The Detection of Bile Acids in the Lungs of Paediatric Cystic Fibrosis Patients Is Associated with Altered Inflammatory Patterns

 ,
,  ,
,
Abstract
1. Introduction
2. Material and Methods
2.1. BALF Collection, Cytology and Cytokine Measurements
2.2. Bile Acid Profiling
2.3. Statistical Analysis
2.4. Ethics, Consent and Permissions
2.5. Data Availability
3. Results
3.1. Clinical and Genetic Characterization of the Study Cohort
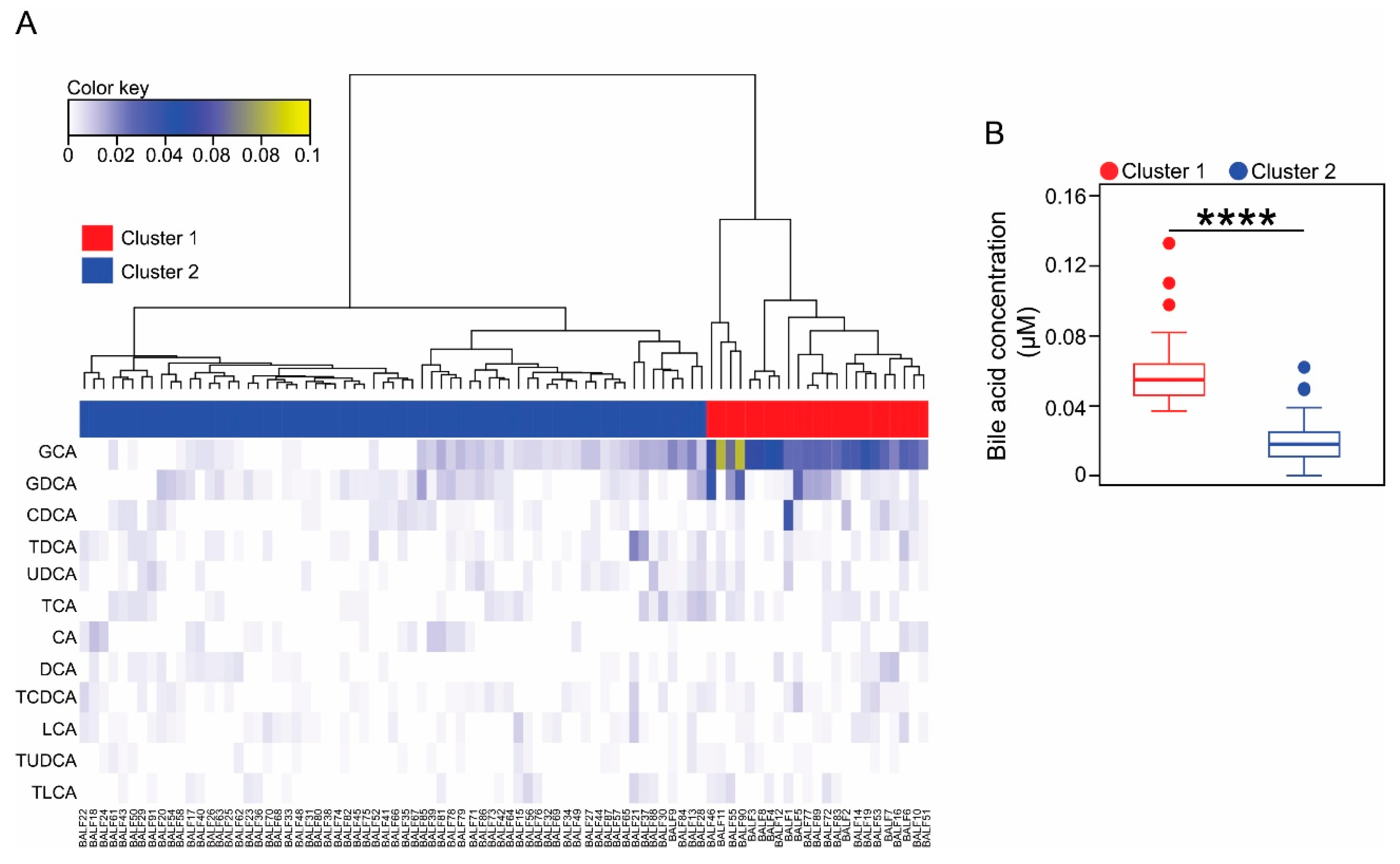
3.2. Classification of the Paediatric Cohort Based on Bile Acid Profiles in BALF
3.3. Cluster 1 Membership Is Associated with Inflammatory Markers
3.4. Cluster Membership Predicts the Progression of CF Lung Disease
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Riordan, J.R.; Rommens, J.M.; Kerem, B.; Alon, N.; Rozmahel, R.; Grzelczak, Z.; Zielenski, J.; Lok, S.; Plavsic, N.; Chou, J.L.; et al. Identification of the cystic fibrosis gene: Cloning and characterization of complementary DNA. Science 1989, 245, 1066–1073. [Google Scholar] [CrossRef] [PubMed]
- Kreda, S.M.; Davis, C.W.; Rose, M.C. CFTR, mucins, and mucus obstruction in cystic fibrosis. Cold Spring Harb. Perspect. Med. 2012, 2, a009589. [Google Scholar] [CrossRef] [PubMed]
- Sabharwal, S. Gastrointestinal Manifestations of Cystic Fibrosis. Gastroenterol. Hepatol. 2016, 12, 43–47. [Google Scholar]
- Trezise, A.E.; Buchwald, M. In vivo cell-specific expression of the cystic fibrosis transmembrane conductance regulator. Nature 1991, 353, 434–437. [Google Scholar] [CrossRef]
- Stick, S.M.; Brennan, S.; Murray, C.; Douglas, T.; von Ungern-Sternberg, B.S.; Garratt, L.W.; Gangell, C.L.; De Klerk, N.; Linnane, B.; Ranganathan, S.; et al. Bronchiectasis in infants and preschool children diagnosed with cystic fibrosis after newborn screening. J. Pediatrics 2009, 155, 623–628. [Google Scholar] [CrossRef]
- Sly, P.D.; Gangell, C.L.; Chen, L.; Ware, R.S.; Ranganathan, S.; Mott, L.S.; Murray, C.P.; Stick, S.M.; Investigators, A.C. Risk factors for bronchiectasis in children with cystic fibrosis. New Engl. J. Med. 2013, 368, 1963–1970. [Google Scholar] [CrossRef]
- Smyth, A.; Elborn, J.S. Exacerbations in cystic fibrosis: 3--Management. Thorax 2008, 63, 180–184. [Google Scholar] [CrossRef]
- Goss, C.H.; Burns, J.L. Exacerbations in cystic fibrosis. 1: Epidemiology and pathogenesis. Thorax 2007, 62, 360–367. [Google Scholar] [CrossRef]
- Bell, S.C.; Robinson, P.J. Exacerbations in cystic fibrosis: 2. prevention. Thorax 2007, 62, 723–732. [Google Scholar] [CrossRef]
- Marsland, B.J.; Trompette, A.; Gollwitzer, E.S. The Gut-Lung Axis in Respiratory Disease. Ann. Am. Thorac. Soc. 2015, 12 Suppl 2, S150–S156. [Google Scholar] [CrossRef]
- Budden, K.F.; Gellatly, S.L.; Wood, D.L.; Cooper, M.A.; Morrison, M.; Hugenholtz, P.; Hansbro, P.M. Emerging pathogenic links between microbiota and the gut-lung axis. Nat. Rev. Microbiol. 2017, 15, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Robinson, N.B.; DiMango, E. Prevalence of gastroesophageal reflux in cystic fibrosis and implications for lung disease. Ann. Am. Thorac. Soc. 2014, 11, 964–968. [Google Scholar] [CrossRef] [PubMed]
- Mandal, P.; Morice, A.H.; Chalmers, J.D.; Hill, A.T. Symptoms of airway reflux predict exacerbations and quality of life in bronchiectasis. Respir. Med. 2013, 107, 1008–1013. [Google Scholar] [CrossRef] [PubMed]
- Hurst, J.R.; Vestbo, J.; Anzueto, A.; Locantore, N.; Mullerova, H.; Tal-Singer, R.; Miller, B.; Lomas, D.A.; Agusti, A.; Macnee, W.; et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. New Engl. J. Med. 2010, 363, 1128–1138. [Google Scholar] [CrossRef]
- Lee, J.S.; Song, J.W.; Wolters, P.J.; Elicker, B.M.; King, T.E., Jr.; Kim, D.S.; Collard, H.R. Bronchoalveolar lavage pepsin in acute exacerbation of idiopathic pulmonary fibrosis. Eur. Respir. J. 2012, 39, 352–358. [Google Scholar] [CrossRef]
- Reen, F.J.; Flynn, S.; Woods, D.F.; Dunphy, N.; Chroinin, M.N.; Mullane, D.; Stick, S.; Adams, C.; O’Gara, F. Bile signalling promotes chronic respiratory infections and antibiotic tolerance. Sci. Rep. 2016, 6, 29768. [Google Scholar] [CrossRef]
- Reen, F.J.; Woods, D.F.; Mooij, M.J.; Adams, C.; O’Gara, F. Respiratory pathogens adopt a chronic lifestyle in response to bile. PLoS ONE 2012, 7, e45978. [Google Scholar] [CrossRef]
- Ulluwishewa, D.; Wang, L.; Pereira, C.; Flynn, S.; Cain, E.; Stick, S.; Reen, F.J.; Ramsay, J.P.; O’Gara, F. Dissecting the regulation of bile-induced biofilm formation in Staphylococcus aureus. Microbiology 2016, 162, 1398–1406. [Google Scholar] [CrossRef]
- Legendre, C.; Reen, F.J.; Woods, D.F.; Mooij, M.J.; Adams, C.; O’Gara, F. Bile acids repress hypoxia-inducible factor 1 signaling and modulate the airway immune response. Infect. Immun. 2014, 82, 3531–3541. [Google Scholar] [CrossRef]
- Blondeau, K.; Dupont, L.J.; Mertens, V.; Verleden, G.; Malfroot, A.; Vandenplas, Y.; Hauser, B.; Sifrim, D. Gastro-oesophageal reflux and aspiration of gastric contents in adult patients with cystic fibrosis. Gut 2008, 57, 1049–1055. [Google Scholar] [CrossRef]
- Vic, P.; Tassin, E.; Turck, D.; Gottrand, F.; Launay, V.; Farriaux, J.P. Frequency of gastroesophageal reflux in infants and in young children with cystic fibrosis. Arch. De Pediatrie: Organe Off. De La Soc. Fr. De Pediatrie 1995, 2, 742–746. [Google Scholar] [CrossRef]
- Gotley, D.C.; Morgan, A.P.; Cooper, M.J. Bile acid concentrations in the refluxate of patients with reflux oesophagitis. Br. J. Surg. 1988, 75, 587–590. [Google Scholar] [CrossRef] [PubMed]
- Mott, L.S.; Park, J.; Murray, C.P.; Gangell, C.L.; de Klerk, N.H.; Robinson, P.J.; Robertson, C.F.; Ranganathan, S.C.; Sly, P.D.; Stick, S.M.; et al. Progression of early structural lung disease in young children with cystic fibrosis assessed using CT. Thorax 2012, 67, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Sly, P.D.; Brennan, S.; Gangell, C.; de Klerk, N.; Murray, C.; Mott, L.; Stick, S.M.; Robinson, P.J.; Robertson, C.F.; Ranganathan, S.C.; et al. Lung disease at diagnosis in infants with cystic fibrosis detected by newborn screening. Am. J. Respir. Crit. Care Med. 2009, 180, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Pillarisetti, N.; Williamson, E.; Linnane, B.; Skoric, B.; Robertson, C.F.; Robinson, P.; Massie, J.; Hall, G.L.; Sly, P.; Stick, S.; et al. Infection, inflammation, and lung function decline in infants with cystic fibrosis. Am. J. Respir. Crit. Care Med. 2011, 184, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Reen, F.J.; Woods, D.F.; Mooij, M.J.; Chroinin, M.N.; Mullane, D.; Zhou, L.; Quille, J.; Fitzpatrick, D.; Glennon, J.D.; McGlacken, G.P.; et al. Aspirated bile: A major host trigger modulating respiratory pathogen colonisation in cystic fibrosis patients. Eur. J. Clin. Microbiol. Infect. Dis.: Off. Publ. Eur. Soc. Clin. Microbiol. 2014, 33, 1763–1771. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2017. [Google Scholar]
- Ward, J.H. Hierarchical grouping to optimize an objective function. J. Am. Stat. Assoc. 1963, 58, 236–244. [Google Scholar] [CrossRef]
- Murtagh, F.; Legendre, P. Ward’s hierarchical agglomerative clustering method: Which algorithms implement Ward’s criterion? J. Classif. 2014, 31, 274–295. [Google Scholar] [CrossRef]
- Maechler, M.R.; Struyf, A.; Hubert, M.; Hornik, K. Cluster: Cluster analysis basics and extensions. R Package Version 2.0.7-1. 2018. Available online: https://cran.r-project.org/web/packages/cluster/ (accessed on 21 August 2018).
- Charrad, M.; Ghazzali, N.; Boiteau, V.; Niknafs, A. NbClust: An R package for determining the relevant number of clusters in a data set. J. Stat. Softw. 2014, 61, 1–36. [Google Scholar] [CrossRef]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting linear mixed-effects models using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Rossi, S.S.; Converse, J.L.; Hofmann, A.F. High pressure liquid chromatographic analysis of conjugated bile acids in human bile: Simultaneous resolution of sulfated and unsulfated lithocholyl amidates and the common conjugated bile acids. J. Lipid Res. 1987, 28, 589–595. [Google Scholar] [PubMed]
- Pauwels, A.; Decraene, A.; Blondeau, K.; Mertens, V.; Farre, R.; Proesmans, M.; Van Bleyenbergh, P.; Sifrim, D.; Dupont, L.J. Bile acids in sputum and increased airway inflammation in patients with cystic fibrosis. Chest 2012, 141, 1568–1574. [Google Scholar] [CrossRef] [PubMed]
- Aseeri, A.; Brodlie, M.; Lordan, J.; Corris, P.; Pearson, J.; Ward, C.; Manning, N. Bile acids are present in the lower airways of people with cystic fibrosis. Am. J. Respir. Crit. Care Med. 2012, 185, 463. [Google Scholar] [CrossRef]
- Calinski, T.; Harabasz, J. A dendrite method for cluster analysis. Commun. Stat. - Theory Methods 1974, 3, 1–27. [Google Scholar] [CrossRef]
- Kaufman, L.; Rousseeuw, P.J. Partitioning around medoids (program PAM). In Finding Groups in Data, an Introduction to Cluster Analysis; John Wiley and Sons: Hoboken, NJ, USA, 1990; pp. 83–88. [Google Scholar]
- Rousseeuw, P.J. Silhouettes - a Graphical Aid to the Interpretation and Validation of Cluster-Analysis. J Comput Appl Math 1987, 20, 53–65. [Google Scholar] [CrossRef]
- Arumugam, M.; Raes, J.; Pelletier, E.; Le Paslier, D.; Yamada, T.; Mende, D.R.; Fernandes, G.R.; Tap, J.; Bruls, T.; Batto, J.-M.; et al. Enterotypes of the human gut microbiome. Nature 2011, 473, 174. [Google Scholar] [CrossRef] [PubMed]
- Rosenow, T.; Oudraad, M.C.; Murray, C.P.; Turkovic, L.; Kuo, W.; de Bruijne, M.; Ranganathan, S.C.; Tiddens, H.A.; Stick, S.M. Australian Respiratory Early Surveillance Team for Cystic, F. PRAGMA-CF. A Quantitative Structural Lung Disease Computed Tomography Outcome in Young Children with Cystic Fibrosis. Am. J. Respir. Crit. Care Med. 2015, 191, 1158–1165. [Google Scholar] [CrossRef]
- Rasmussen, T.R.; Korsgaard, J.; Moller, J.K.; Sommer, T.; Kilian, M. Quantitative culture of bronchoalveolar lavage fluid in community-acquired lower respiratory tract infections. Respir. Med. 2001, 95, 885–890. [Google Scholar] [CrossRef][Green Version]
- Dittrich, A.S.; Kuhbandner, I.; Gehrig, S.; Rickert-Zacharias, V.; Twigg, M.; Wege, S.; Taggart, C.C.; Herth, F.; Schultz, C.; Mall, M.A. Elastase activity on sputum neutrophils correlates with severity of lung disease in cystic fibrosis. Eur. Respir. J. 2018, 51. [Google Scholar] [CrossRef]
- de Aguiar Vallim, T.Q.; Tarling, E.J.; Edwards, P.A. Pleiotropic roles of bile acids in metabolism. Cell Metab. 2013, 17, 657–669. [Google Scholar] [CrossRef]
- Brestoff, J.R.; Artis, D. Commensal bacteria at the interface of host metabolism and the immune system. Nat. Immunol. 2013, 14, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Hylemon, P.B.; Zhou, H.; Pandak, W.M.; Ren, S.; Gil, G.; Dent, P. Bile acids as regulatory molecules. J. Lipid Res. 2009, 50, 1509–1520. [Google Scholar] [CrossRef] [PubMed]
- Duboc, H.; Rajca, S.; Rainteau, D.; Benarous, D.; Maubert, M.A.; Quervain, E.; Thomas, G.; Barbu, V.; Humbert, L.; Despras, G.; et al. Connecting dysbiosis, bile-acid dysmetabolism and gut inflammation in inflammatory bowel diseases. Gut 2013, 62, 531–539. [Google Scholar] [CrossRef]
- Mouzaki, M.; Wang, A.Y.; Bandsma, R.; Comelli, E.M.; Arendt, B.M.; Zhang, L.; Fung, S.; Fischer, S.E.; McGilvray, I.G.; Allard, J.P. Bile Acids and Dysbiosis in Non-Alcoholic Fatty Liver Disease. PLoS ONE 2016, 11, e0151829. [Google Scholar] [CrossRef] [PubMed]
- Neujahr, D.C.; Uppal, K.; Force, S.D.; Fernandez, F.; Lawrence, C.; Pickens, A.; Bag, R.; Lockard, C.; Kirk, A.D.; Tran, V.; et al. Bile acid aspiration associated with lung chemical profile linked to other biomarkers of injury after lung transplantation. Am. J. Transplant. 2014, 14, 841–848. [Google Scholar] [CrossRef]
- Campbell, E.L.; Bruyninckx, W.J.; Kelly, C.J.; Glover, L.E.; McNamee, E.N.; Bowers, B.E.; Bayless, A.J.; Scully, M.; Saeedi, B.J.; Golden-Mason, L.; et al. Transmigrating neutrophils shape the mucosal microenvironment through localized oxygen depletion to influence resolution of inflammation. Immunity 2014, 40, 66–77. [Google Scholar] [CrossRef]
- Lappalainen, U.; Whitsett, J.A.; Wert, S.E.; Tichelaar, J.W.; Bry, K. Interleukin-1beta causes pulmonary inflammation, emphysema, and airway remodeling in the adult murine lung. Am. J. Respir. Cell Mol. Biol. 2005, 32, 311–318. [Google Scholar] [CrossRef]
- Esther, C.R., Jr.; Muhlebach, M.S.; Ehre, C.; Hill, D.B.; Wolfgang, M.C.; Kesimer, M.; Ramsey, K.A.; Markovetz, M.R.; Garbarine, I.C.; Forest, M.G.; et al. Mucus accumulation in the lungs precedes structural changes and infection in children with cystic fibrosis. Sci. Transl. Med. 2019, 11. [Google Scholar] [CrossRef]
- Richardson, P.S.; Peatfield, A.C. The control of airway mucus secretion. Eur. J. Respir. Dis. 1987, 153, 43–51. [Google Scholar]
- Quinn, R.A.; Melnik, A.V.; Vrbanac, A.; Fu, T.; Patras, K.A.; Christy, M.P.; Bodai, Z.; Belda-Ferre, P.; Tripathi, A.; Chung, L.K.; et al. Global chemical effects of the microbiome include new bile-acid conjugations. Nature 2020, 579, 123–129. [Google Scholar] [CrossRef]
- Perez, M.J.; Briz, O. Bile-acid-induced cell injury and protection. World J. Gastroenterol. 2009, 15, 1677–1689. [Google Scholar] [CrossRef] [PubMed]
- Russell, A.B.; Peterson, S.B.; Mougous, J.D. Type VI secretion system effectors: Poisons with a purpose. Nat. Rev. Microbiol. 2014, 12, 137–148. [Google Scholar] [CrossRef] [PubMed]
- Bergsbaken, T.; Fink, S.L.; Cookson, B.T. Pyroptosis: Host cell death and inflammation. Nat. Rev. Microbiol. 2009, 7, 99–109. [Google Scholar] [CrossRef] [PubMed]
- McNally, P.; Ervine, E.; Shields, M.D.; Dimitrov, B.D.; El Nazir, B.; Taggart, C.C.; Greene, C.M.; McElvaney, N.G.; Greally, P. High concentrations of pepsin in bronchoalveolar lavage fluid from children with cystic fibrosis are associated with high interleukin-8 concentrations. Thorax 2011, 66, 140–143. [Google Scholar] [CrossRef]
- Hallberg, K.; Fandriks, L.; Strandvik, B. Duodenogastric bile reflux is common in cystic fibrosis. J. Pediatric Gastroenterol. Nutr. 2004, 38, 312–316. [Google Scholar] [CrossRef]
- O’Brien, S.; Mulcahy, H.; Fenlon, H.; O’Broin, A.; Casey, M.; Burke, A.; FitzGerald, M.X.; Hegarty, J.E. Intestinal bile acid malabsorption in cystic fibrosis. Gut 1993, 34, 1137–1141. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Cluster 1 | Cluster 2 | p-Value |
|---|---|---|---|
| NE (ng mL−1) | 100 (100–100) | 100 (100–100) | 1 |
| IL8 (pg mL−1) | 1075 (300–2150) | 810 (250–1890) | 1 |
| IL1β (ng mL−1) | 83.8 (54.44–122.52) | 10 (10–32.58) | 0.006 |
| IL6 (ng mL−1) | 57.79 (34.73–77.65) | 10 (10–10) | 0.041 |
| Total cell count | |||
| (x106 cells mL−1 BALF) | 0.32 (0.23–0.57) | 0.29 (0.18–0.38) | 1 |
| % viability | 74.8 (62.4–80.05) | 82.8 (73.1–87.3) | 0.038 |
| % macrophages | 83.33 (61.58–93.42) | 86.67 (70.33–94) | 1 |
| % neutrophils | 16.33 (6.58–38.24) | 12 (4.33–29) | 1 |
| % lymphocytes | 0 (0–0.33) | 0 (0–1.67) | 1 |
| % eosinophils | 0 (0–0.33) | 0 (0–0.3) | 1 |
| Variable | Cluster 1 | Cluster 2 | p-Value |
|---|---|---|---|
| Bronchiectasis score | 1 (0–2) | 1 (0–3.5) | 1 |
| BW thickening score | 10 (7–10) | 8 (5–10) | 1 |
| Air trapped score | 1 (0.75–4) | 2 (1–4) | 1 |
| Mu. plugging score | 0 (0–0.25) | 0 (0–1) | 1 |
| % Dis | 2.99 (2.39–4.13) | 2.17 (1.1–3.8) | 0.94 |
| % Bx | 0 (0–0.075) | 0 (0–0.38) | 1 |
| % TA | 2.06 (0.96–6.14) | 1.28 (0.19–5.86) | 1 |
| % Atelec | 0.06 (0–1.77) | 0.2 (0–0.97) | 1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caparrós-Martín, J.A.; Flynn, S.; Reen, F.J.; Woods, D.F.; Agudelo-Romero, P.; Ranganathan, S.C.; Stick, S.M.; O’Gara, F. The Detection of Bile Acids in the Lungs of Paediatric Cystic Fibrosis Patients Is Associated with Altered Inflammatory Patterns. Diagnostics 2020, 10, 282. https://doi.org/10.3390/diagnostics10050282
Caparrós-Martín JA, Flynn S, Reen FJ, Woods DF, Agudelo-Romero P, Ranganathan SC, Stick SM, O’Gara F. The Detection of Bile Acids in the Lungs of Paediatric Cystic Fibrosis Patients Is Associated with Altered Inflammatory Patterns. Diagnostics. 2020; 10(5):282. https://doi.org/10.3390/diagnostics10050282
Chicago/Turabian StyleCaparrós-Martín, Jose A., Stephanie Flynn, F. Jerry Reen, David F. Woods, Patricia Agudelo-Romero, Sarath C. Ranganathan, Stephen M. Stick, and Fergal O’Gara. 2020. "The Detection of Bile Acids in the Lungs of Paediatric Cystic Fibrosis Patients Is Associated with Altered Inflammatory Patterns" Diagnostics 10, no. 5: 282. https://doi.org/10.3390/diagnostics10050282
APA StyleCaparrós-Martín, J. A., Flynn, S., Reen, F. J., Woods, D. F., Agudelo-Romero, P., Ranganathan, S. C., Stick, S. M., & O’Gara, F. (2020). The Detection of Bile Acids in the Lungs of Paediatric Cystic Fibrosis Patients Is Associated with Altered Inflammatory Patterns. Diagnostics, 10(5), 282. https://doi.org/10.3390/diagnostics10050282