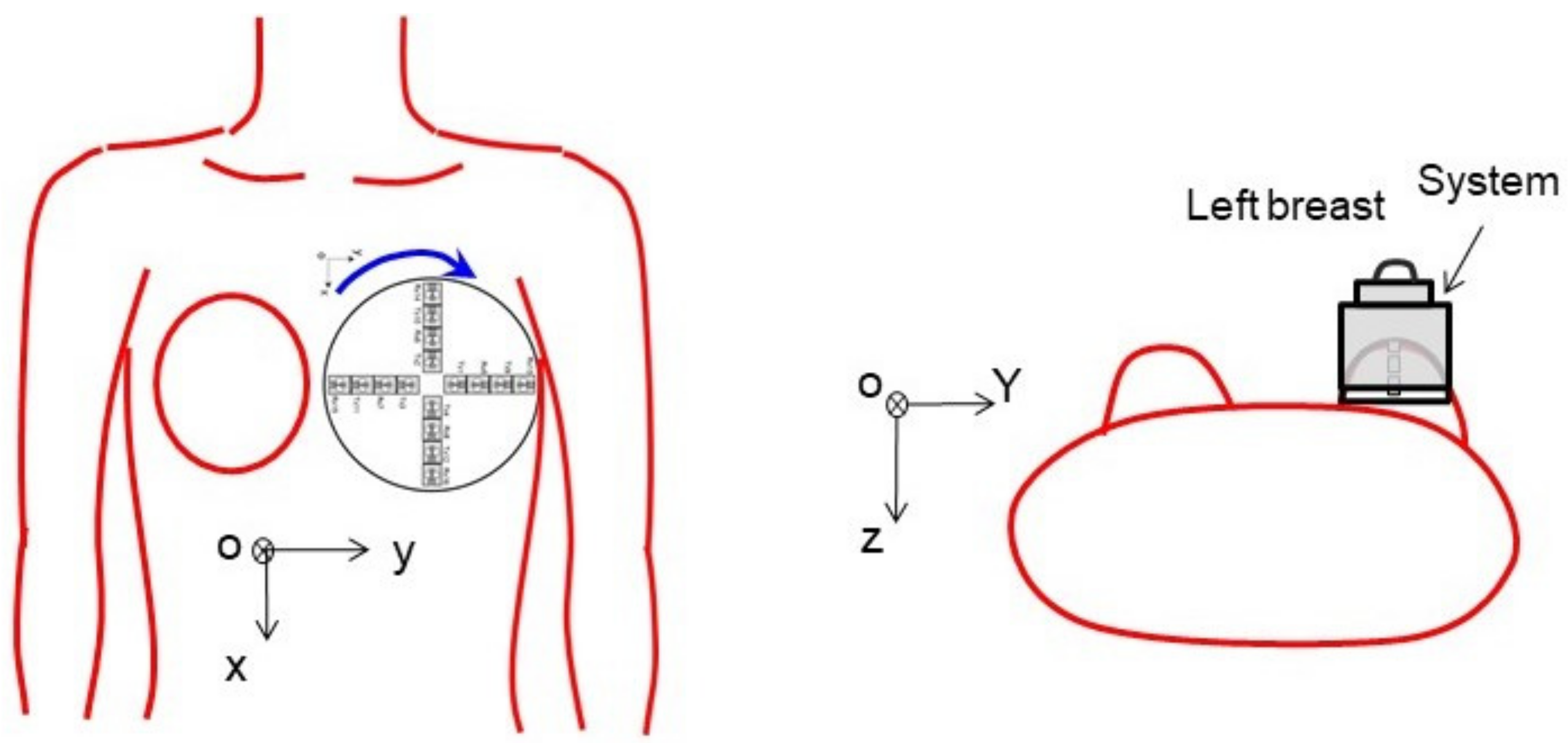
2.3. Microwave Imaging Protocol
2.4. Pathological Evaluation
2.5. Image Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- DeSantis, C.E.; Ma, J.; Gaudet, M.M.; Newman, L.A.; Miller, K.D.; Goding Sauer, A.; Jemal, A.; Siegel, R.L. Breast cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 438–451. [Google Scholar] [CrossRef]
- Tabar, L.; Gad, A.; Holmberg, L.H.; Ljungquist, U.; Group, K.C.P.; Fagerberg, C.J.G.; Baldetorp, L.; Gröntoft, O.; Lundström, B.; Månson, J.C.; et al. Reduction in mortality from breast cancer after mass screening with mammography. Randomised trial from the Breast Cancer Screening Working Group of the Swedish National Board of Health and Welfare. Lancet 1985, 1, 829–832. [Google Scholar] [CrossRef]
- Kolb, T.M.; Lichy, J.; Newhouse, J.H. Comparison of the Performance of Screening Mammography, Physical Examination, and Breast US and Evaluation of Factors that Influence Them: An Analysis of 27,825 Patient Evaluations. Radiology 2002, 225, 165–175. [Google Scholar] [CrossRef] [Green Version]
- Bae, J.-M.; Kim, E.H. Breast Density and Risk of Breast Cancer in Asian Women: A Meta-analysis of Observational Studies. J. Prev. Med. Public Health 2016, 49, 367–375. [Google Scholar] [CrossRef] [Green Version]
- Yaffe, M.J.; Mainprize, J.G. Risk of radiation-induced breast cancer from mammographic screening. Radiology 2012, 264, 306. [Google Scholar] [CrossRef] [Green Version]
- Ohuchi, N.; Suzuki, A.; Sobue, T.; Kawai, M.; Yamamoto, S.; Zheng, Y.-F.; Shiono, Y.N.; Saito, H.; Kuriyama, S.; Tohno, E.; et al. Sensitivity and specificity of mammography and adjunctive ultrasonography to screen for breast cancer in the Japan Strategic Anti-cancer Randomized Trial (J-START): A randomised controlled trial. Lancet 2016, 387, 341–348. [Google Scholar] [CrossRef]
- Chiarelli, A.M.; Blackmore, K.M.; Muradali, D.; Done, S.J.; Majpruz, V.; Weerasinghe, A.; Mirea, L.; Eisen, A.; Rabeneck, L.; Warner, E. Performance Measures of Magnetic Resonance Imaging Plus Mammography in the High Risk Ontario Breast Screening Program. J. Natl. Cancer Inst. 2020, 112, 136–144. [Google Scholar] [CrossRef]
- Tedeschi, E.; Caranci, F.; Giordano, F.; Angelini, V.; Cocozza, S.; Brunetti, A. Gadolinium retention in the body: What we know and what we can do. La Radiol. Med. 2017, 122, 589–600. [Google Scholar] [CrossRef] [Green Version]
- Fujioka, T.; Kubota, K.; Toriihara, A.; Machida, Y.; Okazawa, K.; Nakagawa, T.; Saida, Y.; Tateishi, U. Tumor characteristics of ductal carcinoma in situ of breast visualized on [F-18] fluorodeoxyglucose-positron emission tomography/computed tomography: Results from a retrospective study. World J. Radiol. 2016, 8, 743–749. [Google Scholar]
- Fujioka, T.; Kubota, K.; Kikuchi, Y.; Tsuchiya, J.; Tateishi, U.; Kasaharak, M.; Oda, G.; Ishiba, T.; Nakagawa, T. The feasibility of using 18F-FDG-PET/CT in patients with mucinous breast carcinoma. Nucl. Med. Commun. 2018, 39, 1033–1038. [Google Scholar] [CrossRef]
- Sugitani, T.; Kubota, S.-I.; Kuroki, S.-I.; Sogo, K.; Arihiro, K.; Okada, M.; Kadoya, T.; Hide, M.; Oda, M.; Kikkawa, T. Complex permittivities of breast tumor tissues obtained from cancer surgeries. Appl. Phys. Lett. 2014, 104, 253702. [Google Scholar] [CrossRef]
- Moloney, B.M.; O’Loughlin, D.; Abd Elwahab, S.; Kerin, M.J. Breast Cancer Detection—A Synopsis of Conventional Modalities and the Potential Role of Microwave Imaging. Diagnostics 2020, 10, 103. [Google Scholar] [CrossRef] [Green Version]
- Aldhaeebi, M.A.; Alzoubi, K.; Almoneef, T.S.; Bamatraf, S.M.; Attia, H.; Ramahi, O.M. Review of Microwaves Techniques for Breast Cancer Detection. Sensors 2020, 20, 2390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, H.; Sasada, S.; Kadoya, T.; Okada, M.; Arihiro, K.; Xiao, X.; Kikkawa, T. Detectability of Breast Tumor by a Hand-held Impulse-Radar Detector: Performance Evaluation and Pilot Clinical Study. Sci. Rep. 2017, 7, 16353. [Google Scholar] [CrossRef] [Green Version]
- Song, H.; Azhari, A.; Xiao, X.; Suematsu, E.; Watanabe, H.; Kikkawa, T. Microwave Imaging Using CMOS Integrated Circuits with Rotating 4 × 4 Antenna Array on a Breast Phantom. Int. J. Antennas Propag. 2017, 2017, 6757048. [Google Scholar] [CrossRef] [Green Version]
- Song, H.; Kono, H.; Seo, Y.; Azhari, A.; Somei, J.; Suematsu, E.; Watarai, Y.; Ota, T.; Watanabe, H.; Hiramatsu, Y.; et al. A radar-based breast cancer detection system using CMOS integrated circuits. IEEE Access 2015, 3, 2111–2121. [Google Scholar] [CrossRef]
- Sugitani, T.; Kubota, S.; Toya, A.; Xiao, X.; Kikkawa, T. A Compact 4 ×× 4 Planar UWB Antenna Array for 3-D Breast Cancer Detection. IEEE Antennas Wirel. Propag. Lett. 2013, 12, 733–736. [Google Scholar] [CrossRef]
- Sasada, S.; Masumoto, N.; Song, H.; Kajitani, K.; Emi, A.; Kadoya, T. Portable impulse-radar detector for breast cancer: A pilot study. J. Med. Imaging 2018, 5, 025502. [Google Scholar] [CrossRef] [PubMed]
- Breast Imaging Reporting and Data System Atlas, 5th ed.; American College of Radiology: Reston, VA, USA, 2013; Available online: https://www.acr.org/Clinical-Resources/Reporting-and-Data-Systems/Bi-Rads (accessed on 4 December 2021).
- Janjic, A.; Cayoren, M.; Akduman, I.; Yilmaz, T.; Onemli, E.; Bugdayci, O.; Aribal, M.E. SAFE: A Novel Microwave Imaging System Design for Breast Cancer Screening and Early Detection—Clinical Evaluation. Diagnostics 2021, 11, 533. [Google Scholar] [CrossRef] [PubMed]
- Cynthia E Keen. 2021. Available online: https://physicsworld.com/a/microwave-imaging-could-provide-safer-more-comfortable-breast-cancer-screening/?fr=operanews (accessed on 4 December 2021).
- Moloney, B.M.; McAnena, P.F.; Elwahab, S.M.; Fasoula, A.; Duchesne, L.; Gil Cano, J.D.; Glynn, C.; O’Connell, A.; Ennis, R.; Lowery, A.J.; et al. The Wavelia Microwave Breast Imaging system–tumour discriminating features and their clinical usefulness. Br. J. Radiol. 2021, 94, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Moloney, B.M.; McAnena, P.F.; Elwahab, S.M.A.; Fasoula, A.; Duchesne, L.; Gil Cano, J.D.; Glynn, C.; O’Connell, A.; Ennis, R.; Lowery, A.J.; et al. Microwave Imaging in Breast Cancer–Results from the First-In-Human Clinical Investigation of the Wavelia System. Acad. Radiol. 2021, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Sani, L.; Vispa, A.; Loretoni, R.; Duranti, M.; Ghavami, N.; Alvarez Sánchez-Bayuela, D.; Caschera, S.; Paoli, M.; Bigotti, A.; Badia, M.; et al. Breast lesion detection through MammoWave device: Empirical detection capability assessment of microwave images’ parameters. PLoS ONE 2021, 16, e0250005. [Google Scholar] [CrossRef] [PubMed]
- Mun, H.; Shin, H.; Kim, H.; Cha, J. Screening-detected calcified and non-calcified ductal carcinoma in situ: Differences in the imaging and histopathological features. Clin. Radiol. 2013, 68, e27–e35. [Google Scholar] [CrossRef]
- Preece, A.W.; Craddock, I.; Shere, M.; Jones, L.; Winton, H.L. MARIA M4: Clinical evaluation of a prototype ultrawideband radar scanner for breast cancer detection. J. Med. Imaging 2016, 3, 033502. [Google Scholar] [CrossRef] [PubMed]
- Islam, T.; Mahmud, M.Z.; Kibria, S.; Samsuzzaman, M. A Low Cost and Portable Microwave Imaging System for Breast Tumor Detection Using UWB Directional Antenna array. Sci. Rep. 2019, 9, 15491. [Google Scholar] [CrossRef] [Green Version]
- Duchesne, L.; Fasoula, A.; Kaverine, E.; Robin, G.; Bernard, J.G. Wavelia Microwave Breast Imaging: Identification and Mitigation of possible Sources of Measurement Uncertainty, 2019. In Proceedings of the 13th European Conference on Antennas and Propagation IEEE (EuCAP), Krakow, Poland, 31 March–5 April 2019. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No of Case | Age | BMI | Tumor Side | Histology | Tumor Size (mm) | ER | PR | HER2 | Ki 67 (%) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Invasive Lesion | Total | |||||||||
| 1 | 69 | 25.9 | R | IDC | 28.0 | 112.0 | + | + | - | 4.8 |
| 2 | L | IDC | 38.0 | 85.0 | + | + | - | 35.2 | ||
| 3 | 78 | 17.2 | R | DCIS | 0 | 45.0 | + | + | + | 6.7 |
| 4 | 37 | 25.4 | R | IDC | 60.0 | 60.0 | + | + | - | 3.0 |
| 5 | 66 | 19.1 | R | IDC | 120.0 | 120.0 | + | + | - | 32.7 |
| 6 | 73 | 19.0 | L | IDC | 14.0 | 40.0 | + | + | 12.7 | |
| 7 | 47 | 27.8 | L | IDC | 14.0 | 14.0 | + | + | - | 22.7 |
| 8 | 60 | 17.3 | L | IDC | 0.6 | 60.0 | + | + | - | 15.0 |
| 9 | 40 | 20.6 | R | DCIS | 0 | 60.0 | - | - | - | 20.0 |
| 10 | 67 | 20.2 | L | IDC | 21.0 | 60.0 | + | + | + | 50.0 |
| No of Case | MG | US | MRI | PET/CT | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Breast Density | Finding | Cat | Finding | Size (mm) | Cat | Finding | Size (mm) | Cat | SUVmax | |
| 1 | B | Mass | 5 | Mass | 16 | 5 | Mass | 16 | 5 | NA |
| 2 | B | Mass | 5 | Mass | 23 | 5 | Mass | 46 | 5 | NA |
| 3 | B | FAD | 4 | Mass | 40 | 5 | Mass | 33 | 5 | 4.4 |
| 4 | C | Mass | 5 | Mass | 37 | 5 | Mass | 42 | 5 | 5.4 |
| 5 | B | Mass | 4 | Mass | 70 | 5 | NA | NA | NA | NA |
| 6 | C | FAD | 4 | NML | 19 | 4 | NME | 24 | 4 | 1.6 |
| 7 | B | Mass | 5 | Mass | 14 | 5 | NA | NA | NA | 5.7 |
| 8 | C | Negative | 1 | NML | 22 | 4 | NME | 28 | 5 | Negative |
| 9 | D | Negative | 1 | NML | 38 | 5 | NME | 38 | 5 | NA |
| 10 | D | Calcification | 4 | Mass | 33 | 5 | Mass | 60 | 5 | 4.7 |
| No of Case | Detection | Consistency with Cancer Lesion | Size (mm) | |
|---|---|---|---|---|
| Location | Size | 5 | ||
| 1 | positive | 5 | 5 | 5 |
| 2 | positive | 5 | 4 | 15 |
| 3 | positive | 4 | 5 | 15 |
| 4 | positive | 4 | 4 | 20 |
| 5 | positive | 4 | 4 | 30 |
| 6 | positive | 5 | 4 | 20 |
| 7 | positive | 5 | 5 | 5 |
| 8 | positive | 4 | 4 | 30 |
| 9 | positive | 5 | 4 | 20 |
| 10 | positive | 4 | 3 | 20 |
| Equipment Features (Portable) | Principle | Machine Size, Weight | Number of Cases Total Number of Cases Malignant, Benign | Grades Sensitivity, Specificity, etc. | |
|---|---|---|---|---|---|
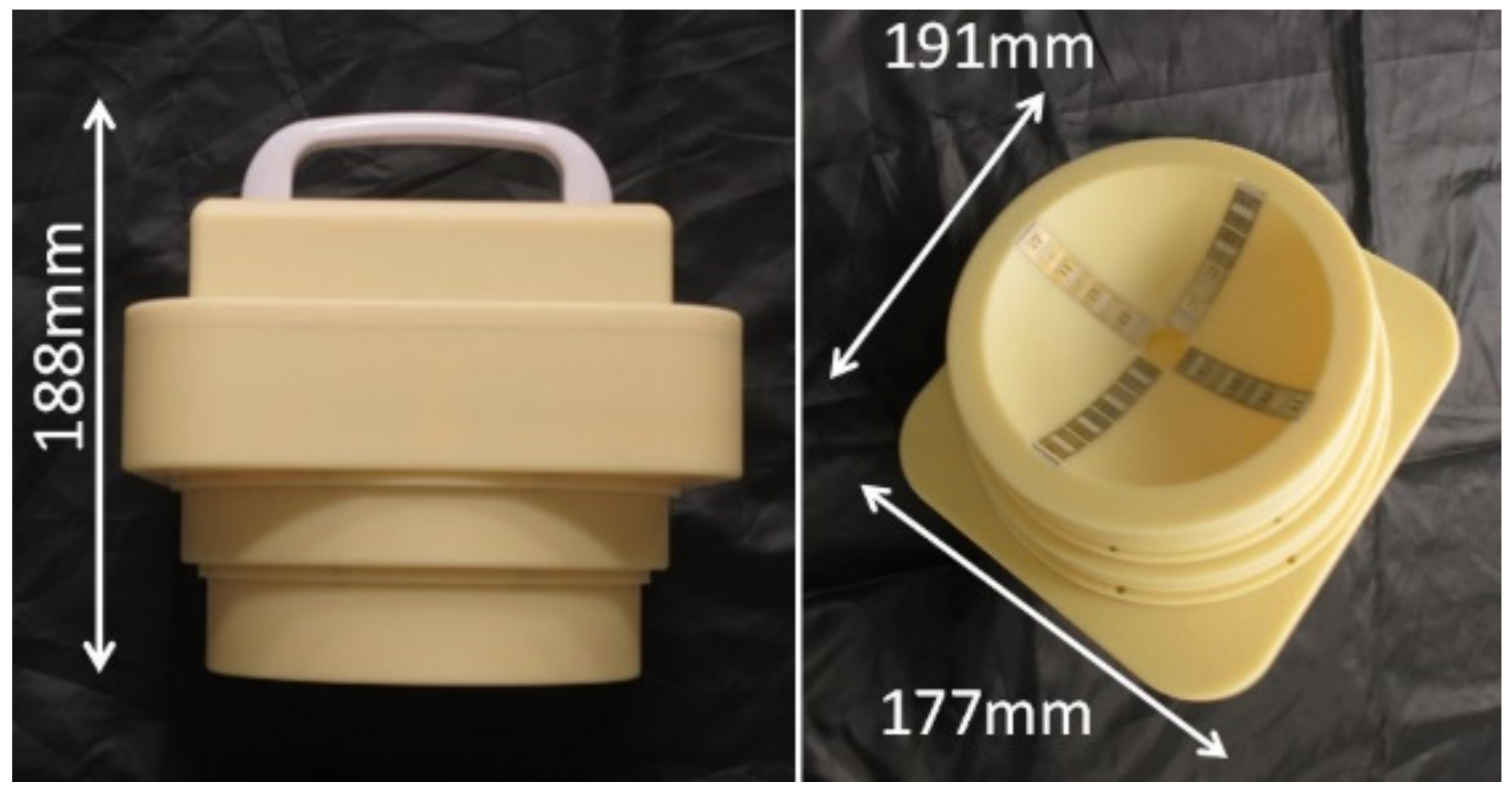
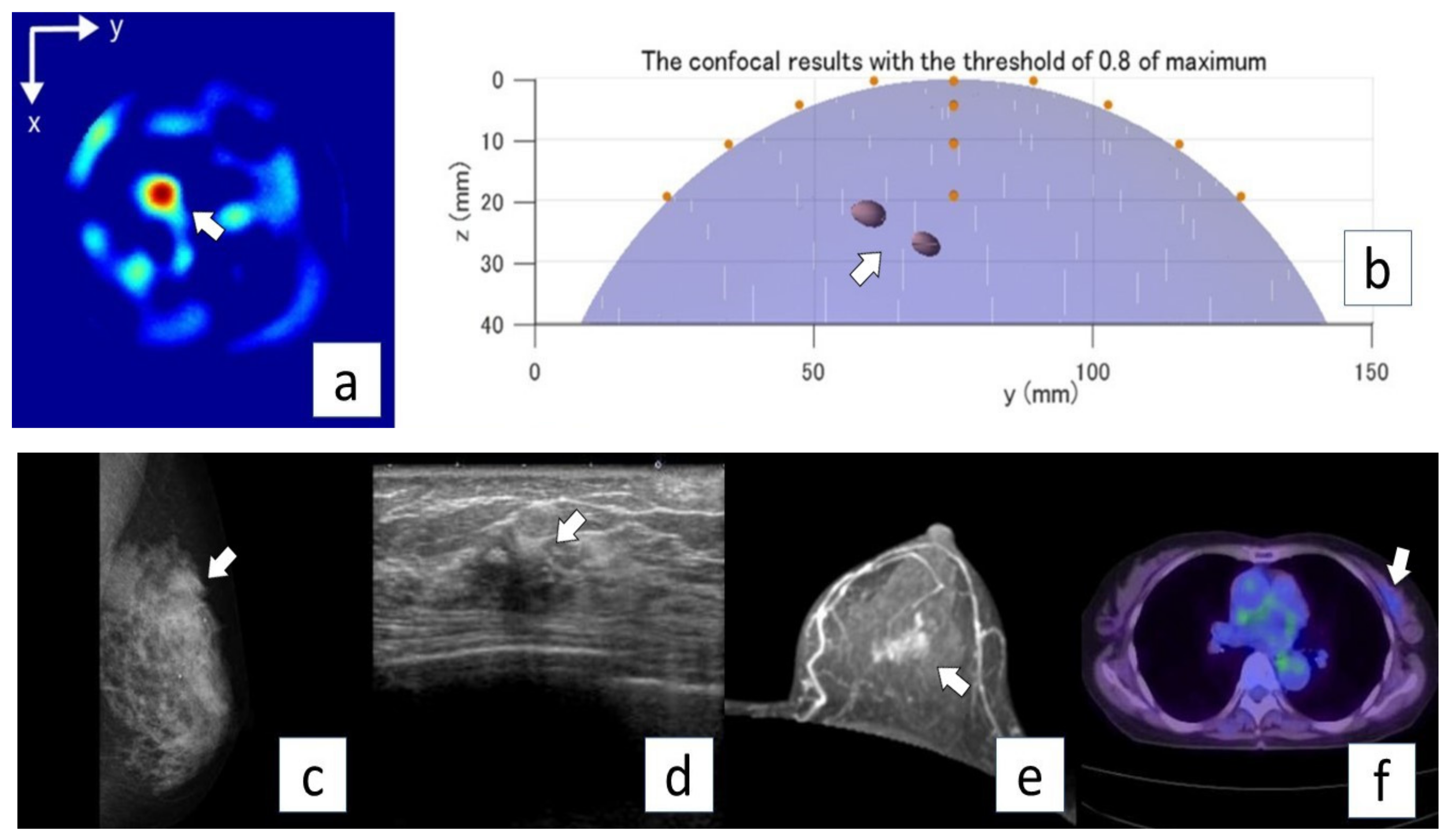
| This study | A prototype of a portable breast cancer detector using a radar-based imaging system | The core functional part of the detector comprises 65-nm technology CMOS integrated circuits covering the ultrawideband width of 3.1–10.6 GHz, which enables the generation and transmission of Gaussian monocycle pulse (GMP) and single port eight throw switching matrices for controlling the 4 × 4 cross-shaped dome antenna array. | Size: 191 × 177 × 188 mm weight: 2 kg | 10 cases (All were malignant). | All cancers were detected. |
| Sanada et al. [18] | A prototype of a portable breast cancer detector using a radar-based imaging system | The core functional part of the detector comprises 65-nm technology CMOS integrated circuits covering the ultrawideband width of 3.1–10.6 GHz, which enables the generation and transmission of Gaussian monocycle pulse(GMP) and single port eight throw switching matrices for controlling the 4 × 4 cross-shaped dome antenna array | Size: 191 × 177 × 188 mm weight: 2 kg | 5 cases (All were malignant). | All cancers were detected. |
| Aleksandar et al. [20] | SAFE (Scan and Find Early) is a novel microwave imaging device. Patients were required to lie prone on the table with one breast inserted into the coupling medium cup. The device is not portable. | Thirty-six receiving transmitter position points, a total of 1296 measurements. The operating frequency band was between 1.4 GHz and 8 GHz. | The size of the device is not stated, but a special cup is embedded in the bed. | 115 cases (benign: 66, high-risk: 8, malignant: 41). | Sensitivity: 63% |
| Cynthia E Keen. [21,22,23] | “Wavelia” including two subsystems, the optical breast contour detection (OBCD) subsystem and the MBI subsystem. The OBCD subsystem consists of a 3D stereoscopic camera placed. The device is not portable. | Eighteen equally spaced wideband Vivaldi-type antennas. Each probe illuminates the imaging domain in turn, while the remaining antennas receive the electromagnetic scattering at various angles around the circle. The probe array also moves at 5 mm intervals. | The size of the device is not stated, but a special cup is embedded in the bed. | 24 cases (11; malignant, 13; benign) | sensitivity of malignant; 81%, sensitivity of benign; 92% |
| Lorenzo Sani et al. [24] | The MammoWave; the hub is internally covered by microwave absorbers. The hub is equipped with a hole with a cup, allowing the insertion of the patient’s breast, with the patient lying in a prone position. The device is not portable. | Consists of an aluminum cylindrical hub containing two antennas, one transmitting and one receiving antenna, which operate in the 1–9 GHz frequency band. | The size of the device is not stated, but a special cup is embedded in the bed. | 103 breasts with no radiological finding (NF) and radiological findings (WF). | a sensitivity of 74% (the sensitivity of lesion detection using the device was 74%, and the sensitivity of malignant lesion was 71%. malignant lesions was 85%). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adachi, M.; Nakagawa, T.; Fujioka, T.; Mori, M.; Kubota, K.; Oda, G.; Kikkawa, T. Feasibility of Portable Microwave Imaging Device for Breast Cancer Detection. Diagnostics 2022, 12, 27. https://doi.org/10.3390/diagnostics12010027
Adachi M, Nakagawa T, Fujioka T, Mori M, Kubota K, Oda G, Kikkawa T. Feasibility of Portable Microwave Imaging Device for Breast Cancer Detection. Diagnostics. 2022; 12(1):27. https://doi.org/10.3390/diagnostics12010027
Chicago/Turabian StyleAdachi, Mio, Tsuyoshi Nakagawa, Tomoyuki Fujioka, Mio Mori, Kazunori Kubota, Goshi Oda, and Takamaro Kikkawa. 2022. "Feasibility of Portable Microwave Imaging Device for Breast Cancer Detection" Diagnostics 12, no. 1: 27. https://doi.org/10.3390/diagnostics12010027
APA StyleAdachi, M., Nakagawa, T., Fujioka, T., Mori, M., Kubota, K., Oda, G., & Kikkawa, T. (2022). Feasibility of Portable Microwave Imaging Device for Breast Cancer Detection. Diagnostics, 12(1), 27. https://doi.org/10.3390/diagnostics12010027