Diagnostic Value of CEUS Prompting Liver Biopsy: Histopathological Correlation of Hepatic Lesions with Ambiguous Imaging Characteristics

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
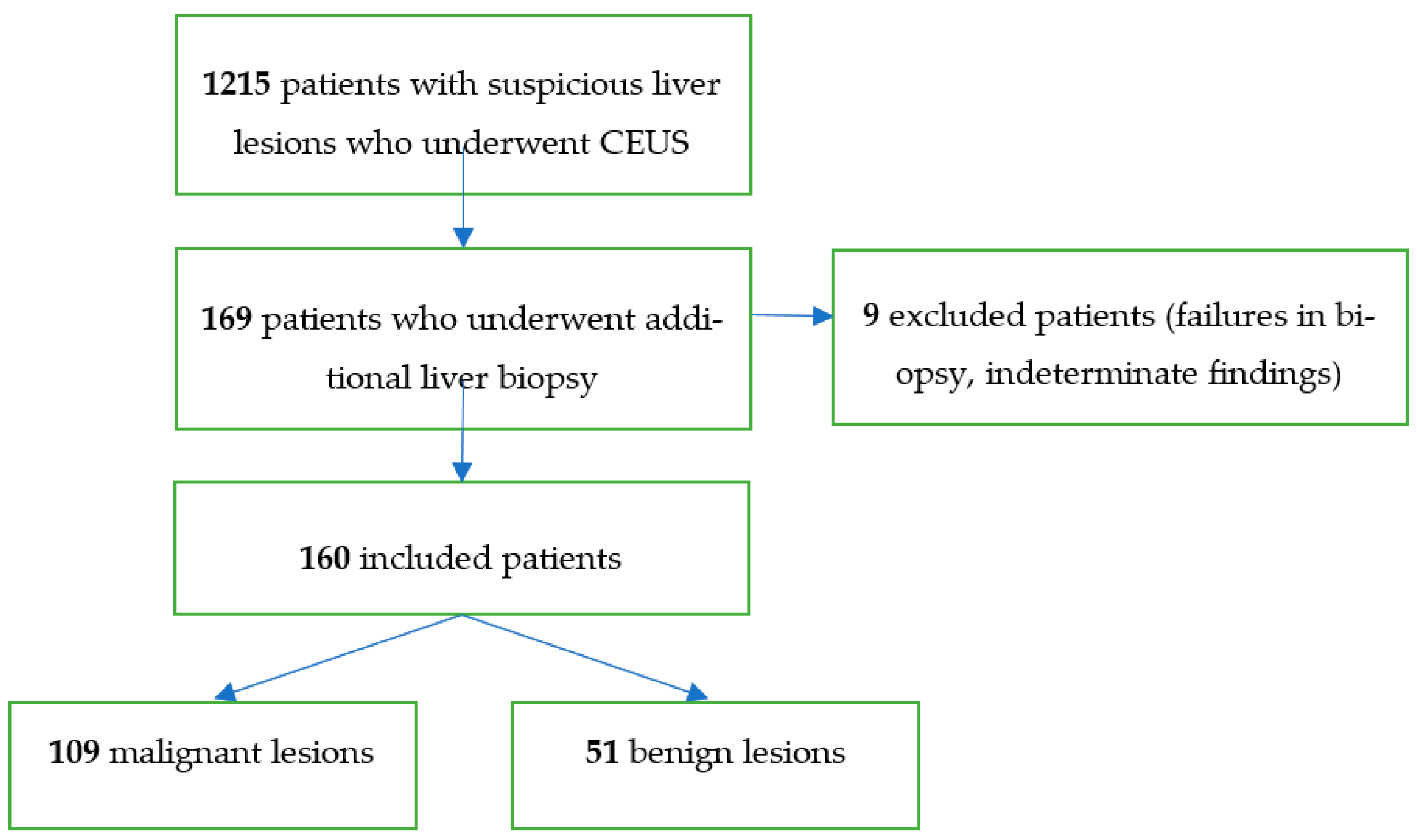
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef]
- Villanueva, A. Hepatocellular Carcinoma. N. Engl. J. Med. 2019, 380, 1450–1462. [Google Scholar] [CrossRef]
- Ghouri, Y.A.; Mian, I.; Rowe, J.H. Review of hepatocellular carcinoma: Epidemiology, etiology, and carcinogenesis. J. Carcinog. 2017, 16, 1. [Google Scholar]
- Zhang, D.Y.; Friedman, S.L. Fibrosis-dependent mechanisms of hepatocarcinogenesis. Hepatology 2012, 56, 769–775. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.Y.; Lee, J.M.; Sirlin, C.B. CT and MR imaging diagnosis and staging of hepatocellular carcinoma: Part I. Development, growth, and spread: Key pathologic and imaging aspects. Radiology 2014, 272, 635–654. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.Y.; Lee, J.M.; Sirlin, C.B. CT and MR imaging diagnosis and staging of hepatocellular carcinoma: Part II. Extracellular agents, hepatobiliary agents, and ancillary imaging features. Radiology 2014, 273, 30–50. [Google Scholar] [CrossRef] [PubMed]
- Claudon, M.; Dietrich, C.F.; Choi, B.I.; Cosgrove, D.O.; Kudo, M.; Nolsøe, C.P.; Piscaglia, F.; Wilson, S.R.; Barr, R.G.; Chammas, M.C.; et al. Guidelines and good clinical practice recommendations for Contrast Enhanced Ultrasound (CEUS) in the liver—Update 2012: A WFUMB-EFSUMB initiative in cooperation with representatives of AFSUMB, AIUM, ASUM, FLAUS and ICUS. Ultrasound Med. Biol. 2013, 39, 187–210. [Google Scholar] [CrossRef]
- Rübenthaler, J.; Bogner, F.; Reiser, M.; Clevert, D.A. Contrast-Enhanced Ultrasound (CEUS) of the Kidneys by Using the Bosniak Classification. Ultraschall Med. 2016, 37, 234–251. [Google Scholar] [CrossRef]
- Rübenthaler, J.; Paprottka, K.; Marcon, J.; Hameister, E.; Hoffmann, K.; Joiko, N.; Reiser, M.; Clevert, D.-A. Comparison of magnetic resonance imaging (MRI) and contrast-enhanced ultrasound (CEUS) in the evaluation of unclear solid renal lesions. Clin. Hemorheol. Microcirc. 2016, 64, 757–763. [Google Scholar] [CrossRef]
- Rübenthaler, J.; Reiser, M.; Clevert, D.-A. Diagnostic vascular ultrasonography with the help of color Doppler and contrast-enhanced ultrasonography. Ultrasonography 2016, 35, 289–301. [Google Scholar] [CrossRef]
- Greis, C. Ultrasound contrast agents as markers of vascularity and microcirculation. Clin. Hemorheol. Microcirc. 2009, 43, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Clevert, D.A.; D’Anastasi, M.; Jung, E.M. Contrast-enhanced ultrasound and microcirculation: Efficiency through dynamics—Current developments. Clin. Hemorheol. Microcirc. 2013, 53, 171–186. [Google Scholar] [CrossRef] [PubMed]
- Gassert, F.; Schnitzer, M.; Kim, S.H.; Kunz, W.G.; Ernst, B.P.; Clevert, D.-A.; Nörenberg, D.; Rübenthaler, J.; Froelich, M.F. Comparison of Magnetic Resonance Imaging and Contrast-Enhanced Ultrasound as Diagnostic Options for Unclear Cystic Renal Lesions: A Cost-Effectiveness Analysis. Ultraschall Med. 2020. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Piscaglia, F.; Bolondi, L. The safety of Sonovue in abdominal applications: Retrospective analysis of 23,188 investigations. Ultrasound Med. Biol. 2006, 32, 1369–1375. [Google Scholar] [CrossRef]
- Mueller-Peltzer, K.; Rübenthaler, J.; Reiser, M.; Clevert, D.-A. Contrast-enhanced ultrasound (CEUS) of the liver: Critical evaluation of use in clinical routine diagnostics. Radiology 2017, 57, 348–355. [Google Scholar]
- Kaltenbach, T.E.; Engler, P.; Kratzer, W.; Oeztuerk, S.; Seufferlein, T.; Haenle, M.M.; Graeter, T. Prevalence of benign focal liver lesions: Ultrasound investigation of 45,319 hospital patients. Abdom. Radiol. 2016, 41, 25–32. [Google Scholar] [CrossRef]
- Strobel, D.; Seitz, K.; Blank, W.; Schuler, A.; Dietrich, C.; Von Herbay, A.; Friedrich-Rust, M.; Kunze, G.; Becker, D.; Will, U.; et al. Contrast-enhanced Ultrasound for the Characterization of Focal Liver Lesions—Diagnostic Accuracy in Clinical Practice (DEGUM multicenter trial). Ultraschall Med. 2008, 29, 499–505. [Google Scholar] [CrossRef]
- Clevert, D.A.; Jung, E.; Stock, K.; Weckbach, S.; Feuerbach, S.; Reiser, M.; Jung, F. Evaluation of malignant liver tumors: Biphasic MS-CT versus quantitative contrast harmonic imaging ultrasound. Z. Gastroenterol. 2009, 47, 1195–1202. [Google Scholar] [CrossRef]
- Dietrich, C.F.; Kono, Y.; Cosgrove, D.O.; Jang, H.-J.; Kim, T.K.; Piscaglia, F.; Sirlin, C.B.; Willmann, J.K.; Vezeridis, A.; Wilson, S.R.; et al. Contrast Enhanced Ultrasound: Liver Imaging Reporting and Data System (CEUS LI-RADS). Ultrasound Med. Biol. 2017, 43, S38–S39. [Google Scholar] [CrossRef]
- Seitz, K.; Strobel, D.; Bernatik, T.; Blank, W.; Friedrich-Rust, M.; Von Herbay, A.; Dietrich, C.F.; Strunk, H.; Kratzer, W.; Schuler, A. Contrast-Enhanced Ultrasound (CEUS) for the Characterization of Focal Liver Lesions—Prospective Comparison in Clinical Practice: CEUS vs. CT (DEGUM Multicenter Trial) Parts of this Manuscript were presented at the Ultrasound Dreiländertreffen 2008, Davos. Ultraschall Med. 2009, 30, 383–389. [Google Scholar] [CrossRef]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, C. Liver Tumor Characterization—Comments and Illustrations Regarding Guidelines. Ultraschall Med. 2012, 33 (Suppl. 1), S22–S30. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, C.F.; Cui, X.W.; Barreiros, A.P.; Hocke, M.; Ignee, A. EFSUMB Guidelines 2011: Comment on Emergent Indications and Visions. Ultraschall Med. 2012, 33 (Suppl. 1), S39–S47. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, C.F.; Cui, X.W.; Boozari, B.; Hocke, M.; Ignee, A. Contrast-Enhanced Ultrasound (CEUS) in the Diagnostic Algorithm of Hepatocellular and Cholangiocellular Carcinoma, Comments on the AASLD Guidelines. Ultraschall Med. 2012, 33 (Suppl. 1), S57–S66. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, C.F.; Cui, X.W.; Schreiber-Dietrich, D.G.; Ignee, A. EFSUMB Guidelines 2011: Comments and Illustrations. Ultraschall Med. 2012, 33 (Suppl. 1), S11–S21. [Google Scholar] [CrossRef] [PubMed]
- Sporea, I.; Badea, R.; Martie, A.; Dumitru, E.; Ioaniţescu, S.; Șirli, R.; Socaciu, M.A.; Popescu, A.; Danilă, M.; Voiculescu, M. Contrast Enhanced Ultrasound for the evaluation of focal liver lesions in daily practice. A multicentre study. Med Ultrason. 2012, 14, 95–100. [Google Scholar]
- Rübenthaler, J.; Paprottka, K.; Hameister, E.; Hoffmann, K.; Joiko, N.; Reiser, M.; Clevert, D. Vascular complications in liver transplantation: Beneficial role of contrast-enhanced ultrasound (CEUS) in the postoperative phase. Clin. Hemorheol. Microcirc. 2016, 64, 475–482. [Google Scholar] [CrossRef]
- Rübenthaler, J.; Paprottka, K.; Hameister, E.; Hoffmann, K.; Joiko, N.; Reiser, M.; Clevert, D.-A. Malignancies after liver transplantation: Value of contrast-enhanced ultrasound (CEUS). Clin. Hemorheol. Microcirc. 2016, 64, 467–473. [Google Scholar] [CrossRef]
- De Figueiredo, G.N.; Mueller-Peltzer, K.; Zengel, P.; Armbrüster, M.; Rübenthaler, J.; Clevert, D.-A. Diagnostic performance of contrast-enhanced ultrasound (CEUS) for the evaluation of gallbladder diseases1. Clin. Hemorheol. Microcirc. 2018, 69, 83–91. [Google Scholar] [CrossRef]
- Palmieri, V.O.; Santovito, D.; Marano, G.; Minerva, F.; Ricci, L.; D’Alitto, F.; Angelelli, G.; Palasciano, G. Contrast-enhanced ultrasound in the diagnosis of hepatocellular carcinoma. Radiol. Med. 2015, 120, 627–633. [Google Scholar] [CrossRef]
- Schwarze, V.; Marschner, C.; De Figueiredo, G.N.; Rübenthaler, J.; Clevert, D.-A. Single-Center Study: Evaluating the Diagnostic Performance and Safety of Contrast-Enhanced Ultrasound (CEUS) in Pregnant Women to Assess Hepatic Lesions. Ultraschall Med. 2019, 41, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Schwarze, V.; Marschner, C.; Völckers, W.; Grosu, S.; De Figueiredo, G.N.; Rübenthaler, J.; Clevert, D.-A. Diagnostic value of contrast-enhanced ultrasound versus computed tomography for hepatocellular carcinoma: A retrospective, single-center evaluation of 234 patients. J. Int. Med Res. 2020, 48, 300060520930151. [Google Scholar] [CrossRef] [PubMed]
- Schwarze, V.; Marschner, C.; Völckers, W.; De Figueiredo, G.N.; Rübenthaler, J.; Clevert, D.-Á. The diagnostic performance of contrast-enhanced ultrasound (CEUS) for evaluating hepatocellular carcinoma (HCC) juxtaposed to MRI findings; a retrospective single-center analysis of 292 patients. Clin. Hemorheol. Microcirc. 2020, 76, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.K.; Lee, E.; Jang, H.J. Imaging findings of mimickers of hepatocellular carcinoma. Clin. Mol. Hepatol. 2015, 21, 326–343. [Google Scholar] [CrossRef]
- Jang, H.-J.; Kim, T.K.; Burns, P.N.; Wilson, S.R. Enhancement Patterns of Hepatocellular Carcinoma at Contrast-enhanced US: Comparison with Histologic Differentiation. Radiology 2007, 244, 898–906. [Google Scholar] [CrossRef]
- Brown, K.T.; Gandhi, R.T.; Covey, A.M.; Brody, L.A.; Getrajdman, G.I. Pylephlebitis and liver abscess mimicking hepatocellular carcinoma. Hepatobiliary Pancreat. Dis. Int. 2003, 2, 221–225. [Google Scholar]
- Mörk, H.; Ignee, A.; Schuessler, G.; Ott, M.; Dietrich, C.F. Analysis of neuroendocrine tumour metastases in the liver using contrast enhanced ultrasonography. Scand. J. Gastroenterol. 2007, 42, 652–662. [Google Scholar] [CrossRef]
- Ran, L.; Zhao, W.; Zhao, Y.; Bu, H. Value of contrast-enhanced ultrasound in differential diagnosis of solid lesions of pancreas (SLP): A systematic review and a meta-analysis. Medicine 2017, 96, e7463. [Google Scholar] [CrossRef]
- Schwarze, V.; Rübenthaler, J.; Marschner, C.; Fabritius, M.P.; Rueckel, J.; Fink, N.; Puhr-Westerheide, D.; Gresser, E.; Froelich, M.F.; Schnitzer, M.L.; et al. Advanced Fusion Imaging and Contrast-Enhanced Imaging (CT/MRI–CEUS) in Oncology. Cancers 2020, 12, 2821. [Google Scholar] [CrossRef]
- Seitz, K.; Strobel, D. A Milestone: Approval of CEUS for Diagnostic Liver Imaging in Adults and Children in the USA. Ultraschall Med. 2016, 37, 229–232. [Google Scholar] [CrossRef]
- Schwarze, V.; Froelich, M.F.; Marschner, C.; Knösel, T.; Rübenthaler, J.; Clevert, D.-A. Safe and pivotal approaches using contrast-enhanced ultrasound for the diagnostic workup of non-obstetric conditions during pregnancy, a single-center experience. Arch. Gynecol. Obstet. 2020. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Histopathology | Frequency |
|---|---|
| HCC | 38 |
| CCC | 4 |
| Metastasis | 59 |
| Lymphoma | 4 |
| HCC/CCC mixed type | 4 |
| Hemangioma | 3 |
| Cyst | 2 |
| Abscess | 3 |
| Hepatitis | 4 |
| Fibrosis | 10 |
| Cirrhosis | 9 |
| Candida infection | 1 |
| FNH | 2 |
| Hemangioma/FNH mixed type | 1 |
| Echinococcus cyst | 1 |
| Focal hepatic steatosis | 3 |
| Other reactive changes | 3 |
| Inconspicuous | 13 |
| Total (n = 160) | CEUS Positive | CEUS Negative | ||
|---|---|---|---|---|
| Sensitivity | ||||
| Malignant | n = 109 | 103 | 6 | 94.5% |
| Specificity | ||||
| Benign | n = 51 | 15 | 36 | 70.6% |
| TPR/ Concordance | TNR/ 1-Discordance | |||
| 87.3% | 85.7% |
| Misclassification | Histopathology |
|---|---|
| False positive | Fibrotic lesions: n = 7 |
| Cirrhotic lesions: n = 3 | |
| No pathologic changes: n = 2 | |
| Adenoma: n = 1 | |
| Reactive changes: n = 1 | |
| Abscess: n = 1 | |
| False negative | HCC: n = 4 |
| Neuroendocrine tumor (Metastasis): n = 1 | |
| Adenoma carcinoma (Metastasis): n = 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Geyer, T.; Clevert, D.-A.; Schwarz, S.; Reidler, P.; Gassenmaier, S.; Knösel, T.; Rübenthaler, J.; Schwarze, V.; Armbruster, M. Diagnostic Value of CEUS Prompting Liver Biopsy: Histopathological Correlation of Hepatic Lesions with Ambiguous Imaging Characteristics. Diagnostics 2021, 11, 35. https://doi.org/10.3390/diagnostics11010035
Geyer T, Clevert D-A, Schwarz S, Reidler P, Gassenmaier S, Knösel T, Rübenthaler J, Schwarze V, Armbruster M. Diagnostic Value of CEUS Prompting Liver Biopsy: Histopathological Correlation of Hepatic Lesions with Ambiguous Imaging Characteristics. Diagnostics. 2021; 11(1):35. https://doi.org/10.3390/diagnostics11010035
Chicago/Turabian StyleGeyer, Thomas, Dirk-André Clevert, Sonja Schwarz, Paul Reidler, Sebastian Gassenmaier, Thomas Knösel, Johannes Rübenthaler, Vincent Schwarze, and Marco Armbruster. 2021. "Diagnostic Value of CEUS Prompting Liver Biopsy: Histopathological Correlation of Hepatic Lesions with Ambiguous Imaging Characteristics" Diagnostics 11, no. 1: 35. https://doi.org/10.3390/diagnostics11010035
APA StyleGeyer, T., Clevert, D.-A., Schwarz, S., Reidler, P., Gassenmaier, S., Knösel, T., Rübenthaler, J., Schwarze, V., & Armbruster, M. (2021). Diagnostic Value of CEUS Prompting Liver Biopsy: Histopathological Correlation of Hepatic Lesions with Ambiguous Imaging Characteristics. Diagnostics, 11(1), 35. https://doi.org/10.3390/diagnostics11010035